

Case Report | DOI: https://doi.org/10.31579/2835-785X/101
Left Main Coronary Artery Aneurysm and Coronary Artery Disease
1 Associate Consultant, Department of Cardiac Anaesthesia, Medanta-The Medicity, Gurugram (Haryana)-122001, India
2 Senior Director, Department of Cardiac Anaesthesia, Medanta-The Medicity, Gurugram (Haryana)-122001, India.
*Corresponding Author: Senior Director, Department of Cardiac Anaesthesia, Medanta-The Medicity, Gurugram (Haryana)-122001, India.
Citation: Ravina Mukati, and Ajmer Singh, (2025), Left Main Coronary Artery Aneurysm and Coronary Artery Disease, International Journal of Clinical Research and Reports. 4(5); DOI: 10.31579/2835-785X/101
Copyright: © 2025, Dr. Ajmer Singh. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 29 August 2025 | Accepted: 16 October 2025 | Published: 27 October 2025
Keywords: Left main coronary artery aneurysm, coronary artery disease, aneurysm ligation, coronary artery bypass graft surgery
Abstract
Coronary artery aneurysms are found in a small percentage of coronary angiograms, with left main coronary artery aneurysms being the least common anomaly found in approximately 0.1% of patients who undergo angiography. The most common cause of coronary artery aneurysms is atherosclerosis. Angiography is the gold standard for diagnosis. We report a 57-year-old female patient who presented with unstable angina, and her electrocardiogram showed T-wave inversion in the precordial leads. Coronary angiography revealed a large saccular aneurysm of the left main coronary artery with significant stenosis in the left anterior descending and left circumflex artery. The patient underwent ligation of the aneurysm and double-vessel coronary artery bypass graft surgery.
Introduction
A coronary artery aneurysm (CAA) is defined as a localized coronary dilatation >1.5 times the diameter of the normal adjacent segment. The reported incidence rate of CAAs ranges from 0.3% to 5.3%, with pooled data showing a mean incidence rate of 1.65%.[1] CAAs are more frequent in the right coronary artery (40%), followed in frequency by the left circumflex and left anterior descending (LAD) artery (32%). Aneurysm of the left main coronary artery (LMCA) is very rare, with a reported incidence of 0.1% in patients undergoing coronary angiography.[2] The coronary portions more often affected are the proximal or mid-segment, rather than the distal segment of the vessels. The prevalence of CAAs is higher in men.
Most CAAs are caused by atherosclerosis. Other possible causes include Kawasaki disease and Takayasu disease in children; and certain infectious, vasculitis (lupus, rheumatoid arthritis, ankylosing spondylitis), trauma, connective tissue disorders (Marfan syndrome, Ehlers-Danlos syndrome, fibromuscular dysplasia), neoplastic disorders, drug abuse (cocaine, amphetamine), idiopathic, and iatrogenic in adult patients. [3] Occasionally, a CAA can become complicated, developing intravascular thrombosis, distal embolization, vessel rupture with a consequent myocardial ischemia, arrhythmias, and heart failure. The management of CAAs remains a challenge for clinicians due to the absence of clear guidelines or treatment protocols. Management options include medical treatment with anticoagulation, percutaneous coronary interventions (PCI), or surgical ligation of the aneurysm with distal coronary artery bypass graft (CABG) surgery.[4] We describe herein a 57-year-old female presenting with unstable angina and failed PCI whose coronary angiogram revealed an aneurysm of the LMCA along with coronary artery disease (CAD).
Case Report
A 57-year-old female presented to our hospital with hypertension and unstable angina in July 2025. She has undergone coronary angiography and a failed attempt at PCI in the previous hospital. Her past records were unavailable. She denied any history of chest trauma, infection, pericarditis, or previous myocardial infection. On examination, she had a pulse of 65 beats/minute, a blood pressure of 160/90 mmHg, and a respiratory rate of 20 breaths/minute. Physical examination and laboratory tests were normal. Electrocardiography showed poor progression of ‘r’ waves in leads I and aVL, and T-wave inversion in the precordial leads (V1-V5, Fig 1). Transthoracic echocardiography showed akinetic mid anterior septum, mid anterior wall, and apex with an ejection fraction of 35%. Coronary angiography revealed a saccular aneurysm of the LMCA, measuring 20 mm x 26 mm. There was 90% stenosis of the LAD, 95% stenosis of the left circumflex artery, and a normal right coronary artery (Fig 2). In view of the LMCA aneurysm and double vessel CAD, the surgical option was considered. Intraoperative transesophageal echocardiography confirmed the presence of LMCA aneurysm (Fig 3A, 3B). Using cardiopulmonary bypass, the ascending aorta was opened and the LMCA aneurysm was oversewn and closed from its origin in the aortic sinus by 3-0 polypropylene pledgeted suture (Fig 3C). The proximal segment of the LAD was also aneurysmal, and it was ligated proximally and distally using pledgeted polypropylene suture (Fig 3D). The LAD and obtuse marginal artery were bypassed using vein grafts as conduits. The patients had an uneventful hospitalization and was discharged on the sixth postoperative day on dual antiplatelet therapy.
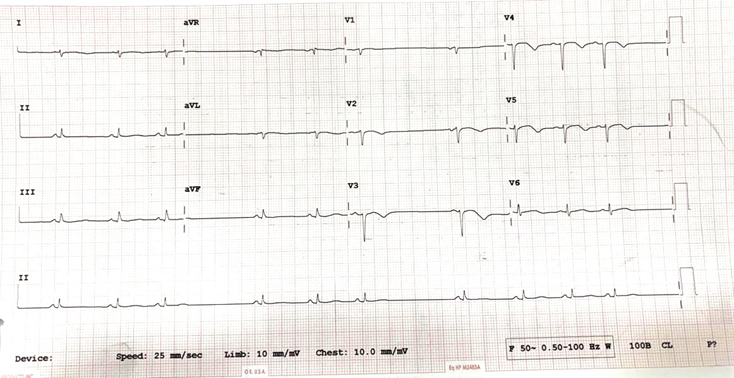
Figure 1: Electrocardiogram showing poor progression of ‘r’ waves in lead I and aVL, and q waves in lead V1-V5.
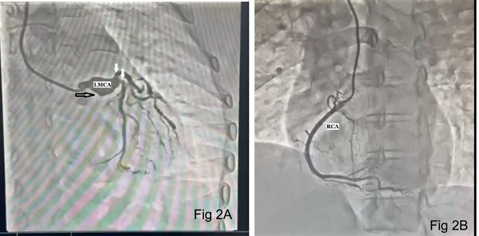
Figure 2: Coronary angiogram showing LMCA (left main coronary artery) aneurysm (black arrow) and stenoses of left anterior descending (LAD) and left circumflex artery (white arrows, Fig 2A). Normal right coronary artery (RCA, Fig 2B).
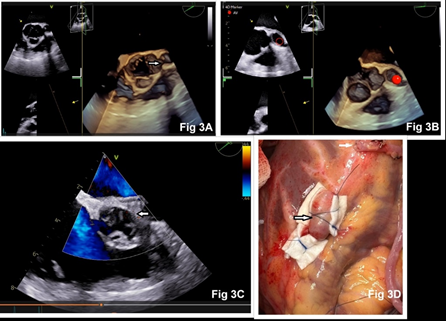
Figure 3: Intraoperative 3-D transesophageal echocardiography showing aneurysmal LMCA arising from the left aortic sinus (arrow and red circle 3A, 3B). Closed communication between aortic sinus and LMCA after its ligation (3C). Surgical photograph showing ligation of aneurysmal LAD artery (black arrow) and vein graft anastomosed to distal LAD (white arrow).
Discussion
Left main CAAs are the most uncommon coronary anomalies among all CAAs. The largest published series of LMCA aneurysm is that of Topaz and coworkers, who reported 22 cases among 20,332 adult patients (0.1%) undergoing coronary angiography.[2] CAAs are often classified by their macroscopic shape and size, according to the transversal and longitudinal size. Saccular aneurysms are spherical and show a transverse diameter greater than the longitudinal diameter, whereas fusiform aneurysms are characterized by a gradual and progressive dilatation that involves the complete circumference of the artery and have a transverse diameter that is smaller than the longitudinal diameter.[5] The clinical manifestations are similar to those seen in CAD, and the patients may have angina pectoris, dyspnea, pulmonary edema, myocardial infarction, and sudden death.
The etiology of CAA varies geographically. In Europe and North America, about 50% of cases are due to atherosclerosis, followed by congenital cases constituting 17%, and Kawasaki disease accounting for the last 10%. [6] In Japan and China, most cases are due to Kawasaki disease. Giant CAAs are thought to be due to congenital heart disease.[6] Iatrogenic CAAs can result from direct intimal injury during PCI with delay in healing due to antiproliferative coating, and/or stent malapposition. A failed PCI attempt could also have resulted in aneurysm formation in the patient described here. One of the procedural risk factors for iatrogenic CAA include chronic total occlusion and long lesions.[7] Atherosclerotic etiology is based on the complex interplay between tissue metalloproteinases (MMP) and the proteolysis of extracellular tissue proteins. Increased levels of the 5A allele of MMP3 and MMP9 serve as additional markers promoting this pathogenesis.
Diagnosis of CAAs may be aided by noninvasive tools, including echocardiography, computed tomography, and magnetic resonance imaging. Nevertheless, coronary angiography remains the gold standard for the evaluation of CAAs, assessment of coronary anatomy and pathology. Coronary angiography provides additional information regarding the size, shape, location, and number of the existing anomalies and shows an image of the coronary artery status, determining the extent and severity of the coronary lumen obstruction in CAD. CAAs are most often incidentally found on coronary computed tomography angiography (CTA) or during catheterization, as most patients are asymptomatic.[8] Coronary angiography paired with intravascular ultrasound (IVUS) provides a better understanding of vessel wall structure. Although optical coherence tomography (OCT) offers greater axial resolution compared to IVUS, penetrating depth is lower. OCT is of limited benefit in assessment of large CAA.[9] Coronary CTA offers advantages due to more accurate assessment of the aneurysm size and degree of thrombus verses invasive angiography. Patients with concomitant CAD can present with stable angina and/or acute coronary syndrome. CAA predisposes patients to thrombus formation and distal embolization, often resulting in acute coronary syndrome, myocardial ischemia, and heart failure.
Treatment of CAA consists of medical management, PCI, and surgical intervention; however, the appropriate treatment for CAAs is controversial and depends on the particular clinical situation. The medical therapy generally consists of attempts to prevent thromboembolic complications in patients with aneurysmal arteries who are at increased thrombotic risk through the administration of antiplatelet and anticoagulant medications. Recently, percutaneous application of polytetrafluoroethylene (PTFE) covered stents has gained popularity due their ability to effectively limit the expansion of CAAs by reducing the blood flow within the aneurysm, thereby preventing their rupture. PTFE-covered stents are preferred in patients with saccular aneurysms, pseudoaneurysms, and aneurysms smaller than 10 mm in diameter.[10] Percutaneous strategies also include coil embolization, autologous saphenous vein covered stent grafting, and drug-eluting stent implantation superimposed on a PTFE-covered stent graft. Holvoet at al have described the successful percutaneous IVUS-guided treatment of a giant LMCA aneurysm with a papyrus-covered stent with an excellent 1-year angiographic follow-up showing no residual filling of the aneurysm and no in-stent restenosis. [11]
Surgical option is commonly chosen when there is associated fistula formation, compression of the adjacent structures, multivessel involvement, a giant (>20 mm) aneurysm, LMCA aneurysm, or need for concomitant cardiac surgery. [8] Surgical strategies that have been described include aneurysm ligation, aneurysm repair, resection, marsupialization with interposition graft, and CABG.[9] The preferred approach for surgical correction of LMCA aneurysm entails proximal and distal end ligation of the aneurysm with bypass of the LAD and left circumflex artery by means of the left internal mammary artery and/or saphenous vein. A significant limitation of LM ligation is subsequent loss of percutaneous coronary access to treat CAD. Patch repair of the LM aneurysm enables future access of the coronary tree.[9] Some case studies reported temporary transection of the main pulmonary artery to access the aneurysm. [12] Extensive dissection between the aorta and pulmonary artery may be necessary. Doronila et al have described the reconstruction of a LMCA aneurysm using a radial artery patch. [13] They have suggested that resection with patch-graft reconstruction maintains native coronary flow with good long-term graft patency. In the absence of obstructive CAD, and in patients with suitable anatomy, patch-graft reconstruction may be a preferred option.
Conclusion
CAAs are an uncommon and often accidental finding. CAAs are usually associated with atherosclerosis in adults. Angiography is the gold standard for diagnosis. Treatment strategies (medical therapy, PCI, or surgery) should be based on the clinical presentation, location and morphology of the aneurysm, extension of aneurysm, side branch involvement, calcification, comorbidity, and patients’ preference. As there is no standard guideline or protocol to treat the CAA of the LMCA, individual patient evaluation and discussion is mandatory.
References
- Nunez-Gil IJ, Terol B, Feltes G, et al (2018). Coronary aneurysms in the acute patient: incidence, characterization and long-term management results. Cardiovasc Revasc Med 19 (5): 589–596.
View at Publisher | View at Google Scholar - Topaz O, DiSciascio G, Cowley MJ, et al (1991). Vetrovec GW. Angiographic features of left main coronary artery aneurysms. Am J Cardiol 67 (13):1139-1142.
View at Publisher | View at Google Scholar - Robinson FC (1985). Aneurysms of the coronary arteries. Am Heart J 109 (1):129-135.
View at Publisher | View at Google Scholar - Doustkami H, Maleki N, Tavosi Z (2016). Left Main Coronary Artery Aneurysm. J Teh Univ Heart Ctr 11(1): 41-45.
View at Publisher | View at Google Scholar - Befeler B, Aranda JM, Embi A, et al (1977). Coronary artery aneurysms. Study of their etiology, clinical course and effect on left ventricular function and prognosis. Am J Med 62(4), 597–607.
View at Publisher | View at Google Scholar - Li D, Wu Q, Sun L, et al (2005). Surgical treatment of giant coronary artery aneurysm. J Thorac Cardiovasc Surg 130 (3): 817-821.
View at Publisher | View at Google Scholar - Ipek G, Gungor B, Karatas MB, et al (2016). Risk factors and outcomes in patients with ectatic infarct-related artery who underwent primary percutaneous coronary intervention after ST elevated myocardial infarction. Catheter Cardiovasc Interv 88 (5): 748-753.
View at Publisher | View at Google Scholar - Kawsara A, Núñez Gil IJ, Alqahtani F, et al (2018). Management of coronary artery aneurysms. JACC Cardiovasc Interv 11 (13): 1211–1223.
View at Publisher | View at Google Scholar - Latyshev YA, Avendano JP, Patankar S (2023). Left main coronary artery aneurysm with rare quadfurcation anatomy. J Med Cases 2023 14 (2): 76-79.
View at Publisher | View at Google Scholar - Cohen P, O’Gara PT (2008). Coronary artery aneurysms: a review of the natural history, pathophysiology, and management. Cardiol Rev 16 (6): 301-304.
View at Publisher | View at Google Scholar - Holvoet W, van den Buijs D, Bogaerts E, et al (2022). Giant coronary artery aneurysm of the left main treated with a covered stent: a case report. Eur Heart J Case 7(1): ytac463.
View at Publisher | View at Google Scholar - Nakamura K, Orii K, Abe T, Haida H (2020). Successful sparing approach between the ascending aorta and the main pulmonary artery to the giant coronary aneurysm of the left main coronary artery. BMJ Case Reports 13 (4): e234203.
View at Publisher | View at Google Scholar - Doronila H, Kypson A, Landvater L, Anderson C (2024). Reconstruction of a left main coronary artery aneurysm using a radial artery patch. Journal of Surgical Case Reports 6: rjae423.
View at Publisher | View at Google Scholar
