

Case Report | DOI: https://doi.org/10.31579/2834-5134/018
Orthodontic Extrusion with Crown Restoration in The Management of Anterior Teeth Crown-Root Fracture: A Case Report
- Wang Jing
- Huo Na
- Cai Chuan
- Xu Lulu *
Department of Stomatology, The First Medical Center of PLA General Hospital, 28 Fuxing Road, Haidian District, Beijing, China
*Corresponding Author: Xu Lulu, Department of Stomatology, The First Medical Center of PLA General Hospital, 28 Fuxing Road, Haidian District, Beijing, China.
Citation: Wang Jing, Huo Na, Cai Chuan, Xu Lulu (2023). Orthodontic Extrusion with crown restoration in the management of anterior teeth crown-root fracture: Journal of Clinical Anatomy, 2(2) DOI:10.31579/2834-5134/018
Copyright: © 2023 Xu Lulu, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 March 2023 | Accepted: 07 April 2023 | Published: 18 April 2023
Keywords: Fracture; Orthodontic extrusion; Anterior teeth; Ceramic crown
Abstract
Crown-root fracture is a rare type of dental traumatic injury. Management of traumatized teeth sometimes requires a multidisciplinary approach to obtain better esthetic results as well as for the conservation of tooth structure. This article describes the management of a case of oblique crown root fracture of anterior teeth. After the removal of the coronal fragment, the roots were filled with calcium hydroxide. Orthodontic extrusion was initiated for 4 months, and 3 mm extrusion was achieved. The ceramic crown was cemented on anterior fracture teeth. The periodontal condition appeared to be healthy and good esthetic was maintained during the follow-up appointment.
Introduction
Crown-root fracture is a rare type of dental traumatic injury, affecting 0.5% to 7% of permanent teeth1. In this type of injury, the wound involves damage to the pulp, cementum, dentin, and periodontal ligament. Depending on the severity of the injury, multiple or single fractures of the root can be observed. Management of traumatized teeth sometimes requires a multidisciplinary approach to obtain better esthetic results as well as for the conservation of tooth structure2. Exposure of the fractured margin into the oral cavity is desirable. This may be achieved by 3: (i) crown lengthening, (ii) surgical extrusion, and (iii) orthodontic extrusion. This case report presents the management of a cervical root fracture using orthodontic extrusion and final restoration with a ceramic crown.
Case report
A 22-year-old man reported to the Department of Orthodontic Dentistry with a complaint of damaged anterior teeth. History revealed that the patient had an injury to the front tooth region 1 month ago, due to a fall. Intraoral examination revealed anterior teeth crown-root fractured, the coronal fragment was extracted (Fig1A). The fracture line was located subgingivally on the mesiobuccal and mesiolingual aspects. The periapical radiograph revealed that the fracture line was extending up to the level of the alveolar crest. The root canal treatment of fractured teeth was finished (Fig1B).
Since the fracture line extended up to the alveolar bone crest, it was possible to initiate extrusion of the root so as to facilitate placement of coronal restoration and long-term attachment health. So orthodontic extrusion was possible. The lingual button was bonded on the fracture side of the anterior teeth (Fig2A). The patient was revisioned once a month and orthodontic traction was taken. Removable appliances were used for the lower arch to tract anterior teeth with the help of the buttons. A small amount of both labial and palatial mucous recontouring was done using the electrotome method to allow for proper finishing of the crown margins (Fig2B). Interactive traction was used for 4 months, and 3 mm extrusion was achieved (Fig2C D). The temporary crown was used for 6 months (Fig). Finally, the ceramic crown was cemented on 12 11, and 21(Fig3B). During the three-month follow-up appointment, the periodontium appeared to be healthy and a good esthetic was maintained.
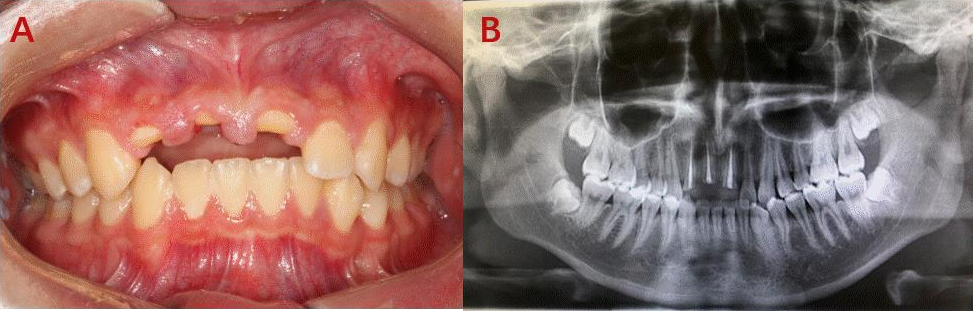
Figure 1 A: Intraoral examination revealed anterior teeth crown-root fractured, and the coronal fragment was extracted: Periapical radiograph revealed that the fracture line was extendingup to the level of the alveolarcrest. The root canal treatment of fractured teeth was finished
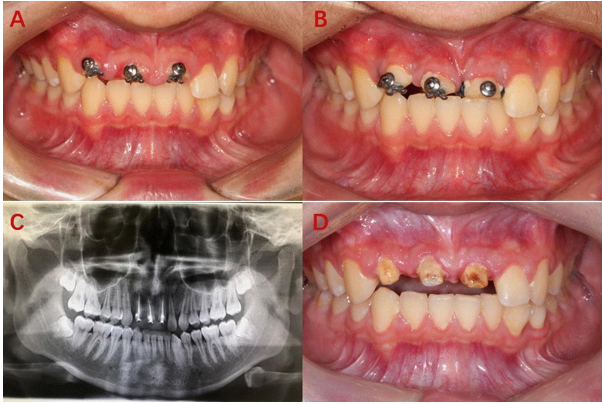
Figure 2 A:Lingual button was bonded on the fracture side of the anterior teeth; B: A small amount of both labial and palatial mucosal recontouring was done using the electrosurgical method to allow for proper finishing of the crown margins; C D: Interactive traction was used for 4 months, and 3 mm extrusion was achieved
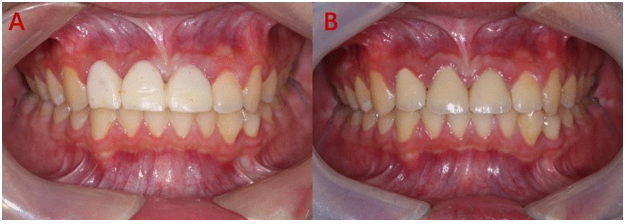
Figure 3 A: The temporary crown was used for 6 months; B: the ceramic crown was cemented on 12 11and 21
Discussion
The orthodontic forced eruption was first describedby Heithersay as coronal orthodontic movement achieved by applying continuous orthodontic force for the purposeof preserving soft tissues and gaining vertical bone height. Orthodontic extrusion is a safe, minimally invasive, and highly predictable treatment. It shows several advantages if compared to surgical crown lengthening4. First, tooth structure and periodontal support maintenance is crucial. As previously mentioned, it is required to extend bone resection on the adjacentteeth to harmonizethe gingival morphology in surgical crown lengthening. This causes bone loss and possible damage of the periodontal support as well as a worsening of the crown/root ratio of these teeth. Conversely, orthodontic extrusion can just cause tooth displacement or even increase the volume of dental support tissues, which is particularly advantageous for implant purposes 5.
Orthodonticextrusion can be obtained using different orthodontic strategies6: fixed appliances, removable appliances, and temporary anchorage devices such as mini-screw. Different treatment choice variables must be considered, such as patient preference, oral hygiene, availability of an appropriate orthodontic anchorage, and amount of dentalcrown available. As a general rule, the less periodontal support, the less force needed for extrusion. An accelerated movement rate may result in a risk of tissue damage and ankylosis. A sufficient crown-root ratio (ideally less than 1:1), healthy gingiva, and osseous structureswithout any pathological signs are requiredfor successful extrusion and favorable estheticoutcomes in crown-root fractured teeth. The current knowledge suggests the application of light and constant forcesof 15 g for the anterior teeth and 50 g for posterior teeth are optimal to extrude a tooth for implant site enhancement7.
After the successful application of orthodontic extrusion, the stabilization phase takes place. The resin crown was used as a temporary crown for 6 months. This phase is important to allow for proper reorganization of the soft tissue and remodeling of the bone in the so-called” osteoid formation’’ phase, thus discouraging relapse.
It is preferable to choose orthodontic extrusion if a highly predictable treatment is requestedif an orthodontic device is already present,and if it is necessary to preserve tooth vitality or treat teethnon- compatible with an atraumatic extraction. Orthodontic movements, especially if performed on traumatized teeth or through the application of heavy forces, can cause root resorption8. However,it can be considered a rare event when performing extrusive movement. Moreover, there was no correlation betweenthe degree of extrusion and the occurrence of root resorption.
Conclusion
Using a combination of orthodontic extrusionand crown restoration may be considered for the treatment of crown root fractures because:
1.Esthetics is maintained until the final restoration placement by highly cost-effective.
2.Excellent esthetics and periodontal health is maintained if the final restoration is made after orthodontic extrusion.3.It is a simple and safe method and hence more acceptable to the patient.
4.The prospects of this treatment modality for crownroot fractures of posterior teeth need to be investigated.
5.Supported by National key research and development program2022YFC3103202; Military medicalscience Foundation of Youth project21QNPY104; National naturalscience foundation 8217086
References
- Cordaro, M., Staderini, E., Torsello, F., Grande,N. M., Turchi, M., & Cordaro, M. (2021). Orthodontic extrusion vs. surgical extrusion to rehabilitate severely damaged teeth: a literature review. International Journal of Environmental Research and Public Health, 18(18), 9530.
View at Publisher | View at Google Scholar - Alsahhaf, A., & Att, W. (2016). Orthodontic extrusion for pre-implant site enhancement: Principles and clinical guidelines. Journal of prosthodontic research, 60(3), 145-155.
View at Publisher | View at Google Scholar - Zasciurinskiene, E., Lindsten, R., Slotte, C., & Bjerklin, K. (2016). Orthodontic treatment in periodontitis‐susceptible subjects: a systematic literature review. Clinical and experimental dental research, 2(2), 162-173.
View at Publisher | View at Google Scholar - Canoglu, H., Gungor, H. C., & Cehreli, Z. C. (2007). Management of cervical root fracture using orthodontic extrusion and crown reattachment: a case report. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 104(3), e46-e49.
View at Publisher | View at Google Scholar - Elisabeth Reichardt, Ralf Krug, Michael M. Bornstein, Jürgen Tomasch, Carlalberta Verna, Gabriel Krastl.Orthodontic Forced Eruption of Permanent Anterior Teeth with Subgingival Fractures: A Systematic Review.Int J Environ Res Public Health. 2021, 18, 12580.
View at Publisher | View at Google Scholar - Huang, G., Yang, M., Qali, M., Wang, T. J., Li, C., & Chang, Y. C. (2021). Clinical considerations in orthodontically forced eruption for restorative purposes. Journal of clinical medicine, 10(24), 5950.
View at Publisher | View at Google Scholar - Isola, G., Nucera, R., Damonte, S., Ugolini, A., De Mari, A., & Migliorati, M. (2022). Implant Site Changes in Three Different Clinical Approaches: Orthodontic Extrusion, Regenerative Surgery and Spontaneous Healing after Extraction: A Systematic Review. Journal of Clinical Medicine, 11(21), 6347.
View at Publisher | View at Google Scholar - Suprabha, B. S., Kundabala, M., Subraya, M., & Kancherla, P. (2006). Reattachment and orthodontic extrusion in the management of an incisor crown-root fracture: a case report. J Clin Pediatr Dent, 30(3), 211-214.
View at Publisher | View at Google Scholar
