

Research Article | DOI: https://doi.org/10.31579/2834-5029/023
The Interface Between Abortion Practice and Community Response in Amhara Region, North Eastern Ethiopia, 2017: A Cross-Sectional Study
- Antehunegn Birhanu *
Department of Sociology, Injibara University, Injibara, Ethiopia.
*Corresponding Author: Antehunegn Birhanu, Department of Sociology, Injibara University, Injibara, Ethiopia.
Citation: Birhanu A., (2023), The Interface Between Abortion Practice and Community Response in Amhara Region, North Eastern Ethiopia, 2017: A Cross-Sectional Study, International Journal of Biomed Research. 2(4); DOI:10.31579/2834-5029/023
Copyright: © 2023, Antehunegn Birhanu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 May 2023 | Accepted: 26 June 2023 | Published: 03 July 2023
Keywords: abortion, lived experience, sociocultural discourse, community attitude, agency structure
Abstract
Background: The issue of abortion is as old as human existence. People have used it as a fertility control from the distant past to the present. It is a universal and global phenomenon that existing competing sociocultural discourses can influence. These discourses, in turn, have profoundly affected women's abortion experiences (reason, intentions, and decision-making process) and on the negative attitude of the community towards abortion, particularly in patriarchal societies.
Objective: To examine the interface between the lived experience of women and the community's attitudes towards abortion in Woldia Town, North Wollo Zone of Amhara Region, Ethiopia, in 2017.
Materials and Methods: This study employed a mixed approach: quantitative (household survey) and qualitative (focus group discussions, in-depth interviews with key informants, and case studies) to collect relevant data. Descriptive and inferential statistics were used to analyze the quantitative data. The qualitative data were analyzed thematically and presented together with the quantitative.
Result: Numerous contextual and structural level factors hampered the practice of safe abortion in general, the lived experience of women who had induced abortions and the larger community's attitude towards abortion in particular. The constraining nature of such factors was more visible in abortion practice than in their enabling influence on the lives of women who performed an induced abortion.
Conclusion: This study claims that structural factors (religion, morality, medico-legal discourses, and gender roles) influenced the smooth functioning of safe abortion, women's reproductive rights and lived experiences on the one hand, and the community's attitude towards abortion on the other. As a result, the abortion experience of women is the result of both agency and structural level factors. Similarly, the community's negative attitude towards abortion stigmatized women in practicing induced abortion. This study's findings proposed policy implications at the agency and structural levels in addressing the prevailing problems associated with societal stigma, health complications, and psychological distress of women practicing abortion.
Introduction
Throughout the dawn of human history, abortion has been a common practice [1]. In the past, abortion was the most popular means of regulating fertility and eliminating unintended pregnancies [2]. In contrast to time-honored traditions, modern society associate induced abortion with an unintended pregnancy. Due to social, cultural, economic, and health concerns, most people in contemporary societies delay having children [3].
Abortion is one of the most contentious topics whiles being a widespread practice throughout time and place to varying degrees. Several cultures reject abortion. Those who practice it at the intersection of societal attitudes, stigma, and the private sphere of pregnancy and reproductive rights experience this profoundly [5, 6].
A variety of religious, moral, legal, and medical discourses have had an impact on the practice of inducing abortion. These contextual factors have an impact on women's lived experiences, such as their decision to have an abortion, the stigma associated with it, their psychological distress, the meaning that is attached to abortion, and public perceptions of the practice in a broader sociocultural context [7]. In spite of these realities, the general public has a little grasp of how they affect women's lives in complex and varied ways [8].
Around the globe, induced abortion has been the subject of several investigations. For example, research has been done in Argentina on women's experiences with medical abortion [9], in Zambia on women's knowledge and views on abortion legalization and access to services [10], and in Ghana on women's attitudes and experiences [11]. Yet, these studies only paid attention to one group of people—primarily women—while ignoring males' perspectives on abortion and the effects of sociocultural discourses on women's lived experiences in particular and community responses in general.
Most previous studies in Ethiopia uncovered women’s attitudes towards abortion practices from the public health perspective and epidemiological dimensions mainly focused on the prevalence and associated risk factors. Several studies were conducted in Ethiopia on the determinants of abortion practice, for instance, [12, 13] in Addis Ababa. However, these studies discussed determinants like cost, time, accessibility, and providers’ perception of providing safe abortion services. Other studies focused on the legalization of abortion. For example, a study conducted [14] in the Tigray region focused on the attitude of women and men toward the legalization of abortion. Similarly, others focused on the attitude of female university students toward the legalization of safe abortion [15, 16]. Still, others focused on psychological aspects of abortion, for example, a study conducted on women's emotional experiences of induced abortion in Addis Ababa [17]. However, some of the studies mentioned above were carried out from the public health perspective and failed to address the interface between the lived experience of women practicing abortion and attitudes of the community towards abortion in a sociocultural context where how abortion affects society's norms, values, and beliefs and vice versa. As a result, the present study seeks to explore women's lived experiences such as negotiating strategies on the decision of abortion, meaning attributed to induced abortion, psychological distress, and resilience mechanisms within the existing sociocultural context on the one hand and attitudes of the community towards abortion on the other. So, studying abortion dialectically will improve our understanding of the complex factors that encourage or discourage safe abortion procedures and women's reproductive rights in the conflicting discourses ingrained in the community. Understanding this link between women's agency and society would also help minimize the stigma, health risks, and psychological harm of abortion.
To examine how normative structures and sociocultural discourses affect women's lived experiences who have had induced abortions, this study used agency structure theory. According to Giddens [18], this theory describes the dialectical interaction between agency and structure, which neither can exist without the other. In this sense, this theory proposes a hallmark to identify contextual/structural, as well as individual level, elements that enable and restrict the practice of abortion.
Materials and Methods:
Study area:
The study was conducted in Woldia town of North Wollo zone in Ethiopia. It is found 521 km away from Addis Ababa to the North East. The study town was expected to have a total population of 68,352 people, of which 35,154 were men and 33,198 were women, according to the forecast made by [20]. Due to the author's exposure to and familiarity with the area and the anticipated ease of accessing informants, the area was purposefully chosen.
Study Design:
The study was conducted from February 28, 2017, to April 7, 2017, and a cross-sectional study design was used. The household survey, FGDs, key informants, in-depth interviews, and case studies were carried out. The survey aimed to learn how much the community knew about the many types of abortion, their causes, their effects, their legal restrictions, the setting in which they occur, and their opinions towards abortion.
To gather survey data, a questionnaire that an interviewer administered was used. Four Likert scales were included in the questionnaire, one of which measured the opinions of the head of households regarding abortion. The other three measures were used to predict these effects on abortion practice and were related to stigma, medico-legal, moral, and religious discourses. Ten Likert scores on the scale, ranging from strongly agree to disagree strongly, are available. Each respondent's responses to these questions were added up to produce an overall score, and the cutoff point for the respondents' total scores was established based on the neutral value, with scores below the neutral value denoting an unfavorable attitude and scores above the neutral representing a favorable attitude [19]. The author closely supervised the training of four research assistants who were hired and trained to conduct the survey. The author conducted interviews with health professionals, women who had undergone induced abortions, religious leaders, lawyers, and the elderly of the community after gathering all qualitative data with the aid of local guides and healthcare practitioners who served as gatekeepers. Three FGDs in total—two FGDs with eight participants each at the household level and one FGD with eight participants from youth groups in the chosen kebeles—were held independently to record the various viewpoints on the topic hand. Nine women who had induced abortions at health facilities participated in in-depth interviews to examine the issues surrounding abortion, negotiation strategies, psychological distress, and the community's reaction.
Study population, sampling and sample size:
Study participants comprised the urban head of households, health professionals, religious leaders and elderly of the community, lawyers and officers, at Woldia Town administration, women and children's office. Probability and nonprobability sampling strategies were used to select the respondents and informants. To choose research kebeles, a multistage sample technique (two-stage sampling) was used. As a result, in the first sampling stage, two kebeles were drawn randomly from a pool of seven kebeles. Households were selected in the second sampling stage using Yamane's sample size determination formula of at a 95% confidence interval for the total population of 1360 households for the two selected kebeles, yielding 310 sample sizes.
Then, 128 and 182 households were chosen using multiple proportions of each kebele (P) calculated using n/N *sample size. Finally, the heads of households were chosen from the given sample frame using the SPSS random sampling method. Finally, at the household level, heads of households were recruited for the study based on the definition of (20). Females replaced their counters due to the absence or unwillingness of the male head of household.
A purposive sampling technique was used to recruit qualitative research informants. As a result, nine women who had induced abortions, three health professionals, three religious’ leaders, four elderly, two health extension workers, two court lawyers, and two women's affairs office professionals were chosen as key informants based on their availability, willingness, and the assumption that they can better explain the issue at hand.
Data Analysis:
Quantitative data were entered into the SPSS version 20 software and analyzed using descriptive and inferential statistics between or among variables. As a result, descriptive statistics such as frequency, percentage, and mean were used to examine the practice of abortion. The study also used statistical tests such as ANOVA, T-Test, correlation, and regression to conclude the target population. Thematic analysis was used to transcribe, categorize, summarize, and present qualitative data from note-taking activities and audio recordings alongside quantitative data.
Theoretical Framework of the Study:
Giddens structuration theory, developed in 1984, was used in this study. According to the theory, structure, and human agency are two sides of the same coin in which all social actions involve structure and all structure involves social action. Women who had induced abortions influenced the moral and normative order of the community and the sociocultural values and beliefs embedded in society that influenced women's lived experiences, such as abortion decisions.
Ethical considerations:
Following receipt of a formal letter from Addis Ababa University's Department of Sociology, the author obtained oral consent from study participants to ensure the confidentiality of any information provided.
Results:
Socio-demographic Characteristics of Respondents:
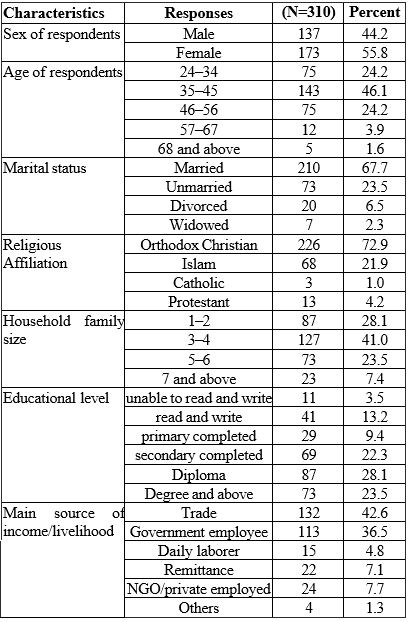
Table 1 shows males (44.2 percentage) and females (54.8 percentage) participated in the study. With a mean age of 41.33, most respondents (46.1 percentage) were between 35 and 45. Most respondents (67.7 percentage) were married, with the remaining unmarried (23.5 percentage). Orthodox Christians account for 72.9 percentage of religious affiliation, followed by Islam (21.9 percentage) and Protestantism and Catholicism (4.2 percentage and 1 percentage, respectively). Regarding household family size, the majority (41 percentage) were 3–4 members. Most respondents were educated, with 28.1 percentage holding a diploma, 23.5 percentage holding a degree or higher and 22.3 percentage having completed secondary school. Finally, most respondents' main source of income was trade, followed by government employment.
Abortion Knowledge and Awareness of Respondents:
Table 2 shows that the majority of respondents, 181 (58.4 percentage), were aware of safe abortion practices performed in healthcare centers, as opposed to unsafe abortion practices and spontaneous abortion, which accounted for 101 (32.6 percentage) and 28 (9 percentage) at the time of the survey, respectively. In terms of respondents' knowledge of women's institutional preferences for terminating pregnancy, the majority currently stated that most women preferred private clinics (50.8 percentage), NGOs (33.7 percentage), government hospitals (34 percentage, and government health posts (24.3 percentage). Nonetheless, 35.3 percentage of respondents said that a large number of women still used unsafe abortion methods to end their pregnancy. Respondents were asked why they had terminated their pregnancy. The findings revealed that 52.8 percentage of them believed women terminated their pregnancies due to fear of societal stigma/judgment. According to one of my FGD participants,
There is a strong community reaction against induced abortion. If a woman bears a child before wedlock and outside of marriage, she is labeled promiscuous. Furthermore, most women terminate their pregnancies for financial reasons. Consider how many babies were born and dumped in back streets (ditches) due to fear of societal reactions and economic reasons (FGD, Male).
While performing an induced abortion, 66 percentage and 54.5 percentage of respondents, respectively, believed women faced health-related risks and problems, including death. The remaining 27.1 percentage reported societal stigma, stereotypes, and labeling after having an induced abortion. A woman who had an induced abortion described the following societal reactions:
My neighbors and colleagues have said hurtful things to me. They referred me as being arrogant, a killer, and a murderer. I was always embarrassed, and I cried at times. Only God is aware of my situation. I work as a housemaid (domestic worker). Life is miserable and I may not be married because the community sees me badly (Unmarried, age 24).
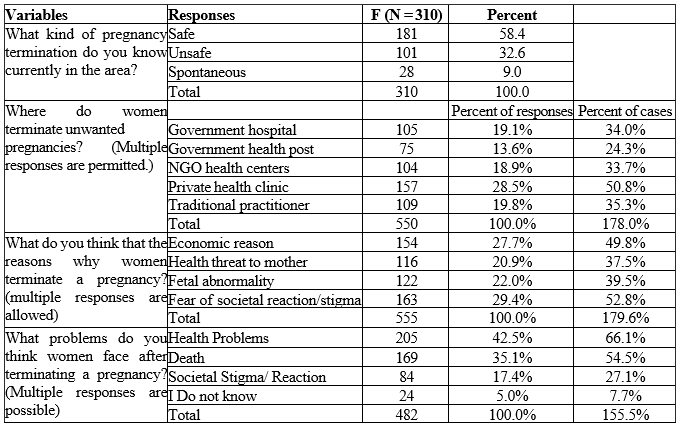
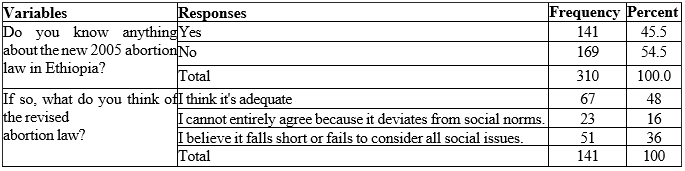
Table 3 shows that when respondents were explicitly asked whether they knew anything about Ethiopia's revised abortion law, only 141 (45.5 percentage) responded positively. To put it another way, more than half of the respondents (54.5 percentage) lacked any knowledge of the legality of abortion. The majority of FGD participants had no understanding what the abortion law was or what it said. Out of 141 people who claimed they were aware of the law, 67 (48 percentage) thought it was adequate, 23 (16 percentage) said it broke societal standards, and 51 (36 percentage) said it was insufficient or did not take into account all social considerations.
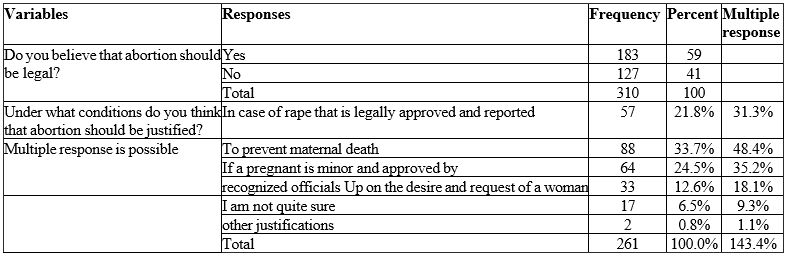
Table 4 shows that 183 respondents (59 percentage) thought that abortion should only be legalized in cases of preventing maternal death (48.4 percentage), rape that is officially reported (31.3 percentage), minor age when approved by recognized officials (35.2 percentage), and upon the wish and request of women (18.1 percentage).
Conversely, the majority of FGD discussants and some key informants, such as lawyers, advocated that abortion should be legalized and permitted upon the request of a woman who lives under commercial sex work, a woman with a poor economy, and other victims that are being clandestinely practiced and ultimately led to maternal mortality.
On the contrary, except Muslim and Christian religious leaders, who had fierce resistance towards the legalization of abortion, most FGD discussants and some key informants such as lawyers, recommended that abortion should be legalized and permitted upon the request of a women who live under commercial sex work, women with poor economy and other victims which are being clandestinely practiced and ultimately led to maternal mortality. For instance, a senior key informant described her viewpoint on abortion's legalization as follows:
I believe that abortion should be permitted as unsafe abortions can be performed at any time. For instance, there are circumstances outside rape and incest that force women to get abortions for financial, social, and psychological reasons. Legal abortion should be permitted right now because, without it, most women will be susceptible to various unwelcome life events, including mortality, health concerns, and societal discrimination (Female, age 68).
Contextual Factors and The Practice of Abortion:
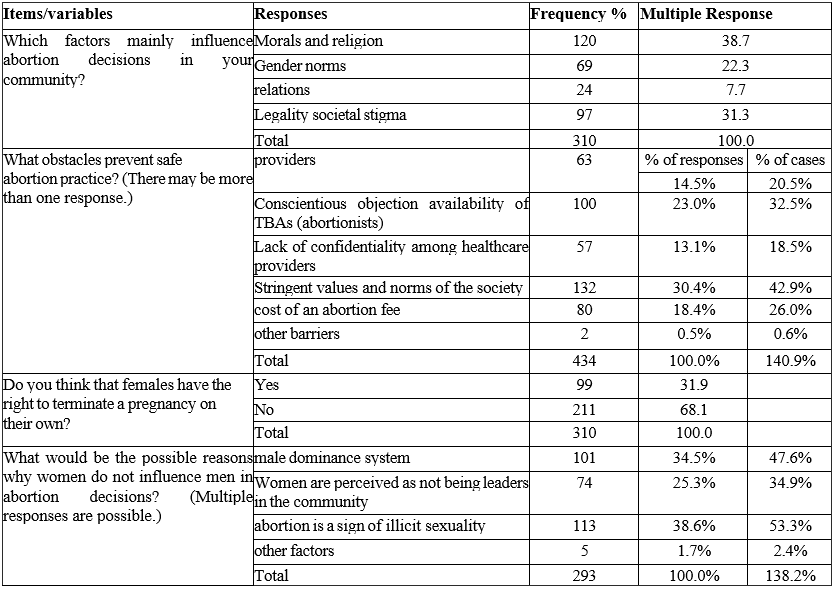
Results on contextual influences on abortion decisions revealed that 120 respondents (38.7 percentage) believed morality and religion influenced abortion decisions in the community. Roughly 97 (31.3 percentage) of the respondents cited social stigma and stereotypes, 69 (22.3 percentage) gender roles, and the final 24 (7.7 percentage) mentioned legality concerns. A 22 -year-old woman having induced an abortion narrated in an in-depth interview how her religion influenced on her abortion decision as follows:
When the pregnancy test returned positive, I got stressed between continuing and ending the pregnancy. Above all things, I was concerned about religion and the morality of killing a baby because I frequently attended church events that increased my anxiety; spiritual leaders often lectured us on the evil of killing an unborn child and the honor of celibacy. Also, having a child out of wedlock and having an abortion are social sins; this made me anxious since I could also become socially excluded and mistreated.
The results support Reardon (2003) and Kimport et al. (2011), who claim that choosing to have an abortion is not a simple process and requires several phases because the decision has an impact on the social, cultural, emotional, spiritual, physical, and even economic well-being of the woman.
Similarly, gender roles significantly impacted women's decisions to have abortions. In light of this, 211 respondents (68.1 percentage) indicated that women have no rights regarding abortion-related decisions and actions, whereas about 99 respondents (31.9 percentage) agreed.
The reason women could not influence men in performing induced abortions was because 113 (53.3 percentage) believed abortion was a sign of illicit sexuality (pregnancy outside of marriage) by women, followed by 101 (47.5 percentage) in the male dominance system (men's power to decide over women). The remaining 74 (34.9 percentage) and 5 (2.4 percentage) thought that women are perceived as not being leaders in the community and other factors, respectively. One of the key informants who worked in the North Wollo Zone's office for women and children provided the following explanation:
Gender roles and gender relations are manifestations of larger societal trends. Yet, masculine dominance is still evident. Particularly in married couples, men predominate over women in many areas, including the decision to have an abortion. Women are inferior to men; thus, they feel ashamed of influencing them when making abortion decisions. Due of their lower voice than men, women typically bear the brunt of this responsibility (male, age 38).
Several limiting factors affected safe abortion practices. 100 (32.5 percentage) of the respondents mentioned the covert nature of unsafe abortion practices, 132 (42.9 percentage) strict societal values and norms that stigmatize and discriminate against women who have had induced abortions, 80 (26.2 percentage) the price of abortions, 63 (20.5 percentage) doctors' conscientious objections (an incompatibility of medical professionals' moral, religious, and ethical perspectives), and 57 (18.5 percentage) problems with healthcare providers' confidentiality to their clients' private information.
Experience of the Community with Abortion Practice:
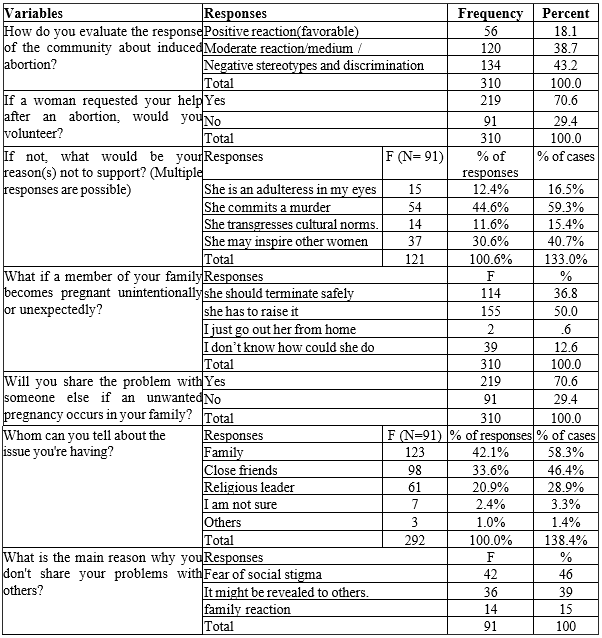
Respondents were asked about the community's response to induced abortion. Accordingly, 56 (18.1 percentage) respondents anticipated that the community had favorable responses, 120 (38.7 percentage) said moderate or medium reactions and 134 (43.2 percentage) said unfavorable reactions towards abortion. During an in-depth interview, a 34-year-old woman having an induced abortion also strengthened the adverse reaction of the community as follows: "I have faced negative reactions from my neighbors. They labeled me as 'shermuta’ [a promiscuous and immoral woman], and they do not respect me as the previous one, and now I got divorced".
About their willingness to offer social assistance following a woman's induced abortion, respondents were posed a straightforward question. As a result, 219 people (70.6 percentage) said they would be willing to assist a woman with an abortion. In comparison, 91 people (29.5 percentage) said they would not be because they think the woman is an adulterer (16.5 percentage), a murderer (54.3 percentage), a transgressor of cultural norms (15.4 percentage), and a motivator of others to do the same (40.7 percentage). One percent (1.1 percentage) of respondents cited additional factors. Nonetheless, respondents were questioned about what might be done if an unintended pregnancy happened to a family member.
Consequently, 155 respondents (50 percentage) said they would decide to have a child, 114 (36.6 percentage) would safely get an abortion, 39 (12.6 percentage) were unsure what to do, and 2 (0.6 percentage) would be kicked out of the family if they had an abortion. The respondents were also asked if they would talk to someone else about the issue of an unintended pregnancy and their abortion experience. According to the responses, 219 respondents (or 70.6 percentage) said they would share if they encountered the situation. Of these, 123 respondents (58.3 percentage) said they would share with their family, 98 respondents (46.4 percentage) said they would share with their peers or closest friends, 61 respondents (28.7 percentage) said they would share with their religious leaders, and three respondents (1.4 percentage) said they would share with others. The remaining 91 respondents (or 29.4 percentage) said they would not be willing to share. For instance, during the in-depth interview, a woman who had undergone an induced abortion narrated her experience of telling others as follows:
While I was working as a housemaid, I was raped by someone and got pregnant. I did not have any information about how and where to terminate. I do not want to tell the case to someone else either. Later, I went to my parents and told my mother. My mother then directed someone else to go get money. Then, we went to a private clinic and paid 1500 Birr. The pregnancy lasted for five months. It was very painful. Now everybody insults me; no one gives me any respect. Had I not been poor and found it challenging to get money, I would not have disclosed the case to others. Now I am stigmatized by those who know my history (uneducated, unmarried, age 24).
The Effect of Sociocultural Discourses on Attitudes of Abortion Practices:
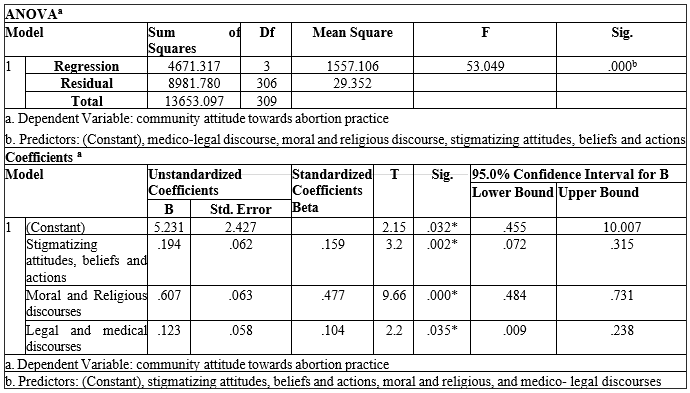
Multiple regression analysis revealed that stigmatizing attitudes, beliefs, and behaviors, moral and religious discourse, and medico-legal discourse were all statistically significant at p 0.05. In contrast, stigmatizing attitudes, beliefs, and behaviors were significant at p = .032, moral and religious discourse at p = 0.000, and medico-legal discourse at p = 0.035.
Furthermore, the F ratio in an ANOVA in Table 7 reveals that the independent factors statistically significantly predict the dependent variable (F 3, 306 = 53.049, p less than 0.5, R2 = .342). Hence, it was observed that the aforementioned discourses were significant factors that influence respondents' attitudes towards abortion practice and had a cumulative effect of 34.2 percentage on it.
One professional in the Women and Children's Office explained its impact upon the lives of women and the attitude of the community towards abortion as follows:
Both pregnancy and abortion can happen in any situation. This is because community beliefs, discourses, and expressions as well as existing sociocultural institutions impact how communities see abortion and how women are allowed to exercise their reproductive rights. Abortion is condemned by spiritual leaders and their followers as being, among other things, an unacceptable, immoral, and sinful act that violates God's law. People's opinions on abortion practices were actually influenced by gender norms (male dominance), cultural stigma, social exclusion, bad language, and other factors. Also, a major obstacle to performing abortions is the doctors' hesitation and lack of secrecy (male key informant, age 38).
Public Attitude and Abortion Practices:
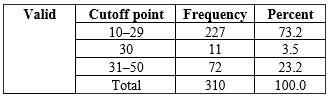
About 227 (73.2 percentage) of the respondents reported that they had unfavorable attitudes towards abortion practice, while 11 (3.5 percentage) and 72 (23.2 percentage) had neutral and favorable attitudes towards it, respectively.
Women’s Negotiating Strategies in Performing Induced Abortion:
During the in-depth interview, women who experienced induced abortion, identified strategies such as confessing to spiritual father, silence, perceived risks and benefits, and a world view (openly discussing the issue, considering abortion as normal) as the main negotiating strategies in their abortion decision and practice within the existing discourses by most women. A 19-year-old woman described her experience in the following way:
When I had an unintended pregnancy, I struggled with the decision to end it because I feared the stigma from my family, religion, and society. In our community, giving birth outside of marriage exposes one to moral and psychological crisis and public disgrace. In addition, I fear that God will punish me by forbidding me to have any more children. But, having children will complicate my life, and I want to finish my degree. I decided to stop and tell my mother the story at that point. In addition, I felt that I ought to apologize to my devout father.
On the contrary, unlike social factors external to the individual, personal factors also play a greater role in abortion decisions. Hence, some view abortion as a relief, so they could easily decide to perform it despite external factors. A 22 -year-old and married woman, who participated in an in-depth interview, narrated her experience in an abortion decision as follows:
Although to some extent my religion influenced my decision not to perform an abortion, to me it was easy to decide because I knew that the problem, I would face otherwise was difficult. I am a high school student; I married when I was 19; and I have one child. I got pregnant immediately after my first baby. My husband works for a private organization, but his salary is not enough to raise our children, so I should decide on the future lives and living conditions. However, after performing an abortion, I got depressed and felt guilty.
Lived Experience of Women Practicing Induced Abortion: Before, During, And After:
Women who practiced abortion encountered various difficulties, including remorse, fear of losing their lives and health threats, dread of God's wrath, psychological and emotional effects, and fear of being held accountable by others. Throughout the in-depth interview, the majority of the women frequently mentioned these common issues. Before having an induced abortion, several structural and personal factors, including the results of pregnancy tests, fear of dying and health threats, gossip, stigma, and shame, the availability of services, the cost, the quality, and the preference of health centers, social networking (to whom shall I share or keep a secret), and a depressive state made it difficult for women to make their decision. Contrary to those who underwent surgical abortions, most women who undergo medical abortions, merely take misoprostol to end a pregnancy, report feeling good afterward. Yet, there was a considerable shift after undergoing an induced abortion compared to pre-abortion. In other words, after having an abortion, most women felt guilty, distressed, and suffered from serious health issues like nausea, bleeding (hemorrhage), abdominal discomfort, and similar symptoms.
Above all else, societal reactions like prejudices and rumors, as well as offensive terms like "nefsegeday" (killer or murderer) and "newregna" (deviant from the norm), were frequently described. Nevertheless, despite the many difficulties women faced after having an induced abortion, they used a variety of coping strategies, including effective family planning, social connections like talking about the issue with others, consulting medical professionals about health risks, confessing to spiritual fathers, praying, and fostering self-confidence [the I can principle], among others. Jemila says the following:
I am at a loss for words. I had a wretched existence. I lost a lot of stuff, like my house (my marriage). I committed a sin that Allah [God] disallowed. It was unlawful. It was dark; I had no idea of the future. But these days, I always pray. I pray that Allah would pardon me. I made an effort to keep things a secret, but it did not work out that way. I've finally persuaded myself to beg my husband's pardon so we can cohabitate and raise our children (Jemila, 34).
Discussion:
The findings of this study showed that more than half of the respondents (58.4 percentage) had information about medical termination of pregnancy (MTP). This study has not confirmed the previous research done by [21] at Mizan-Tepi University, which showed that most respondents—382 (90.52 percentage)—reported they had never heard about safe abortion. Conversely, in the present study, 32.6 percentage of respondents heard about unsafe abortion practices. This study concurs with [22] that unsafe and illegal abortions continue to be the main causes of death, particularly for young Ethiopian women. Only 45.5 percentage of respondents reported having knowledge of Ethiopian abortion law (revised in 2005), consistent with [12] research conducted in Addis Ababa, which found that only 44 percentage of respondents reported knowing Ethiopian abortion law and its circumstances. More than half of those polled (59 percentage), when asked about the legalization of abortion, agreed that it should only be permitted in cases of rape or minor age when adequately reported to authorities; however, this result conflicts with [23], which supports a woman's right to decide to end a pregnancy under her circumstances. This is because abortion is not only a moral, religious, or medical issue, but also a human rights issue. After all, it violates a woman's right to privacy. Around 53 percentage of respondents believed that strict community norms and 49 percentage believed that economic factors were the main causes of pregnancy termination. This study's findings are consistent with [24], which claims that women opt to abort unintended pregnancies worldwide for various socioeconomic and cultural reasons.
About 38.7 percentage, 31.3 percentage, and 22.3 percentage of the respondents said that societal stigma, gender roles, and religion and morality, respectively, had a significant part in choosing to have an abortion. The current study thus agrees with [25, 26, 27] that contextual factors such as societal attitudes, religious views, morality, and cultural ideas and interpretations significantly influence abortion decisions. The current finding suggested that there were impediments to safe abortion practice. In this regard, 20.5 percentage of respondents mentioned conscious objections of doctors, 32.5 percentage unsafe abortion practices in the research area, 42.9 percentage strict values and social standards, 18.5 percentage lack of secrecy of healthcare professionals, and 26 percentage cost of the abortion fee as obstacles to safe abortion. Our study, therefore, agrees with [28], which asserts that moral agency, religious convictions, and societal stigma are personal and contextual factors affecting the decision to abort and the procedure's safety.
Nearly 43 percentage of respondents said that there were negative attitudes in society against abortion, and some respondents stated that they did not want to offer any kind of social support to women because they believed that having an abortion was against community norms. In light of this, the current finding is consistent with [29], where conservative cultural reactions led to unfavorable reactions towards abortion, and [14, 15], where most individuals expressed negative attitudes and reactions towards the practice of abortion in Ethiopia.
The regression tests revealed that stigmatizing attitudes, moral and religious discourse, and legal and medical discourse affected the community's perception of abortion. Hence, the independent variables influenced the dependent variable by 34 percentage. This result may be in accordance with [30] since there is a connection between community-level stigma, discriminatory views, and negative actions towards abortion that exist in communities. As a result, the current survey found that 73 percentage of respondents had negative sentiments concerning abortion practice and 23 percentage had positive attitudes. This result is consistent with earlier research in Zambia, where women were humiliated and shunned as murderers and strong opinions about the immorality of abortion were held [10]. According to surveys, most Ethiopians have a negative opinion of abortion [12, 15]. In order to do this, disobeying social standards as well as traditional views of what it is to be a woman led to feelings of regret, guilt, and remorse [31]. In light of this, the current study found that most women who had induced abortions experienced remorse, a fear of God's wrath, intense social stigma, rumors, and occasionally even discrimination. The current study, however, revealed that women are not only passive victims but also social actors with agency in a larger context, bound by the sociocultural contexts of their environment. In order to return to regular life, they used a variety of resilience strategies, including social ties (sharing the issue with others), consulting with medical specialists, confessing to the spiritual fathers, and praying. The results of this study [32] in Sweden, in which women employ typical strategies including cognitive, social, and symbolic strategies as rational actors try to overcome the difficulty of the decision-making process to abort the pregnancy, are consistent with this finding.
Implication:
The author would like to contribute to policy debates and further research on the constraining and enabling factors regarding safe abortion practices to address competing discourses that impede women's sexual and reproductive rights in Ethiopia. The present study showed that community-level stigma, a negative attitude of the community towards abortion, the conscious objection of healthcare providers, a lack of awareness of abortion law, and ignorance of social and psychological factors were the deterring factors in safe abortion practice.
The intersection of structural and individual-level determinants of women's experiences with abortion and public attitudes makes such gaps the greatest entrance points for socio-legal and health policies and their implementation. In other words, despite the Ministry of Health's issue of guidelines for safe abortion services, the current abortion law has to be reviewed while taking the social dynamic into account, and the national health policy's implementation needs to be reviewed. The impact of present normative systems and conflicting discourses on women's reproductive rights and maternal health circumstances hence calls for greater emphasis on current reproductive health strategies.
The implementation of community-based initiatives to address contextual factors that are against safe abortion practices will thereby boost women's capacities. Future research should therefore focus on the long-term effects of induced abortion on women's psychological sequelae and mental illness, the role of religious institutions in reducing unsafe abortion practices, and the stigma associated with having an abortion on a community level because religion both restricts and facilitates the practice of abortion. Moreover, since the current law ignores socioeconomic variables like the poverty connected with performing abortions, future scholars should concentrate on the impact of the current abortion law on social dynamics.
Conclusion:
This study showed several structural and contextual barriers to safe abortion practice. The decision-making process, as well as the practices and attitudes of the community towards abortion, were primarily influenced by sociocultural discourses and stringent community values and standards. For instance, religion is one of the best indicators of views against abortion and has a significant impact on both the lived experiences of women who undergo medically-induced abortions and the attitudes of the general public. Yet, the structure is always both confining and facilitating and should not be equated with restriction. According to the current study results, women who choose to have an abortion experience both burden and relief from religion.
The present study claimed that the normative structures and the agents are interfaced. In other words, various discourses frequently uttered in the community and the unfavorable attitudes of the community towards abortion affected not only women's lived experiences, such as reproductive rights and safe abortion practices, but also provided little or no social support for women who experienced abortion. Similarly, women's free will as active agents influenced community values for motherhood despite impeding normative structures. In this finding, the constraining nature of the existing contextual factors was more evident than its enabling factors in women's lives regarding abortion practices. This implies that the scope of the control of an agent is limited to the immediate contexts of actions and interactions [18].
The findings from this research showed that neither agency-level nor structural factors alone are sufficient to explain the complexity of abortion practices, the decision-making procedure, or the community's views about abortion. Instead, the combined impacts of structural and individual-level factors effectively explain the practice of abortion and community reactions. In order to address issues including societal stigma, health issues, psychological suffering of women having abortions, and community views about abortion practice, this study suggested policy implications both at the structural and personal levels.
Declarations:
Data Availability: To keep respondents’ confidentiality, the raw data would not be shared; however, it is available from the corresponding author on reasonable request and the summary data are available in the main document.
Conflict of Interest:
The author of this article declares that he has no conflict of interest
Funding Statement:
The funding source of this research was obtained from Addis Ababa University and the University has no role in design, data collection, analysis, decision to publish as well as preparation of the manuscript.
Author contributions:
I was involved in the conception and design of the study, participated on the data collection, analyzed the data, drafted the manuscript and approves the final version of the manuscript.
Acknowledgments:
Although many individuals and organizations have contributed a lot to accomplish this paper, the author is grateful to thank Addis Ababa University for its financial support in realizing this study. Secondly, the author would like to thank the Woldia Town Family Guidance Association of Ethiopia for allowing me to conduct this study. Thirdly, I extend my gratitude to the field coordinators, data collectors, and informants.
References
- Gilbert, Indira. (2013). Narratives on Abortion: Psychosocial, Ethical and Religious Considerations. PhD dissertation submitted to department of social work, University of KwaZulu-Natal Durban. Retrieved from ProQuest dissertation.
View at Publisher | View at Google Scholar - Tsehai Wada. (2008). Abortion Law in Ethiopia: A Comparative Perspective. Addis Ababa University.
View at Publisher | View at Google Scholar - Alex, L and Hammarstrom, A. (2003). Women’s experiences in connection with induced abortion–a feminist perspective: University, Umea, and Sweden.
View at Publisher | View at Google Scholar - Lauro, Don. (2011). Abortion and Contraceptive Use in Sub-Saharan Africa: How Women Plan Their Families, African Journal of Reproductive Health; 15 (1).
View at Publisher | View at Google Scholar - Reardon, D.C. (2003). Abortion Decisions and the Duty to Screen: Clinical, Ethical, and Legal Implications of Predictive Risk Factors of Post-Abortion Maladjustment. Journal of Contemporary Health Law and Policy; Vol. 20(33).
View at Publisher | View at Google Scholar - Agrawal, S. (2008). Determinants of Induced Abortion and Its Consequences on Women’s Reproductive Health: Findings from India’s National Family Health Surveys. Macro International Inc.
View at Publisher | View at Google Scholar - Adamczyk, A. (2009). Understanding the effects of personal and school religiosity on the decision to abort a premarital pregnancy. Journal of Health and Social Behavior; 50(5):180-195.
View at Publisher | View at Google Scholar - Balkin, Jack M. (2007). Abortion and Original Meaning Faculty Scholarship Series. Paper 228. Constitutional commentary; vol24 (291).
View at Publisher | View at Google Scholar - Ramos, Silvina, Mariana Romero, and Lila Aizenberg. (2014). Women’s experiences with the use of medical abortion in a legally restricted context: the case of Argentina. Journal of Reproductive Health Matters; Supplement (43):1–12.
View at Publisher | View at Google Scholar - Cresswell J, Schroeder R, Dennis M. et al. (2016). Women’s knowledge and attitudes surrounding abortion in Zambia: across- sectional survey across three provinces. BMJ Open access, 6: e 010076.
View at Publisher | View at Google Scholar - Aniteye, P and Susannah, M. (2011). Attitudes and Experiences of Women Admitted to Hospital with Abortion Complications in Ghana. Afr J Reprod Health;15 [1]:47-55.
View at Publisher | View at Google Scholar - Mihret Habte. (2010). Determinants of Abortion Practice in Addis Ababa.MA thesis submitted to Population studies, Addis Ababa University.
View at Publisher | View at Google Scholar - Selamawit Adnew. (2013). Views of Women about Accessibility of Safe Abortion Care Services in Addis Ababa, Ethiopia. MA thesis submitted to Department of public health, University of South Africa.
View at Publisher | View at Google Scholar - Assessment of the Attitudes of 15–49-Year-Old Women and Men towards Legalization of Abortion in Mekelle Town, Tigray, Ethiopia. MA thesis submitted to department of PUBLIC HEALTH, Addis Ababa University, (2002).
View at Publisher | View at Google Scholar - Worku Animaw and Binyam Bogale. (2014). Awareness and attitude to liberalized safe abortion services among female students in University and Colleges of Arba Minch Town, Ethiopia. Science Journal of Public Health.
View at Publisher | View at Google Scholar - Sintayehu Mekuriaw, Robel Mesay, Adissalem Dereje, Abera Kumalo, Mulugeta Feyissa et al. (2015). Knowledge, Attitude and Practice towards Safe Abortion among Female Students of Mizan-Tepi University, South West Ethiopia. Women’s Health Care.
View at Publisher | View at Google Scholar - Kidist Degifie. (2015). Exploring Women’s Socio-Emotional Experiences of Induced Abortion in Marie Stopes Ethiopia. MA Thesis Report Submitted to the School of Psychology, Addis Ababa University.
View at Publisher | View at Google Scholar - Giddens, Anthony. (1984). The constitution of society: outline of the theory of structuration. University of California press, Berkeley and Los Angeles.
View at Publisher | View at Google Scholar - Kothari, C.R. (2004). Research Methodology: Methods and Techniques. New Delhi: New Age International (P) Limited, Publishers.
View at Publisher | View at Google Scholar - CSA (Central Statistical Authority). (2012). The 2010/2011 Ethiopian household consumption and expenditure survey: “results for county level” Statistical report. Addis Ababa, Ethiopia: EPDRF CSA.
View at Publisher | View at Google Scholar - Mekuriaw S, Mesay R, Dereje A, Kumalo A, Feyissa M, et al. (2015). Knowledge, Attitude and Practice towards Safe Abortion among Female Students of Mizan-Tepi University, South West Ethiopia. J Women’s Health Care, 4:275.
View at Publisher | View at Google Scholar - Senbeto, Elias, Getu Alene, Nuru Abesno, and Hailu Yeneneh. (2005).
View at Publisher | View at Google Scholar - Denbow, Jennifer. (2013). Abortion: When Choice and Autonomy Conflict. Berkeley Journal of Gender, Law & Justice; Volume 20 (13) issue no 1.
View at Publisher | View at Google Scholar - Grimes, D. A., Benson, J., Singh, S.et al. (2006). Unsafe Abortion: the preventable pandemic.
View at Publisher | View at Google Scholar - Atkins, Rachel. (1994). The abortion Discussion: Abortion and Ethical Considerations.
View at Publisher | View at Google Scholar - McCulloch, U. R. (1996). Women’s Experiences of Abortion in South Africa: An Exploratory Study: MA thesis submitted for clinical psychology, university of Cape Town.
View at Publisher | View at Google Scholar - Komut, S. (2009). Discourse Analysis of the Abortion Debate in Turkey and the United States. MA Thesis T.C. Kadir Has University, Istanbul.
View at Publisher | View at Google Scholar - Lamina M.A. (2013). Health care providers‟ attitudes towards termination of pregnancy: A qualitative study in Western Nigeria. Open Journal of Obstetrics and Gynecology; 3, 400-410.
View at Publisher | View at Google Scholar - Kumar, A., Hessini, L., & Mitchell, E. M. (2009). Conceptualizing abortion stigma. Culture, Health & Sexuality, 11, 625–639.
View at Publisher | View at Google Scholar - Cockrill, Kate, Steph Herold, Ushma Upadhyay. (2013). Addressing Abortion Stigma through Service Delivery. Routledge.
View at Publisher | View at Google Scholar - Madeira, Jody L. (2014). Aborted Emotions: Regret, Relationality, and Regulation, Michigan Journal of Gender & Law.
View at Publisher | View at Google Scholar - Stålhandske, Liljas, M., Ekstrand, M. & Tydén, T. (2011). Existential Experiences and Strategies in Relation to Induced Abortion: An Interview Study with 24 Swedish Women. Uppsala University, Sweden.
View at Publisher | View at Google Scholar
