

Case Report | DOI: https://doi.org/10.31579/2835-785X/102
Valve-in-Valve Leaflet Dysfunction After TMVR: The Problem and the Panacea
1 Senior Consultant, Department of Cardiac Anaesthesia, Medanta-The Medicity, Gurugram (Haryana)-122001, India.
2 Senior Director, Department of Cardiac Anaesthesia, Medanta-The Medicity, Gurugram (Haryana)-122001, India.
3 Associate Consultant, Department of Cardiac Anaesthesia, Medanta-The Medicity, Gurugram (Haryana)-122001, India.
*Corresponding Author: Dr. Ajmer Singh, Senior Director, Department of Cardiac Anaesthesia, Medanta-The Medicity, Gurugram (Haryana)-122001, India.
Citation: Dr. Ravi Mahavar, Dr. Ajmer Singh, and Dr. Ravina Mukati, (2025), Valve-in-Valve Leaflet Dysfunction After TMVR: The Problem and the Panacea, International Journal of Clinical Research and Reports. 4(6); DOI: 10.31579/2835-785X/102
Copyright: © 2025, Dr. Ajmer Singh. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 September 2025 | Accepted: 20 October 2025 | Published: 03 November 2025
Keywords: Transcatheter mitral valve replacement; valve-in-valve procedure; leaflet dysfunction
Abstract
Bioprosthetic valves are increasingly being used to treat valvular heart disease because they eliminate the need for lifelong anticoagulant therapy. Considering the limited durability of bioprosthetic valves, these patients need a repair or replacement of the prostheses by redo open- heart surgery in the future. Repeat cardiac surgery, however, involves significant morbidity and mortality. With the rapid evolution of transcatheter heart valve therapy, this alternative modality of implanting a valve within a failed tissue valve by a transcatheter technique has been established. The transcatheter valve-in-valve therapy, in addition to procedural challenges, can have adverse clinical outcomes, as described in this case report. The patient developed bioprosthetic valve leaflet dysfunction after transcatheter mitral valve-in-valve replacement and required another transcatheter intervention, leading to a successful outcome.
Introduction
Increasing use of bioprosthetic valves, combined with their shorter durability and the increasing life expectancy of an aging population, can translate into a major increase in the incidence of patients with surgical valve failure in the near future.[1] The standard of care for a degenerated bioprosthesis involves a redo open-heart surgery, which may be associated with significant morbidity and mortality. Transcatheter valve replacement is now established as the preferred treatment option and a valid alternative for inoperable or high-risk patients with severe symptomatic valvular heart disease.[2] With the rapid advances in the transcatheter valve technology, the successful placement of new valves within a degenerated prosthesis via a transcatheter approach, called a valve-in-valve procedure, has been established.
Bioprosthetic valves are prone to undergo structural dysfunction and failure due to progressive tissue degeneration. The structural dysfunction can result from cusp calcification or progressive collagen deterioration. This mineralization process may produce valvular stenosis via cusp stiffening and may also precipitate regurgitation due to secondary tears or paravalvular leak.[1] Treatment of bioprosthetic heart valves to enhance their durability can also lead to collagen fiber disruption under the stress of repeated leaflet bending. When the valve leaflets are subjected to compressive forces (like when they are forced to bend in a restricted manner), they can ‘buckle’, leading to a localized deformation or wrinkling of the tissue. This buckling can lead to incomplete opening of the valve, high transvalvular gradient, and clinical features of heart failure. In this case report, we describe the leaflet dysfunction caused by buckling that occurred after a transcatheter mitral valve replacement. The problem was solved via another transcatheter interventional procedure.
Case Report
A 52-year-old female was admitted with complaints of worsening dyspnea (New York Heart Association class III-IV) and palpitations. She underwent closed mitral valvotomy in 1997 for rheumatic mitral stenosis, followed by mitral valve replacement and aortic valve replacement with bioprosthetic valves in 2012. Transthoracic echocardiography (TTE) revealed a thickened and fibrosed bioprosthetic heart valve (BHV) at the mitral position with restricted mitral valve opening, causing severe mitral stenosis (MS) and moderate mitral regurgitation (Fig. 1A, 1B). The transvalvular gradients across the mitral valve were 41/19 mmHg (peak/mean). The BHV at the aortic position was functioning normally with no significant gradient across the valve and mild aortic regurgitation. There was severe tricuspid regurgitation, and the estimated pulmonary artery systolic pressure was 80 mmHg. The left ventricular function was normal, while there was moderate right ventricular systolic dysfunction.
The estimated EuroSCORE II for a redo-valve surgery was high (10.01%). The ‘Heart-team’ suggested transcatheter mitral valve-in-valve replacement (TMViVR), and the patient’s informed consent was obtained. TMViVR was performed in a hybrid operating room under general anesthesia with all standard cardiac monitoring, including 3-D transesophageal echocardiography (TEE). A balloon-expandable 23 mm MyvalTM transcatheter mitral valve (Meril Life Sciences Pvt. Ltd., Vapi, Gujarat, India) was deployed by trans-septal puncture through the femoral route uneventfully (Fig. 1C, 1D, 1E). Anticoagulation therapy was commenced with intravenous unfractionated heparin followed by oral warfarin. On the third day of the procedure, the patient developed acute heart failure with severe breathlessness requiring intubation and mechanical ventilation. Soon, the patient developed cardiogenic shock requiring high-dose inotropes and vasopressors. A repeat TEE evaluation revealed buckling of the TMViV leaflets, leading to incomplete opening of the valve, causing severe MS with transvalvular gradient of 28.1/20.1 mmHg (peak/mean, Fig 2A, 2B). The patient was again wheeled into the operating room and balloon re-expansion of the TMViV was performed (Fig 2C). The hemodynamic parameters improved immediately with the reductions in transvalvular pressure gradient and inotropic/vasopressor support (Fig. 2D). Further course of the patient in the hospital was unremarkable. At one week, before discharge from the hospital, TTE showed normal functioning of the TMViV with a mean gradient of 6 mmHg, mild tricuspid regurgitation, and pulmonary artery systolic pressure of 36 mmHg (Fig. 2E). At a 3-month follow-up, the patient showed marked improvement in her symptoms and normal echocardiogram findings.
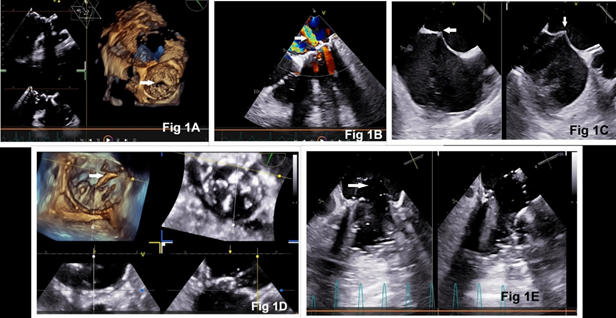
Figure 1: Transesophageal echocardiography 3-D en-face view of the mitral valve showing degenerated bioprosthesis with restricted opening (Fig 1A) and moderate mitral regurgitation (Fig 1B). Steps of transcatheter mitral valve replacement: trans-septal puncture (Fig 1C), insertion of Agilis sheath into the left atrium (Fig 1D), and valve deployment (Fig 1E).
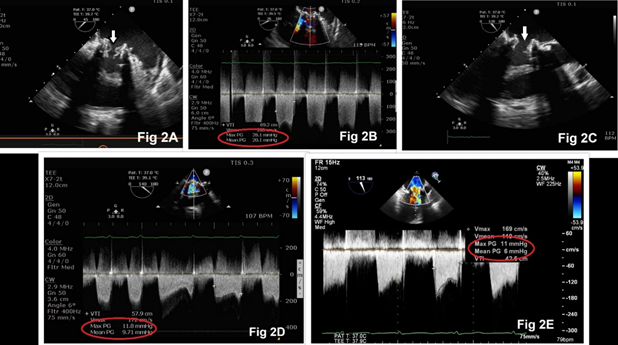
Figure 2: Transesophageal echocardiography demonstrating buckling of the mitral valve with high transvalvular gradient (Fig 2A, 2B). Re-expansion of mitral valve resulted in adequate mitral valve opening (Fig 2C) with reduction in valve gradient (Fig 2D, 2E).
Discussion
Treatment of patients with failing bioprosthetic mitral valves is challenging. While surgery is considered the standard of care, redo surgery carries significant morbidity and mortality risk compared with primary valve replacement. Transcatheter mitral valve-in-valve replacement (TMViVR) has emerged as a minimally invasive alternative, particularly for high-risk patients who may not be ideal candidates for repeat open-heart surgery. The data from the STS/ACC TVT Registry (Society of Thoracic Surgeons-American College of Cardiology Transcatheter Valve Therapy Registry) reinforce the feasibility and favorable short-term (30-day and 1-year) outcomes associated with TMViVR for the treatment of bioprosthetic MVR structural degeneration.[3]
The leaflet dysfunction of a bioprosthetic valve can occur either because of (i) thrombosis caused by inadequate anticoagulation, or (ii) incomplete expansion of the valve during deployment, or (iii) structural deformity of the valve. It is reported that there occurs a >50% increase in Doppler mean gradient from baseline within 5 years after bioprosthetic valve implantation.[4] It can be caused by increased cusp thickness, abnormal cusp mobility, subtherapeutic international normalized ratio, and paroxysmal atrial fibrillation. All foreign bodies, including prosthetic valves, are thrombogenic, potentially implying the need for short- or long-term anticoagulation to prevent thrombosis.
Reduced leaflet motion after a surgical or transcatheter valve replacement is less prevalent among patients receiving therapeutic anticoagulation than among those receiving subtherapeutic or no anticoagulation.[5] Transthoracic echocardiography may rule out valve stenosis or incompetence, but it has limited usefulness in the detection of the subclinical form of reduced leaflet motion, due to inadequate visualization within the valve stent frame and normal transvalvular gradients. Normalization of leaflet motion with anticoagulation suggests that thrombus formation is the primary event leading to reduced leaflet motion rather than reduced leaflet motion leading to the formation of an overlying thrombus. Furthermore, leaflet thrombosis may be associated with overall and regional under-expansion of the transcatheter valve. Previous studies also suggested that alterations in the degree of stent expansion lead to distorted leaflet coaptation, which affects valve hemodynamics, puts the patients at higher risk of patient–prosthesis mismatch, and over time can negatively influence long-term valve durability. [5,6]
Buckling is defined as a sudden change in shape (deformation/distortion) caused by excessive load or pressure. In bioprosthetic valves, tissue buckling occurs when collagen fibers are disrupted from cyclic leaflet bending, causing the leaflets to buckle under compressive stress. This buckling is observed as compressive deformation in valve leaflets, especially under conditions where the leaflets are restricted in their motion, like after fixation and during implantation. BHVs, made from animal tissue, are treated to enhance their durability. However, this treatment can also lead to collagen fiber disruption under the stress of repeated leaflet bending. When the valve leaflets are subjected to compressive forces (like when they are forced to bend in a restricted manner), they can buckle, leading to a localized deformation or wrinkling of the tissue. Another mechanism of buckling is the process of fixing the valve tissue (e.g., with glutaraldehyde), which can alter the tissue's mechanical properties, potentially making it more susceptible to deformation or distortion. The presence and stability of glycosaminoglycans (GAGs), the molecules present in the valve tissue, are also thought to influence buckling. GAGs help maintain tissue hydration and influence mechanical properties. Loss of GAGs can potentially contribute to buckling-related failure. Buckling, along with other factors like calcification, is a recognized mechanism of bioprosthetic valve failure. Results of an animal study have demonstrated that neomycin followed by ethanol treatment effectively preserves GAGs both in vitro as well as in vivo after subdermal implantation in rats. [7] Neomycin fixation followed by ethanol treatment of BHVs could prevent failure of bioprosthetic valves, thereby increasing the effective durability and lifetime of these bioprostheses several-fold.
It has been observed that fresh tissue and glutaraldehyde-treated tissue responded differently to bending.[8] Glutaraldehyde-treated tissue always buckles more than fresh tissue. In addition, when the direction of bending is compared, leaflet tissue always buckles more during reverse bending. The compressive buckling observed during prosthetic tissue bending may be an important factor in bioprosthetic valve failure. It appears, therefore, that normal leaflets are unlikely to buckle at all during normal valve function because reverse curvatures do not usually occur, and normal bending does not lead to buckling. Since buckling of bioprosthetic tissue results mainly from reverse curvatures, it seems advisable that these deformations be kept to a minimum. So, the greatest factor responsible for reverse curvatures and resultant buckling is the design of the supporting valve stent.
The treatment approach for a buckled valve will be determined by (i) the type of valve: (mechanical or bioprosthetic), (ii) the presence of a thrombus, (iii) the cause of the buckling: (delivery system or structural valve damage), and (iv) the patient's overall clinical condition: and suitability for surgery or other interventions. If the buckled valve is a mechanical prosthetic valve with a thrombus, thrombolysis may be recommended for right-sided valves or smaller left-sided valve thrombi (< 0>
Conclusion
In conclusion, patients may experience symptoms related to valve dysfunction, such as heart failure, shortness of breath, or even sudden death in severe cases of valve-in-valve dysfunction caused by buckling. Regular monitoring of prosthetic valve function using echocardiography is therefore crucial to detect potential issues like buckling or other signs of valve failure.
References
- Paradis JM, Del Trigo M, Puri R, Rodés-Cabau J (2015). Transcatheter valve-in-valve and valve-in-ring for treating aortic and mitral surgical prosthetic dysfunction. J Am Coll Cardiol 66 (18): 2019-2037.
View at Publisher | View at Google Scholar - Barnett SD, Ad N (2009). Surgery for aortic and mitral valve disease in the United States: A trend of change in surgical practice between 1998 and 2005. J Thorac Cardiovasc Surg 137 (6):1422–1429.
View at Publisher | View at Google Scholar - Whisenant B, Kapadia SR, Eleid MF, et al (2020). One-year outcomes of mitral valve-in-valve using the SAPIEN 3 transcatheter heart valve. JAMA Cardiol 5(11):1245-1252.
View at Publisher | View at Google Scholar - Makkar RR, Fontana G, Jilaihawi H, et al (2015). Possible subclinical leaflet thrombosis in bioprosthetic aortic valves. N Engl J Med 373 (21): 2015-2024.
View at Publisher | View at Google Scholar - Fuchs A, De OB, Brooks M, et al (2017). Subclinical leaflet thickening and stent frame geometry in self-expanding transcatheter heart valves. EuroIntervention 13 (9): e1067–1075.
View at Publisher | View at Google Scholar - Khodaee F, Barakat M, Abbasi M, et al (2020). Incomplete expansion of transcatheter aortic valves is associated with propensity for valve thrombosis. Interact CardioVasc Thorac Surg 30:39–46.
View at Publisher | View at Google Scholar - Raghavan D, Shah SR, Vyavahare NR. (2010) Neomycin fixation followed by ethanol pretreatment leads to reduced buckling and inhibition of calcification in bioprosthetic valves. Biomaterials 29:1645–1653.
View at Publisher | View at Google Scholar - Vesely I, Boughner D, Song T (1988). Tissue buckling as a mechanism of bioprosthetic valve failure. Ann Thorac Surg 46 (3): 302-308.
View at Publisher | View at Google Scholar
