

Review Article | DOI: https://doi.org/10.31579/2835-8295/127
The Female Athlete Triad: A Case Study
- Michael Mc Ginnis,
- James Keane
- Leonard B. Goldstein *
Assistant Vice President for Clinical Education Development, A.T. Still University.
*Corresponding Author: Leonard B. Goldstein, Assistant Vice President for Clinical Education Development, A.T. Still University.
Citation: Michael Mc Ginnis, James Keane, Leonard B. Goldstein., (2025), The Female Athlete Triad: A Case Study, International Journal of Clinical Reports and Studies, 4(4); DOI:10.31579/2835-8295/127
Copyright: © 2025, Leonard B. Goldstein. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 May 2025 | Accepted: 25 July 2025 | Published: 04 August 2025
Keywords: acutest elevation myocardial infarction; cardiogenic shock; percutaneous coronary intervention; double culprit vessel occlusion
Abstract
Stroke remains a leading cause of disability and death in the United States, disproportionately affecting Black, Latinx, and Asian or Pacific Islander populations. Atrial Fibrillation (AF), a prevalent arrhythmia, further elevates stroke risk. This article reviews the impact of culturally tailored prevention programs on health equity, particularly in underserved populations. Evidence from studies highlights the effectiveness of culturally specific education in improving stroke awareness, prevention behaviors, and emergency response in minority communities. Programs that integrate cultural beliefs and address systemic barriers show promise in reducing stroke-related disparities. However, challenges in sustaining long-term behavior change and addressing healthcare access persist. Future research should focus on refining these programs, fostering trust between patients and providers, and overcoming systemic obstacles to improve stroke outcomes for all populations.
Introduction
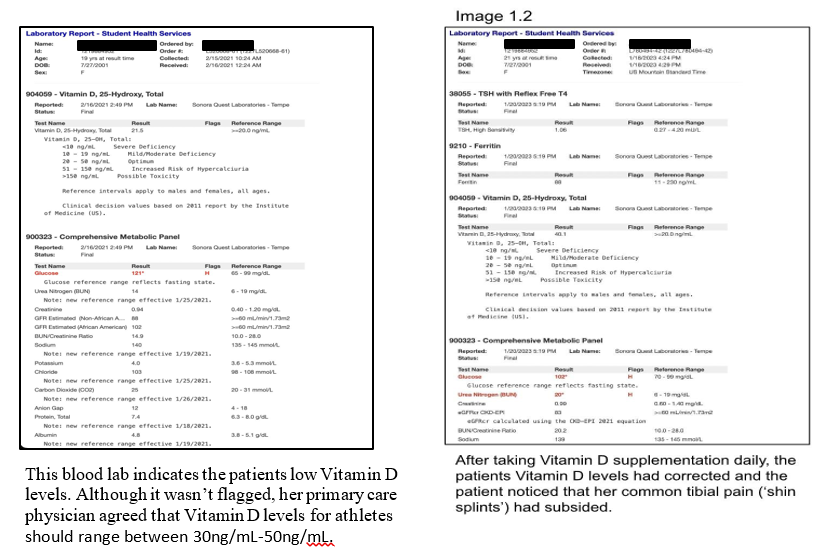
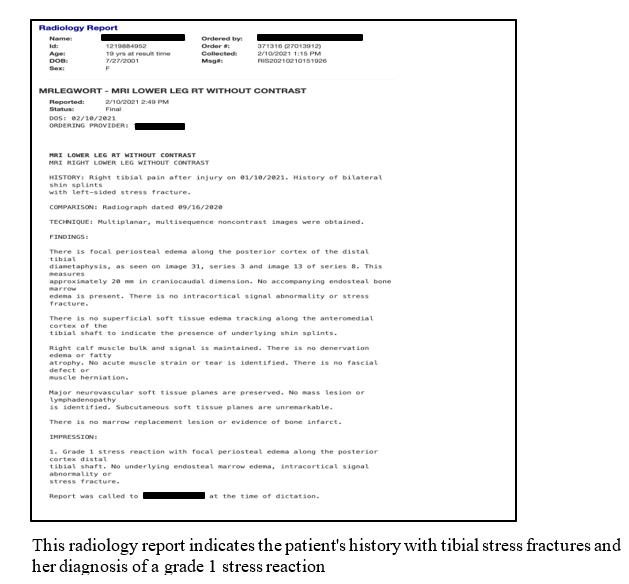
Case: A 19-year-old competitive female triathlete with a 6-month history of amenorrhea, stress fractures, disordered eating, and anxiety presents to her primary care physician for progressive fatigue. Her fatigue began 6 months ago, after beginning her competitive season for triathlon. She had been previously seen by healthcare professionals, but her concerns were dismissed as she was told that her fatigue was due to being a full-time student athlete. 3 months into her season, she noted consecutively missed menstrual cycles. She began having anterior tibial pain that she presumed was from a difficult training regime. Upon further examination her PCP ordered a CBC, BMP, TSH, and Vitamin D levels. Studies revealed all to be normal besides a low Vitamin D count. Further testing was done to rule out causes of her amenorrhea such as: beta-hcg, ovary function test, and prolactin tests which were all unrevealing. MRIs were taken to assess her recurring shin pain, with impressions of a grade 1 stress fracture and history of previous stress fractures. Discussion of the patient's prior eating habits revealed a history of bulimia nervosa. Patient was started on Vitamin D supplementation (30 mcg once per day), an increased caloric intake, and supplemental counseling appointments to address her eating disorder. Attached are blood labs, and a radiology report that are used for reference.
Overview:
The female athlete triad is relatively common amongst young female athletes and may present with: menstrual dysfunction, low energy availability (with or without an eating disorder), and decreased bone mineral density. This recognized pattern of symptoms became prevalent amongst young female athletes in the early 1990’s. It has been over 30 years since it was first described and clinicians are still debating on the relationship between the various symptoms, as well as the treatment for their patients. This case vignette will provide an exhaustive review of the female athlete triad, which in turn, will address the risk factors/pre-disposition of the condition, the components of the disease, the possible causations, as well as its treatments.
Menstrual irregularities:
Menstrual irregularities can present in many ways amongst young females who partake in vigorous activities. Amenorrhea (absence of menstruation) and oligomenorrhea (irregular menstrual blood flow) are some examples of the menstrual irregularities that female athletes can experience. When looking at the general population, 2%-5% of females experience menstrual abnormalities, however when the control group is narrowed down to female athletes, the prevalence of menstrual abnormalities (specifically amenorrhea) jumps to 65% [Saadedine et al., 2023]. Amenorrhea can be further divided into primary and secondary causes. Primary amenorrhea is defined as the failure to reach menarche in a female of reproductive age. Physicians should clinically evaluate a female if no onset of menarche has occurred by age 16 with secondary sex characteristics or if no onset of menarche by age 14 without secondary sex characteristics [Saadedine et al., 2023]. In comparison, secondary amenorrhea is the disappearance of an established menarche after 6 months. There are many different etiologies that can give rise to amenorrhea, however, in regards to the triad the specific type that we will examine is hypothalamic causes. A form of secondary amenorrhea is known as functional hypothalamic amenorrhea (FHA). FHA is due to a disruption of the hypothalamic-pituitary-ovarian axis (HPO axis). In this condition gonadotropin-releasing hormone pulsatility happens at irregular fluctuations, which in turn, results in inconsistent gonadotropin secretion. Due to this inconsistency, both gonadotropin-releasing hormone (GnRH) and luteinizing hormone secretion (LH) become disrupted. These hormones are vital for ovulation and the maintenance of a normal menstrual pattern. When assessing possible causes of FHA research has categorized 3 possibilities: psychological stress, disordered and restrictive eating patterns, and excessive exercise [Saadedine et al., 2023]. The psychological stress that is associated with the triad is represented by the increase of glucocorticoids like cortisol, which is seen in patients with FHA having an increased 24-hour cortisol levels [Morrison, 2020]. Cortisol has a suppressing effect on hypothalamic GnRH synthesis and secretion, directly affecting the HPO axis.
The HPO axis is further disrupted in patients with the triad due to disordered eating and excessive exercising. This combination leads to an energy imbalance which has direct effects on the GnRH and LH pulsatility. As mentioned before the pulsatility is required for ovulation and normal menstrual patterns, which ultimately involves a female's estrogen production. Estrogen production in patients with the triad is severely diminished, which contributes to the second component of decreased bone mineral density [Saadedine et al., 2023]. Along with low energy and decreased bone mineral density, menstrual dysfunction/amenorrhea forms an important pillar to the female athlete triad condition.
Energy Imbalance & Disordered Eating:
The second component of the triad is energy imbalance, or simply put the difference between the patient's nutritional intake and the amount of energy expended. As patients with the triad are athletes, they have greater physiological demands needed to maintain the normal bodily functions. The low energy availability can be associated with an eating disorder but also has been noted to occur in the absence of one. Failing to attain the adequate nutritional intake needed to replenish one's metabolic needs can arise from time constraints, such as in our college athlete. Rushing between sport and class can make it difficult to sit down and properly refuel one’s self. In addition, most adolescent athletes do not have the proper education in regards to nutritional knowledge to know which macro nutrients they should consume following hard training sessions [Dusek, 2001]. With that being said, the energy imbalance seen in the triad is most commonly associated with some form of disordered eating.
Unfortunately, female athletes are at risk of developing an eating disorder due to the pressure of maintaining an ‘aesthetic’. Many sports that encourage or emphasize leanness such as running, swimming, triathlon, and ballet, has resulted in a prevalence of 70% of females with FHA, which is a staggering difference when compared to the prevalence of the general population of 5% (Dusek, 2001). This high percentage of FHA is associated with a disordered or restrictive eating pattern to maintain that leanness.
Disordered eating is fairly common amongst modern day society with 65% of women [between the ages of 25 years and 45 years] reportedly being diagnosed with an eating disorder [Gillings School of Global Public Health, 2008]. Although women are more commonly diagnosed, around 20% of men are also affected by various forms of an eating disorder. When looking at athletes, the statistics increase drastically with 45% of female athletes and 19% of male athletes struggling with eating disorders [Conviser, J. H et al., 2018]. Athletes are a smaller control group than the general population, therefore these percentages show a large effect of eating disorders amongst this specific population of people.
Female athletes are most commonly diagnosed with anorexia nervosa, bulimia, and binge eating disorder which can all contribute to negative physical and mental effects. In the athletic community performance is key and the attainment of the performance comes with strict dietary protocols. It is noted that up 65% of competing athletes in the professional level partake in stringent dietary restrictions, with the prevalence to female athletes ranging from 18% to 52% [Conviser, J. H et al., 2018]. These strict dietary protocols can result in forming negative habits that promote low caloric intake or over-training to compensate for caloric intake. These habits all contribute to the diagnosis of an eating disorder, and result in low energy or fatigue and have a direct effect on bone health.
Osteopenia:
The interrelatedness of the components all contribute to one another. The first two components of amenorrhea and caloric/nutritional deficiency are entangled in the root causes of the third component, low bone mineral density (BMD).
It is important to note that usually physical activity increases BMD. Athletes that practice weight bearing and endurance exercises, on average have higher BMD than the general population. Exercising helps the bones stimulate more growth of bone tissue, reinforcing and making it stronger [MC Staff, 2023]. However, in amenorrheic athletes such as the ones found in the triad, they are more susceptible to low bone mineral density, stress fractures, and osteoporosis. This is partly due to the estrogen deficiency that they experience. Estrogen is an important modulator of overall bone health. Estrogen has the direct effect of stimulating bone formation and suppressing bone resorption. Peak bone mass for females is typically reached by the age of 21 and given the high prevalence of the triad occurring in patients between 15 to 21, the adverse complication of bone health is of major concern.
A low state of estrogen in addition to a low lean body mass in patients with FHA is an independent predictor of lower BMD [Pedreira et al., 2022]. Estrogen, although a primary modulator of bone health, requires supplemental contribution from nutritional intake. Patients with an energy deficiency are associated with hormonal imbalances such as: growth hormone and insulin like growth factor 1 (IGF-1) [Pedreira et al., 2022]. Both hormones help to stimulate bone growth. Furthermore, the high cortisol levels mentioned before are also associated with a reduction in osteoblastic activity, as well as the secretion of growth hormone and IGF-1. As it can be seen, the triad's components have an overlapping effect and greatly contribute to the severity of the condition.
Screening/Diagnostics:
When assessing the components of the triad, a study performed by Monica Torstveit and Jornunn Sundgot-Borgen, discovered the prevalence of all 3 components occurring simultaneously around 4% [Torstviet, 2005]. This is not a significant finding in comparison to the general population with a prevalence of 3.5%, however, there is a dramatic increase in findings when assessing for at least 2 components of the triad. We can see an increase from 4% to 26.5%, thus indicating that the prevalence of all 3 components at once is low, but a high percentage of female athletes suffer from some component of the disease. This is important to keep in consideration when clinically assessing a female athlete, because the presentation and timing of the components may vary in each individual.
It can be challenging to adequately assess an athlete for the triad due to the fragmented presentation of the disease, and partly the reason why this condition has been disregarded in the past. That is why when screening and diagnosing the triad we must be cognizant of the interrelated relationships of the components. Early intervention should take place during preseason physicals. Screening should include a thorough menstrual history, prior and current physical activity levels, diet history with current dietary behaviors, a full CBC, vitamin D levels, endocrine labs, and lastly family history.
Amenorrhea could be considered one of the most identifiable components of the triad and should not be overlooked by clinical physicians as a typical response to exercise. Studies suggest that a female's past menstrual history has a significant correlation to her current bone density. Missing more than 3 consecutive periods is a cause for concern, especially in a young developing female. In a patient presenting with amenorrhea, other tests should be conducted to rule out other potential causes. Ordering beta-hcg to rule out pregnancy, getting a full thyroid workup including thyroid stimulating hormone and free thyroxine to rule out thyroid dysfunction, ordering follicle stimulating hormone to rule ovarian dysfunction, and lastly ordering prolactin to rule out pituitary mass [Manore et al., 2007].
Disordered eating is a sensitive topic and should be approached with care. It can present in many different forms: bulimia, anorexia nervosa, excessive exercise, laxative abuse etc. Physicians should ask questions about the patient's past eating habits, as it is easier for a patient to admit to previous habits then current dietary behaviors [Mulcahey, 2020]. Being able to get a sense of your patients’ expectations they have for themself, in regard to their ideal body mass they believe is required to compete in their sport can offer much insight into a patient's thought process, and can help navigate a clinical examination. Upon physical examination it is worth noting if there are any signs of persistent vomiting such as calloused knuckles (clinically referred to as “Russel Signs”), loss of tooth enamel, gingival abrasions, or enlarged parotid gland. These clinical clues can help aid in the diagnosis of an eating disorder [Gordon, 2010].
Screening for bone mineral density is recommended in a female patient who presents with amenorrhea. The low estrogen state has a direct correlation on decreased bone health. Collecting a thorough history of a patient’s diet, medications, menstrual cycles, and previous injuries, assessing for the recurrence of bone pain and fractures. Certain medications that could cause low bone density such as: heparin, warfarin, cyclosporine, glucocorticoids, thyroid hormones etc, should be asked if being taken. [Rosen, 2023]. Physicians can utilize bone mineral density testing via dual-energy x-ray absorptiometry (Lewiecki, 2023) to help diagnose osteoporosis and monitor therapeutic response given a specific “Z-score" [Rosen, 2023]. Z-scores replaced the outdated ‘T-score’ screening method; which was not applicable to adolescent athletes. Adolescent teens are not expected to measure the same BMD as women outside of their age group, as they are still growing. When assessing a Z-score measurement of low bone mineral density for the general population, the International Society for Clinical Densitometry defines a score of greater than or equal to -2.0 SD as “within expected range for age” and a score of less than or equal to - 2.0 SD as “below expected range for age” [Nazem & Ackerman, 2012]. However, when addressing the athletic community, the American College of Sports Medicine defines “low BMD” as a Z-score between -1 and -2, along with the clinical risk factors for fracture (decreased energy availability, amenorrhea, history of stress fractures) [Nazem & Ackerman, 2012]. Osteoporosis is defined with a Z-score of -2 as well as clinical risk factors for a fracture.
Treatment:
Treatment of the triad is a joint effort. As mentioned before, the components of the triad do not typically present all at once, rather appearing individually and potentially during different time periods. Adequate treatment of the triad requires a multidisciplinary team, with goals of improving caloric intake, increasing overall energy availability, and the return of consistent menstrual cycles [Chamberlain, 2018]. Utilization of nutritional experts such as nutritionists or dieticians can be helpful in formulating individualized meal plans that address the caloric deficit. This is usually paired with a decrease in the training load for the athlete, allowing for sufficient rest and recovery. Referral to psychological counseling is recommended when the triad is accompanied with an eating disorder, aiming to modify unhealthy eating habits as well as perceived body image. With improving a caloric deficit, most of the time the patient's menses will return on its own. However, where a caloric deficit is not the main cause for amenorrhea, or if menses do not return after 6 to 12 months of a lifestyle modification, then it is recommended that a short-term course of transdermal estrogen with cyclic progesterone is utilized [Saadedine et al., 2023]. A study performed on women who suffered from anorexia and amenorrhea, encourages the usage of a 100ug transdermal estradiol patch applied twice a week and 2.5mg of medroxyprogesterone daily, for 10 days each month. Along with the return of consistent menstruation, this treatment plan showed an improvement in BMD over 6-, 12- and 18-month periods [Saadedine et al., 2023]. Oral contraception is not recommended as a treatment option for the female athlete triad, as there are no significant benefits to BMD in patients. There is still much debate on the optimal range of dietary calcium and vitamin D supplementation levels, however, it has been suggested that 1300 mg of calcium and 600 IU of vitamin D is recommended for premenopausal women [Ross et al., 2011]. An additional option that can be used for an athlete suffering from a low BMD who needs to reduce physical activity is the use of mechanical stimulation. Vibratory platforms have shown to aid in the reduction of bone mass loss with only a 20-minute session (Slatkovska et al., 2010), helping to mimic the results of impact training.
Conclusion:
The female athlete triad is a common condition that affects many adolescent female athletes. It consists of three components: amenorrhea, low energy availability (with or without an eating disorder), and low bone mineral density. The condition has been easily overlooked in the past and requires a joint effort from physicians, coaches, and family members to help assist in the rehabilitation process. While there is still some debate on how to adequately prevent and treat this condition, it is noted that it requires a holistic approach addressing the mind, body, and spirit of the growing athlete to ensure no long-lasting complications.
References
- Survey finds disordered eating behaviors among three out of four American women (fall, 2008). UNC Gillings School of Global Public Health.
View at Publisher | View at Google Scholar - Conviser, J. H., Schlitzer Tierney, A., Nickols, R. (2018). Essential for best practice: treatment approaches for athletes with eating disorders. Journal of Clinical Sports Psychology, 12.
View at Publisher | View at Google Scholar - T. G. Nazem, K. E. Ackerman, The female athlete Triad. Sports health (2012),
View at Publisher | View at Google Scholar - MC Staff. (2023). Strength training: Get stronger, leaner, healthier. Mayo Clinic.
View at Publisher | View at Google Scholar - Manore, M. M., Loucks, A. B., & Kam, L. C. (2007). The female athlete triad: Components, nutrition issues, and Health Consequences. Journal of sports sciences.
View at Publisher | View at Google Scholar - Mulcahey, M. K. (2020). Female athlete triad: Problems caused by extreme exercise and dieting - orthoinfo - aaos. OrthoInfo.
View at Publisher | View at Google Scholar - Gordon, C. M. (2010). Functional hypothalamic amenorrhea. The New England Journal of Medicine.
View at Publisher | View at Google Scholar - Rosen, H. N. (2023). Drugs that affect Bone Metabolism. UpToDate.
View at Publisher | View at Google Scholar - Chamberlain, R. (2018). The female athlete Triad: Recommendations for management. American Family Physician.
View at Publisher | View at Google Scholar - Lewiecki, E. M. (2023). Overview of dual-energy x-ray absorptiometry. UpToDate. Saadedine ,
View at Publisher | View at Google Scholar - M., Kapoor, E., & Shufelt, C. (2023). Functional hypothalamic amenorrhea: Recognition and management of a ... Mayo Clinic Proceedings.
View at Publisher | View at Google Scholar - Morrison, A. E. (2020). A review of the pathophysiology of functional ... - wiley online library. Wiley Online Library.
View at Publisher | View at Google Scholar - Meczekalski B, Podfigurna-Stopa A, Warenik-Szymankiewicz A, Genazzani AR. (2008). Functional hypothalamic amenorrhea: current view on neuroendocrine aberrations. Gynecol Endocrinol;24(1):4-11
View at Publisher | View at Google Scholar - Dusek T. (2001). Influence of high intensity training on menstrual cycle disorders in athletes. Croat Med J.;42(1):79-82
View at Publisher | View at Google Scholar - Pedreira, C. C., Maya, J., & Misra, M. (2022). Functional hypothalamic amenorrhea: Impact on bone and neuropsychiatric outcomes. Frontiers.
View at Publisher | View at Google Scholar - Torstveit, M. K., & Sundgot‐Borgen, J. (2005). The female athlete triad exists in both elite athletes and controls. Medicine and Science in Sports and Exercise, 37(9), 1449–1459
View at Publisher | View at Google Scholar - Ross, A. C., Manson, J. E., Abrams, S. A., Aloia, J. F., Brannon, P. M., et all., (2011). The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What Clinicians Need to Know. OUP Academic.
View at Publisher | View at Google Scholar - Slatkovska, L., Alibhai, S. M. H., Beyene, J., & Cheung, A. M. (2010). Effect of whole-body vibration on BMD: A systematic review and meta-analysis - osteoporosis international. SpringerLink.
View at Publisher | View at Google Scholar
