

Research Article | DOI: https://doi.org/10.31579/2834-5029/051
Non-diabetic, obesity associated fatty liver: Educational ultrasound images and expert opinion
- Aamir Jalal Al-Mosawi *
The National Training and Development Center and Baghdad Medical City Baghdad.
*Corresponding Author: Aamir Jalal Al-Mosawi, The National Training and Development Center and Baghdad Medical City Baghdad.
Citation: Aamir Jalal Al-Mosawi (2024), non-diabetic, obesity associated fatty liver: Educational ultrasound images and expert opinion, International Journal of Biomed Research, 3(1): DOI:10.31579/2834-5029/051
Copyright: © 2024, Aamir Jalal Al-Mosawi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 February 2024 | Accepted: 15 February 2024 | Published: 22 February 2024
Keywords: fatty liver; a historic overview; ultrasound images; educational article; expert opinion
Abstract
Background: Obesity and diabetes are generally considered the most important risk factors for developing fatty changes in the liver. This paper integrates historical context with contemporary findings, clarifies patient details and treatment approaches, and emphasizes the relevance of recent research in managing fatty liver disease. Patients and methods: This study includes two patients presented with symptoms suggestive of urolithiasis and underwent abdominal ultrasound. Besides urinary abnormalities, both patients exhibited moderate fatty changes in their livers. Results: Patient 1, 39-year-old male weighing 100 kilograms, abdominal ultrasound showed a normal-sized liver with moderate fatty changes. There were also coarse crystals within the renal collecting systems of both kidneys. Abdominal ultrasound of the second patient, a 45-year female patient weighing 95 kilograms, showed normal-sized liver with moderate fatty changes. In addition, there were coarse crystals within the renal collecting systems of both kidneys. The evidence-based treatment of fatty liver included oral silymarin and oral metformin. Conclusion: Based on current evidence, a combination of silymarin and metformin appears promising for managing non-diabetic obese patients with fatty liver disease, offering a potential therapeutic approach for patients without significant hepatic symptoms. |
Introduction
<!-- /* Font Definitions */ @font-face {font-family:"Cambria Math"; panose-1:2 4 5 3 5 4 6 3 2 4; mso-font-charset:0; mso-generic-font-family:roman; mso-font-pitch:variable; mso-font-signature:-536869121 1107305727 33554432 0 415 0;} @font-face {font-family:Calibri; panose-1:2 15 5 2 2 2 4 3 2 4; mso-font-charset:0; mso-generic-font-family:swiss; mso-font-pitch:variable; mso-font-signature:-469750017 -1073732485 9 0 511 0;} /* Style Definitions */ p.MsoNormal, li.MsoNormal, div.MsoNormal {mso-style-unhide:no; mso-style-qformat:yes; mso-style-parent:""; margin-top:0in; margin-right:0in; margin-bottom:8.0pt; margin-left:0in; line-height:107%; mso-pagination:widow-orphan; font-size:11.0pt; font-family:"Calibri",sans-serif; mso-ascii-font-family:Calibri; mso-ascii-theme-font:minor-latin; mso-fareast-font-family:Calibri; mso-fareast-theme-font:minor-latin; mso-hansi-font-family:Calibri; mso-hansi-theme-font:minor-latin; mso-bidi-font-family:"Times New Roman"; mso-bidi-theme-font:minor-bidi;} span.authors-list-item {mso-style-name:authors-list-item; mso-style-unhide:no;} .MsoChpDefault {mso-style-type:export-only; mso-default-props:yes; mso-ascii-font-family:Calibri; mso-ascii-theme-font:minor-latin; mso-fareast-font-family:Calibri; mso-fareast-theme-font:minor-latin; mso-hansi-font-family:Calibri; mso-hansi-theme-font:minor-latin; mso-bidi-font-family:"Times New Roman"; mso-bidi-theme-font:minor-bidi; mso-font-kerning:0pt; mso-ligatures:none;} .MsoPapDefault {mso-style-type:export-only; margin-bottom:8.0pt; line-height:107%;} @page WordSection1 {size:8.5in 11.0in; margin:.5in .5in .5in .5in; mso-header-margin:.5in; mso-footer-margin:.5in; mso-paper-source:0;} div.WordSection1 {page:WordSection1;} @page WordSection2 {size:8.5in 11.0in; margin:1.0in 1.0in 1.0in 1.0in; mso-header-margin:.5in; mso-footer-margin:.5in; mso-paper-source:0;} div.WordSection2 {page:WordSection2;} -->
Thomas Addison (Figure-1A), an English physician from Guy's Hospital in London, is credited with one of the earliest reports in 1836 associating fatty liver with excessive alcohol drinking and tuberculosis [1].

Figure-1A: Thomas Addison (April 1795 - June 1860)
In 1849, Carl von Rokitansky (Figure-1B), an Austrian physician and pathologist, expanded on these associations by describing fatty liver in children with visceral adiposity due to excessive food intake, alongside its connections to tuberculosis and alcoholism [2].
Figure-1B: Baron Carl von Rokitansky (February 19, 1804 - July 23, 1878)
George Budd (Figure-1C), another English physician, in 1857, defined fatty liver as the presence of excess fat in over 5% of hepatocytes, primarily linked with a diet rich in fatty foods in asymptomatic adults [3].
Figure-1C: George Budd (February 23, 1808 - March 14, 1882)
Obesity and diabetes are generally considered the most important risk factors for developing fatty changes in the liver. In 2015, Ludovico Abenavoli from Italy and his research team considered fatty liver that is not related to alcohol to be the most common liver disorder throughout the world. Zobair Younossi from the United States and his international research group emphasized that obesity is the major risk factor for the development of non-alcoholic liver disease [4, 5, 6].
This paper integrates historical context with contemporary findings, clarifies patient details and treatment approaches, and emphasizes the relevance of recent research in managing fatty liver disease.
Patients and methods
This study includes two patients presented with symptoms suggestive of urolithiasis and underwent abdominal ultrasound. Besides urinary abnormalities, both patients exhibited moderate fatty changes in their livers.
Results
<!-- /* Font Definitions */ @font-face {font-family:"Cambria Math"; panose-1:2 4 5 3 5 4 6 3 2 4; mso-font-charset:0; mso-generic-font-family:roman; mso-font-pitch:variable; mso-font-signature:-536869121 1107305727 33554432 0 415 0;} @font-face {font-family:Calibri; panose-1:2 15 5 2 2 2 4 3 2 4; mso-font-charset:0; mso-generic-font-family:swiss; mso-font-pitch:variable; mso-font-signature:-469750017 -1073732485 9 0 511 0;} @font-face {font-family:Verdana; panose-1:2 11 6 4 3 5 4 4 2 4; mso-font-charset:0; mso-generic-font-family:swiss; mso-font-pitch:variable; mso-font-signature:-1610610945 1073750107 16 0 415 0;} /* Style Definitions */ p.MsoNormal, li.MsoNormal, div.MsoNormal {mso-style-unhide:no; mso-style-qformat:yes; mso-style-parent:""; margin-top:0in; margin-right:0in; margin-bottom:8.0pt; margin-left:0in; line-height:107%; mso-pagination:widow-orphan; font-size:11.0pt; font-family:"Calibri",sans-serif; mso-ascii-font-family:Calibri; mso-ascii-theme-font:minor-latin; mso-fareast-font-family:Calibri; mso-fareast-theme-font:minor-latin; mso-hansi-font-family:Calibri; mso-hansi-theme-font:minor-latin; mso-bidi-font-family:"Times New Roman"; mso-bidi-theme-font:minor-bidi;} p {mso-margin-top-alt:auto; margin-right:0in; mso-margin-bottom-alt:auto; margin-left:0in; mso-pagination:widow-orphan; font-size:12.0pt; font-family:"Times New Roman",serif; mso-fareast-font-family:"Times New Roman";} .MsoChpDefault {mso-style-type:export-only; mso-default-props:yes; mso-ascii-font-family:Calibri; mso-ascii-theme-font:minor-latin; mso-fareast-font-family:Calibri; mso-fareast-theme-font:minor-latin; mso-hansi-font-family:Calibri; mso-hansi-theme-font:minor-latin; mso-bidi-font-family:"Times New Roman"; mso-bidi-theme-font:minor-bidi; mso-font-kerning:0pt; mso-ligatures:none;} .MsoPapDefault {mso-style-type:export-only; margin-bottom:8.0pt; line-height:107%;} @page WordSection1 {size:8.5in 11.0in; margin:.5in .5in .5in .5in; mso-header-margin:.5in; mso-footer-margin:.5in; mso-columns:2 even .5in; mso-paper-source:0;} div.WordSection1 {page:WordSection1;} @page WordSection2 {size:8.5in 11.0in; margin:.5in .5in .5in .5in; mso-header-margin:.5in; mso-footer-margin:.5in; mso-paper-source:0;} div.WordSection2 {page:WordSection2;} @page WordSection3 {size:8.5in 11.0in; margin:.5in .5in .5in .5in; mso-header-margin:.5in; mso-footer-margin:.5in; mso-columns:2 even .5in; mso-paper-source:0;} div.WordSection3 {page:WordSection3;} @page WordSection4 {size:8.5in 11.0in; margin:.5in .5in .5in .5in; mso-header-margin:.5in; mso-footer-margin:.5in; mso-paper-source:0;} div.WordSection4 {page:WordSection4;} @page WordSection5 {size:8.5in 11.0in; margin:1.0in 1.0in 1.0in 1.0in; mso-header-margin:.5in; mso-footer-margin:.5in; mso-paper-source:0;} div.WordSection5 {page:WordSection5;} -->
Patient 1, 39-year-old male weighing 100 kilograms, abdominal ultrasound (Figure-2) showed a normal-sized liver with moderate fatty changes on ultrasound. No focal lesions or dilatations were observed in the intra-hepatic ducts. The gallbladder was contracted, and there was no evidence of hepatic venous congestion, and the common bile duct was not dilated (4 mm in diameter). The spleen, and pancreas were both normal in appearance.
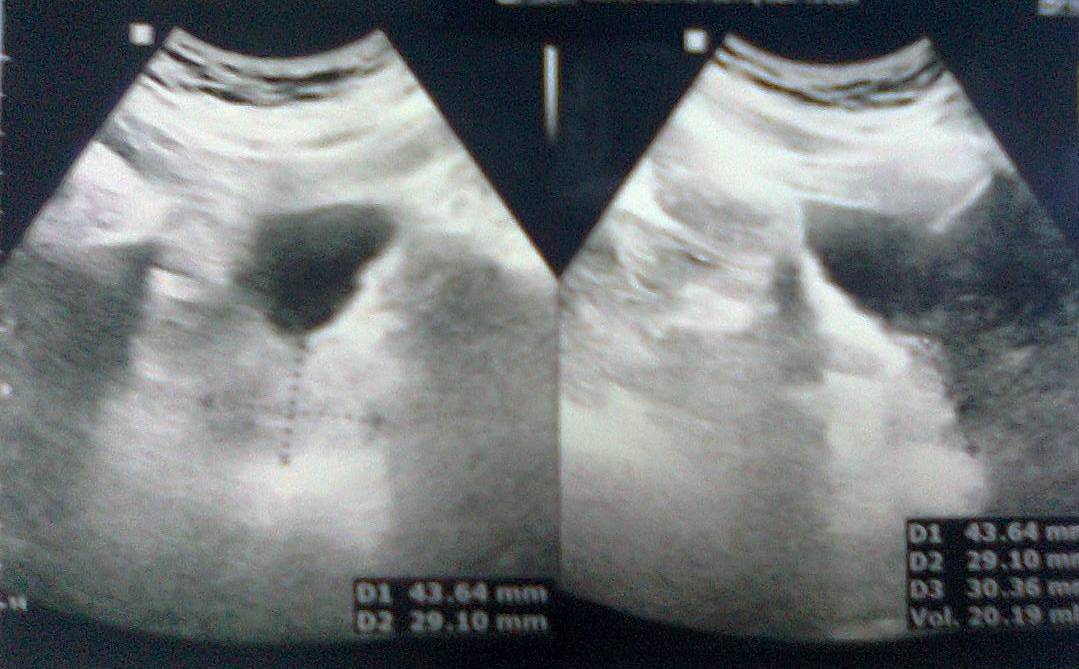
Figure-2A

Figure-2B

Figure-2C

Figure-2D
Both kidneys were normal in size (Right kidney: 12.6 x 5 cm, left kidney: 13.3 x 5 cm), shape and position. Both kidneys had normal parenchyma (Thickness 18 mm) with no pelvi-calyceal dilatation. However, there were coarse crystals within the renal collecting systems of both kidneys. The urinary bladder and prostate both had normal appearance and the prostate volume was 20 milliliters.
Abdominal ultrasound (Figure-3) of the second patient, a 45-year female patient weighing 95 kilograms, showed normal-sized liver with moderate fatty changes. The liver margin was smooth and there was neither focal lesion nor dilatation of the intra-hepatic duct. The gall bladder had normal capacity and normal thickness with no abnormality. There was no evidence of hepatic venous congestion, and the common bile duct was not dilated (4 mm in diameter). The spleen and pancreas were both normal in appearance.
Both kidneys were normal in size (Right kidney: 11.6 x 5 cm, left kidney: 11.3 x 5 cm), shape and position. Both kidneys had normal parenchyma (Thickness 18 mm) with no pelvi-calyceal dilatation. Renal ultrasound also showed two renal sinuses suggesting bifid collecting systems. In addition, there were coarse crystals within the renal collecting systems of both kidneys.
The urinary bladder had normal appearance, and a normal vaginal cap was seen (9.5 mm) but the uterus and both ovaries were not seen because of surgical removal.
For the coarse urinary crystals, both patients received oral essential oil terpenes (Urinex) based on the evidence provided and presented by Al-Mosawi AJ [7, 8, 9, 10]. For the fatty liver changes, both patients received oral silymarin (Legalon) 75 mg once daily was prescribed based on the evidence provided by Buturova and colleagues (2010), Luis (2015) [11,12].
Both patients received also an initial dose of 500 mg daily of oral metformin to help with weight reduction based on the evidence provided by Schwimmer et al (2005) and Seifarth and colleagues (2013) [13,14].
Discussion
Obesity associated fatty liver has been reported as early as the 1800s [2.3]. As early as 2005, Colicchio et al from Italy emphasized that obesity per se can increase the risk of liver disease. They reported the usefulness of abdominal ultrasound in the detection of fatty liver (steatosis), and the classification of the severity into mild, moderate, and severe in non-diabetic obese patients [15].
In 2024, Li et al from China performed systematic review and meta-analysis which included 26 controlled studies involving 2375 patients. The review and analysis showed that silymarin can attenuate liver damage and markedly improve hepatic steatosis on liver histology study [16].

Figure-3A

Figure-3B

Figure-3C

Figure-3D
The use of metformin in non-diabetic obesity has been increasingly suggested [17]. As early as 2005, Bugianesi et al from Italy considered metformin to have a proven usefulness in the treatment of nonalcoholic fatty liver disease. They reported a one-year study which included non-diabetic patients; 55 patients received metformin 2000 mg daily, 28 patients received vitamin E 800 IU daily, and 27 treated by a dietary intervention to lower weight. The study showed the superiority of metformin over dietary therapy and vitamin E [18].
Conclusion
The association between obesity and fatty liver has been recognized since the 1800s. Recent studies, such as those by Colicchio et al. and Li et al., emphasize the utility of abdominal ultrasound in detecting and classifying fatty liver severity. Silymarin has shown promise in attenuating liver damage and improving hepatic steatosis, while metformin has been increasingly considered for its benefits in non-diabetic obese patients.
Based on current evidence, a combination of silymarin and metformin appears promising for managing non-diabetic obese patients with fatty liver disease, offering a potential therapeutic approach for patients without significant hepatic symptoms.
Acknowledgment
The author has the copyright of the sketch in this paper.
Conflict of interest: None.
References
- Addison T. Observations on fatty degeneration of the liver. Guys Hosp Rep 1836; 1:485.
View at Publisher | View at Google Scholar - Rokitansky C. vol. 2. Sydenham Society; London: 1849. (A Manual of Pathological Anatomy). Translated by William Edward Swaine, Edward Henry Sieveking, Charles Hewitt Moore, George Edward Day.
View at Publisher | View at Google Scholar - Budd G. 3rd ed. John Churchill; London: 1857. On diseases of the liver.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. Intestinal Dialysis Research Progress and the Early Treatment of A Non-Diabetic Patient with Symptomatic Uremia and Fatty Liver with Intestinal Dialysis: the Practice of Evidence-Based Medicine. Journal of Biomedical Sciences and Biotechnology Research (ISSN: 3049-7272) March 11, 2024; 2 (1): 1-4.
View at Publisher | View at Google Scholar - Abenavoli L, Greco M, Na zionale I, Peta V, Milic N, Accattato F, Foti D, Gulletta E, Luzza F. Effects of Mediterranean diet supplemented with silybin-vitamin E-phospholipid complex in overweight patients with non-alcoholic fatty liver disease. Expert Rev Gastroenterol Hepatol 2015 Apr; 9(4):519-527.
View at Publisher | View at Google Scholar - Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, George J, Bugianesi E. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol 2018 Jan; 15(1):11-20. Doi: 10.1038/nrgastro. 2017.109.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. A possible role of essential oil terpenes in the management of childhood urolithiasis. Therapy (Clinical practice) [p-ISSN: 2044-9038, e-ISSN: 2044-9046] Mar 2005; 2(2):243-247.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. Essential oil terpenes: adjunctive role in the management of childhood urolithiasis J Med Food. 2010 Apr; 13(2):247-250.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. The treatment of childhood progressive bilateral multiple renal stone disease: A role of essential oil terpenes. Archive Urological Research (ISSN: 2692-4706) 2020 March 19; 4(1): 007-009.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. Role of plant essential oil terpenes in renal disorders. In: J.N. Govil and Sanjib Bhattacharya (Ed). Recent Progress in Medicinal Plants Vol. 36: Essential Oils. Studium Press LLC, Jan 2013 (ISBN: 1-933699-96-5).
View at Publisher | View at Google Scholar - Buturova LI, Tsybizova TA, Kalinin AV. [Use of Legalon in non-alcoholic fatty liver disease]. Eksp Klin Gastroenterol 2010 ;( 5):69-75 [Article in Russian].
View at Publisher | View at Google Scholar - Aller R, Izaola O, Gómez S, Tafur C, González G, Berroa E, Mora N, González JM, de 12-Luis DA. Effect of silymarin plus vitamin E in patients with non-alcoholic fatty liver disease. A randomized clinical pilot study. Eur Rev Med Pharmacol Sci 2015 Aug; 19 (16):3118-3124.
View at Publisher | View at Google Scholar - Schwimmer JB, Middleton MS, Deutsch R, Lavine JE. A phase 2 clinical trial of metformin as a treatment for non-diabetic paediatric non-alcoholic steatohepatitis. Aliment Pharmacol Ther 2005 Apr 1; 21(7):871-9.
View at Publisher | View at Google Scholar - Seifarth C, Schehler B, Schneider HJ. Effectiveness of metformin on weight loss in non-diabetic individuals with obesity. Exp Clin Endocrinol Diabetes 2013 Jan; 121(1):27-31.
View at Publisher | View at Google Scholar - Colicchio P, Tarantino G, del Genio F, Sorrentino P, Saldalamacchia G, Finelli C, Conca P, Contaldo F, Pasanisi F. Non-alcoholic fatty liver disease in young adult severely obese non-diabetic patients in South Italy. Ann Nutr Metab 2005 Sep-Oct; 49(5):289-295.
View at Publisher | View at Google Scholar - Li S, Duan F, Li S, Lu B. Administration of silymarin in NAFLD/NASH: A systematic review and meta-analysis. Ann Hepatol 2024 Mar-Apr; 29(2):101174.
View at Publisher | View at Google Scholar - Al-Mosawi AJ. The Use of Metformin in Non-Diabetic Obesity: An Educational Article and Expert Opinion. Cancer Research and Cellular Therapeutics (ISSN: 2640-1053) 24 July 2023; 7 (3):1-3.
View at Publisher | View at Google Scholar - Bugianesi E, Gentilcore E, Manini R, Natale S, Vanni E, Villanova N, David E, Rizzetto M, Marchesini G. A randomized controlled trial of metformin versus vitamin E or prescriptive diet in nonalcoholic fatty liver disease. Am J Gastroenterol 2005 May; 100(5):1082-1090.
View at Publisher | View at Google Scholar
