

Review Article | DOI: https://doi.org/10.31579/2834-5029/035
Prostate Stromal Sarcoma of The Prostate Gland: A Review and Update
- Anthony Kodzo-Grey Venyo *
North Manchester General Hospital; Delaunays Road, Manchester, M85RB. United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital; Delaunays Road, Manchester, M85RB. United Kingdom.
Citation: Anthony Kodzo-Grey Venyo, (2023), Prostate Stromal Sarcoma of The Prostate Gland: A Review and Update, International Journal of Biomed Research. 2(6); DOI:10.31579/2834-5029/035
Copyright: © 2023, Anthony Kodzo-Grey Venyo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 October 2023 | Accepted: 20 November 2023 | Published: 27 November 2023
Keywords: prostate stromal sarcoma; prostatic stromal sarcoma; stump; histopathology; immunohistochemistry; molecular studies; cytogenetics studies; surgery; chemotherapy; radiotherapy; immunotherapy; prostate biopsy
Abstract
Primary prostate stromal sarcoma is ais an uncommon clinical entity which has most often tended with poor prognosis and which most commonly manifests with the development of urinary retention, lower urinary tract symptoms, abnormal digital rectal examination features of the prostate gland, visible haematuria or haematospermia, palpable mass within the rectum in contiguity with the prostate gland, palpable suprapubic mass, loin pain and loin tenderness in males. Primary prostate stromal sarcoma does originate from the mesoderm within the reproductive tract. Risk factors associated with primary prostate stromal sarcoma might be related to previous prostatitis, perineal trauma, previous biopsy of the prostate gland as well as radiotherapy. The sub-types of primary prostate stromal sarcoma include: leiomyosarcoma, rhabdomyosarcoma malignant fibrous histiocytoma and unclassified sarcoma. So far it does appear based upon searching the English literature that less than 40 cases of primary stromal sarcoma of the prostate gland had been reported. The ages of patients who had been reported as having primary stromal sarcoma of the prostate so far have ranged between 14 years and 86 years. Some of the reported manifestations of primary prostate sarcoma include: incidental finding of primary prostate sarcoma in the pathology examination specimen of an individual who has had trans-urethral resection of prostate for lower urinary tract symptoms for a presumed benign prostatic hypertrophy, lower urinary tract symptoms, retention of urine,, urinary tract infection, visible haematuria and or haematospermia, loin pain or back pain, abnormal digital rectal examination finding of prostate mass localized to the prostate or extending into the rectum, a rectal mass, palpable suprapubic mass, at times there may be presentations related to metastasis including the finding of subcutaneous nodules, lung nodules, mass in the liver, or swelling of the lower limbs. The serum prostate specific antigen (PSA) levels of patients who have prostatic stromal sarcoma tends to be low or normal but on rare occasions when there is an associated prostatitis or prostatic abscess or a contemporaneous primary adenocarcinoma of the prostate gland the serum PSA level could be elevated. Radiology imaging scans including ultrasound scan, computed tomography scan and magnetic resonance imaging scan of the prostate gland and pelvis and abdomen would only define features of the prostate lesion but are not utilized to confirm the diagnosis of the sarcoma. Diagnosis of primary sarcoma of the prostate gland is based upon pathology examination features of specimens of the prostate gland that had been obtained from (a) trans-urethral resection of prostate (TURP), (b) Prostate-biopsy, or (c) prostatectomy. Diagnosis of prostate stromal sarcoma tends to be made based upon pathology examination finding of cellular pleomorphism, necrosis, mitotic activity, extension beyond the prostate gland and evidence of metastasis in some cases which distinguishes the sarcoma from its benign simulants. Histopathology examination of specimens of primary prostate sarcoma does tend to demonstrate greater cellularity, mitotic activity, necrosis, as well as stromal overgrowth in comparison with STUMP. Histopathology examination of specimens of primary stromal sarcomas of the prostate gland also do demonstrate storiform as well as infiltrative growth pattern of the tumour. Based upon the microscopy histopathology examination features of sarcomas of the prostate gland, the sarcomas are divided into: low-grade sarcoma and high-grade sarcoma of the prostate gland based upon the mitotic rate of the tumour, necrosis within the tumour as well as the degree of atypia within the tumour. There might be either stromal elements within the tumour with benign glands that simulate malignant breast phyllodes tumours or pure stromal elements within the tumour. Primary stromal sarcomas of the prostate gland upon immunohistochemistry staining studies exhibit positive staining for the following tumour markers as follows: (a) Vimentin (100%), (b) CD34 (100%), (c) progesterone receptor (85% of tumours), Desmin (50%). Prostate stromal sarcomas do exhibit high Ki67 proliferation index stands in comparison with STUMP. Prostate stromal sarcomas of the prostate tend to exhibit negative immunohistochemistry staining for the ensuing tumour markers: (a) smooth muscle actin (33% may be positive, (b) HHF35 (25% may be positive, (c) S100 (100%), ER (usually negative), STAT6. It has been pointed out that with regard to molecular / cytogenetics studies, both primary stromal sarcomas and stromal hyperplasia with atypia (STUMP) do share chromosomal aberrations by array comparative genomic hybridization (aCGH). It had also been iterated that specificity of chromosome 13 and 14 had been questioned and whole exome sequencing had found various changes in STUMP and prostate stromal sarcoma which was interpreted as implying that the two types of tumours represent part of the same spectrum of tumours. With regard to treatment options, it has been pointed out that even though surgery can be undertaken in the treatment of primary prostate stromal sarcoma, surgery alone tends to be inadequate. It has also been pointed out that primary stromal sarcoma does respond to chemotherapy and radiotherapy. Considering the aggressive biological behaviour of majority of primary prostate sarcoma, a multi-disciplinary team approach needs to be discussed including the options of (a) Surgery alone; (b) surgery and a combination of chemotherapy and radiotherapy; (c) surgery and radiotherapy alone; (d) surgery and chemotherapy; (e ) radiofrequency ablation of the primary tumour first to reduce the size of the tumour followed by (a), (b), (c); or (f), cryotherapy of the primary prostate tumour to reduce the size of the tumour followed by (a), (b), (c), or (d); (g) irreversible electroporation of the prostate tumour to reduce the size of the prostate tumour followed by (a), (b), (c), or (d); (h) selective angiography and super-selective embolization of the arterial branch supplying the tumour to shrink the tumour plus (a), (b), (c), or (d); Immunotherapy option also needs to be discussed pursuant to genomic studies undertaken by the multi-disciplinary team to ascertain the molecular genetic changes that had been found. With regard to outcome following treatment, low-grade primary sarcomas of the prostate gland tend to be associated with local invasion and high-grade tumours have tended to be associated with the development of metastasis and aggressive biological behaviour.
Introduction
The prostate stromal tumour does originate from mesenchymal components of the prostate gland. [1] In 1998, prostate stromal was first classified into 2 types by Gaudin et al: [2] including prostatic stromal sarcoma (PSS) and stromal tumours of uncertain malignancy potential. It had been suggested that PSS was especially rare and it only accounts for less than 0.1% of primary prostate malignancies in adults. [1] It had been documented that many scholars had reported that the common symptom of PSS was urinary retention and the prostatic-specific antigen (PSA) in the blood often remains at a normal level.[1] [3] Nevertheless, with the low incidence, the clinical information was still unclear. Considering the fact that primary prostate gland stromal tumours and sarcomas are rare, it would be envisaged or imagined or expected that majority of clinicians globally in all fields of medicine would be unfamiliar with the manifestations, diagnostic features and treatment outcomes of these tumours because they had not encountered a case of primary stromal tumours / sarcomas of the prostate gland during their training and medical practices. In view of this, the ensuing extensive article on prostate stromal sarcomas has been divided into two parts: (A) Overview which has discussed the general aspects of stromal carcinomas and (B) Miscellaneous Narrations Related to Some Case Reports, Case Series And Some Studies Related to Primary Stromal Tumours and Sarcomas of the Prostate Gland in order to illustrate reported manifestations, diagnostic features, Treatment, and Treatment Outcomes as Well as Difficulties that had been encountered by various authors with regard to the diagnosis, and treatment, of their tumours.
Aims
To review and update the literature on prostate stromal sarcomas.
Methods
Internet data bases were searched including: Google; Google Scholar; Yahoo, and PUBMED. The search words that were used included: Prostate stromal tumours; Prostate Stromal Sarcomas; Prostatic Stromal Tumours; Prostatic Stromal Tumours. Eighty one (81) references were identified which were used to write the article that had been divided into two parts: (A) Overview which has discussed the general aspects of stromal carcinomas and (B) Miscellaneous Narrations Related to Some Case Reports, Case Series And Some Studies Related to Primary Stromal Tumours and Sarcomas of the Prostate Gland in order to illustrate reported manifestations, diagnostic features, Treatment, and Treatment Outcomes as Well as Difficulties that had been encountered by various authors with regard to the diagnosis, and treatment, of their tumours.
Results
[A] Overview [4]
Definition / general statements
- It has been pointed out that stromal sarcoma of the prostatic gland or prostatic stromal sarcoma (PSS) is an uncommon entity [4] [5]
- It has also been pointed out that stromal sarcoma of the prostate gland usually manifests with urinary retention; as well as the finding of abnormal prostate gland upon digital rectal examination, haematuria or hematospermia, as well as palpable rectal mass. [4]
- It has been iterated that prostatic stromal sarcoma includes phyllodes tumours which are like phyllodes tumours within the breast) [4] [6]
Essential features [4]
- It has been documented that in stromal sarcoma of the prostate gland cellular pleomorphism does exceeds that of stromal proliferation of undetermined malignant potential (STUMP) [4]
- It has been pointed that in stromal sarcoma of the prostate gland, pathology examination of the prostate specimen containing the stromal sarcoma demonstrates evidence of necrosis. [4]
- It has also been documented that in stromal sarcoma of the prostate gland, pathology examination of the prostate gland specimen does demonstrate evidence of mitotic activity. [4]
- It has been highlighted that in cases of stromal sarcoma of the prostate gland examination does demonstrate evidence of extension outside the prostate gland. [4]
Terminology [4]
It has been highlighted that the ensuing terminologies have been utilized for stromal sarcoma of the prostate gland: [4]
- Phyllodes tumour of the prostate gland,
- Cystic epithelial - stromal tumour of the prostate gland
- Cystadenoleiomyofibroma of the prostate gland.
- Cystosarcoma phyllodes of the prostate gland
Epidemiology
- It has been documented that stromal sarcoma of the prostate gland is very rare and that approximately 30 reported cases of this sarcoma had so far been reported in the global literature. [4] Bearing this in mind, it would be envisaged that majority of clinicians including urologists, general surgeons, pathologists, oncologists in the world, would not have encountered a case of stromal sarcoma of the prostate gland before during their training and clinical experience and hence they would tend to be unfamiliar with the manifestations, diagnostic features, management and outcome following treatment. For this reason, there would the possibility that there might be delay in the diagnosis or misdiagnosis of the sarcoma if the pathologist does not have a high index of suspicion for the sarcoma in order to select appropriate immunohistochemistry studies and genetic testing of specimen of the tumour so as to enable prompt and accurate diagnosis of the sarcoma so as to enable, prompt, accurate and appropriate treatment of the patient / tumour.
- The mean age of patients who had so far been reported to have primary stromal sarcoma of the prostate gland to 54 years, and the ages had ranged between 14 years and 86 years. [2] [4]
- Nevertheless, the documented mean age in 1 study was 37, versus 61 for STUMP [7]
Sites
- With regard to the sites of stromal sarcoma of the prostate gland, it has been iterated that the sarcoma tends to involve the prostate gland as well as the peri-prostatic tissue [7]
Aetiology
- Due to the rarity of stromal sarcoma of the prostate gland, it has been highlighted that the aetiology of the sarcoma has remained unknown [4] This means that clinicians globally should report new cases of stromal sarcoma of the prostate gland and studies of primary sarcomas of the prostate should be undertaken in a multi0centre undertaking.
Clinical features
- The most common manifestation of primary stromal sarcoma of the prostate gland had been iterated to be urinary bladder outlet obstruction, which is followed by the finding of an abnormal digital rectal examination features of the prostate gland, haematuria and rectal fullness [4] [8]
- It has been highlighted that inclusion of phyllodes tumour of the prostate gland as representing primary stromal sarcoma of the prostate gland is justified by its frequent early recurrence, infiltrative growth, extra-prostatic extension and metastatic spread if the tumour is incompletely excised [4] [9] [10] [11] [12]
Diagnosis
- The diagnostic feature upon pathology examination of primary stromal sarcomas of the prostate gland has been summated to include the following: Cellular pleomorphism, necrosis, mitotic activity, extension outside the prostate gland and metastasis which rules out benign mimics and simulators of primary stromal sarcomas of the prostate gland [4]
Laboratory tests
Some of the laboratory tests that tend to be undertaken in the assessment of individuals who have primary as well as secondary / metastatic stromal sarcoma of the prostate gland include the following:
Urinalysis, urine microscopy and culture:
The results would usually tend to be normal but if there is any evidence of urinary tract infection, it would be treated appropriately with utilization of the correct antibiotic sensitivity pattern of the cultured organism to provide effective treatment so as to eradicate the infection as well as to make the individual patient well enough to undergo treatment for his stromal sarcoma of the prostate gland.
Full blood count, INR and Coagulation screen
- Full blood count, INR, and coagulation screen tend to be undertaken as part of the full assessment of patients who have primary or metastatic stromal sarcoma of the prostate gland as general assessment and the results would tend to be normal but if there is any evidence of anaemia or impairment in the INR and coagulation screen, it would be investigated appropriately and the patient would be treated well to be well enough to undergo treatment. If there is evidence of anaemia, then the anaemia would be appropriately treated.
- At times blood for grouping and holding / blood for grouping and crossmatching tends to be undertaken preceding the surgical management of the patient in the case of the undertaking of radical prostatectomy of a localised tumour plus / minus radiotherapy / any other additional treatment.
Routine Biochemistry Analysis
- CRP, Serum urea and electrolytes, liver function tests, Bone profile, and Random Blood Glucose tend to be undertaken and on most occasions the results would be normal; however, if there is any abnormal result, it would be investigated appropriately and effectively treated to improve upon the general condition of the patient.
- Serum prostate specific antigen (PSA) is a usual test that is undertaken in the scenario of lower urinary tract symptoms and the finding of abnormal digital rectal examination features of the prostate gland like irregularity of an area of the prostate, hardness of the prostate, or firmness of an area of the prostate gland which usually tends to be within the normal range and in such situations, the possibility of an unusual cell type of carcinoma of the prostate gland instead of adenocarcinoma of the prostate gland which tends to associated with raised levels of serum PSA should be suspected.
Radiology imaging
Some of the radiology imaging studies that tend to be undertaken in the general assessment of patients who have stromal prostatic sarcomas who manifest with retention of urine, haematuria, and lower urinary tract symptoms and abnormal digital rectal examination features of the prostate gland include:
Ultrasound scan
- Ultrasound scan of the renal tract, prostate, and pelvis as well as trans-rectal ultrasound scan of the prostate gland tend to be undertaken in a number of cases in the initial assessment of patients and ultrasound-guided biopsies which these has tended to be trans-perineal biopsies of the prostate gland including targeted biopsies of abnormal areas of the prostate gland tend to be most often undertaken under antibiotic cover for histopathology examination to minimise or avoid infection instead of trans-rectal ultrasound-guided biopsies of the prostate under antibiotic cover which has tended to be associated with a higher infection rate.
- Within areas of the world, where facilities for computed tomography (CT) scan and /or magnetic resonance imaging (MRI) scan are not available, then ultrasound scan of abdomen and pelvis and chest radiographs tend to be undertaken in the initial assessment as well as follow-up study assessments of patients who have undergone treatment for primary prostatic stromal sarcomas.
Computed Tomography (CT) Scan
- Contrast-CT scan of the prostate gland tends to be undertaken in some areas of the well to assess the prostate gland for the extent of the sarcoma; nevertheless, in well-resourced areas, CT scan has been superseded by the undertaking of contrast-magnetic resonance imaging (MRI) scan of the prostate gland because, MRI scan of the prostate gland does tend to define the features of the prostate gland better than the undertaking of CT-Scan.
- Contrast-Enhanced CT scan of the Thorax, Abdomen, and Pelvis, do tend to be undertaken to establish full radiology image staging of the tumour to ascertain if the tumour is localized, locally advanced or has metastasized.
- Contrast-Enhanced CT scan of the Thorax, Abdomen, and Pelvis, do tend to be undertaken in some parts of the world to establish full radiology image staging of the tumour to ascertain if the tumour is localized, locally advanced or has metastasized. Contrast-Enhanced CT-Scan of thorax, abdomen and pelvis could also be used in the follow-up assessments of patients who have undergone treatment for primary stromal sarcoma of the prostate as part of regular follow-up assessment of patients who have undergone treatment of primary prostatic stromal sarcoma by radical prostatectomy, radiotherapy plus / minus chemotherapy.
Magnetic Resonance Imaging (MRI) Scan
- Contrast-Enhanced Magnetic Resonance Imaging (MRI) scan of the prostate gland tends to be undertaken in some areas of the well to assess the prostate gland for the extent of the sarcoma; nevertheless, in well-resourced areas. MRI scan of the prostate gland does tend to define the features of the prostate gland better than the undertaking of CT-Scan.
- Contrast-Enhanced MRI scan of the Thorax, Abdomen, and Pelvis, do tend to be undertaken in some parts of the world to establish full radiology image staging of the tumour to ascertain if the tumour is localized, locally advanced or has metastasized. Contrast-Enhanced MRI Scan of thorax, abdomen and pelvis could also be used in the follow-up assessments of patients who have undergone treatment for primary stromal sarcoma of the prostate as part of regular follow-up assessment of patients who have undergone treatment of primary prostatic stromal sarcoma by radical prostatectomy, radiotherapy plus / minus chemotherapy.
- It has been pointed out that MRI shows a multi-nodular mass with homogeneous or heterogeneous low signal intensity upon T1 weighted imaging and heterogenous high signal intensity on T2 weighted imaging [13]
Isotope Bone Scan
- Isotope Bone scan tends to be undertaken in the follow-up assessment of patients who have undertaken treatment for primary stromal sarcoma of the prostate gland to ascertain if they have developed bone metastasis or not developed bone metastases.
Positron Emission Tomography – Computed Tomography (PET-CT)-scan
- Positron Emission Tomography – Computed Tomography (PET-CT) scan has tended to be undertaken in well resourced areas of the world to ascertain early recurrence of the sarcoma in order to undertake, prompt treatment before the recurrent tumour becomes big.
- It has been documented that a lesion which became metastatic was distinguished by the finding of intense uptake on 18F-FDG PET imaging [9]
- This high intensity is in contrast to the benign entity of stromal hyperplasia with atypia, also called STUMP
Prognostic factors
Some of the factors of prognostication had been summated as follows: [4]
- It has been pointed out that low-grade stromal sarcoma of the prostate gland could invade locally, whereas high grade stromal sarcoma has the potential to metastasize
- It has been documented that the metastatic sites of primary stromal sarcoma of the prostate gland do include the ensuing sites:
- Lymph nodes [13] [14] [13]
- Liver [15]
- Subcutaneous [14] [16]
- Bones [9]
Treatment
Summations that had been made regarding the treatment of primary stromal prostatic sarcoma include the following: [4]
- It has been pointed out that primary stromal sarcoma of the prostate gland could be managed by the undertaking of robotic procedure (radical prostatectomy) but surgery alone is inadequate [14]] [17] [18 duplication] [19]
Microscopy (histology)examination description
The undertaking of histopathology examination of specimens of the primary prostatic tumour lesion is pivotal to the establishment of primary stromal sarcoma of the prostate gland with supportive immunohistochemistry pathology examination findings as follows: [4]
- Microscopy pathology examination of specimens of the prostatic tumour depicts: Greater cellularity, mitotic activity, necrosis and stromal overgrowth than STUMP
- Microscopy pathology examination of specimens of the prostatic tumour depicts: Storiform and infiltrative growth pattern of the prostatic tumour.
- It has been pointed out that sarcomas
- are subdivided into low grade and high grade based upon mitotic rate, necrosis and degree of atypia seen upon histopathology examination of the tumour [8]
Immunohistochemistry staining study features
Positive staining
It has been pointed out that primary stromal tumours of the prostate gland upon immunohistochemistry staining examination demonstrate the ensuing positive staining features: [4]
- Vimentin (100%).
- CD34 (100%).
- Desmin (50%)
- Positive High Ki67 proliferation index strands in contrast to STUMP. [20]
Negative staining
It has been pointed out that primary stromal tumours of the prostate gland upon immunohistochemistry staining examination demonstrate the ensuing positive staining features:
- Smooth muscle actin (33% may be positive).
- HHF35 (25% may be positive)
- S100 (100% negative)
- ER (Oestrogen receptor usually negative)
- STAT6 [20]
Molecular / cytogenetics study description
- It has been iterated that both prostatic stromal sarcoma (all 4 cases) and stromal hyperplasia with atypia (also termed STUMP) (7 of 8 cases) examined had shared chromosomal aberrations by array comparative genomic hybridization (aCGH) and that [4]
- The most common was loss of chromosome 13 followed by losses of chromosomes 14 or 10 [15]
Specialized stromal tumours of the prostate encompass stromal sarcoma and stromal tumours of uncertain malignant potential (STUMP). The molecular signature associated with stromal sarcoma and STUMP has not been unravelled. The study was conducted to detect the chromosomal imbalances in stromal sarcoma and STUMP by using array comparative genomic hybridization (aCGH). The study consisted of two cases of stromal nodule, eight cases of STUMP (three degenerative atypia type, three myxoid type, one hypercellular type, and one phyllodes type), and four cases of stromal sarcoma, including a distant metastasis developed metachronously after a primary stromal sarcoma of the prostate. DNA was extracted from the representative paraffin-embedded formalin-fixed specimens and was submitted for aCGH. All stromal sarcomas and seven STUMPs revealed chromosomal aberrations. Overall, the most common alteration was loss of chromosome 13 (10 cases), followed by loss of chromosome 14 (9 cases), and loss of chromosome 10 (7 cases). Except one stromal sarcoma, which showed a distinct chromosomal profile of multiple amplifications, other stromal sarcomas showed a similar pattern to those of STUMP. Stromal sarcoma and STUMP shared similar profiles of chromosomal imbalances. From a molecular genetic perspective, the recurrent chromosomal alterations support the concept of specialized stromal tumours of the prostate as a distinctive tumour entity.
- Additional mutations, such as CHEK2 and KTM2D, had favoured benign entities, whereas TP53 and RB1 mutations had favoured malignant [15]
- This had suggested 2 separate entities; nevertheless, either mutations or rearrangements were found via DNA sequencing in 10 of 10 cases of both STUMP and PSS, while only PSS included phyllodes pattern [21] [22]
Differential diagnoses
The differential diagnoses of primary stromal sarcoma of the prostate gland had been summated to include the ensuing: [4]
- Stromal hyperplasia with atypia which is also referred to as STUMP:
- Stromal hyperplasia is more common than stromal sarcoma
- In Stromal hyperplasia there is no marked atypia or necrosis
- In stromal hyperplasia, there is presence of degenerative nuclei
- Leiomyoma of the prostate gland
- Leiomyoma of the prostate gland is much more common in comparison with primary stromal sarcoma of the prostate gland.
- Leiomyoma of the prostate gland consistently exhibits positive immunohistochemistry staining for smooth muscle markers
- In leiomyoma of the prostate gland, CD34 upon immunostaining studies is negative
- Synovial sarcoma of the prostate gland:
- This is ruled out if CD34 immunohistochemistry staining is positive
- Gastrointestinal stromal tumour of prostate gland:
- This is ruled out if the prostate lesion exhibits negative CD117 immunohistochemistry staining.
[B] Miscellaneous Narrations and Discussions from Some Case Reports, Case Series and Studies Related to Primary Stromal Sarcoma of the prostate Gland.
Ren et al. [3] described the imaging features and the correlation with clinical findings of adult prostate sarcoma. Ren et al. [3] undertook a retrospectively analysed radiological data of seven adult male patients who had prostate sarcoma, documented by pathological examination of specimens. Ren et al. [3] correlated the radiological features of the prostate tumours with clinical and pathological findings. Ren et al. [3] summarized the results as follows: The mean age of the study population was 45.8 years and the ages of the study population had ranged between 21 years and 76 years. The mean value of the serum prostate specific antigen (PSA) in seven patients was 1.59 ng/ml and the serum PSA levels had ranged between 0.735 / ng/ml and 3.72 ng/ml. Five patients had leiomyosarcomas and two had rhabdomyosarcomas. The most common symptom was urinary obstruction in 7 cases and the most common sign was the markedly enlarged prostate as revealed by digital rectal examination in 7 cases. The mean size of the tumours was 8.7 x 7.2 x 7 cm and the size of the tumour had ranged from 6.5 x 5x 6.5 to 12.1 x 10.2 x 8.9 cm. The tumours were noted to be round in 4 cases, lobular in 2 cases, or irregular in 1 case. Two tumours had occupied the majority of the prostate and five had occupied the entire prostate gland. The tumour reported by Ren et al. [3] appeared as a homogeneous mass, and six tumours contained cystic areas on computed tomography (CT) and magnetic resonance imaging (MRI). The tumours had enhanced avidly on contrast-enhanced CT in 5 cases and on MRI scan in 2 cases. Magnetic resonance spectroscopy (MRS; in 2 cases showed the ratio of choline:citrate to be 1.6 and 10.75. Tumour invasion was present in the urinary bladder in 3 cases and rectum in 1 case. Ren et al. [3] made the ensuing conclusions:
- Adult prostate sarcoma was characteristically shown to be a large and heterogeneous mass with rapid, hyper-vascular and heterogeneous enhancement upon CT scan and MRI scan.
- The main MRS feature was a marked increase in the choline:citrate ratio.
- The clinical manifestations had corresponded mainly to local mass effects and tumour invasion.
Cavaliere et al. [18] in 2014, reported the first case of PSS occurring in an adolescent who was 14-years old. There was evidence of a good response to chemotherapy including ifosfamide, doxorubicin, vincristine and actinomycin-D, although the final outcome was dismal. They reviewed the English literature and their review revealed 14 additional patients with PSS treated with chemotherapy: tumour shrinkage was reported in 4 of the 6 evaluable patients. They stated that patients with PSS might benefit from the use of chemotherapy in combination with early aggressive local treatment. Cavaliere et al. [18] stated that prostatic stromal sarcoma (PSS) is a rare tumour that normally occurs in adult age. Its management relies mainly on surgery. They had reported the first case of PSS occurring in an adolescent. There was evidence of a good response to chemotherapy including ifosfamide, doxorubicin, vincristine and actinomycin-D, although the final outcome was dismal. A review of the English literature revealed 14 additional patients with PSS treated with chemotherapy: tumour shrinkage was reported in 4 of the 6 evaluable patients. Patients with PSS may benefit from the use of chemotherapy in combination with early aggressive local treatment.
- Other treatment options that could be utilized for the management of primary localized stromal carcinoma of the prostate gland include:
- Cryotherapy of the localized prostate tumour plus radical radiotherapy alone of plus / minus chemotherapy.
- Radiofrequency ablation of the prostatic stromal sarcoma alone or plus radiotherapy alone or plus chemotherapy
- Irreversible electroporation of the primary stromal sarcoma of the prostate alone or plus radical radiotherapy alone or plus chemotherapy alone or plus chemo-radiotherapy.
- Selective angiography of the prostatic artery plus super-selective embolization of the arterial branch of the prostatic artery supplying the localized stromal sarcoma of the prostate gland alone or plus radical radiotherapy alone or plus chemotherapy alone or plus chemo-radiotherapy.
- Treatment of metastatic disease upon the establishment of metastases utilizing radiology imaging and the undertaking of genomic / genetic testing to identify genetic deletions and mutations could guide oncologists and pharmacology research workers to consider utilization of immune modulation treatment options in a global multi-centre treatment trial.
Kim et al. [22] stated that rhabdoid tumours had been reported in many different anatomic sites as an aggressive-tumours and usually they present with a rhabdoid tumour components: a composite tumour, rather than a pure rhabdoid tumour. Rhabdoid tumour within the prostate gland had been described only once in the prostatic region as a possible epithelial origin. Rhabdoid features in prostatic stromal sarcomas (PSSs) had never been described in the literature. Kim et al. [22] reported a case of a PSS with rhabdoid features. Kim et al. [22] reported a 31-year-old man who had presented with a 4-month history of voiding difficulty and anal pain. He had computed tomography scan of the abdomen which revealed an ovoid mass in his prostate gland invading his rectum and urinary bladder. A needle biopsy of the prostate gland lesion was undertaken and pathology examination features of the biopsy specimen was diagnosed as an unclassified spindle cell sarcoma, and 2 cycles of adriamycin-based neoadjuvant chemotherapy were given, followed by radical prostatectomy. The prostatectomy specimen upon pathology examination revealed a high-grade sarcoma with fascicles of highly cellular spindle cells and numerous mitoses with haemorrhage and necrosis. In areas, the tumour also contained sheets of loosely cohesive epithelioid cells with rhabdoid tumour component. Both spindle and rhabdoid tumour cells were upon immunohistochemistry staining studies were positively stained for vimentin, CD34, and progesterone receptor and negatively stained for desmin and cytokeratin. The rhabdoid tumour cells retained INI1 expression. The tumour had recurred in his urinary, and the patient died of sepsis. Kim et al. [22] stated that to the best of their knowledge, their reported case was the first case of PSS with rhabdoid features. The tumour demonstrated an aggressive clinical and biological behaviour with a short-term survival of 7 months after the diagnosis.
Ueda et al. [23] stated that sarcomas and related proliferative lesions of the specialized stroma of the prostate are very rare and they had been classified into prostate stromal sarcoma (PSS) and prostatic stromal tumour of uncertain malignant potential based upon histology features of the tumour. Ueda et al. [23] reported a case of PSS. They reported a 40-year-old male, who had presented at a hospital with urinary distention. He had magnetic resonance imaging (MRI) scan which revealed a large prostate mass, and the diagnosis was prostate sarcoma of uncertain differentiation by ultrasound-guided needle biopsy. The patient underwent total pelvic exenteration and a pathological diagnosis of PSS was ultimately reached. Ten months later, there had been no signs of metastasis or recurrence.
Wickramasinghe et al., [16] stated the following:
- Prostatic stromal sarcomas do account for about 0.1% of all prostatic malignancies.
- Local recurrence into the urinary bladder, seminal vesicles and rectum had been documented.
- Distal metastasis, had up to the time of their case had been reported in lung and bone.
Wickramasinghe et al. [16] reported the case of a 42-year-old man with a subcutaneous metastatic deposit of a prostatic stromal cell sarcoma 5 years after he had undergone radical prostatectomy. He had additional staging with computed tomography (CT) scan and PET-scan which showed lymph node involvement in his neck and left axilla. A core biopsy of the skin lesion was undertaken, of which the histology examination of the specimen revealed a low-grade spindle cell tumour that was morphologically identical to his previously diagnosed prostatic stromal sarcoma. Wickramasinghe et al. [16] stated that inn literature distant metastases to the lung and bone had been documented before. They also stated that their reported case was the first documented case of a subcutaneous metastasis of prostatic stromal cell sarcoma. Wickramasinghe et al. [16] made the following conclusions:
- The preferred treatment for prostatic stromal cell sarcoma is surgery by radical prostatectomy or cystoprostatectomy.
- There was at the time of the report of their case, not enough literature on the topic to elucidate the role of chemo- or radiotherapy in loco-regional or distant spread.
Morikawa et al. [24] reported a unique case of prostatic stromal sarcoma (PSS) which had recurred in the pelvic cavity with massive high-grade prostatic intraepithelial neoplasia. Morikawa et al. [24] reported a 52-year-old man, who had manifested with urinary retention and who underwent a radical cystoprostatectomy. Pathology examination of the surgical specimen showed that the tumour tissues of the prostate demonstrated an admixture of hyperplastic glands and markedly cellular stroma of spindle cells which were arranged in a fascicular pattern, and the tumour was diagnosed as PSS. 66 months after the operation, he had CT scans which revealed three recurrent tumours around the bilateral obturator and left iliopsoas region. The recurrent tumours were found upon pathology examination to be biphasic neoplasms, as before, but the epithelial component had grown prominent and manifested overt atypia in a manner simulating high-grade prostatic intraepithelial neoplasia. Morikawa et al. [24] iterated that their findings had indicated that not only the stromal component but also and the epithelial components of PSS may have malignant potential.
Hicks et al. [14] stated that primary prostate sarcomas are rare, and they reportedly comprise just 0.7% of all prostate malignancies. Hicks et al. [14] reported the case of a 66-year-old man who was diagnosed with prostate stromal sarcoma after he had undergone a routine transurethral resection of prostate for bladder outflow obstruction. Hicks et al. [14] made the ensuing iterations:
- Primary prostate sarcoma could be aggressive even when the tumour is low-grade, with a high risk of local recurrence and, high malignant potential when high-grade.
- They require aggressive multimodality treatment with the undertaking of surgery, chemotherapy and radiotherapy for durable survival outcomes.
- They also do require close surveillance with long-term follow-up.
- It is also worth pointing out that primary localized stromal sarcoma of the prostate gland can be treated by the undertaking of open radical prostatectomy in areas of the world where robotic surgery service is not available or there is no one trained to undertake robotic surgery.
- It has furthermore been pointed out that primary stromal sarcoma tumour of the prostate gland does respond to chemotherapy and radiotherapy [18]
- They also require close surveillance with long-term follow-up.
Zamparese et al. [25] stated that primary sarcoma tumours of the prostate gland are rare and they are classified, according to their histology, as stromal tumours of uncertain malignant potential (STUMP) and stromal prostatic sarcoma (PS; low and high grade). Zamparese et al. [26] reported a case of a 71-year-old man who had developed progressive urinary obstruction symptoms and who was subjected to a transurethral prostatic resection (TURP). Histopathology examination of the resected prostate chips demonstrated evidence of a diffuse proliferation of epithelioid and spindle cells that showed rare atypical mitotic figures. Immunohistochemistry staining studies of the tumour specimens showed that, the tumour cells had expressed diffusely CD34 and focally progesterone whereas no immunoreactivity was seen for cytocheratin, desmin, S-100, Bcl-2, chromogranin, CD117, and actin smooth muscle. A final diagnosis of low-grade prostatic stromal sarcoma (LG-PS) was made. Zamparese et al. [26] stated that prostatic stromal sarcoma is a really rare neoplasm; in the literature, and in fact, to their knowledge, only 6 cases had been described before the report of their case and all of these were alive and free of disease at follow-up. Their reported patient too was free of disease at 15 months from the diagnosis.
Choi et al. [17] stated that stromal sarcoma of the prostate is very rare and shows rapid growth, which consequently is related to poor prognosis and that they had recently treated two cases of prostatic stromal sarcoma: one with robot-assisted laparoscopic radical prostatectomy and the other with open radical cysto-prostatectomy with an ileal conduit. To the best of their knowledge, this was the first case report of a prostatic stromal sarcoma managed by use of a robotic procedure. They had reported their experiences in the treatment of prostatic stromal sarcoma by use of two different methods.
Herawi et al. [8] stated that specialized stromal tumours of the prostate gland encompass stromal sarcoma and stromal tumours of uncertain malignant potential (STUMP). As a result of their relative rarity and lack of long-term follow-up, the prognosis of STUMP is unclear. Herawi et al. [8] studied 50 cases of STUMP and stromal sarcoma with regard to their clinical presentation and follow-up. The ages of the patients had ranged from 27 years to 83 years and their mean age was 58 years. The major presenting signs and symptoms were urinary obstructive symptoms in 25 cases, abnormal digital rectal examination findings in 15 cases, haematuria in 7 cases, hematospermia in 1 case, and rectal dysfunction/fullness in 3 cases. An elevated serum prostate-specific antigen (PSA) level was either the sole or a compounding rationale for initial urological examination and prostate biopsy in a subgroup of patients in 11 cases. The histology in the 36 cases of STUMP were not associated with sarcoma were as follows: 25 composed of stroma with scattered cytologically atypical cells associated with benign glands; 8 resembling glandular-stromal hyperplasia but with hypercellular stroma; 6 with extensive myxoid stroma; and 1 with phyllodes pattern. Four of these cases had mixed patterns. Seven cases of STUMP were associated with sarcoma, either concurrently or subsequently. In another 7 cases, pure sarcomas were found: 3 low grade (LG) and 4 high-grade (HG). In 19 STUMPs, the location of the lesion was determinable: 10 cases arose in the peripheral zone, 7 cases were located in the transition zone, and 2 cases seemed to involve both zones. In 3 of these cases, the tumours were adherent to the rectum at the time of resection. There was no evidence of progression of disease for 14 STUMPs after biopsy, TUR, or enucleation where follow-up ranged from 0.3 to 14 years (mean 4.9 years). Five cases of STUMP showed local tumour growth: 1 case had increased in size from 6 cm to 7.5 cm in 3 years and 4 cases had recurred frequently necessitating multiple TURs of the prostate (n=2, n=3, n=3, n=3) over 1.1, 2, 7, and 8 years, respectively. Fourteen patients who had STUMP had undergone radical prostatectomy (RP) soon after the diagnosis; of these, 12 were organ confined where the tumour size had ranged from 0.7 cm to 7.5 cm with a mean tumour size of 2.7 cm; 2 cases with a history of a 28 grams TUR and a 275 grams enucleation showed no residual tumour in the RP specimen. Three cases were lost to follow-up. The histological subtypes of STUMP did not correlate with the clinical behaviour or likelihood of being associated with sarcoma. Two of the LG sarcomas locally invaded around the seminal vesicle, yet all of the LG sarcomas with follow-up were free of disease at 3, 13, 24, 25, 30, and 36 months. Of the 6 HG sarcomas with follow-up, 3 were free of disease at 3 months, 17 months, and 72 months. One man was alive with metastasis to the lung 10 months after Radical Prostatectomy, 1 man was alive at 280 months with multiple metastases, and another died of disease at 115 months. STUMPs can recur frequently, occur at a young age, they often involve the peripheral zone where they could be adherent to the rectum requiring its removal, and could be associated with stromal sarcoma. Even though STUMPs could be histologically misdiagnosed as nodular hyperplasia, it is important to recognize that these are neoplasms with unique local morbidity and malignant potential. Whereas LG stromal sarcomas can locally invade, HG sarcomas can metastasize and lead to death.
- It has been pointed out that microscopy pathology examination of the primary stromal sarcoma of prostate may either demonstrate either stromal elements with benign glands simulating malignant breast phyllodes tumours or pure stromal elements
- Xu et al. [19] stated the following:
- Mesenchymal tumours of the prostate gland are rare; however, they encompass a wide differential diagnosis.
- They had undertaken a study, which was aimed to investigate the clinicopathological features that could be used to differentiate malignant solitary fibrous tumours (mSFTs) occurring in the prostate gland from prostatic stromal tumours.
Xu et al. [19] identified a total of 15 patients with mesenchymal tumours of the prostate gland in Nanjing Drum Tower Hospital from 2009 to 2019, including 3 mSFTs, 9 stromal tumours of uncertain malignant potential (STUMPs), and 3 prostatic stromal sarcomas (PSSs). Xu et al. [20] performed immunohistochemistry staining studies for signal transducer and activator of transcription 6 (STAT6), aldehyde dehydrogenase 1 (ALDH1), CD34, desmin, smooth muscle actin (SMA), progesterone receptor (PR), CD117, and cytokeratin (CK) on representative sections from each tumour, and the clinical features, histology, and immunophenotype of these three groups were analysed. Xu et al. [20] reported that there was no significant difference in the mean patient age of patients who were diagnosed with mSFTs, STUMPs, and PSSs. mSFTs and PSSs had shown significantly increased tumour size (p < 0>
Pan et al. [15] stated the following:
- Specialized stromal tumours of the prostate gland encompass stromal sarcoma and stromal tumours of uncertain malignant potential (STUMP).
- The molecular signature associated with stromal sarcoma and STUMP had not been unravelled.
Pan et al. [15] undertook a study in order to detect the chromosomal imbalances in stromal sarcoma and STUMP by utilizing array comparative genomic hybridization (aCGH). The study had consisted of two cases of stromal nodule, eight cases of STUMP (three degenerative atypia type, three myxoid type, one hypercellular type, and one phyllodes type), and four cases of stromal sarcoma, including a distant metastasis developed metachronously after a primary stromal sarcoma of the prostate gland. DNA was extracted from the representative paraffin-embedded formalin-fixed specimens and it was submitted for aCGH. Pan et al. [15] reported the following results:
- All stromal sarcomas and seven STUMPs demonstrated chromosomal aberrations.
- Overall, the commonest alteration was loss of chromosome 13 (10 cases), followed by loss of chromosome 14 (9 cases), and loss of chromosome 10 (7 cases). Except one stromal sarcoma, which showed a distinct chromosomal profile of multiple amplifications, other stromal sarcomas showed a similar pattern to those of STUMP.
- Stromal sarcoma and STUMP had shared similar profiles of chromosomal imbalances.
- From a molecular genetic perspective, the recurrent chromosomal alterations support the concept of specialized stromal tumours of the prostate as a distinctive tumour entity.
- Additional mutations, such as CHEK2 and KTM2D, had favoured benign entities, whereas TP53 and RB1 mutations had favoured malignant [20]
- This had suggested 2 separate entities; nevertheless, either mutations or rearrangements were found via DNA sequencing in 10 of 10 cases of both STUMP and PSS, while only PSS included phyllodes pattern [21]
- Acosta et al. [20] stated the following:
- Tumours of purported specialized prostatic stromal origin comprise prostatic stromal sarcomas (PSS) and stromal tumours of uncertain malignant potential (STUMP).
- Previous studies had described their clinicopathologic characteristics, however, the molecular features had remained incompletely understood. Furthermore, these neoplasms are morphologically heterogeneous and the lack of specific adjunctive markers of prostatic stromal lineage make precise definition more difficult, leading some to question whether they represent a specific tumour type.
Acosta et al. [20] undertook a study, in which they used next-generation DNA and RNA sequencing to profile 25 primary prostatic mesenchymal neoplasms of possible specialized prostatic stromal origin, including cases originally diagnosed as PSS (11) and STUMP (14). Morphologically, the series comprised 20 cases with solid architecture (11 PSS and 9 STUMP) and 5 cases with phyllodes-like growth pattern (all STUMP). Combined DNA and RNA sequencing results had demonstrated that 19/22 (86%) cases that underwent successful sequencing (either DNA or RNA) had harboured pathogenic somatic variants. Except for TP53 alterations (6 cases), ATRX mutations (2 cases), and a few copy number variants (-13q, -14q, -16q and +8/8p), the findings were noted to be largely non-recurrent. Eight gene rearrangements were noted, and 4 (NAB2-STAT6, JAZF1-SUZ12, TPM3-NTRK1 and BCOR-MAML3) were found useful for reclassification of the cases as specific entities. Acosta et al. [20] stated that their study had shown that mesenchymal neoplasms of the prostate gland are morphologically and molecularly heterogeneous and they include neoplasms that harbour genetic aberrations that are seen in specific mesenchymal tumours arising in other anatomic sites, including soft tissue and the uterus. They also iterated their data had suggested that tumours of purported specialized prostatic stromal origin might perhaps not represent a single diagnostic entity or specific disease group and that alternative diagnoses should be carefully considered.
Acosta et al. [20] also iterated the following:
- It was also stated that it was also reported that the specificity of chromosome 13 and 14 had been questioned and whole exome sequencing found a variety of changes in STUMP and PSS, implying these 2 entities are part of the same spectrum [21]
Yang et al. [1] reported a 49-year-old man, who had been admitted to the local hospital 2 months preceding the report of his case due to his having repeated dysuria, and he accepted to be catheterized and upon his catheterization then, liquid yellow urine had been drained and he was given antibiotic therapy until his urinary catheter was removed 7 days subsequently. He was admitted to the hospital with a manifestation of visible haematuria which had commenced 9 days preceding his admission. He did not have any pain, fever, or abdominal distension when he was suffering from his urinary tract symptoms. He was found to be stable during his initial assessment and his examination was generally unremarkable. The results of his blood analysis demonstrated an increase in his eosinophil count, and all of his other blood routine indexes were within the normal limits. His serum PSA level was 0.64 ng/mL which was within normal range (<4>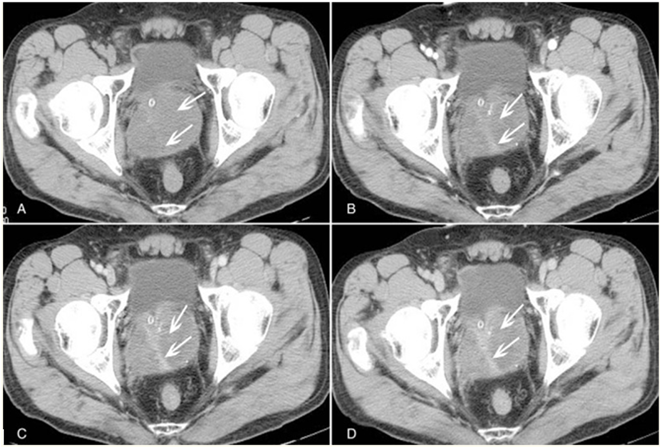
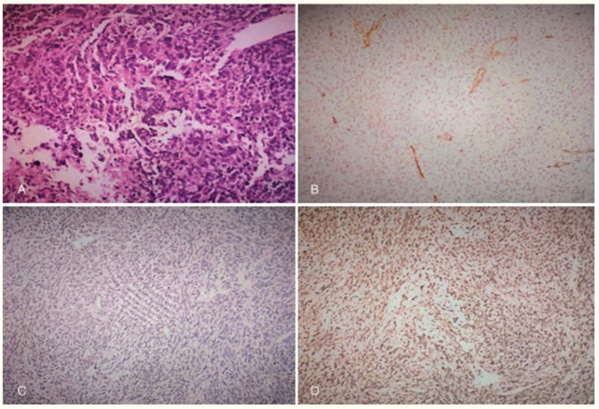
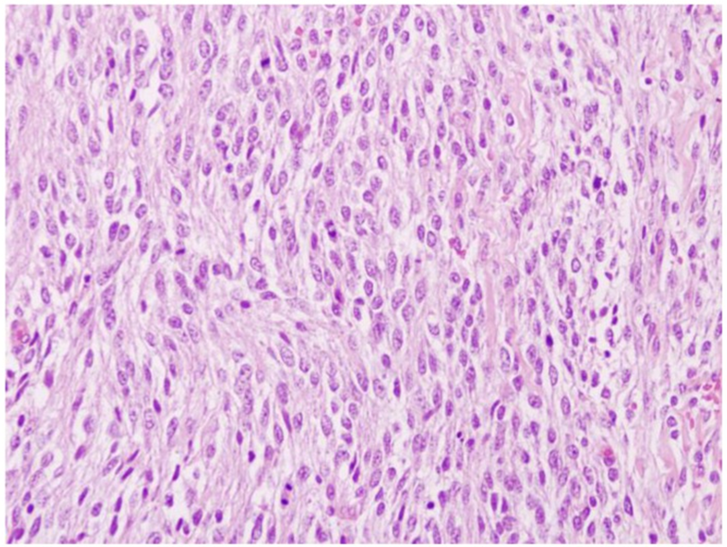
His CT scan examination did not demonstrate any other adjacent organ-invasion or enlarged lymph node. Since he did not have any surgical contraindication, he was advised to undergo radical prostatectomy in consideration of the inefficacy of conservative treatment. His operation was undertaken via a midline incision within his lower abdomen. Macroscopically, the prostate was found to be enlarged and it had slightly squeezed the urinary bladder, and an oval, soft tumour with smooth surface was visible within the prostate gland, there was no obvious synechia between the tumour and his normal prostate tissue. Microscopy pathology examination of the prostatectomy specimen showed that the tumour was growing with invasive potential, there were abundant heteromorphic interstitial cells with pleomorphic shapes and increased nucleocytoplasmic ratio (see Figure 2A). Combined with the immunohistochemistry staining features of the tumour which had demonstrated positive staining for vimentin (see Figure 2B,), PSA and CD34 were negative (see Figure (Figure 2C, and 2D), the final diagnosis of prostate-specific stromal sarcoma was made definitely based upon the basis of the histopathological features of the tumour.
His post-operative recovery was unremarkable. His retropubic drainage tube was removed 3 days pursuant to his surgery and his urinary catheter was removed 7 days after his operation. The importance of follow-up had been emphasized in case of recurrence and lymph node metastasis, while unfortunately there were no further follow-ups the hospital up to the time of publication of the case and hence his long-term outcome was not available to be reported or discussed.
Yang et al. [1] made the ensuing detailed summating discussions:
- It had been documented that primary prostate sarcoma is a rare malignancy of the prostate with poor prognosis. [22] [25] [26]
- Stromal sarcoma of the prostate gland does originate from the mesoderm in the reproductive tract, and its risk factors might be related to prostatitis, perineal trauma, previous prostate biopsy, and radiation induced. [27]
- The subtypes of prostate sarcoma do include: leiomyosarcoma, rhabdomyosarcoma, malignant fibrous histiocytoma, and unclassified sarcoma.
- Among the above-mentioned subtypes of prostatic sarcoma, rhabdomyosarcoma, which is mostly with high malignancy, is the most common histological subtype which does account for about 40% of prostate sarcoma in children.
- The secondary sub-type is leiomyosarcoma which accounts for about 25% and this mostly occurs in the elderly with a slightly lower degree of malignancy.
- Unclassified sarcoma can be further divided into primary stromal sarcoma (PSS) and stromal tumours of uncertain malignancy potential upon the basis of the invasive area of mesenchyme and mitosis, as well as the extent of mesenchyme overgrowth. [2] [28] [29] [30]
- To the best of their knowledge, since the first case of PSS was reported in 1998, there had been about 30 reports up to the time of the report of their case. [22] [24] [31] [32] [33] [34]
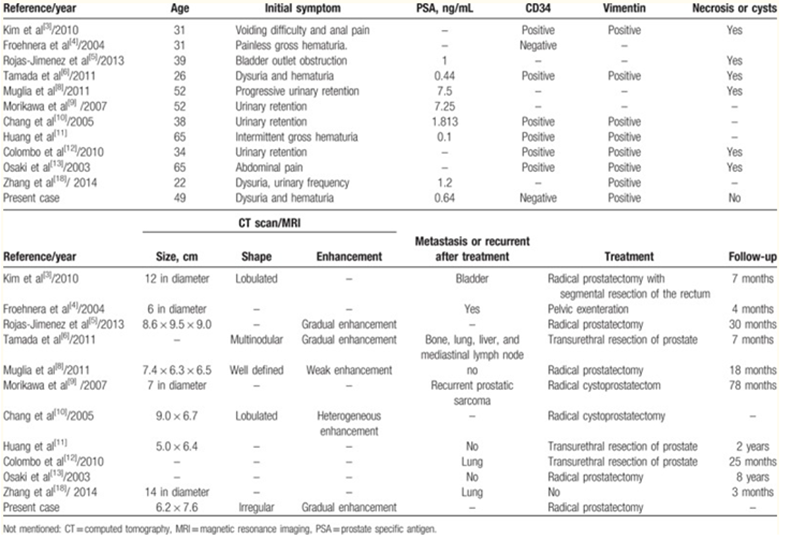
They had made a conclusion about some previous cases with detailed information, and their case was also included in the tabulation of their findings from the review of the reported cases (see Table 1). Among the twelve cases of PSS, patients’ age had ranged between 22 years and 65 years of age, the median age was 38.5 years of age. The vast majority of initial manifesting symptoms were urinary retention and/ haematuria, except only 1 patient who had the first manifesting complaint of anal pain and another patient of abdominal pain. [34] Except for 2 cases and one of which was about recurrent prostatic sarcoma, PSA levels of all other patients in the Table (Table1) were within the normal ranges. With regard to the immunohistochemical staining studies, PSS were typically positive for vimentin and CD34; nevertheless, 2 cases that included their reported case had exhibited negative staining for CD34, [27] [28] which meant that immunohistochemistry does give an important reference significance for diagnosing PSS, however, it cannot be an exclusive-diagnostic criteria.
- It has been documented that there are no specific manifestations of PSS, and patients normally present with dysuria, urinary retention, haematuria at the late stage but they tend to have no symptom during early stage. [26]
- In view of the lack of typical clinical symptoms, the tumour has tended to be easily overlooked or misdiagnosed as benign prostatic hyperplasia, therefore, in many cases the prostate was found to be significantly enlarged when the tumour was diagnosed, for example, in their reported case the size of the tumour was 6.22 cm × 7.64 cm, and it had occupied the majority of the prostate gland, which had indicated that the patient was in a serious condition, therefore early detection is vital to the patients with PSS.
- Upon trans-rectal ultrasound scan, a markedly enlarged volume and irregular margins are important characters of prostate sarcoma [35] in addition, trans-rectal ultrasound scan is usually utilized to guide a biopsy of the prostatic lesion to confirm the diagnosis.
- Unenhanced CT scan often tends to demonstrate an enlarged, well or ill-defined prostate gland, the shape of the tumour might be round, lobular, or irregular, [36] normally necrosis and cystic changes in the tumour are common because of the high malignancy and rapid growth, but there are no evidence of cystic changes on unenhanced CT.
- Limited published data related to the CT enhancement characteristics of the adult prostate sarcoma had shown that the tumours had a heterogeneous enhancement or delayed enhanced compared with the normal prostate tissue, whereas the necrosis and cystoids areas were unenhanced thus tend to be obvious, indicating rapid and hyper-vascular enhancement of these tumours. [3] [36]
- The radiology imaging features of magnetic resonance imaging (MRI), such as a large size, irregular margins and heterogeneity, are similar to those of transrectal ultrasonography and CT, besides that, the peripheral solid part of the lesion had shown a slightly hyperintense on T1WI and T2WI, a hyperintense on DWI. The centric part of the lesion presents as a hypointense on T1WI, T2WI, and diffusion-weighted imaging; in addition, it has an advantage in detecting metastatic lesions and revealing the adjacent structures, which could show clearer than CT findings. PET/CT is not sensitive to prostate sarcoma, because it is a qualitative analysis method based upon the uptake of glucose in tumours, very limited literature had been reported which had compared imaging with FDG-PET, PET/CT improves especially in the lesion localization as well as characterization. [27] [37]
- When the tumour is too large, it might invade the adjacent tissues and organs, and the urinary bladder and rectum are the most vulnerable organs, once the tumour is involved in the urinary bladder and rectum, it could emanate in the development of symptoms such as abdominal pain and frequent urination [31] [38]
- Early metastases are not rare in those PSS patients, and the most common site is lung metastasis.
- In their reported case, their patient had neither metastasis nor lower abdomen pain and this might be due to the disease duration that was short and the tumour was also not too large. [39]
- Macroscopy examinations does tend to indicate that PSS could be solid or mixed with cystic areas, necrosis, and haemorrhage might also occur especially in high-grade tumours. Unexpectedly, size is not related to tumour grade and the prognosis, because tumours are graded based upon the degree of cellular atypia.
- Microscopically, PSS is typified by proliferation of spindle and ovoid stromal cells, some of which poses atypical nucleus and necrotic focuses.
- Immunochemically, PSS normally exhibits expression of a positive staining for: vimentin, CD34, and progesterone receptor, but not for oestrogen receptors.
- It had also been reported that in majority of cases of PSS, a significant increase in the Ki-67 labelling index had been observed if a high grade of intraepithelial neoplasia is associated with the tumour. [27] [33]
- Surgical resection remains the mainstay treatment of prostate sarcoma, including radical prostatectomy, cystoprostatectomy, and total pelvic exenteration; nevertheless, except for metastatic lesions.
- Even though, it is still unclear whether treatment with adjuvant radiotherapy and chemotherapy does improve patients’ survival, they are needed to prevent local relapse and distant metastasis.
- In their reported case, a radical prostatectomy without radiotherapy or chemotherapy had been undertaken and the operative effect was good.
- Differentiating between prostate sarcoma and other prostatic disorders is quite important since there is difference between their treatments and prognoses.
- The differential diagnoses of prostatic stromal sarcoma should include: carcinoma of prostate gland, benign prostatic hyperplasia (BPH), and abscess of the prostate, they share similar clinical manifesting symptoms, but their radiology imaging characteristics do vary.
- Carcinoma of Prostate gland often does occur within the peripheral zone of the prostate gland, with a lower density than the normal prostate tissue, CT scan shows an uneven enlargement of the prostate gland or nodular protrusion in the prostate gland. The hyper-vascular nodules are demonstrated clearly upon enhanced CT; however, the density is still lower than normal prostate tissue.
- The MRI detection and display of carcinoma of prostate gland are mainly based upon T2WI, which mainly manifested as a hypointense defect area in the peripheral zone, where it is significantly different from hyperintense of normal prostate tissue in peripheral zone. [40] [41] Nevertheless, CT imaging and MR imaging alone are not sufficient to identify prostate sarcoma, clinical information should also be taken into account.
- Prostate carcinoma used to appear mostly in the aged people with obviously increased serum PSA levels, while PSS mostly affects the younger age with normal levels of serum PSA, simply because PSA is produced by prostate epithelial cells, while sarcoma originates from stromal cells.
- BPH occurs in elderly men, the radiology imaging differences from prostate sarcoma are that BPH patients show an evenly enlarged prostate gland with even density. On MRI, T2WI clearly shows that BPH is the hyperplasia of the central zone of the prostate, while the peripheral zone of the prostate is thinned by the extrusion of hyperplasia, besides, pseudo-capsule can be seen in hyperplasia.
- For prostate abscess, there are different manifestations on MRI among the prostate abscess wall, abscess cavity and the separations in the cavity. On T1WI, both the prostate abscess cavity and the separations in the cavity depict hypointense features, and the wall of the prostate abscess shows hyperintense features, the prostate abscess cavity shows hyperintense features on T2WI, on dynamic contrast-enhanced MR, abscess border and partitions in the cavity show apparently enhancement. [42] In addition, patients who have prostate abscess often have fever and shiver, which should not be overlooked when making the differential diagnosis, since prostate sarcoma and prostate cancer patients do not present these symptoms.
They had made the ensuing conclusions:
- Adult prostatic stromal sarcoma is rare and high aggressive malignant tumour.
- Even though the clinical manifestations of prostatic stromal sarcoma are unspecific, radiology imaging results may provide a clue for discovering the tumour and distinguishing it from other similar lesions before surgery.
- When an adult male shows the same CT or MRI findings as mentioned above, and symptoms like dysuria, haematuria, PSS should be taken into consideration.
Rojas Jimenez et al. [27] stated the following:
- Adult prostatic stromal sarcoma is a rare malignant tumor.
- The main manifesting symptom is urinary retention secondary to bladder outlet obstruction.
- Serum Prostatic Specific Antigen level could be normal.
- Radiology imaging features demonstrate a prostate mass with or without pelvic organ invasion depending on the aggressiveness of the tumor.
- They had reported a patient with prostatic stromal sarcoma who debuted with urinary obstruction, leukocytosis and neutrophilia, prostate enlargement, and hypodense prostate areas on CT images, simulating prostatitis with abscess formation
Rojas Jimenez et al. [27] reported a 39-year-old patient presented at the emergency room with bladder outlet obstruction (BOO). He did not have any history of urinary tract infection, urinary lithiasis, trauma/congenital urethral anomalies, or other symptoms suggestive of genitourinary pathology. He underwent digital rectal examination (DRE) which revealed a palpable, painful, and tumescent prostatic mass. The results his blood tests had indicated leukocytosis (16.06 × 103 cells/μl; normal range is 3.5–10.8 × 103 cells/μl) and neutrophilia (87.6; normal range is 1.3–8.0 × 103 cells/μl). All hemocultures and urine cultures were negative, and the Prostatic Specific Antigen (PSA) level was 1 ng/ml (normal PSA < 4>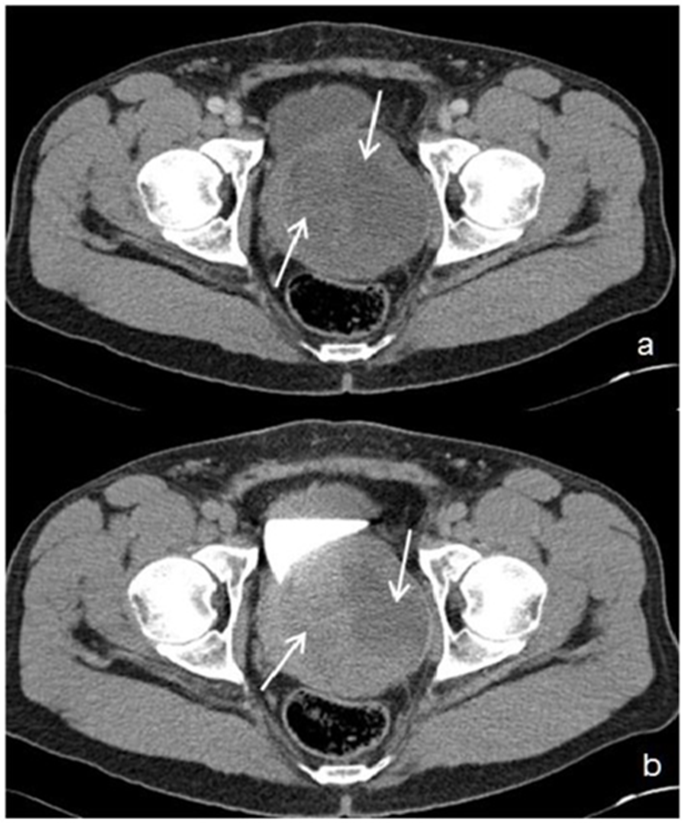
In the portal phase - Figure 3a: axial image, demonstrates an enlarged (8.6 cm × 9.5 cm in the latero-lateral, antero-posterior diameters, respectively), and heterogeneous prostate gland, with low contrast enhancement and central hypodense areas (white arrows). During the excretory phase (Figure 3b: axial image), the prostatic mass displaces the bladder and the left ureter, and contacts the anterior face of the rectum, displacing it discreetly backwards. No lymphadenopathy or metastases were visible in the rest of the abdomen. Reproduced from [27]
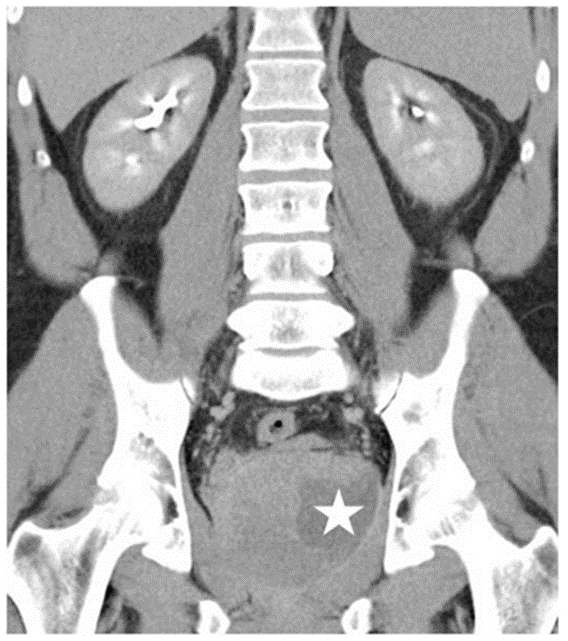
Coronal Multiplanar Reformatted Image (MPR) (5 mm thickness) in the excretory phase demonstrates delayed contrast enhancement in the prostate gland and cystic areas (white star) with slight peripheral rim enhancement. Reproduced from [27]
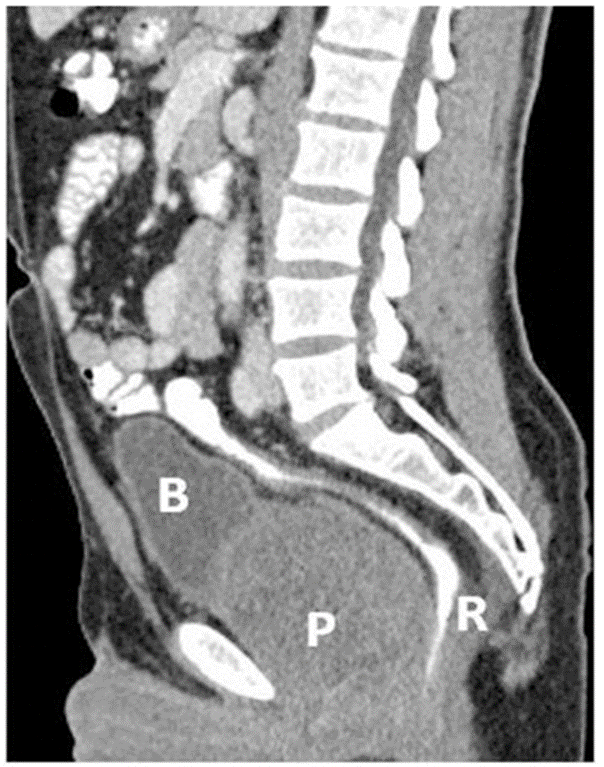
Sagittal image (MPR) (5 mm thickness) in the portal phase shows an increased (9 cm in the sagittal diameter) prostate gland (P) that displaces the rectum (R) backwards and the bladder (B) upwards. Reproduced from [27] Figure 5: 39-year-old male patient with stromal prostatic sarcoma. CT (16 Multidetector Somatom Sensation 16 - Siemens Medical Systems, Forchheim, Germany), technique: single-bolus 2-phase protocol (portal and excretory phases at 70 s and 600 s delays, respectively, from the start of contrast material injection, (100 ml of 320 mgI/ml Optiray™ 320-Ioversol, Covidien, Spain) with the following acquisition parameters: 150 effective mAs, 120 kV, 2 mm with 1mm reconstruction increment slice thickness.
Sagittal image (MPR) (5 mm thickness) in the portal phase shows an increased (9 cm in the sagittal diameter) prostate gland (P) that displaces the rectum (R) backwards and the bladder (B) upwards. Reproduced from [27]
With regard to treatment, he received analgesic and antibiotic. Despite leukocytosis and neutrophilia, the patient did not demonstrate any other clinical features of either prostatitis or prostatic abscesses, since his blood and urinary cultures were negative. 48 hours after his admission and pain relief, a TRUS-guided prostate biopsy was undertaken and the histological sampling of prostate needle biopsy specimens was prostatic sarcoma.
The patient underwent radical cystoprostatectomy and ileal conduit derivation without pelvic lymphadenectomy (see figure 6). The final histopathology diagnosis was prostatic stromal sarcoma (PSS) with infiltration of the prostate capsule, without infiltration of the urinary bladder and rectum (see figure 7). There were also areas of necrosis and interstitial haemorrhage. The patient continued to demonstrate no evidence of relapse 30 months after his surgical intervention.

Axial image after radical cystoprostatectomy, shows bowel loops occupying the pelvic space with left colostomy (yellow arrow), and right ileal conduit (white arrow and arrowheads). Reproduced from [27]
Reproduced from [27]
Rojas Jimenez et al. [27] made the ensuing summating discussions:
- Urinary bladder outlet obstruction (BOO) is a blockage which slows or stops urine flow out of the urinary bladder.
- Chronic urinary bladder outlet obstruction causes urinary bladder stones, infection and damage to the bladder and kidneys.
- Benign prostatic hyperplasia (BPH) is the leading cause of BOO in aging men (> 50).
- Causes of BOO in young men do include urethral stricture secondary to urethral injury or surgery, dysfunctional voiding, neurogenic-based detrusor-sphincter dyssynergia (DSD), and primary bladder neck obstruction. In these cases, the prostate gland does not demonstrate enlargement unlike BPH. Scarring of the urinary channel (urethra) or bladder neck, as a result of injury, surgery, or lower urinary tract infection is the leading cause of BOO in young men. [42]
- Even though, their patient had manifested with BOO, the presence of leukocytosis and neutrophilia in a young man, made the diagnosis of an inflammatory/infectious disease more probable. However, young men rarely develop urinary tract infections.
- In male children, infections do occur in patients who have complicating factors, including: abnormal anatomy, voiding disorders, or urinary tract instrumentation. In contrast, ii has been iterated that clinical series had suggested that few healthy young men manifesting with acute urinary tract infections had anatomical or functional urinary tract abnormalities. [43] Previous prostate biopsy and prior fluoroquinolone intake are significant risk factors for the development of BOO behind a rising incidence of acute prostatitis. [44]
- Based upon the National Institutes of Health (NIH) prostatitis classification, Category I has been defined as follows: “Patients with acute bacterial prostatitis manifest with acute symptoms of a urinary tract infection characteristically including urinary frequency and dysuria. Some patients do have symptoms that are suggestive of systemic infection, such as malaise, fever, and myalgias. Bacteriuria and pyuria are related to infection of the prostate and bladder”. Category II has been defined like chronic bacterial prostatitis with recurrent infection of the prostate. Category III has been defined as chronic nonbacterial prostatitis or chronic pelvic pain syndrome, where there is no demonstrable infection by conventional microbiologic techniques. Category IV is an asymptomatic inflammatory prostatitis, where there are no subjective symptoms, but white blood cells are found in prostate secretions or in prostate tissue during an evaluation for other disorders. [45]
- It has been pointed out that prostatic abscesses are uncommon in clinical practice because early antibiotic therapy has reduced complications of prostatitis. Prostatic abscess mainly does tend to affect diabetic, immunosuppressed patients, and old patients with pre-existent chronic obstructive troubles or urinary episodic inflammation. [46] Escherichia coli (E. Coli) is the causative organism in most of the cases of acute prostatitis, post-biopsy prostatitis (E. Coli with a high rate of fluoroquinolone resistance), and prostatic abscesses. [43], [44], [45], [46]
- With regard to their patient, since blood and urinary cultures were negative, a TRUS-guided prostate biopsy was necessary to establish the correct diagnosis.
- With regard to prostate tumours, the most frequent tumour is prostate adenocarcinoma. Adenocarcinoma of the prostate gland does account for 95 percent of all prostate cancers. The risk for the development of adenocarcinoma of the prostate gland rises steeply with age, and about three-quarters of all cases occur in men aged 65 years or older than 65 years of age. With the introduction of serum PSA screening, increased detection of preclinical disease was allowed. It has been pointed out that Serum PSA tends to be elevated beyond the arbitrary cut-off point of 4.0 ng/ml in the majority of patients with prostate cancer. [47] [48] Most adenocarcinomas of the prostate gland are asymptomatic and detected upon serum PSA screening and prostatic biopsy, by (TRUS)-guided biopsy and more recently, by magnetic resonance imaging (MRI)-guided biopsy [49] [50]
- TRUS is primarily utilized to direct the biopsy needle to desired anatomic locations of the prostate gland to estimate the volume of the prostate gland and to assist in sampling prostate tissue in a spatially systematic way, however, it is not reliable in differentiating normal prostate gland from cancer tissue, and up to 40% of cancers are missed by TRUS. Adenocarcinomas of the prostate gland are located within the peripheral and posterior zone; nevertheless, it can extend or arise within the transitional zone. Contrast-enhanced colour Doppler radiology imaging and contrast-enhanced ultrasound scan, is a promising tool since it takes advantage of the difference in the microvasculature between areas of prostate cancer and benign prostate tissue. [51] [52]
- CT has does have low sensitivity to detect and stage prostate cancer due to the fact that it does not provide sufficient soft-tissue contrast beyond size assessment of the prostate gland. Even though CT scan is valuable in the evaluation of pelvic lymphadenopathy and bone metastases, MR scan imaging and bone scanning had been found superior in their assessment. [52] [53] [54] MRI and MRI-spectroscopy is a valuable method for the detection and staging of prostate cancer. An increase in the choline-to-citrate ratio or the (choline + creatine)/citrate ratio is often utilized as a marker of malignancy in prostate cancer and increases the specificity of diagnosis; nevertheless, it is most reliable in the peripheral zone [52] [55] [56] Diffusion-weighted MRI (DWI), and dynamic contrast-enhanced MRI (DCE-MRI), had been investigated for potential to complement T2-weighted MRI in improving prostate cancer localization. DWI is based upon the diffusion properties of water within tissue. Regions of prostate cancer do demonstrate increased cell density and reduced apparent diffusion coefficient (ADC) relative to normal prostate gland. DCE-MRI scan does measure tumour vascularity. After injecting a gadolinium chelate contrast agent, areas of hyper-vasculature such as prostate cancer show rapid enhancement and early washout of signal intensity. Nevertheless, some prostate cancers are not detectable by this method because of low vascularity. It has been documented that combining DCE-MRI with T2-weighted MRI improved prostate cancer detection and staging accuracy. [52] [55] [57]
- Nuclear medicine (Fluorine-18-labeled FDG-PET and 11C and 18F choline and acetate PET/CT) methods are increasingly being utilized for radiology imaging of prostate cancer. PET/CT, in comparison to FDG-PET, does improve especially the lesion localization as well as characterization. On the contrary, FDG-PET does have a limited value when the lesion is close enough to a hot source such as urinary bladder due to isotope shine through [58]. At the time of publication of their article, [(11) C]-choline PET/CT had not been recommended in the primary setting but it may be used in clinically suspected prostate cancer with repeatedly negative prostate biopsies, in preparation of a focused re-biopsy [52] [59]
- Prostatic urothelial carcinoma does represent 0.7–2.8% of prostatic tumours in adults. Majority of the patients do have the same age range as urinary bladder urothelial carcinoma (45–90 years). In patients who have invasive urinary bladder carcinoma, there is involvement of the prostate in up to 45% of cases. The prostate gland is a rare site of extra-nodal lymphoma and only a few cases had been reported. Out of patients who have chronic lymphocytic leukaemia, 20% had been reported to have prostate involvement at autopsy. The most presenting frequent symptoms had been those related to lower urinary obstruction. Metastatic tumours do tend to arise outside of the prostate gland and they do spread to the gland by vascular channels, since contiguous spread from other pelvic tumours into the prostate gland does not constitute a metastasis. Metastases from lung, skin (melanoma), gastrointestinal tract, kidney, testis and endocrine glands had been reported. Lung is the commonest primary site of metastases to the prostate gland. It had been pointed out that direct spread of urinary bladder carcinoma is the commonest secondary prostatic tumour. [47]
- Primary prostate sarcomas are not common. Rhabdomyosarcoma is the commonest tumour of the lower genitourinary tract in the first two decades of life and it represents 5% to 10% of malignant solid tumours of childhood. PSS are uncommon mesenchymal tumours, representing less than 0.1% of primary prostate malignancies in adults [47]. The patient age ranges from 25 years to 86 years, and one half of these patients are younger than 50 years [59] The common clinical manifestation of adult prostate sarcoma is urinary retention, haematuria or hematospermia, and a palpable rectal mass. Serum PSA levels are usually normal. [2] [24] [33] [47] See table 1.
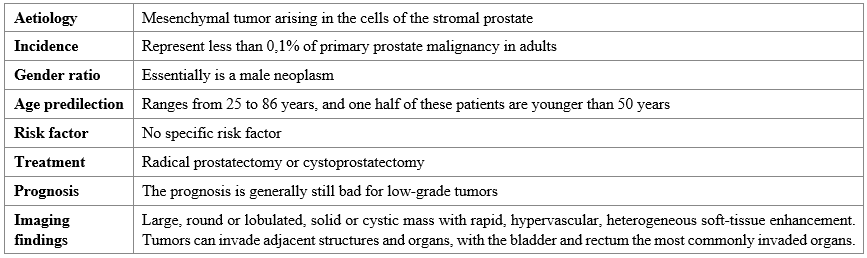
PSS was formally described by Gaudin et al. in 1998 [2] This tumour originates in the cells of the stromal prostate. The current World Health Organization classification characterizes this tumour as a distinctive spindle cell neoplasm. [47] The term “stromal tumours of uncertain malignant potential” (STUMP) was coined in recent years to describe a proliferation of stromal cells that is behaviourally and histologically distinct from benign hyperplasia and whose behaviour cannot be predicted by histological appearance. Gaudin et al. identified four distinct STUMP types based on their histological pattern and degree of atypia. Stromal sarcoma may arise de novo or coexist with pre-existent or concurrent STUMP, suggesting a potential for STUMP to dedifferentiate into stromal sarcoma. A literature review of patients younger than 40 years identified only 21 stromal prostatic tumours from 1977 until 2010. [2] [33]
Macroscopically, PSS can be solid or mixed with cystic areas. Necrosis and haemorrhage may also occur, especially in high-grade tumours. Size varies (2–18 cm) in the reported cases; interestingly, size does not correlate with the grade or clinical behaviour of the tumour. The tumour tends to occupy the majority of or the entire prostate. Microscopically, PSS is characterized by proliferation of spindle and ovoid stromal cells, some of which poses atypical nuclei, scattered mitotic figures, and necrotic foci. PSS is divided into low-grade and high-grade tumours based on moderate to high cellular atypia and hypercellularity in high-grade tumours. Immunochemically, this neoplasm expresses a positive progesterone receptor, and occasional cases have exhibited oestrogen-receptor positivity. CD34 and Vimentin are both expressed diffusely, and in most cases a marked increase in the Ki-67 labelling index is observed if a high grade of intraepithelial neoplasia (PIN) is associated with the tumour. [33] [47]
- Up to the time of publication of the article, majority of reports had been based upon histological characteristics of the tumour, and limited published data had been available regarding the CT or MRI characteristics of PSS. The published cases had described a large, round or lobulated, solid or cystic mass with rapid, hyper-vascular, heterogeneous soft-tissue enhancement [3]. CT scan in their reported patient had shown an enlarged prostate gland with little enhancement and hypodense areas with peripheral rim enhancement on the excretory phase, mimicking a prostatic abscess formation (figures 1, ,2,2, and and3).3). Pathology analysis had revealed that these hypodense areas were areas of necrosis, a probable cause of the observed low contrast material enhancement, leucocytosis and neutrophilia. They had not found published data regarding this unusual clinical manifestation of prostate sarcoma. The authors had tabulated examples of detailed differential diagnosis between PSS and other prostatic entities, in table 2.
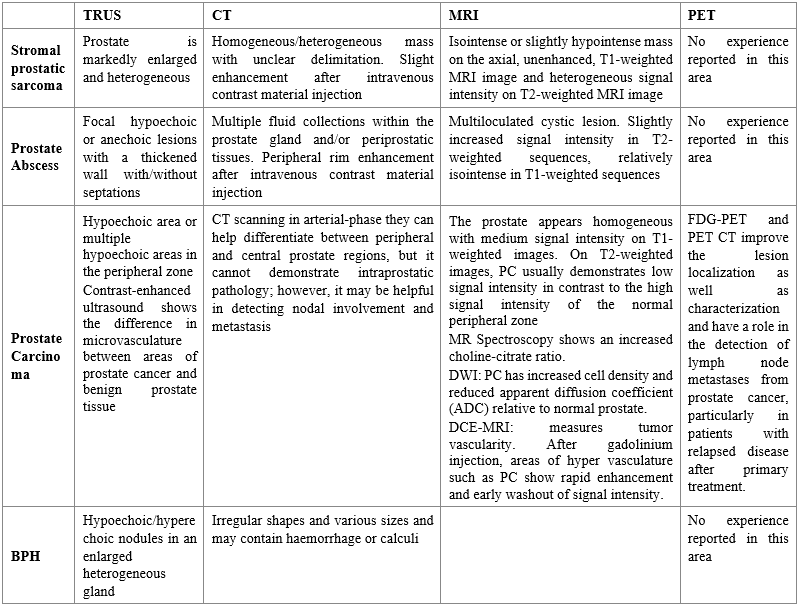
TRUS: Transrectal Ultrasound, CT: Computed Tomography, MRI: Magnetic Resonance Imaging, PET: Positron Emission Tomography, BPH: Benign prostatic hyperplasia, PC: Prostate carcinoma, ADC: apparent diffusion coefficient, DCE-MRI Dynamic-contrast enhanced MRI, FDG-PET: Fluorine-18-labeled PET, PET/CT: 11C and 18F choline and acetate PET/CT. Reproduced from: [27]
- Tumours could invade adjacent structures and organs, with the urinary bladder and rectum the most commonly invaded. No published case had included pelvic lymphadenopathy on CT and MRI as demonstrated by operation and pathology, and thus pelvic lymphadenectomy is not routinely undertaken. [3] [33]
- A poor prognosis still does tend to accompany low-grade prostate sarcoma tumours, that have a high prevalence of spreading to the seminal vesicles, urinary bladder, and rectum. Surgical margins are sometimes difficult to obtain due to involvement of adjacent structures by the tumour. Vascular invasion of the tumour and metastases to the liver and lung had also been reported in high-grade sarcomas. Treatment has been based on radical prostatectomy or cystoprostatectomy, and there was no current data regarding the effectiveness of chemotherapy or radiotherapy [47]
Rojas Jimenez et al. [27] highlighted their teaching as follows:
- Sarcoma of the prostate gland should be included in the differential diagnosis of a prostatic mass with heterogeneous or low enhancement of the contrast material, and clinical symptoms of inflammatory prostatic disease, in a young patient with normal PSA levels.
Yamazaki et al. [60] stated the following:
- Prostatic stromal sarcoma is a fairly rare tumour which constitutes about 0.1% to 0.2% of all prostatic cancers.
- Detailed characteristics of the tumour are still unclear due to its rarity.
Yamazaki et al. [60] reported a case of prostatic stromal sarcoma in a 63-year-old man who had suffered from urinary obstructive symptoms. He underwent palliative transuterine resection and the preliminary histopathology examination-based diagnosis was neuroendocrine carcinoma. After he had received chemotherapy, total pelvic exenteration was undertaken. Histopathology examination of the surgically excised specimen showed that, the tumour was composed of monotonously proliferating small to medium-sized round cells, which existed in compact islands with loose or dense fibrovascular networks. Immunohistochemically, the tumour cells were noted to be widely positively stained for vimentin, CD56, CD99 and focally positively stained for synaptophysin, CD10, progesterone receptor, desmin and CD34, but negatively stained for EMA, cytokeratin, oestrogen receptor, S-100 and myoglobin. Yamazaki et al. [60] made the ensuing summating iterations:
- Majority of the previously reported tumours had exhibited positive immunohistochemistry stainability for CD10 and progesterone receptor.
- In addition to these tumour markers, immunohistochemistry expressions of CD56, CD99 and synaptophysin were characteristically detected in their reported case.
- To the best of their knowledge, they had presented the first case of prostatic stromal sarcoma with characteristic immunohistochemical staining properties.
- Even though the biological characteristics of this rare tumour had not yet been elucidated, these findings had suggested that prostatic stromal sarcoma can potentially exhibit neuroectodermal differentiation.
Yamazaki et al. [60] iterated the ensuing:
- It has been documented that prostatic stromal sarcoma (PSS) is a fairly rare tumour, which does constitute about 0.1% of all prostatic cancers. [61] [62]
- It has been pointed out that prostatic sarcoma and related proliferative lesions, including prostatic phyllodes tumours, had been classified as prostatic stromal tumours of uncertain malignant potential (STUMP) and prostatic stromal sarcoma (PSS) based upon their cellularity, mitotic index, cellular atypia and necrosis (WHO 2004). [63]
- Some STUMP had been reported as malignant transformation into PSS. [64]
- There had not yet been a clear differentiation between PSS and STUMP in view of the rarity of these tumours.
- In their article, prostatic stromal sarcoma had potentially neuroectodermal characteristics.
Ding et al. [65] stated they had assessed the effects of clinical factors and treatments on the overall survival (OS) of patients with prostate sarcomas.
Ding et al. [65] reported 41 cases that were diagnosed with prostate sarcomas from eight hospitals in China and they had retrospectively analyzed the prognostic factors by combining their data with cases from five previously published cohorts, including one extra Chinese cohort and four cohorts from United States of America (US) cohorts. Additionally, Ding et al. [66]] investigated the differences in treatment regimens between China (n = 66) and the USA (n = 74). Ding et al. [65] summarized the results as follows:
- The median survival time of the 41 cases was 18.6 months (95% confidence interval [CI]: 13.9–23.2).
- The status of negative distant metastasis (P = 0.004) and radical tumor resection with negative margin (P = 0.001) were found to be significantly associated with better overall survival, whereas age, tumor size, duration of initial symptoms, and chemo/radiotherapy were not significantly related to OS.
- The survival time was found to be longer in patients with who had rhabdomyosarcoma in comparison with those who had leiomyosarcoma (P = 0.049).
- Combined analysis of their current and 5 prior cohorts had shown that more patients in the US cohorts had undergone underwent radical surgery (P = 0.005), and the overall survival was better among those who had undergone radical cyst prostatectomy in comparison with those who had undergone radical prostatectomy alone (P = 0.008).
Ding et al. [65] concluded that radical resection undertaken to achieve a negative margin contributes to better survival for patients with prostate sarcoma.
Addesso et al. [66] stated that common prostatic neoplasms are diagnosed frequently, whereas rare entities require particular awareness and special clinical management. Addesso et al. [66] reported a 31-year-old man, who had manifested with dysuria, haematuria and urinary retention. Histomorphology analysis of material obtained by transurethral resection of his prostate gland had initially favoured a sarcomatoid carcinoma, but immunohistochemistry allowed the correct diagnosis of sarcoma of the specialized stroma of the prostate to be confirmed. Addesso et al. [66] made the ensuing summating discussions:
- The patient had refused to undergo surgical treatment and, despite chemotherapy, he died 8 months after his diagnosis.
- They had highlighted the diagnostic and therapeutic challenge of prostatic stromal sarcoma by illustrating their case and they had reviewed the relevant literature.
Addesso et al. [66] concluded that even though rare and shadowed by more common neoplasms that may simulate it, prostatic stromal sarcoma should be considered in the differential diagnosis of bladder and prostate neoplasms because of its dismal prognosis.
Tamada et al. [67] stated that prostatic stromal sarcoma (PSS) is quite rare. Tamada et al. [67] described magnetic resonance imaging (MRI) features of a PSS identified in a 26-year-old man with dysuria and haematuria. MRI clearly depicted the extent and multinodular appearance of the tumour, which was mainly located in the central zone of the prostate. The tumour appeared as a heterogeneously signal-hyperintense mass with a pseudo-capsule on T2-weighted imaging. Contrast-enhanced T1-weighted MRI showed necrotic portions in the gradually enhanced solid mass, and diffusion-weighted imaging permitted the accurate assessment of the local extent of the tumour. Hence, the appearance on MRI was quite different from that of adenocarcinoma of the prostate. Index terms: Prostatic stromal sarcoma; Prostatic neoplasms; Magnetic resonance (MR); Diffusion magnetic resonance imaging; T2-weighted imaging, dynamic contrast-enhanced MRI
Mao et al. [13] reported a rare case of prostatic stromal sarcoma (PSS) which was treated with a robot assisted laparoscopic radical prostatectomy (RLRP). Mao et al. [13] reported a 32-year-old man who had presented to the Department of Urology, The First Affiliated Hospital, School of Medicine, Zhejiang University (Hangzhou, China) with obstructive voiding symptoms which had persisted for 2 years. He had a computed tomography (CT) scan of the pelvis which showed an 8 cm prostatic mass protruding into his bladder. He underwent a trans-perineal ultrasound guided prostate biopsy and pathology examination of the biopsy specimen revealed a diagnosis of PSS. An RLRP was undertaken, and neither chemotherapy nor radiotherapy were administered prior to or subsequent to the surgery. No recurrence of the tumour was found at 6 months post surgery. Mao et al. [13] stated that to the best of their knowledge, less than 30 cases of PSS had been reported in the English literature, and their reported case was only the second case to be treated with RLRP.
Hodotsuka et al. [68] stated that prostatic stromal sarcoma is an extremely rare malignancy of the prostate with a poor prognosis. Hodotsuka et al. [68] reported a- 65-year-old man who had presented with dyschezia, and he had computed tomography which showed a large prostate mass. The diagnosis was prostate stromal sarcoma by transrectal needle biopsy. He had magnetic resonance imaging which had suggested rectal infiltration. The patient underwent 4 courses of neoadjuvant chemotherapy with gemcitabine and docetaxel hydrate followed by total pelvic exenteration. Hodotsuka et al. [68] made the ensuing conclusions:
- No recurrence has occurred at 5 years after the surgery.
- Their reported case was the first report of complete resection in prostate stromal sarcoma after neoadjuvant chemotherapy with gemcitabine and docetaxel hydrate.
Chang et al. [69] stated that prostate stromal sarcoma is quite rare, comprising only 0.1–0.2% of all prostate cancers. Chang et al. [69] reported one case of prostate stromal sarcoma in a 38-year-old man. Initially, the patient had suffered from lower urinary tract symptoms, and he had intravenous pyelography which showed a larger filling defect within his urinary bladder. He had trans-rectal ultrasound scan which demonstrated a huge heterogenous mass between his urinary bladder and rectum. He had abdominal computed tomography scan which showed a prostate tumour with local invasion. He underwent radical cystoprostatectomy with ileal conduit and pathology examination of the surgical specimen revealed high-grade prostate stromal sarcoma with invasion to the right seminal vesicle and urethra.
Ruihe and Chongyang [70] stated the following:
- Primary prostatic stromal sarcoma is an extremely rare disease that predominantly occurs in adults, accounting for only 0.1% of all prostate cancers.
- Prostatic stromal sarcoma is quite aggressive and has the ability to spread to lung, liver, bone, and other organs.
- Metastasis is one of the most important predictors for prognosis.
The authors. [70] reported a case of a 17-year-old adolescent boy who was diagnosed with primary prostatic stromal sarcoma through prostate biopsy, and the stage of the tumour was confirmed by 18F-FDG PET/CT.
Li and Huang. [71] reported a 34-year-old man who referred to their hospital to address a 2-month history of visible haematuria and progressive dysuria. He had Pelvic computed tomography scan which demonstrated a 6.0 cm × 5.2 cm × 7.2 cm mass in his prostate gland, with bladder invasion. The patient underwent transurethral prostatectomy as upfront therapy. He refused further treatment and died of uncontrollable tumour growth 3 months following his surgery. Pathology examination of the prostate specimen revealed the stroma to be pleomorphic, with a huge number of atypical spindle cells. Rhabdomyoblastic cells, with abundant eosinophilic cytoplasm, were identified. The spindle cells exhibited positive staining for vimentin, INI1 and β-catenin, and the rhabdomyoblastic cells exhibited were positive staining for MyoD1, myogenin and INI1. The spindle cells and epithelial cells had sporadically exhibited positive staining for P53. Li and Huang. [71] concluded that the prostatic stromal sarcoma tumour was immunoreactive for β-catenin, suggesting a role for the Wnt/β-catenin pathway in this tumour type.
Chan et al. [72] stated the following:
- Stromal tumour of uncertain malignant potential (STUMP) is exceedingly rare.
- Diagnosis and management of STUMP present a challenge to the urologist due to the absence of specific clinical findings and its unpredictable clinical course. Hence, radical resection is often recommended.
Chan et al. [72] reported a case of a 64-year-old male, who presented with mild obstructive voiding symptoms with a raised age-specific prostate-specific antigen (PSA) of 3.1. Magnetic resonance imaging (MRI) showed an area of suspicion, in an area thought to be the left seminal vesicle, containing a malignant lesion within it. Biopsy of this area and the prostate confirmed concurrent prostatic STUMP and Gleason 3+3=6 adenocarcinoma of the prostate, managed with robotic-assisted laparoscopic radical prostatectomy with wide local excision.
Gonzalez et al. [73] stated the following:
- Prostate tumours represent the most frequent malignancy in men.
- Epithelial lesions are frequent, whereas malignancies of mesenchymal origin represent only 1-2 % of all prostatic malignant tumours. They are little known, mostly those of stromal origin.
Gonzalez et al. [73] reported a case of a 77-year- old man who had prostatic stromal sarcoma to whom partial exeresis was performed. The tumour was reported to have practically occupied the totality of the pelvic abdominal cavity, and it had a diameter of 35 cm and a weight of 3 800 g. Histologically, it was recognized as prostatic sarcoma even though an evident link with this organ was not found during the transoperatory. Gonzalez et al. [73] also made the ensuing iterations:
- The clinical behaviour of these tumours, based on the little cases described in the literature, is practically unknown and its preoperative diagnosis becomes difficult.
- The patient had manifested with weight loss, he did not have any pain, haematuria, or obstructive symptoms.
Kwak et al. [74] stated that prostatic stromal tumour of uncertain malignant potential (STUMP) is a rare neoplasm with distinctive clinical and pathological characteristics. Kwak et al. [74] reported a case of laparoscopic radical prostatectomy performed in a patient with prostatic STUMP. Kwak et al. [74] stated that in their reported case, the patient had suffered from LUTS, which had occurred at a younger age than would be expected for typical benign prostatic hyperplasia. TRUS of the prostate gland had demonstrated the increasing size of the lesion which had originated from the peripheral zone of the prostate gland. The age of the patient was an important factor in their decision to undertake radical surgery to differentiate a prostatic lesion from a prostatic sarcoma,
Mazron et al. [75] reported a case of neglected atypical high grade prostatic stromal sarcoma (PSS) at the transitional zone, which had invaded the peripheral zone, prostatic capsule as well as the peri prostatic fat reaching to pelvic side wall, and which had demonstrated T2WI hyperintense signal (compared to typical cases of PSS showing T2WI hypointense signal) corresponding to developing on top of pre-existing nodular hyperplasia. Mazron et al. [75] iterated the following:
- Careful reviewing of prostatic central / transitional zone lesions is mandatory especially at T2WI, diffusion & contrast images to exclude malignancy which could be easily missed due to multiple signal patterns described.
- Most common tumours within the transitional zone of the prostate gland is stromal sarcoma which could be typical showing T2 hypointense signal or atypical showing T2 hyperintense signal intensity.
Segawa et al. [76] stated that prostatic stromal sarcoma (PSS) is an unusual lesion which had been reported only occasionally. Seqawa et al. [76] reported a case of prostatic stromal sarcoma in a 33-year-old man who had complained of perineal pain. His serum prostate-specific antigen (PSA) level was above the normal limit at 5.8 ng/ml, and he had abdominal computed tomography (CT) scan which had revealed a giant mass in the retro-vesical region. He had Chest CT scan which demonstrated lung metastases. He had transrectal needle biopsy of the prostate gland and pathology examination of the biopsy specimen suggested a mesenchymal tumour, but a precise diagnosis required a larger specimen. Palliative transurethral resection (TUR-P) was undertaken because of obstruction of the urogenital tract, and the final diagnosis was made from this specimen. The tumour contained yellowish gelatinous materials, and the stromal element appeared histologically malignant, with increased cellularity, mitotic figures and pleomorphism. The histology examination diagnosis was PSS, and the patient received VIP (etoposide, ifosfamide, cisplatin) chemotherapy regimen. Nevertheless, the pelvic mass continued to increase in size, and the patient's condition rapidly deteriorated and he died. Segawa et al. [76] stated the following:
- Sarcoma of the prostate gland showing aggressive biological behaviour is quite rare.
- The detailed histological and immunohistochemical findings in this case were reported, together with a review of the literature.
Khurram et al. [77] stated the following:
- Prostate stromal sarcoma (PSS) are solid organ mesenchymal sarcomas.
- PSS may pose difficult challenges on fine needle aspiration biopsy.
Khurram et al. [77] reported a 49-year-old man who had been diagnosed with metastatic high-grade prostatic stromal sarcoma based upon CT-scan-guided fine needle aspiration (FNA) biopsy of his right lower lung nodule.
Henry et al. [78] stated the following:
- Primary spindle cell sarcoma of the prostate is exceedingly rare and does account for 0.1% of all prostate cancers.
- Typically, the disease course has tended to be rapid and portends a short and dismal prognosis.
- They had reported a case of prostatic stromal sarcoma (PSS) which likely lay dormant for several years after a transurethral resection of the prostate.
- This case was unique in that this cancer did not display the rapid growth of PSS that was reported in prior reports.
- Their patient had undergone a cystoprostatectomy and an ileal conduit.
- Their article had described a rare presentation of a rare tumour and a brief review of the literature.
Mohideen Fathima Seeni Mohamed et al. [79] stated the following:
- Prostate malignancy is the second commonest cancer in men. But among prostatic malignancies; prostatic stromal sarcoma (PSS) is quite rare and this accounts for only about 0.1% to 0.2% of all malignant prostate tumours. [31]
- Sarcoma of the prostate is a rare malignancy that affects younger men and has a poorer prognosis in comparison with prostate cancer [8] Transrectal ultrasound (TRUS) abdominal ultrasound of the prostate is the main methods for early diagnosis. In advanced cases, computed tomography (CT) and magnetic resonance imaging (MRI) are important for staging and surgical planning.
- Treatment of prostate sarcoma consists of radical surgery, chemotherapy, and radiotherapy. Absence of metastasis at the time of diagnosis and negative surgical margins are more important for prognosis.
- They had described ultrasonography, computed tomography and magnetic resonance imaging (MRI) features of a prostatic stromal sarcoma which was identified in a 40-year-old man. MRI scan had depicted the extent and infiltrating nature of the tumour with no zonal predilection. There was no lymphadenopathy, but distant metastasis to the liver was identified. Thus, the appearance of prostatic stromal sarcoma upon CT and MRI was quite different from that of adenocarcinoma of the prostate
Mohideen Fathima Seeni Mohamed et al. [79] reported a-40-year-old man who came to the emergency department with complaints of pain abdomen, retention of urine and constipation for 2 days. He had undergone laparotomy and band removal for small intestinal obstruction 3 years earlier. He underwent an ultrasound of his abdomen which demonstrated a large heterogenous lesion within his prostatic region that measured 8.1 cm x 8.0 cm x 9.0 cm with irregular margins extending posteriorly and superiorly, which was adjudged to be possibility of prostatic malignancy. He underwent a transrectal ultrasound which demonstrated dilated seminal vesicles along with the above same findings.
Fahad Ahmad Alzahrani et al. [80] stated the following:
- Prostatic stromal sarcoma (PSS) is a fairly rare tumour, which comprises only 0.1% to 0.2% of all malignant prostate tumours [31]. classified PSS into two categories: Prostatic stromal proliferation of uncertain malignant potential and PSS.
- The aetiology and pathogenesis of PSS was unknown at the time of publication of their case, and no confirmed risk factors had been identified [31] [34]
Fahad Ahmad Alzahrani et al. [80] reported a 67 years old man who had a past history of Hypothyroidism and left cataract surgery 1 year preceding his presentation. He habitually smoked shisha and he did not have any family history of cancer. He presented to urology department with a history of central abdominal swelling over the preceding 9 months. The swelling was central, firm, non-tender, with smooth skin over it. It was noticed 9 months earlier and it had increased with time. 2 months after the patient developed dysuria and constipation. His serum prostate-specific antigen (PSA) concentration was 0.6 ng/mL. He had computed tomography (CT) scan which revealed a prostatic mass lesion which had displeased his urinary bladder inferiorly. He had MRI scan performed, and it revealed a Large well-circumscribed fairly solid enhancing mass and showing markedly restricted diffusion in the rectovesical pouch inseparable from the superior prostate, but showing no invasion of the bladder or rectum. No features to suggest involvement of the ureters. No metastatic spread seen in the abdomen or pelvis. The lesion appeared to be aggressive and it was suspicious for sarcoma / leiomyosarcoma arising from the prostate. He underwent transurethral resection of prostate and pathology examination of specimens of the prostate biopsy showed: Infiltrating poorly differentiated epithelioid neoplasm. The epithelial cells had exhibited weakly focally positive staining for CKAE1/AE3. the tumour was histologically diagnosed as PSS. Even though the patient was planned to undergo resection of tumour after undergoing neo-adjuvant chemotherapy, he lost his follow up.
Fahad Ahmad Alzahrani et al. [1] made the ensuing summating discussions:
- Prostatic stromal sarcoma is a rare tumour which constitutes about 0.1% to 0.2% of all prostatic cancers. [31] [34]
- Prostatic mesenchymal tumours sometimes cannot be clearly classified as histological entities due to their rarity. [8]
- The majority of these lesions manifest in the sixth and seventh decades of life, and the majority of patients manifest with symptoms of urethral obstruction. [8] [34] [81]
- In previous reports on PSS, age at diagnosis had ranged from 19 years to 86 years (mean, 48 years). [2] [8] [24] [31] [34]
- Serum PSA levels in patients with PSS including the present case had been relatively low (0.1-4.5 ng/mL) in comparison with prostatic adenocarcinoma. [2] [8] [24] [31]
- PSS is often large, with majority of tumours having a diameter of greater than 4 cm [2] [8] [24] [31]
- PSS does present a significant treatment challenge.
- In view of the rare occurrence of PSS and the paucity of published literature, the optimal treatment for the disease had remained unknown. [34]
- Reported management strategies had ranged from observation to radical prostatectomy or cystoprostatectomy with or without concomitant radiotherapy or chemotherapy. Nevertheless, outcomes in these studies are difficult to interpret because of the heterogeneity of treatment modalities. Even though short-term outcomes appear to be promising. [8]
Fahad Ahmad Alzahrani et al. [80] made the following conclusions:
- They had described a rare case of prostatic stromal sarcoma (PSS) in a patient who had an abdominal swelling for 9 months and he also suffered from dysuria and constipation for 8 months.
- And their reported patient was only the 3rd case to be presented with dysuria and constipation.
Conclusions
- Primary Stromal sarcoma of the prostate gland is a rare tumour of the prostate gland that has been reported sporadically and majority of these reported sarcomas had portended an aggressive biological behaviour and poor prognosis.
- Primary stromal sarcomas of the prostate in the scenario of pure tumours have tended to be associated with non-specific lower urinary tract symptoms and or urinary retention associated with normal or low levels of serum prostate specific acid levels unless the tumours are associated with contemporaneous adenocarcinoma of the prostate gland.
- Primary prostate sarcoma can also affect young males including the report of the affliction of a 14-year-old male.
- A high index of suspicion is required in order to establish a quick and accurate diagnosis of primary prostate stromal sarcoma.
- Diagnosis of primary prostate stromal sarcoma of the prostate gland does require histopathology and immunohistochemistry staining of specimens of the prostate gland.
- Furthermore, the undertaking of molecular and cytogenetics studies of patients who have primary stromal sarcomas of the prostate gland could enable oncologists, and Urology multi-disciplinary teams to consider possible additional treatment options to manage this usually aggressive tumour.
- Clinicians should report cases of primary sarcomas of the prostate the encounter including the treatment and outcome to enable clinicians to learn more about the biology behaviour of the tumour.
- A global multi-centre trial of various treatment options would be required to advance as well as improve upon the treatment of this usually very aggressive tumour.
Conflict of interest:
None.
Acknowledgements
Acknowledgements to:
- Medicine (Baltimore) and Wolters Kluwer for granting permission for reproduction of figures and contents of their journal articles under Copy Right: Copyright © 2018 the Author(s). Published by Wolters Kluwer Health, Inc. This is an open access article distributed under the terms of the Creative Commons Attribution-Non-Commercial-No Derivatives License 4.0 (CCBY-NC-ND), where it is permissible to download and share the work provided it is properly cited. The work cannot be changed in any way or used commercially without permission from the journal. http://creativecommons.org/licenses/by-nc-nd/4.0
- Journal of Radiology Case Reports and Wolters Kluwer for granting permission for reproduction of figures and contents of their journal article under Creative Commons Agreement under Copyright Journal of Radiology Case Reports.
References
- Yang W, Liu A, Wu J, Niu M. (2018). Prostatic stromal sarcoma: A case report and literature review. Medicine (Baltimore). 97(18):e0495.
View at Publisher | View at Google Scholar - Gaudin PB, Rosai J, Epstein JI. (1998). Sarcomas and related proliferative lesions of specialized prostatic stroma: a clinicopathologic study of 22 cases. Am J Surg Pathol. 22(2):148-162.
View at Publisher | View at Google Scholar - Ren FY, Lu JP, Wang J, Ye JJ, Shao CW, et al. (2009). Adult prostate sarcoma: radiological-clinical correlation. Clin Radiol. 64(2):171-177.
View at Publisher | View at Google Scholar - Iczkowski KA. (2023). Prostatic stromal sarcoma. PathologyOutlines.com website.
View at Publisher | View at Google Scholar - Tavora F, Kryvenko ON, Epstein JI. (2013) Mesenchymal tumours of the bladder and prostate: an update. Pathology. 45(2):104-115.
View at Publisher | View at Google Scholar - Bostwick DG, Egevad L. (2021). Prostatic stromal proliferations: a review. Pathology. 53(1):12-25.
View at Publisher | View at Google Scholar - Shen Q, Zhou Z, Liu Z, Hu S, Lin Z, et al. (2021). Clinical and Pathological Features of Prostatic Stromal Tumor of Uncertain Malignant Potential: A Retrospective Study of 23 Chinese Cases. Urol Int. 105(3-4):206-214.
View at Publisher | View at Google Scholar - Herawi M, Epstein JI. (2006). Specialized stromal tumors of the prostate: a clinicopathologic study of 50 cases. Am J Surg Pathol. 30(6):694-704.
View at Publisher | View at Google Scholar - Fabio M, Alfredo B, Antonella C, Stefano P, Sergio B. (2021). 18F-FDG PET/CT Imaging of Prostate Stromal Tumor of Uncertain Malignant Potential. Clin Nucl Med. 46(4):348-349.
View at Publisher | View at Google Scholar - Bostwick DG, Hossain D, Qian J, Neumann RM, Yang P, et al. (2004). Phyllodes tumor of the prostate: long-term follow up study of 23 cases. J Urol. 172(3):894-899.
View at Publisher | View at Google Scholar - Razi A, Yahyazadeh SR, Saffar H. (2019). Phyllodes tumor of the prostate: Long-term follow up of a rare condition. Urol Case Rep. 28:101015.
View at Publisher | View at Google Scholar - Wang X, Jones TD, Zhang S, Eble JN, Bostwick DG, et al. Amplifications of EGFR gene and protein expression of EGFR, Her-2/neu, c-kit, and androgen receptor in phyllodes tumor of the prostate. Mod Pathol. 2007 Feb;20(2):175-182.
View at Publisher | View at Google Scholar - Mao QQ, Wang S, Wang P, Qin J, Xia D, et al. (2016). Treatment of prostatic stromal sarcoma with robot-assisted laparoscopic radical prostatectomy in a young adult: A case report. Oncol Lett. 11(4):2542-2544.
View at Publisher | View at Google Scholar - Hicks N, Gurung PM, Deshmukh N, Apakama I, Patel P. (2016). Primary prostate sarcoma: how to manage following diagnosis at transurethral resection. J Surg Case Rep. (5): rjw065.
View at Publisher | View at Google Scholar - Pan CC, Epstein JI. (2013). Common chromosomal aberrations detected by array comparative genomic hybridization in specialized stromal tumors of the prostate. Mod Pathol. 26(11):1536-1543.
View at Publisher | View at Google Scholar - Wickramasinghe S, Beenen E, He M. (2015). Is it really an abscess? An unusual case of metastatic stromal cell sarcoma of the prostate. Int J Surg Case Rep. 17:82-84.
View at Publisher | View at Google Scholar - Choi SH, Kim TH, Yoon GS, Chung SK, Kim BW, et al. (2014). Two different surgical approaches for prostatic stromal sarcoma: robot-assisted laparoscopic radical prostatectomy and open radical cysto-prostatectomy with ileal conduit. Korean J Urol. 55(9):620-623.
View at Publisher | View at Google Scholar - Cavaliere E, Alaggio R, Castagnetti M, Scarzello G, Bisogno G. (2014). Prostatic stromal sarcoma in an adolescent: the role of chemotherapy. Rare Tumors. 6(4):5607.
View at Publisher | View at Google Scholar - Xu Y, Li Z, Shi J, Fu Y, Zhu L, Fan X, Foo WC. (2021). Clinicopathological features to distinguish malignant solitary fibrous tumors of the prostate from prostatic stromal tumors. Virchows Arch. 478(4):619-626.
View at Publisher | View at Google Scholar - Acosta AM, Sholl LM, Dickson BC, McKenney JK, Gordetsky JB, et al. (2021). Re-evaluating tumors of purported specialized prostatic stromal origin reveals molecular heterogeneity, including non-recurring gene fusions characteristic of uterine and soft tissue sarcoma subtypes. Mod Pathol. 34(9):1763-1779.
View at Publisher | View at Google Scholar - Acosta AM, Sholl LM, Marino-Enriquez A, Dal Cin P, Dickson BC, et al. (2021). In Response to Reexamining the molecular findings in specialized stromal tumors of the prostate. Mod Pathol. 34(11):2082-2083.
View at Publisher | View at Google Scholar - Kim JY, Cho YM, Ro JY. (2010). Prostatic stromal sarcoma with rhabdoid features. Ann Diagn Pathol. 14(6):453-456.
View at Publisher | View at Google Scholar - Ueda S, Okada K, Kanzawa M, Fukuda T, Furukawa J, et al. (2020). A case of prostate stromal sarcoma involving the rectum. J Surg Case Rep. (6):rjaa165.
View at Publisher | View at Google Scholar - Morikawa T, Goto A, Tomita K, Tsurumaki Y, Ota S, et al. (2007). Recurrent prostatic stromal sarcoma with massive high-grade prostatic intraepithelial neoplasia. J Clin Pathol. 60(3):330-332.
View at Publisher | View at Google Scholar - Zamparese R, Corini F, Braccischi A, D'Angelo A, Diamanti L, et al. (2011). Primary sarcoma of the specialised prostatic stroma: a case report and review of the literature. Case Rep Pathol. 252805.
View at Publisher | View at Google Scholar - Froehner M, Bartholdt E, Meye A, et al. (2004). Adult prostate sarcoma diagnosed from tissue spontaneously excreted through the urethra. Urol. Oncol. 22:119–120.
View at Publisher | View at Google Scholar - Rojas-Jimenez A, Otero-Garcia M, Mateos-Martin A. (2013). Stromal prostatic sarcoma: a rare tumor with rare clinical and imaging presentation. J Radiol. Case Rep; 7:24–31.
View at Publisher | View at Google Scholar - Tamada T, Sone T, Miyaji Y, et al. (2011). MRI appearance of prostatic stromal sarcoma in a young adult. Korean J Radiol; 12:519–523.
View at Publisher | View at Google Scholar - Venyo AK. (2015). A review of the literature on primary leiomyosarcoma of the prostate gland. Adv Urol; 2015:485786.
View at Publisher | View at Google Scholar - Muglia VF, Saber G, Maggioni G, Jr, et al. (2011). MRI findings of prostate stromal tumour of uncertain malignant potential: a case report. Br J Radiol;84: e194–196.
View at Publisher | View at Google Scholar - Chang YS, Chuang CK, Ng KF, et al. (2005). Prostatic stromal sarcoma in a young adult: a case report. Arch Androl; 51:419–424.
View at Publisher | View at Google Scholar - Huang YC, Wang JY, Lin PY, et al. (2006). Synchronous prostate stromal sarcoma and gastrointestinal stromal tumor of rectum: case report and review of the literature. Urology; 68:672 e11–13.
View at Publisher | View at Google Scholar - Colombo P, Ceresoli GL, Boiocchi L, et al. (2010). Prostatic stromal tumor with fatal outcome in a young man: histopathological and immunohistochemical case presentation. Rare Tumors, 2: e57.
View at Publisher | View at Google Scholar - Osaki M, Osaki M, Takahashi C, et al. (2003). Prostatic stromal sarcoma: case report and review of the literature. Pathol Int; 53:407–411.
View at Publisher | View at Google Scholar - Stilgenbauer R, Benedict M, Bamshad R, et al. (2007). Sarcoma of the prostate: sonographic findings and pathologic correlation. J Ultrasound Med; 26:1789–1793.
View at Publisher | View at Google Scholar - Lee CH, Lin YH, Lin HY, et al. (2006). Gastrointestinal stromal tumor of the prostate: a case report and literature review. Hum Pathol; 37:1361–5.
View at Publisher | View at Google Scholar - Dong A, Gong J, Wang Y, et al. (2014). MRI and FDG PET/CT findings of malignant fibrous histiocytoma of the prostate. Clin Nucl Med 39:889–891.
View at Publisher | View at Google Scholar - Tazi K, Moudouni SM, Elfassi J, et al. (2001). Leiomyosarcoma of the prostate: a study of two cases. Ann Urol (Paris); 35:56–59.
View at Publisher | View at Google Scholar - Zhang Q, Wang H, Ren L, et al. (2014). Primary synovial sarcoma of the prostate metastatic to the liver and lung: a case report. World J Surg Oncol; 12:194.
View at Publisher | View at Google Scholar - Dorsam J, Kalble T, Riedasch G, et al. (1994). The value of diagnostic imaging in benign prostatic hyperplasia and prostatic cancer. Radiologe 34:101–108.
View at Publisher | View at Google Scholar - Aphinives C, Pacheerat K, Chaiyakum J, et al. (2004). Prostatic abscesses: radiographic findings and treatment. J Med Assoc Thai; 87:810–815.
View at Publisher | View at Google Scholar - Dmochowski RR. (2005). Bladder Outlet Obstruction: Etiology and Evaluation. Rev Urol. 7(Suppl 6): S3–S13.
View at Publisher | View at Google Scholar - Krieger JN, Dobrindt U, Riley DE, Oswald E. (2011). Acute Escherichia coli Prostatitis in Previously Health Young Men: Bacterial Virulence Factors, Antimicrobial Resistance, and Clinical Outcomes. Urology. 77:1420–1425.
View at Publisher | View at Google Scholar - Mosharafa AA, Torky MH, El Said WM, Meshref A. (2011). Rising Incidence of Acute Prostatitis Following Prostate Biopsy: Fluoroquinolone Resistance and Exposure Is a Significant Risk Factor. Urology. 78:511–515.
View at Publisher | View at Google Scholar - Krieger JN, Nyberg L, Jr, Nickel JC. (1999). NIH consensus definition and classification of prostatitis. JAMA. 282(3):236–237.
View at Publisher | View at Google Scholar - Barozzil L, Pavlica P, De Matteis M, Canepari M. (1998). Prostatic Abscess: Diagnosis and treatment. 1 59259 886 2; 170:753–757.
View at Publisher | View at Google Scholar - Eble JN, Sauter G, Epstein JI, Sesterhenn IA, editors. (2004). Tumors of the urinary system and male genital organs. Lyon: IARC Press; Pathology and genetics; pp. 218–249.
View at Publisher | View at Google Scholar - DeAntoni EP, Crawford ED, Oesterling JE, Ross CA, Berger ER, et al. (1996). Age- and race-specific reference ranges for prostate-specific antigen from a large community-based study. Urology. 48:234–239.
View at Publisher | View at Google Scholar - Ravery V, Goldblatt L, Royer B, Blanc E, Toublanc M, Boccon-Gibod L. (2000). Extensive biopsy protocol improves the detection rate of prostate cancer. J Urol. 1 64:393–396.
View at Publisher | View at Google Scholar - Yacoub JH, Verma S, Moulton JS, Eggener S, Oto A. (2012). Imaging-guided Prostate Biopsy: Conventional and Emerging Techniques. RadioGraphics. 32:819–837.
View at Publisher | View at Google Scholar - Hamper UM, Sheth S, Walsh PC, Holtz PM, Epstein JI. (1990). Carcinoma of the prostate: value of transrectal sonography in detecting extension into the neurovascular bundle. AJR. 155:1015–1019.
View at Publisher | View at Google Scholar - Kelloff GJ, Choyke P, Coffey DS., (2009). The Prostate Cancer Imaging Working Group. Challenges in Clinical Prostate Cancer: Role of Imaging. AJR. 192:1455–1470.
View at Publisher | View at Google Scholar - Rasch C, Barillot I, Remeijer P, Touw A, van Herk M, Lebesque JV. (1999). Definition of the prostate in CT and MRI: a multi-observer study. Int J Radiat Oncol Biol Phys. 43:57–66.
View at Publisher | View at Google Scholar - Dotan ZA. (2008). Bone imaging in prostate cancer. Nat Clin Pract Urol. 5(8):434–444.
View at Publisher | View at Google Scholar - Choi YJ, Kim JK, Kim M, Kim KW, Choi EK, et al. (2007). Functional MR Imaging of Prostate Cancer. RadioGraphics. 27:63–77.
View at Publisher | View at Google Scholar - Claus FG, Hricak H, Hattery RR. (2004). Pretreatment Evaluation of Prostate Cancer: Role of MR Imaging and 1H MR Spectroscopy. RadioGraphics. 24: S167–S180.
View at Publisher | View at Google Scholar - Oto A, Yan CH, Kayhan A, Tretiakova M, Antic T, et al. (2011). Diffusion-Weighted and Dynamic Contrast-Enhanced MRI of Prostate Cancer: Correlation of Quantitative MR Parameters with Gleason Score and Tumor Angiogenesis. AJR. 197:1382–1390.
View at Publisher | View at Google Scholar - Liu Yiyan. (2012). Invalidity of SUV measurements of lesions in close proximity to hot sources due to “shine-through” effect on FDG PET-CT interpretation. Radiology research and practice: 1–5.
View at Publisher | View at Google Scholar - Murphy RC, Kawashima A, Peller PJ. (2011). The Utility of 11C-Choline PET/CT for Imaging Prostate Cancer: A Pictorial Guide. AJR. 196:1390–1398.
View at Publisher | View at Google Scholar - Yamazaki, H., Ohyama, T., Tsuboi, T. Taoka Y, Kohguchi D, et al. (2012). Prostatic stromal sarcoma with neuroectodermal differentiation. Diagn Pathol 7, 173.
View at Publisher | View at Google Scholar - Bernard T, John R S, Bostwik DG. (1990). In: Pathology of the Prostate. Bostwick G B, editor. New York: Churchhill Livingstone; Soft tissue tumors: pp. 117 -135.
View at Publisher | View at Google Scholar - Bostwick D G, Eble J N. (1997). In: Urologic Surgical Pathology. Bostwick D G, Eble J N, editor. Philadelphia: Mosby; Neoplasms of the prostate pp. 399 – 401.
View at Publisher | View at Google Scholar - Cheville J, Cheng L, Algaba F, Boccon-Gibod L, Furusato M, et al. (2004). In: Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs. Eble J N, Sauter G, Epstein J I, Sesterhenn I A, editor. Lyon: IARC Press; Mesenchymal tumours; pp. 209 – 211.
View at Publisher | View at Google Scholar - Hasegawa S, Yoshikawa M, Konomoto T, Andou S, Inoue M, et al. (2002). Prostatic stromal sarcoma: a case report. Nishinihonkinyokika, 64: 619 – 626.
View at Publisher | View at Google Scholar - Ding B, Zhang Y, Hu W, Hu D, Liu J, et al. (2021). Adult primary prostate sarcoma. A multi-centre cohort study and comparison between Chinese and American cases. Asian J Surg, 44(1): 247 – 253.
View at Publisher | View at Google Scholar - Maria Addesso, Alessandro Caputo, Pio Zeppa, Antonio D’Antonio, (2023). Prostatic stromal sarcoma: Report of a rare case in a young male and review of the literature, International Journal of Surgery Case Reports. 106: 108193.
View at Publisher | View at Google Scholar - Tamada T, Sone T, Miyaji Y, Kozuka Y, Ito K, (2011). MRI Appearance of Prostatic Stromal Sarcoma in a Young Adult Tsutomu, Korean J Radiol, 12(4): 519 – 523.
View at Publisher | View at Google Scholar - Hodotsuka N, Suzuki Y, Suzuki K, Honda Y, Endo S, et al. (2023). A case of complete resection of prostate stromal sarcoma after neoadjuvant chemotherapy. International Journal of Urology Case Reports.
View at Publisher | View at Google Scholar - Chang Y S, Chuang C K, Ng K F, Liao S K. (2005). Prostatic Stromal Sarcoma in A Young Adult: A Case Report, Cancer, Arch Androl. 51(6): 419 – 424.
View at Publisher | View at Google Scholar - Ruihe L; Chongyang D. (2019). 18F-FDG PET/CT Imaging in an Adolescent Patient with Primary Prostatic Stromal Sarcoma. Clinical Nuclear Medicine. 44(1): 45 – 47.
View at Publisher | View at Google Scholar - Li RG, Huang J. (2020). Clinicopathologic characteristics of prostatic stromal sarcoma with rhabdoid features: A case report. World J Clin Cases, 8(3): 606-613.
View at Publisher | View at Google Scholar - Chan K, Piedad J, Mudivaanselage A, et al. (2022). A Rare Case of prostatic Stromal Tumour of Uncertain Malignant Potential Surrounding Ejaculatory Ducts in a Patient with Concurrent Prostate Adenocarcinoma, Cureus; 14(11): e31690.
View at Publisher | View at Google Scholar - González GJL, Menéndez NJ, Rassi D., (2013). Giant prostatic stromal sarcoma. Revista Cubana de Cirugia. 52(2): 146 – 153.
View at Publisher | View at Google Scholar - Kyung Won Kwak, Dae Jin Jo, Eun Hee Lee, Dong Soo Ryu, Tae Hee Oh. (2011). A Case of Laparoscopic Radical Prostatectomy for a Prostatic Stromal Tumor of Uncertain Malignant Potential. Korean Journal of Urology; 52(8): 578-581.
View at Publisher | View at Google Scholar - Mazroa J A, Almakhalas K A, Bashanfer G. (2023). Atypical Prostatic Stromal Sarcoma Presented with T2WI Central Heterogeneous Hyperintense Lesion Showing Peripheral Zone & Peri Prostatic Fat Invasion. Interesting Images; 1-3.
View at Publisher | View at Google Scholar - Segawa N, Hamada S, Takahara K, Azuma H, Tsuji M, et al. (2008). Prostatic stromal sarcoma: a case report. Hinyokika Kiyo. 54(1):29-34.
View at Publisher | View at Google Scholar - Khurram M S, Tanesh G Sakhi, R Hamza A, Ibrar W, Bano R. (2017). Metastatic prostatic stromal sarcoma: A challenging diagnosis on fine-needle aspiration with broad differential diagnosis. Case Report. 14; 15.
View at Publisher | View at Google Scholar - Henry W, Britton C, Coco C, Dadhania V S, Slobodov G. (2019). Stomal sarcoma of the prostate. Can J. Urol. 26(1): 9683-9685.
View at Publisher | View at Google Scholar - Mohamed M F S, Indiran V, Kalaichezhian M. (2016). Imaging of A Rare Prostate Malignancy Prostatic Sarcoma., 4(8B):2863-2866.
View at Publisher | View at Google Scholar - Alzahrani F A, Alsenani F M, Sultan M A, Aljohani A H, Alassiri A A. (2017). Prostatic Stromal Sarcoma: Case Report and Review of the Literature. International Journal of Healthcare Sciences; 5(1): 1-3 ISSN 2348-5728
View at Publisher | View at Google Scholar - Probert JL, O’Rourke JS, Farrow R, Cox P. (2000). Stromal sarcoma of the prostate. Eur J Surg Oncol; 26:100-101.
View at Publisher | View at Google Scholar
