

Review Article | DOI: https://doi.org/10.31579/2834-5029/022
Systematic Literature Review on Nutritional Habits of 0–6-Year-Olds with Early Childhood Caries (ECC)
- Sophie Antoniou *
- Samah Naeem
- Mandeep Kaur
- Khaled Almukhtar
Barts and The London school of Dentistry, UK.
*Corresponding Author: Sophie Antoniou, Barts and The London school of Dentistry, UK.
Citation: Sophie Antoniou, Samah Naeem, Mandeep Kaur, Khaled Almukhtar, (2023), Systematic Literature Review on Nutritional Habits of 0–6-Year-Olds with Early Childhood Caries (ECC), International Journal of Biomed Research, 2(3): DOI:10.31579/2834-5029/022
Copyright: © 2023, Sophie Antoniou. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 May 2023 | Accepted: 31 May 2023 | Published: 09 June 2023
Keywords: early childhood caries; nutritional habits; dentist
Abstract
This systematic review aims to highlight potential areas of importance within a child’s diet that play a primary role in their development of early childhood caries. Caries is a multifactorial disease, influenced by a number of factors including, oral hygiene, degree of mineralization of teeth, salivary flow rates in addition to dietary factors.
Introduction
This review will specifically focus on the nutritional aspect involved in the pathogenesis of caries. Targeting the main dietary risk factors will aid in the prevention of ECC and severe early childhood caries (SECC), with an overall aim to reduce the DMFT (Decayed Missing and Filled Teeth) in children. This is of particular relevance to the secondary dentition of these children, as those with ECC are much more likely to develop caries and subsequent infections in their adolescence and adulthood also (1), further underlining the immense significance of prevention.
Early childhood caries (ECC) is defined as the presence of one or more decayed tooth surfaces in any primary tooth in a child 71 months of age or younger (2,3). It currently represents the most common chronic illness amongst children and represents a serious problem in dentistry due to its rapid progression. The consequence of ECC can affect the immediate and long-term quality of life for the child and has been reported to result in eating limitations, difficulties in language development, increased absence from schools and reduced self-esteem (4).
The move to a more holistic approach to patient care will be well supplemented by a dentist and nutritionist approved dietary plan from which parents and guardians can base their child’s diet upon. Dental care professionals can use this dietary guide as a primary structure in which they can provide concise and bespoke dietary advice to the guardians of each individual pediatric patient dependent on the routine of the child, the age, guardian’s occupation, and guardian motivation and participation.
This in turn, will likely reflect well on the patient’s general health as they grow throughout life with a good foundation set in childhood. Such good habits often echo in generations to follow with positive examples already established from such a young age. The shift towards a healthier diet in children has already been initiated with healthier school meals, the sugar tax, and numerous other examples, this dietary plan aims to facilitate the transition into a more nutritiously balanced diet to nourish our patient’s lifestyle and reduce the risk of a multitude of non-communicable diseases, principally caries. This concept may initially appear utopian, yet we are in prime position to see our patients regularly to motivate and enforce good dietary habits for which the benefits are endless.
Aim:
To construct a dietary proposal for public dissemination based on nutritional and dental recommendations for children under 6.
Objectives:
To evaluate the various dietary habits implicated in the development of ECC and how they interact with the indirect factors that also predispose children under 6 to ECC.
Prevalence:
An oral health survey conducted in 2019/2020 by Public Health England showed the prevalence of ECC in 3-year- olds is 10.7% (5). The National Dental Epidemiology Programmed looking at 5-year-olds in England in 2018/2019 showed the prevalence of ECC in 5-year-olds was 23.4%, which varied according to different regions in England with 17.6% in the South East to 31.7% in the North West (6). The mean prevalence of ECC in children in England increases over two-fold from 3 years to 5 years old, at age 3 almost all children have all 20 primary teeth, as the primary dentition is retained a further 2 years in the mouth, the evidence of visible decay doubles.
Aetiology:
The answer to the question “What causes dental caries?” is not as straightforward as it may first seem - the complex, multi-factorial nature of the aetiology of ECC involves the interaction between the pathogenic microorganisms, fermentable carbohydrates, susceptible tooth surface and time. With sufficient time, the cariogenic microorganisms can induce demineralisation of the tooth structure in the presence of fermentable carbohydrates and induce cavitation (1).
Microbiological risk factors
Streptococcus mutans and Streptococcus sobrinus are among the most commonly isolated bacterial species found in dental caries. Many investigations have shown that S. mutans exceed 30% of the plaque flora in those children suffering from ECC (7). In the presence of fermentable carbohydrates, such as sucrose, the acidogenic bacteria begin fermentation causing a rapid fall in pH to 5.0 or below. It is within these low pH conditions that initiates a change in the composition of the biofilm matrix and subsequent demineralisation occurs.
Microorganisms can colonise the oral cavity by both vertical and horizontal transmission, however as bacteria alone are not sufficient for disease to occur, it is considered a non-communicable disease (8).
Dietary habits
As with many other non-communicable diseases, dietary routines are integral to the development of the condition. In addition to the establishment of the oral flora, poor dietary habits such as quantity and frequency of sugar intake increase the risk of development of ECC. The recommended daily sugar limit for children under 6 is no more than 19 g sugar per day, or a maximum of 5 sugar cubes. Further to this, children under the age of 4 are recommended to avoid sugar and sugar sweetened beverages altogether (9). Data from Public Health England has demonstrated that children in this age group are consuming over double the recommended sugar quantity, with high-sugar soft drinks prevailing as the main culprit (10). Not only does this directly correlate with higher incidences of ECC, but a number of other non-communicable diseases, namely type II diabetes mellitus and obesity.
There is abundant epidemiological evidence, both from groups that have consumed low quantities of sugar and from groups that have consumed high quantities of sugar, that sugar, namely sucrose, is the primary dietary factor affecting dental caries prevalence and progression (10).
ECC may also be referred to as ‘baby bottle caries’ as there appears to be a clinical consensus that prolonged and nocturnal breastfeeding and/or bottles filled with milk containing several cariogenic sugars is associated with ECC. Reduced saliva production at night results in higher levels of lactose in the resting saliva, favoring demineralisation (rather than remineralisation) at night. Unfortunately, it is becoming more common for bottles and sippy cups to be filled with fruit drinks for ingestion during the day and even at night. These juices are often well accepted by both parents and children due to the sweetened taste and false belief by parents that they are nutritious. Their consumptions should however be considered as highly cariogenic (11).
Characteristics of enamel:
Enamel is the hardest tissue in the human body, consisting mainly of hydroxyapatite, and has extraordinary mechanical properties (12). The enamel of deciduous teeth is built by ameloblasts within a significantly shorter period (24 months) in comparison to permanent teeth (up to 16 years). As a result, the enamel developed in deciduous teeth has a very thin and less organized microstructure, making it more susceptible to demineralization by acids (13).
There are, of course, many other risk factors for ECC. Developmental defects, believed to be caused by prenatal conditions and common childhood systemic illnesses, is a common occurrence in primary teeth. These defects can be classified based on their clinical appearance - enamel hypoplasia, demarcated opacities and diffuse opacities. The incomplete enamel calcification on pits and fissures provides the ideal site for cariogenic bacteria and consequently, ECC can develop more rapidly on tooth surfaces (14).
Materials and Methods:
Our review is based on research in line with our PEO question as demonstrated in figure 1.
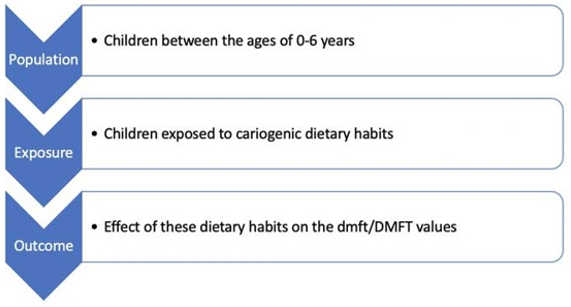
Electronic databases that we screened to gather research undertaken conforming to our PEO included: Pubmed, Cochrane, Embase and Wiley online library. The search was undertaken using the following keywords “diet*” AND “early childhood caries” OR “severe early childhood caries” OR “dental decay” OR “dental caries” AND “primary dentition” OR “primary teeth” OR “deciduous teeth” and the flow diagram below maps out the search strategy that was undertaken to identify appropriate studies for this review.
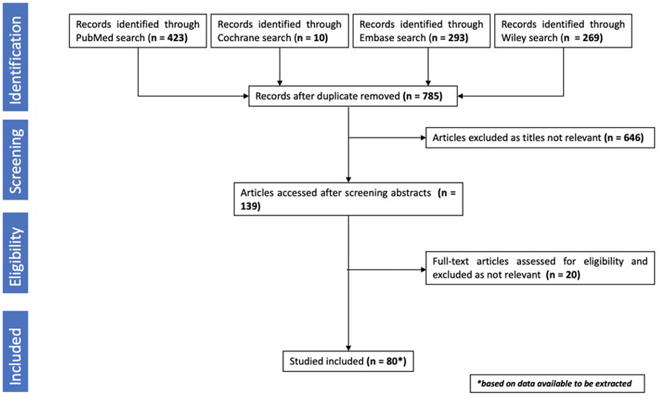
A total number of 995 studies were found from the electronic databases and those that were published in English were analysed, including investigating the screening titles and full-test articles, according to our inclusion criteria:

Research within the United Kingdom was found to be limited in numbers and thus global studies have been incorporated into this literature review, with the hope to stimulate further primary research into this topic of interest within the UK.
The analysis of the studies revealed significant dietary risk factors that were frequently seen in association with ECC. We can deduce a correlational relationship from these, directing us towards potential further studies to be conducted to prove causative mechanisms of action.
Nutritional habits:
We are all taught as dental care professionals to use our trusty oral hygiene instructions and dietary advice as the basis of dental disease prevention and to combat the risk factors that predispose our patients to preventable diseases. Yet by dietary counselling, we highlight the presence, frequency and quantity of sugar present in our patient’s diets. Not only is this heavily subjective to reporting bias from our patients or their caregivers - which is unlikely to be accurate, we have to contemplate whether focusing solely on the sugar aspect of our patients’ diets is doing them a disservice by only addressing one facet of a highly complex interaction of dietary components. We do not consume food in isolated food groups but in a varied way with different consumption methods, times of day and diverse food choices. Hence, analysis of the integration of different components should prove more helpful in providing targeted nutritional advice for the prevention of ECC.
The correlation between what one consumes and one’s caries risk has long been established, since Aristotle first hypothesised that caries was caused by eating sweet figs which stuck to teeth in 4th century B.C. (15). Since then, we have found that the cariogenic potential of fermentable carbohydrates can be magnified by numerous additional dietary factors in combination with oral commensal flora and host factors, such as substrate clearance via rate of salivary flow.
Findings:
Table 2 delineates dietary factors that directly contribute to higher risk of caries development and the various studies from which we gathered the findings.
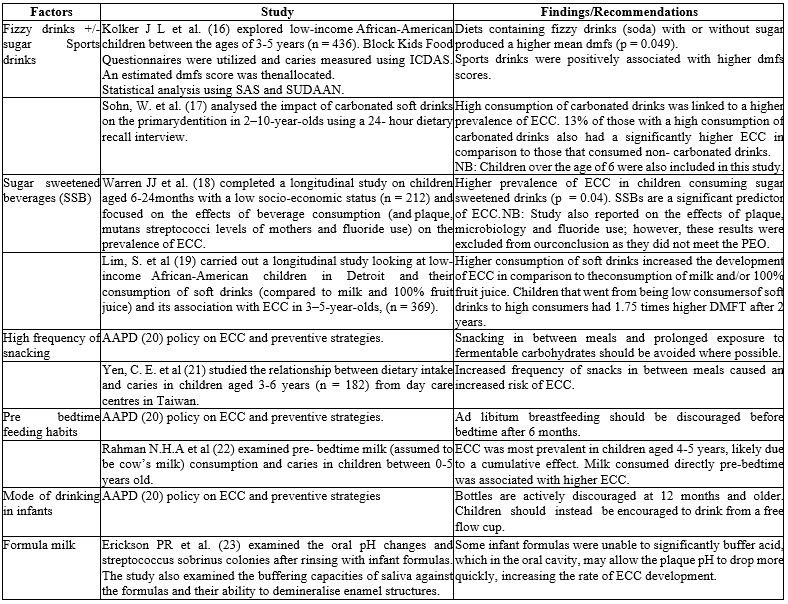
NB: dmfs and dmft are both quantitative measures of caries present using either the teeth (dmft) or tooth surfaces (dmfs)
Sucrose has been found to be twice as cariogenic as fructose (37) which is commonly found in western diets of children under 6 who are given foods containing sugar, maple syrup, dates and honey, to name a few.
The cariogenic potential of foods containing these sugars also depends on the substantivity and the frequency of consumption. It must also be noted that when eaten in conjunction with other foods, the cariogenic effects may be mitigated. Presence of cheese, cocoa, and xylitol among other foods, appears to reduce the cariogenic potential of a sucrose-containing meal in the mechanisms outlined in the third column of table 2 (38). Imfeld, T et al. (39) recorded interdental plaque pH during different meal patterns using plaque pH telemetry. It was found that peanuts and cheddar cheese increase oral alkalinity, and cheese reduces pH drop (but the comparison used in the study was a sugar rinse) (40).
Similarly, Jensen, M.E et al. (41) discussed the acidogenic potential of a variety of foods by using short-term pH telemetry (30 min) on interdental plaque (n=5) dairy sources such as; cheddar cheese and skimmed milk were less acidogenic than other common dietary foods.
Raw, unrefined cocoa without added sugar was shown to inhibit oral acidification with anti-plaque activity at the ADA conference in 2015 (38). From the findings that can be concluded from the studies collated in the table above, the necessity to consider the diet as a whole is further underlined.
It is prudent to consider the structure of the foods consumed. The cariogenic potential of an apple or a toffee varies even if the sugar content of both is equal. Aside from substantivity in the mouth, the water content, fibre and presence of minerals, such as calcium reduce the cariogenic potential of natural bound sugars such as those found in fruit. Furthermore, the mastication usually needed intra-orally during consumption of foods containing natural bound sugars mitigates the risk of developing dental caries by increasing salivary secretions and sugar clearance. The WHO has stated that it is the intake of free sugars that should be limited to prevent non-communicable diseases, including ECC (42). Interestingly, the research was conflicting but the majority of studies found that presence of fruit in the diet was inversely correlated with ECC, this may reflect socio-economic status or health behaviours of the parents but fruit, when eaten whole, should not be excluded in a child’s diet due to the sugar content. It must also be noted that different fruits have different substantivities, minerals, fibre content and thus varying degrees of cariogenicity.
WHO guidelines recommend that consumption of free sugars should provide ≤10% of energy intake, with a suggestion to further reduce intake to <5>
The most prevalent dietary factors implicated in the development of ECC as seen in the current literature are frequent consumption of food and drinks containing fermentable carbohydrates as free sugars, particularly when consumed outside of mealtimes. As aforementioned, the cariogenic potential of these substances is in combination with time, host surface and biofilm formation, and is often exacerbated by non-dietary factors such as insufficient fluoride exposure, poor oral hygiene and a subsequent alteration of oral microflora (3).
Indirect factors increasing the risk of ECC
Socioeconomic status of children belonging to ethnic and racial minorities have higher prevalence of malnourishment, leading to increased risk for enamel hypoplasia and insufficient fluoride exposure, combined with a greater inclination for a cheaper and more sugary diet (43). A similar pattern was seen in children born to single mothers (44).
Having parents earning low-income salaries put the child with a higher likelihood of having a DMFT/dmft score that was four times higher than those with parents earning high-income salaries (45,46). Parents’ own lifestyles often dictate the diet and prognosis of their child’s health particularly in children under 6. Parents influence which foods are present in the house, the meals that are frequently consumed, as well as timings and feeding behaviours. High- energy and low-cost foods are more prevalent in households that are in the low-income category as they are generally more affordable. These high-energy foods are usually saturated with sugar and salt. Unfortunately, this often reduces the overall diet quality by providing energy without micronutrients. It can also be hypothesised that those from low-income households are often not advantaged enough to be provided education regarding good oral hygiene practices and are likely to access a dental care professional less frequently due to financial pressures which may be confounding factors. The research draws conclusions that children at either extreme of weight; either significantly underweight or overweight, have higher prevalence of caries, this finding resounded with low socioeconomic status families from deprived backgrounds presenting with more ECC.
It is important to note the use of sugar sweetened foods and beverages given as a reward to a child. Not forgetting the administration of cariogenic foods given by caregivers even after having a dental appointment. Paediatric patients will eagerly await their sugary snack from parents who are simply too exhausted to refuse, immediately relegating their child’s oral health secondary to management of the child’s emotional requests. Extensive literature has elucidated the addictive properties of sugar (47), hence it is unsurprising that when given regularly, rather than as a one off treat, an often painful cycle of deteriorating oral health commences.
Dietary acids are often overlooked in paediatric dietary analysis as sugar takes the main precedence. As described earlier, the pathogenesis of caries involves anaerobic metabolism of dietary substrates by acidogenic bacteria which demineralise the tooth surface in the presence of substrate and time. Direct extrinsic acids can also form an optimum environment for tooth decay to occur. Fortified when in combination with free sugars, an example would be coca cola, which has a pH of 2.6 owing to its phosphoric acid content. We know that enamel is demineralised at a critical pH less than 5.5, as delineated by Stephan’s curve [48].
Enamel defects and erosion are often exacerbated by dietary acids without bacterial aetiology. The weakening of the hexagonal enamel prisms due to effects from extrinsic acids leaves the tooth structure more susceptible to decay and breakdown. Thus, it is integral to examine the combination of foods consumed in our patient’s meals and snacks and the timings of consumption.
Eating disorders will also weigh heavily on the development of caries due to the weakening of tooth structures, leaving the hydroxyapatite more likely to demineralise. However, illnesses such as anorexia and bulimia nervosa are significantly more pronounced in older paediatric patients, with a peak prevalence in puberty (49). It is rare to discover eating disorders in children under 6, likely due to reduced self-awareness, high activity levels and a large proportion of meals being supervised and provided by caregivers.
Discussion:
Every child has the right to the best start in life and this has been highlighted by programmes initiated by Public Health England. Dietary routines form patterns of behaviour and when repeated over a prolonged period of time, this will result in lasting impacts on not only the primary dentition, but also secondary.
There is universal recognition that consumption of free sugars and fermentable carbohydrates heavily precipitates the development of caries. However, a holistic approach to diet including all food groups needs to be investigated to devise an easy to follow and nutritionally balanced guide for caregivers to utilize when providing nourishment to children under 6. Examining the diet as a whole gives a further understanding of contribution to the development of caries, as opposed to examining sugar intake and frequency alone.
There are many dietary guidelines currently disseminated to the public, such as The Eatwell guide and Start4Life. The dietary proposal based upon the research in this review is unique in that it includes examples of foods containing the necessary macro and micronutrients with appropriate timings and combination of food groups in an easily
adaptable structure that can be tailored to individual children and caregivers' daily routines and circumstances, along with advice for good dietary practice including sipping water after meals, mode of drinking beverages other than water and many more good habits.
There is a large overlap in diets that are beneficial for oral and systemic health (50,51). Habits are more likely to be efficacious and sustainable long-term if primary caregivers implement healthy habits earlier, the importance of which cannot be understated. Dietary counselling may even begin as early as prenatally. This in turn, will likely reflect well on the patient’s general health as they grow throughout life with a firm foundation set in childhood. Such good habits often echo in generations to follow with positive examples of health-supporting dietary routines already established from such a young age. The shift towards a healthier diet in children has already been initiated with healthier school meals (52) the sugar tax, and many other examples. The dietary plan which is to follow from this literature review aims to facilitate the transition into a more nutritiously balanced diet to nourish our patient’s lifestyle and reduce the risk of a multitude of non-communicable diseases, principally caries. This concept may appear utopian, yet we are in prime position to see our patients regularly to motivate and enforce good dietary habits, for which the benefits are endless.
The transition to a more holistic approach to patient care will be well supplemented by a dentist and nutritionist approved dietary plan from which parents and guardians can base their child’s diet upon. Child health professionals, dental care professionals, schools and caregivers may use this dietary guide as a primary structure in which they can provide concise and bespoke dietary advice to the guardians of each individual paediatric patient dependent on the routine of the child, the age, guardian’s occupation, and guardian motivation and participation. The dietary guide will aim to provide a tool that child health professionals, dentists and guardians can employ to simplify the intricate, yet highly crucial, weapon towards prevention.
Conclusion:
All children deserve the best start to life and with tooth decay as one of the most common oral diseases, prevention is vital as the consequences of ECC can be detrimental to the overall quality of life. Significant regional inequalities remain based on differences in socio-economic status, although we are fortunate for the movement towards preventative care, further research needs to be carried out to highlight the importance of all dietary aspects.
During this literature review, it has been highlighted that recent studies and those that have been carried out within the UK are sparse and single-faceted, focusing mainly on the presence of sugar within the diet. Many of the studies carried out in other countries have limited applications within the varying demographics in the UK. Despite the Eatwell guide serving as the highest regarded dietary reference for the population, it has its limitations; the advice to ‘eat less often and in small amounts’, is not easily interpreted by members of the public and perhaps evokes a negative connotation with eating. Conversely, we aim to provide positive dietary aids that not only support a well nutritioned diet that prevents non-communicable diseases, but gives detailed advice on behavioural habits such as timing of snacks, mode of consumption, examples of food groupings.
As the authors understand the complexity of the interaction between different factors in the process of dental decay, we would suggest that the future studies should be directed more towards dietary habits rather than focusing on the presence or absence of sugar within the diet. We believe that this will have a better impact on the dietary habits in the community as the perception and understanding of such advice would be more applicable into daily life. It would be interesting to conduct a study looking at children under the age of 6 who follow different dietary plans based on geographic location, with all other oral health factors such as oral hygiene, socioeconomic status and fluoride controlled, and assess the resulting dmft, although we acknowledge that controlling these variables is extremely difficult in a real-life setting.
Conflicts of Interest:
The authors of this article declare no conflicts of interest.
Acknowledgements:
The authors of this review would like to give great thanks to Dr Mandeep Kaur and Dr Khaled Almukhtar who lent copious amounts of support and patience as our authors conducted their review during the process of final exams and graduation. A final thanks to nutritionist-dietitian Yiota Savva, who approved the nutritional guide in the second part of this two-part series.
References
- Colak, Hakan et al. (2013). Early childhood caries update: A review of causes, diagnoses, and treatments.” Journal of natural science, biology, and medicine. vol. 4,1: 29-38.
View at Publisher | View at Google Scholar - Drury TF, Horowitz AM, Ismail AI, Maertens MP, Rozier RG, et al. (1999). Diagnosing and reporting early childhood caries for research purposes. A report of a workshop sponsored by the National Institute of Dental and Craniofacial Research, the Health Resources and Services Administration, and the Health Care Financing Administration. J Public Health Dent. 59: 192-197.
View at Publisher | View at Google Scholar - AAPD. (2008). Definition of Early Childhood Caries.
View at Publisher | View at Google Scholar - Casamassimo PS, Thikkurissy S, Edelstein BL, Maiorini E. (2009). Beyond the dmft: the human and economic cost of early childhood caries. J Am Dent Assoc. 140:650–657.
View at Publisher | View at Google Scholar - England PH. (2019). National Dental Epidemiology Programme for England: oral health survey of 5-year-olds.
View at Publisher | View at Google Scholar - England PH. (2020). Oral health survey of 3-year-old children.
View at Publisher | View at Google Scholar - Tahir, L., Nazir, R., (2018), Dental Caries, Etiology, and Remedy through Natural Resources, in Z. Akarslan (ed.), Dental Caries - Diagnosis, Prevention and Management, Intech Open, London.
View at Publisher | View at Google Scholar - Nurelhuda NM, Al-Haroni M, Trovik TA, Bakken V. (2010). Caries experience and quantification of Streptococcus mutans and Streptococcus sobrinus in saliva of Sudanese schoolchildren. Caries Res. 44(4):402-407.
View at Publisher | View at Google Scholar - NHS UK. (2020). Sugar: the facts: NHS.
View at Publisher | View at Google Scholar - England PH. (2018). Children consume more than a year’s worth of sugar in 6 months.
View at Publisher | View at Google Scholar - Tinanoff N, Baez RJ, Diaz Guillory C, Donly KJ, Feldens CA, et al. (2019). Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: Global perspective. Int J Paediatric Dent. 29(3): 238-248.
View at Publisher | View at Google Scholar - Dorozhkin S. V., Epple M. (2002). Biological and medical significance of calcium phosphates. Angewandte Chemie International Edition. 41(17):3130–3146.
View at Publisher | View at Google Scholar - Wilson P. R., Beynon A. D. (1989). Mineralization differences between human deciduous and permanent enamel measured by quantitative microradiography. Archives of Oral Biology. 34(2):85–88.
View at Publisher | View at Google Scholar - Nota A, Palumbo L, Pantaleo G, Gherlone EF, Tecco S. (2020). Developmental Enamel Defects (DDE) and Their Association with Oral Health, Preventive Procedures, and Children’s Psychosocial Attitudes towards Home Oral Hygiene: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 17(11):4025.
View at Publisher | View at Google Scholar - Forster, E.S. (1927). The works of Aristotle, Vol. VII. Problemata. Oxford University Press, London. 931 pp.
View at Publisher | View at Google Scholar - Kolker JL, Yuan Y, Burt BA, Sandretto AM, Sohn W, et al. (2007). Dental caries and dietary patterns in low-income African-American children. Paediatr Dent. 29: 257–264.
View at Publisher | View at Google Scholar - Sohn W, Burt BA, Sowers MR. (2006). Carbonated soft drinks and dental caries in the primary dentition. J Dent Res. 85(3):262-266.
View at Publisher | View at Google Scholar - Warren JJ, Weber-Gasparoni K, Marshall TA, Drake DR, Dehkordi-Vakil F, et al. (2009). A longitudinal study of dental caries risk among very young low SES children. Community Dent Oral Epidemiol. 37:116–122.
View at Publisher | View at Google Scholar - Lim S, Sohn W, Burt BA, Sandretto AM, Kolker JL, et al. (2008). Cariogenicity of soft drinks, milk and fruit juice in low-income African-American children: a longitudinal study. J Am Dent Assoc. 139(7):959-967.
View at Publisher | View at Google Scholar - Policy on early childhood caries (ECC): Classifications, consequences, and preventive strategies. Pediatr Dent. (2008); 30:40–43.
View at Publisher | View at Google Scholar - Yen CE, Huang YC, Hu SW. (2010). Relationship between dietary intake and dental caries in preschool children. Int J Vitam Nutr Res. 80(3):205-215.
View at Publisher | View at Google Scholar - NHA Rahman et al. (2017). Relationship between Milk Consumption and Dental Caries in Children Aged 0-5. J. Pharm. Sci. & Res. Vol. 9(2), 170-172.
View at Publisher | View at Google Scholar - Erickson PR, McClintock KL, Green N, LaFleur J. (1998). Estimation of the caries-related risk associated with infant formulas. Pediatr Dent. 20:395–403
View at Publisher | View at Google Scholar - Branger B, Camelot F, Droz D, Houbiers B, Marchalot A, et al. (2019). Breastfeeding and early childhood caries. Review of the literature, recommendations, and prevention. Arch Pediatric. 26(8):497-503.
View at Publisher | View at Google Scholar - Hallonsten AL, Wendt LK, Mejàre I, Birkhed D, Håkansson C, et al. (1995). Dental caries and prolonged breast-feeding in 18-month-old Swedish children. Int J paediatric Dent. 5(3):149-155.
View at Publisher | View at Google Scholar - Ghazal, T., Levy, S. M., Childers, N. K., Broffitt, B., Cutter, G. R., et al. (2015). Factors associated with early childhood caries incidence among high caries-risk children. Community dentistry and oral epidemiology, 43(4), 366–374.
View at Publisher | View at Google Scholar - Abbasoğlu. Z, et al. (2015). ECC and Genetic Variants in Enamel Formation and Immune Response Genes. Caries Res; 49:70–77.
View at Publisher | View at Google Scholar - Petti, Stefano & Cairella, Giulia & Tarsitani, Gianfranco. (2000). Rampant Early Childhood Dental Decay: An Example from Italy. Journal of public health dentistry. 60. 159-166.
View at Publisher | View at Google Scholar - Bhat, Sham & Madan, I. (2003). Cariogenic potential of homemade weaning diet v/s commercial formula feeds an in-vitro study. Journal of the Indian Society of Pedodontics and Preventive Dentistry. 20. 165-168.
View at Publisher | View at Google Scholar - Colak H, Dülgergil CT, Dalli M, Hamidi MM. (2013). Early childhood caries update: A review of causes, diagnoses, and treatments. J Nat Sci Biol Med. 4(1):29-38.
View at Publisher | View at Google Scholar - Roberts M.W., Wright J.T. (2012). Nonnutritive, Low Caloric Substitutes for Food Sugars: Clinical Implications for Addressing the Incidence of Dental Caries and Overweight/Obesity. Int. J. Dent:1–8.
View at Publisher | View at Google Scholar - Mäkinen KK. (2010). Sugar alcohols, caries incidence, and remineralization of caries lesions: a literature review. Int J Dent. 981072.
View at Publisher | View at Google Scholar - Luke GA, Gough H, Beeley JA, Geddes DA. (1999). Human salivary sugar clearance after sugar rinses and intake of foodstuffs. Caries Res. 33:123–129
View at Publisher | View at Google Scholar - Butera, A., Maiorani, C., Morandini, A., Simonini, M., Morittu, S., et al. (2022). Evaluation of Children Caries Risk Factors: A Narrative Review of Nutritional Aspects, Oral Hygiene Habits, and Bacterial Alterations. Children (Basel, Switzerland), 9(2), 262.
View at Publisher | View at Google Scholar - Yen CE, Huang YC, Hu SW. (2010). Relationship between dietary intake and dental caries in preschool children. Int J Vitam Nutr Res. 80(3):205-215.
View at Publisher | View at Google Scholar - Krasse, B. (1982). Oral effect of other carbohydrates. Int. Dent. J. 32:24-32.
View at Publisher | View at Google Scholar - Paes Leme AF, Koo H, Bellato CM, Bedi G, Cury JA. (2006). The role of sucrose in cariogenic dental biofilm formation-new insight. J Dent Res. 2006;85(10):878-887.
View at Publisher | View at Google Scholar - Paolino, V. (1982). Anti-plaque activity of cocoa. Pp. 43-58 in J.J. Hefferren, editor; and H.M. Koehler, editor., eds. Foods, Nutrition and Dental Health, Vol. 2: Third Annual Conference. American Dental Association, Chicago.
View at Publisher | View at Google Scholar - Imfeld, T., R.S. Hirsch, and H.R. Mühlemann. (1978). Telemetric recordings of interdental plaque pH during different meal patterns. Br. Dent. J. 144:40-45.
View at Publisher | View at Google Scholar - Geddes, D.A., W.M. Edgar, G.N. Jenkins, and A.M. Rugg-Gunn. (1977). Apples, salted peanuts and plaque pH. Br. Dent. J. 142:317-319.
View at Publisher | View at Google Scholar - Jensen, M.E., and C.F. Schachtele. (1983). The acidogenic potential of reference foods and snacks at interproximal sites in the human dentition. J. Dent. Res. 62:889-892.
View at Publisher | View at Google Scholar - Diet, nutrition and the prevention of chronic diseases. World Health Organ Tech Rep Ser (2003);916: i–viii, 1– 149, back cover. WHO. Sugars intake for adults and children. Geneva: WHO.
View at Publisher | View at Google Scholar - Ramos-Gomez FJ, Tomar SL, Ellison J, Artiga N, Sintes J, et al. (1999). Assessment of early childhood caries and dietary habits in a population of migrant Hispanic children in Stockton, California. ASDC J Dent Child. 66:395–403.
View at Publisher | View at Google Scholar - Quinonez RB, Keels MA, Vann WF, Jr, McIver FT, Heller K, et al. (2001). Early childhood caries: Analysis of psychosocial and biological factors in a high-risk population. Caries Res. 35:376–383.
View at Publisher | View at Google Scholar - Tang JM, Altman DS, Robertson DC, O’Sullivan DM, Douglass JM, et al. (1997). Dental caries prevalence and treatment levels in Arizona preschool children. (30-1). Public Health Rep. 112:319–329
View at Publisher | View at Google Scholar - Al-Rashdan O, AlZoubi Z, Ibrahimi M, Al-Khraisha A, Almajali N. (2022). Mother's Characteristics and Socioeconomic Status as Possible Risk Factors for Children's Caries in Jordan. Int J Dent. 2006088.
View at Publisher | View at Google Scholar - Mysels DJ, Sullivan MA. (2010). The relationship between opioid and sugar intake: review of evidence and clinical applications. J Opioid Manag. 6(6):445-452.
View at Publisher | View at Google Scholar - Stephan R. (2022). Stephan's curve - Oxford Reference.
View at Publisher | View at Google Scholar - Klump KL. (2013). Puberty as a critical risk period for eating disorders: a review of human and animal studies. Horm Behav. 64(2):399-410.
View at Publisher | View at Google Scholar - Hu, S., Sim, Y.F., Toh, J.Y. et al. (2019). Infant dietary patterns and early childhood caries in a multi-ethnic Asian cohort. Sci Rep. 9, 852.
View at Publisher | View at Google Scholar - Scardina GA, Messina P. (2012). Good oral health and diet. J Biomed Biotechnol. 720692.
View at Publisher | View at Google Scholar - Vik FN, Van Lippevelde W, Øverby NC. (2019). Free school meals as an approach to reduce health inequalities among 10-12- year-old Norwegian children. BMC Public Health. 19(1):951.
View at Publisher | View at Google Scholar
