

Case Report | DOI: https://doi.org/10.31579/2835-8295/144
Suicidal Ideation in a Patient with Schizoaffective Disorder, Bipolar Type: A Case Report
- Sultan Akbar,
- Mohamed Ramadan,
- Leonard B. Goldstein *
University Mesa, Arizona and A.T. Still University, Mesa, Arizona, USA.
*Corresponding Author: Leonard Goldstein, University Mesa, Arizona and A.T. Still University, Mesa, Arizona, USA
Citation: Sultan Akbar, Mohamed Ramadan, Leonard B. Goldstein, (2026), Suicidal Ideation in a Patient with Schizoaffective Disorder, Bipolar Type: A Case Report, International Journal of Clinical Reports and Studies, 5(1); DOI:10.31579/2835-8295/144
Copyright: © 2026, Leonard Goldstein. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 November 2025 | Accepted: 29 December 2025 | Published: 16 January 2026
Keywords: suicidal ideation; schizoaffective disorder; mental health; valproic acid; mood stabilizers; antipsychotics
Abstract
Schizoaffective disorder, bipolar type can result in significant symptoms if left unmanaged. Significant care must be made in order to ensure that the correct therapeutic regimen is continued for a patient as long as the patient can tolerate treatment without considerable side effects. Abruptly withdrawing from mood stabilizing medication can result in grave consequences. We present the case of a patient with schizoaffective disorder, bipolar type who after a recent inpatient psychiatry ward discharge was left without a sufficient amount of medication to get him to his outpatient follow-up. He then became suicidal and needed to be readmitted. Questions about potential systemic inadequacies with the mental health system and stigma regarding mental illness are discussed.
Introduction
Schizoaffective disorder is a psychiatric condition characterized by a combination of 1) psychotic symptoms, such as those seen in schizophrenia and 2) mood symptoms, such as those seen in depression or bipolar disorder (1).It is considered a psychotic disorder because it has the prominent features of hallucinations and delusions(1).People with this illness have periods when they have difficulty understanding the reality around them(1).They may have unusual thoughts and suspicions, such as believing that other people can read their minds, control their thoughts, or plot to harm them(1). Numerous studies have attempted to understand the relationship between suicidal behavior among patients with schizoaffective disorder. Previous studies have found up to thirty-four percent of subjects with schizoaffective disorder having had a past suicide attempt (2).
The pharmacotherapy for schizoaffective disorder treatment includes antipsychotics, mood-stabilizers, and antidepressants (3). Antipsychotics are used to target psychosis and aggressive behavior in schizoaffective disorder (3). Mood-stabilizers are used if the patient has a history of manic or hypomanic symptoms (3). Additionally, antidepressants are used to target depressive symptoms (3).
This article will follow a patient with schizoaffective disorder from his inpatient psychiatric hospitalization to his outpatient appointment which he presented to with suicidal ideation.
Case Presentation:
Julio was a patient with schizoaffective disorder, bipolar type. He was well-known to the inpatient psychiatry ward provider, and it was his 5th admission since June 2024. He was again suffering a psychotic crisis and unable to live. His psychiatric status on examination was extensively remarkable. He was found to have poor insight and judgement and endorsing homicidal and suicidal ideation. His depakote level was found to be in subtherapeutic levels which was attributed to his psychosis, and he needed to be detoxified following a methamphetamine binge he faintly recalls. Figure 1 showcases the DSM-V criteria for the diagnosis of schizoaffective disorder [4].
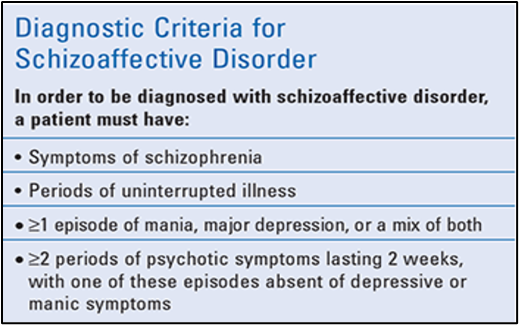
Figure 1: Diagnostic Criteria for Schizoaffective Disorder
He proceeded to have agitated events in which he became uncooperative with inpatient psychiatric staff and directed numerous vulgarities towards them throughout his stay. Shadows and voices would indicate to him which staff member to get next. When he had these events staff members were able to control him without the use of physical restraints.
He seemed to respond well to the treatment over the course of the next 6 days. When the provider felt like his psychotic symptoms were stabilized a suicide risk reassessment was performed, and he was found to be eligible to be discharged. His medication list and prescriptions were provided to him for him to then follow-up with outpatient psychiatry. He was released from the inpatient psychiatric ward on 09/29/25. His follow-up with outpatient psychiatry was on 11/11/2025. Upon completion of a brief psychiatric survey with the nurse, he indicated that he had suicidal ideation. His provider performed a suicide risk assesment and established that this was a passive suicidal ideation as compared to an active suicidal ideation. The clinic’s mental health crisis protocol was then implemented. He was then kept in the waiting room awaiting a bed in the inpatient psychiatry ward. Upon further questioning, he stated that it had been 5 days since he had taken his depakote due to running out of the supply provided to him upon his inpatient discharge. Upon further review of Julio’s medical history, this was not the first time he had suicidal ideation. In fact, he had numerous suicide attempts, one of which left him with a broken jaw.
Discussion:
Julio had been responding very well to treatment in the inpatient psychiatry ward. His symptoms had also been under appreciable control until his depakote had run out. Patients time and time again have been placed at the blame for nonadherence to medications. However, in Julio’s case, he was forthcoming to getting his treatment and was willing to do whatever was necessary to make sure his schizoaffective disorder was under control. He had the courage to pursue significant medical treatment despite the intense stigma surrounding mental health treatment. Ultimately, he ended up with a
6 days stay in a psychiatric ward, another suicidal event, and a return to the psychiatric ward a month and a half later.Julio had been to the inpatient psychiatric ward five times in less than two years. There is no telling to what degree potential clinical shortcomings could have contributed to this incredibly robust hospitalization history. On the other hand, concessions must be granted to the inpatient provider who oversaw his discharge and couldn’t foretell when he would get into a busy outpatient psychiatric clinic. There seems to be an all-around inadequacy of the mental health system. This could be attributed to both the oversaturation of the healthcare industry and the significant lack of funding available.
Conclusion:
Getting patients with mental health issues the adequate medical care that they need has always been a perplexing issue. Even minor inadequacies in the healthcare system can result in significant hardships that a patient can face. Ample care must be put into making revisions to the current systems in place to maximize the quality of care provided to patients.
Statement of Informed Consent:
Informed consent was obtained from the patient that was presented in the case report.
References
- Noosha Niv, Ph.D.; et al. (2016). What Is Schizoaffective Disorder? U.S. Dept. of Veterans Affairs, Mental Illness Research, Education & Clinical Centers (MIRECC) VISN 22.
View at Publisher | View at Google Scholar - Harkavy-Friedman, J. M.; et al. (2004). Suicidal Behavior in Schizophrenia and Schizoaffective Disorder. Suicide and Life-Threatening Behavior; 34(1): 66–76.
View at Publisher | View at Google Scholar - Wy, T. J. P.; Saadabadi, (2023). A. Schizoaffective Disorder. In: StatPearls. Treasure Island (FL): StatPearls Publishing; updated March 27.
View at Publisher | View at Google Scholar - Saljoughian M: (2019) “An Overview of Schizoaffective Disorder”; US Pharmacist; 44(11): 10-12.
View at Publisher | View at Google Scholar
