

Research Article | DOI: https://doi.org/10.31579/2834-5029/015
Medication Related Problems and Its Predictors Among Heart Failure Patients at A Tertiary Care Hospital in Ethiopia: A Prospective Interventional Study
1 Jimma University, School of pharmacy, Jimma, Ethiopia.
2 Jimma University Medical Center, Jimma, Ethiopia.
*Corresponding Author: Aster Wakjira Garedow, Jimma University, School of pharmacy, Jimma, Ethiopia.
Citation: Aster W. Garedow, Gorfineh T. Tesfaye, (2023), Medication Related Problems and Its Predictors Among Heart Failure Patients at A Tertiary Care Hospital in Ethiopia: A Prospective Interventional Study, International Journal of Biomed Research. 2(2): DOI: 10.31579/2834-5029/015
Copyright: © 2023, Aster Wakjira Garedow. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 24 February 2023 | Accepted: 17 March 2023 | Published: 27 March 2023
Keywords: medication related problems; heart failure; Jimma medical center; interventions
Abstract
Background: Medication related problems in cardiovascular disease patients, especially among heart failure patients were found to be high. Medication related problem is a critical problem to provide high quality health care service for the patient which is associated with high mortality, complication, prolonged hospital stays, compromised quality of life and increase health care cost.
Objective: To determine medication related problems and its predictors in hospitalized heart failure patients at Jimma Medical Center, from May 30, 2019 to November 28, 2020.
Methods: A prospective interventional study was conducted among heart failure patients from May 30, 2020 to November 28, 2021 at Jimma Medical Center. Medication related problems were sorted based on pharmaceutical care network Europe drug classification tool version 9.0. Patient’s specific data was collected using questionnaire. The data were coded, cleaned, and entered into Epidata version 4.6 and exported to SPSS version 25.0 for analysis. Binary Logistic regression was used to identify independent predictors of medication related problems occurrence. Variables having P-values < 0.05 were considered statistically significant.
Results: A total of 384 heart failure patients were included in the study. The mean (SD) age was 49.06+17.79. Two third of study participants had at least one medication related problem. A total of 483 MRPs were identified among 231(60.15%) patients. Treatment effectiveness related problem (55.48%) was the most common observed medication related problems. Alcoholism (AOR; 3.25, 95% CI (1.46-7.23), prolonged hospital stays [AOR=3.67, 95%CI= (1.85-7.27)]; comorbidity [AOR=2.88, 95%CI= (1.47-5.66)] and polypharmacy [AOR=3.07, 95%CI= (1.57-5.99) were the independent predictors of medication related problems.
Conclusion: The prevalence of medication related problem was high among heart failure patients. Alcoholism, prolonged hospital stay, comorbidity and polypharmacy were the predictors of medication related problems. Hence, to overcome these problems, clinical pharmacists, physicians and other health care professionals have to work in collaboration.
Introduction
Heart failure (HF) is a complex clinical syndrome that results from any structural or functional impairment of ventricular filling [1]. It has emerged as dominant form of cardiovascular disease in Africa and places great stresses on patients, caregivers and healthcare system [2-3]. Hence, the development of effective treatment regimens targeted reducing morbidity and mortality of HF patients and this led to a large number of drugs with which HF patients are treated on a regular basis. However, this causes acceptance problems from the side of the patient and the treating physician. Increasing expenses for HF medication might prevent physicians from prescribing all medications that are recommended in the recent guidelines. spite of the fact that, these regimens have beneficial effect in the long-term treatment, accumulation side effects might prevent the patient from receiving full treatment [4].
Medication related problems (MRPs) are a consequence of medication -related needs that have gone unmet, central to pharmaceutical care practice [5]. There are different MRP classification systems that different literatures use. According to Pharmaceutical Care Network Europe (PCNE) classification version9, MRPs is an event or circumstance involving drug therapy that interferes with desired health outcomes (6). MRPs are common in hospitalized patients and result in patient morbidity, mortality, increased costs, impact on patients’ quality of life, prolong hospital stays and increase the overall burden of healthcare expenditures (7). Older ages, different co morbidities and polypharmacy may complicate management of HF, which probably put patients at risk for MRPs (8-12). The systematic review on MRPs revealed that, need additional drug therapy was the most common MRPs, which showed that treatment of MRP is still suboptimal (13). Systematic review carried out in Ethiopia showed that MRPs among HF was higher than other medical conditions. Taking multiple medications and having comorbid condition have been linked to adverse health outcomes including drug interaction and poor adherence to treatment (14).
The clinical pharmacist, as a part of the multidisciplinary team, could reduce MRPs (15). Interventional study done in United State of America (USA) showed that the average of MRPs reduced from 2.8 to 1.95 after intervention of clinical pharmacist (16). Pharmacist-based services can empower patients with heart failure to understand and manage their complex medication regimens through medication reconciliation, identification of drug-drug interactions. In addition, pharmacist-based interventions may improve clinical outcomes, reduce hospital stay, fewer re-admissions and fewer disease events such as HF events or thromboembolism, reuce costs of readmissions and emergency room (17, 18).
MRPs contribute to a high number of morbidities and mortalities worldwide and responsible for undesirable health consequences in patients that often result in hospitalization (19). Studies revealed that one out of six patients admitted because of MRPs (20) and up to 30% of hospital admissions related to MRPs (21). MRPs are relatively common among hospitalized patients and can result in patient morbidity and mortality thus increased cost (7, 22,23). Studies done in different parts of Ethiopia showed that MRPs were high among hospitalized HF patients (24,25, 26). Thus, hospitalization is the primary contributor to the staggering medical cost of HF: $30.7 billion annually (27, 28). Little is known about the extent of MRPs and the clinical pharmacist role in the management of HF patients in Ethiopia. Knowing extent MRPs among HF patients will lead healthcare professionals to optimize drug therapy that may influence health expenses; save lives, improves health, reduces morbidity and mortality and increases quality of life (29, 30). Hence, this study aimed to identify MRPs and predictors among HF patients and evaluate the impact of clinical pharmacist intervention for treatment optimization.
Methods and Participants
Study area and Period
This study was conducted from May 30, 2020 to November 28, 2021 at JMC, which is located in Jimma town; 345 km Southwest of Addis Ababa, the capital. JMC is the only teaching and medical center hospital in the south western part of the country with bed capacity of 600. It provides service for approximately 9000 inpatient and 80,000 outpatient clients per year with a catchment population of about 15 million people. The medical services provided by the JMC include internal medicine, surgery, orthopedics, ophthalmology, pediatrics, gynecology and obstetrics, dermatology, Oncology, psychiatric service, pathology, pharmacy, medical laboratory, intensive care unit, radiology, and others as both inpatient and outpatient services. Medical ward is among the ward which has different unit such as: cardiac unit, renal unit, Stroke unit, Intensive care unit (ICU), pulmonary unit and TB unit. Annually, about 637 HF patients were admitted to JMC.
Study Design and variable
A prospective interventional study design was conducted. All HF patients who admitted to internal medicine ward of JMC were Source Population. Study Population was All HF patients who were admitted to internal medicine ward of JMC during study period and fulfill the inclusion criteria. Heart failure patients’ age ≥15 years and willing to give written consent were included. Heart failure patients died or were discharged before initiation of treatment and with incomplete chart information was excluded. Dependent variable was medication related problems. Independent Variables include Socio demographic characteristics (age, sex, marital status, educational status, residence, medication belief, Cost coverage, occupation, and social drug use), Clinical characteristics (Co morbidity, etiology of HF, LVEF, class and number of drugs, number of drugs per patient, duration of hospital stay, clinical pharmacist interventions).
Sample size determination and sampling technique
The sample size was determined by using the single population proportion formula. By considering the proportion (P) of MRP among HF patients 50 % (45), 95% confidence interval (CI) and 5% marginal error the final minimum sample size was 384. Consecutive sampling technique was used until the required sample size was achieved.
Data collection instrument
Pharmaceutical care network Europe (PCNE) version 9.00 MRP classification was used to classify and document MRPs. It has three primary domains for problems (P1-treatment effectiveness, P2-Treatment Safety and P3-others). There are nine primary domains for causes (C1-drug selection, C2-drug form, C3-dose selection, C4-treatment duration, C5-dispensing, C6-Drug use process, C7-patient related, C8- patient transfer related and C9-Others). Structured collection tool was used to extract relevant information regarding patient demographics and clinical data. Medication belief was measured by belief about medication questionnaire (BMQ), in which the patient’s belief was considered as positive when the average sum of 5-item patient’s medication necessity scale score exceeded the average 5-item medication concerns scale otherwise it was considered as negative (57). ADR was assessed by Naranjo drug reaction probability scale which has also been standardized and validated (58). Lexi comb, Medscape drug interaction checker accessed to check drug-drug, and drug-disease interaction. MRPs were identified by comparing patient’s treatment with guidelines (60-62).
Data collection procedure
Data were collected by two pharmacists and two medical interns. The data collectors were trained for three days before starting data collection. Data were collected through medical record review of patients using a prepared standard checklist and structured questionnaire. Content of checklist include patient details, investigations, current and past medications and medical condition. The structured questionnaire content includes socio-demographic characteristics, drug and disease related questions. Provisional diagnosis was confirmed by physicians after patient stayed at least 24hours and Medication related problems were identified by evaluating the appropriateness of prescription regarding indication, dosage, and safety and by assessing patients. Interventions were done by the principal investigator and two senior clinical pharmacists. After data were collected, clinical pharmacist reviewed patient’s therapy to assess MRPs. For the identified MRPs, interventions were provided through discussion with individual prescriber immediately. Additionally, recommendation was delivered during round and the prescriber acceptance documented. MRPs which are not accepted were further discussed with senior physicians or residents for further interventions.
Data Quality assurance
The questionnaires were prepared in English and translated into Amharic and local language Afan Oromo, and back-translated into English by an independent person to assure its consistency. A pre-test was conducted on 19(5%) study participants by randomly selected patients before the actual data collection to check the consistency and validity of the structured data collection format. Data were compiled, cleared, coded, and checked for consistency. All steps in data collection and recording were closely monitored by the supervisor and any gaps identified were immediately communicated with the data collectors.
Data processing, analysis and presentation
Data were entered into Epidata version 4.6.0.4 and exported to the SPSS version 25 for analysis. First, data were edited and checked for completeness and consistency, then exported into SPSS for descriptive statistical analysis. Categorical variables were described by frequencies and percentages. Continuous variables were presented by means and standard deviations. A bivariate analysis was performed with binary logistic regression to assess association between the MRPs and independent variables. Those variables with a p value<0>
Ethical Consideration
The study was conducted in accordance with the principles of the Declaration of Helsinki and the International Council on Harmonization Guidelines for Good Clinical Practice. The Jimma University institution review board (IRB) granted ethical clearance and approval, and the JMC clinical director office was given a letter of authorization. The internal medical ward unit received a letter from the JUMC clinical director office. By employing identification numbers rather than patient names, confidentiality was guaranteed. Written informed consent was obtained from patients, parent or legal guardian.
Operational definition and definition of terms
Medication related problem: event or circumstance involving drug therapy that actually or potentially interferes with desired health outcomes.
Hospitalized heart failure patients: those patients who have been diagnosed with heart failure and stayed at least 24hours in medical ward
Adverse drug reaction: is a noxious and unintended response to a drug which occurs at doses normally used for the prophylaxis, diagnosis, or treatment of disease that reducing the study period (58).
Poly-pharmacy: defined as concomitant use of five or more prescription medications (4).
Clinical pharmacist interventions: Is any action by a clinical pharmacist that directly results in a change in patient management or therapy.
Comorbidity: presence of other medical condition other than heart failure
Duration of hospital stay: length of days from admission to discharge
Non-compliance: the patient doesn’t understand instruction, cannot afford drug product, prefers not to take medication, and forgets to take medication timely and drug product not available
Insurance:
cost coverage of available medication provided by health institution
Results
Socio-Demographic characteristics of the study participants
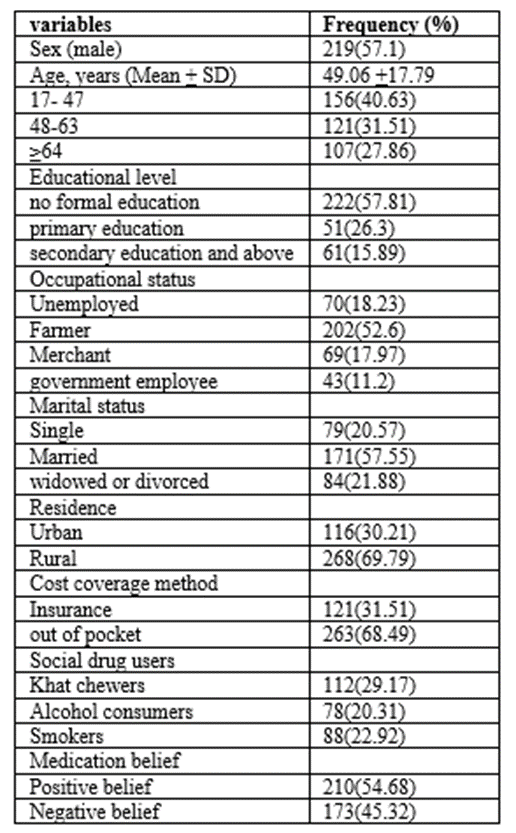
Among 384 study participants included in this study,219(57.1%) were male. The mean ± SD age of the patients was 49.06 +17.79 years. Most156(40.63%) of them were in the age range of 17-47 years. About 268(69.79%) of patients were residing in the rural area. More than half of patients were farmers, married, while 222(57.81%) of participants had no formal education and 133(56.1%) of patients have positive belief (Table1).
Clinical Characteristics of study participants
Of 384 patients included in the study, more than half of the patients had 246(64.1%) comorbid condition. The most common causes of HF were IHD134(34.89%) followed by CRVHD96(25%) and CMP 91(23.69%) and most of them 234(60.94%) are newly diagnosed HF patients. About 210(54.69%) of patients had stayed less than eighteen days in hospital with the mean duration of 18.25 + 7.82 (Table2).
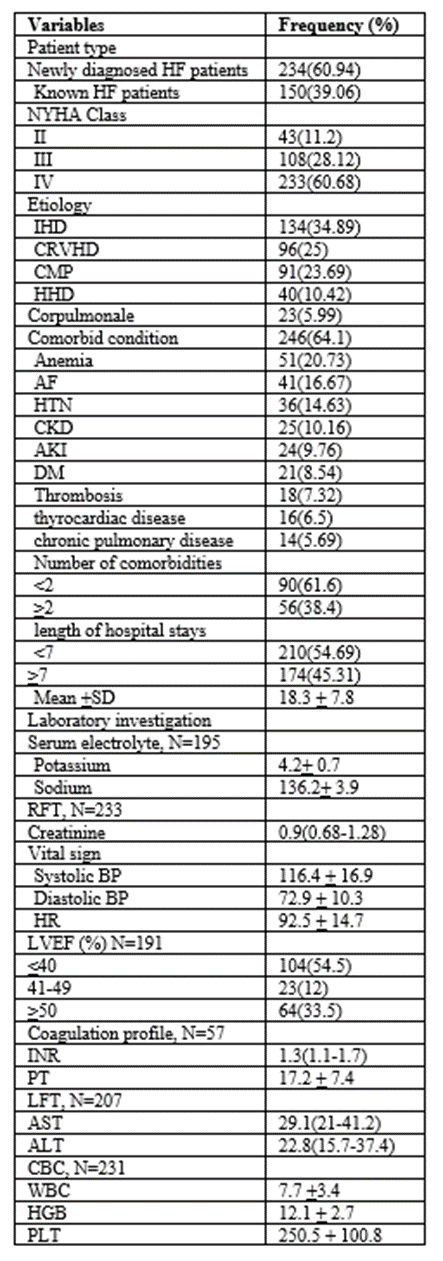
NB: IHD=ischemic heart disease, CRVHD=chronic rheumatic valvular heart disease .HHD=hypertensive heart disease, CMP=cardiomyopathy, NYHA=New York Heart Association, AF= Atrial fibrillation, HTN=hypertension, CKD= chronic kidney disease, AKI= acute kidney injury, DM=diabetes mellitus, BP=blood pressure, HR=heart rate, INR=internationalized normal ratio, PT=prothrombin time, LFT=liver function test, AST=aspartate transaminase, ALT=alanine transaminase, RFT=renal function test, CBC=complete blood count, WBC=white blood cell, HGB=hemoglobin, PLT=platelet
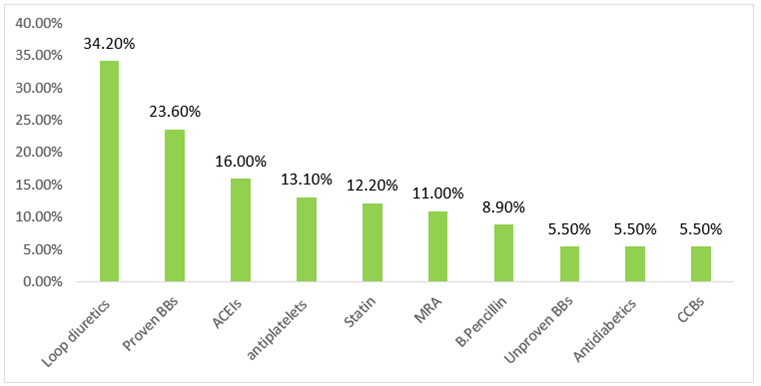
Past medications and Medications during hospital stay
Of the study participants 210(54.69%) patients do have past medication history. The most common drugs were loop diuretics (34.2%), proven BBs (23.6%) ACEIs (16%), antiplatelet (13.1%) (figure1).
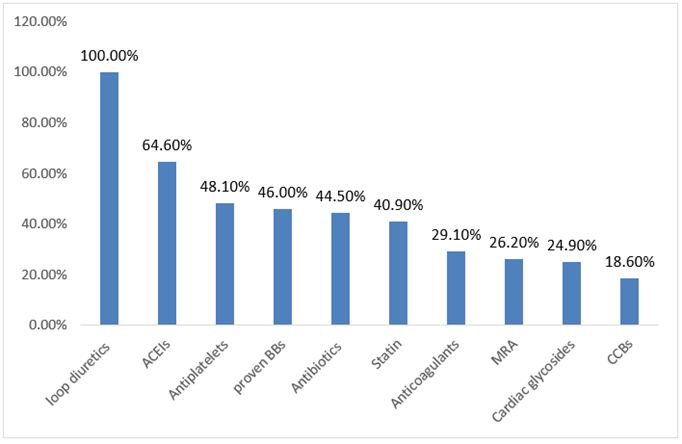
Total of 1442 drugs were prescribed for384 patients during study period. The mean number of drugperpatientwas3.75±1.82. The most commonly prescribed drugs were furosemide384 (100%) followed by enalapril 153(64.6%), antiplatelet 114(48.1%) and proven BBs 109(46%) Among study participants, 146(61.6%) of them had polypharmacy. (figure2).
The prevalence, type and causes of Medication Related Problems
From a total of 384 patients, 231(6 0.15%) patients experienced Medication related problems. A total of 483 MRPs were identified, out of this 40 MRPs were in non-heart failure. The average number of MRP per patient was 1.25+ 1.18. Among Patients experienced MRPs, 130 (61.93%) had 1 MRP, 56(26.67%) 2 MRPs and 45(21.42%) > 3 DRPs. The most commonly found DRPs were treatment effectiveness related (no effect of drug treatment, untreated indication, effect of drug not optimal) 55.46% followed by others (unnecessary drug treatment, compliance and cost effectiveness related) 22.97% and safety related (ADE occur or may occur) 21.57% (figure3).
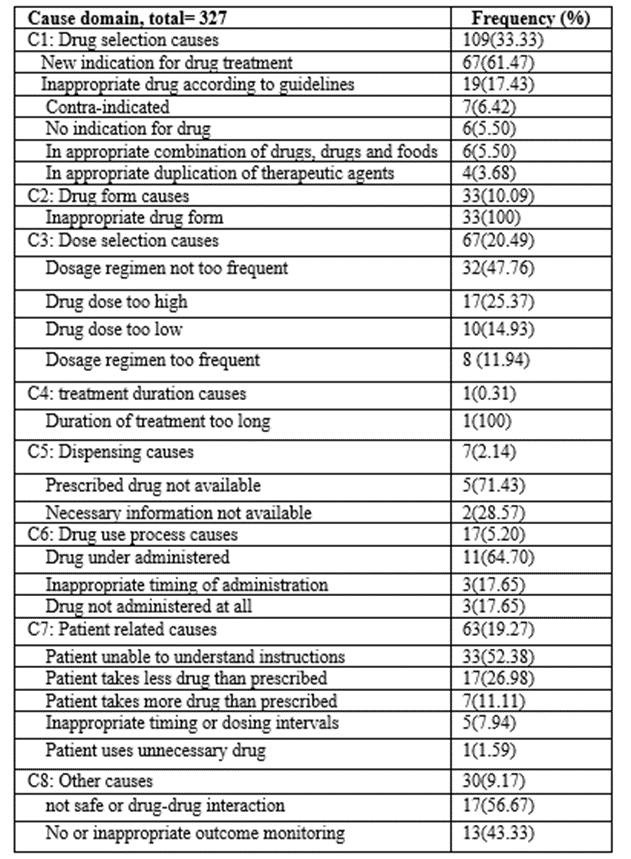
Three hundred twenty-seven causes of MRPs were identified. Drug selection (33.33%), dose selection (20.49%) and patient related were the most common causes (table 3).
Drugs involved in Medication Related Problems
There were different classes of drugs involved among HF patients with Medication related problems. The most frequently encountered drug classes were beta-blockers (34%), of which 11% was unproven BBs. Angiotensin converting enzyme inhibitors and antithrombotic were about 24 % and 22% respectively. From the antithrombotic, anticoagulant was about six percent (Figure 4).
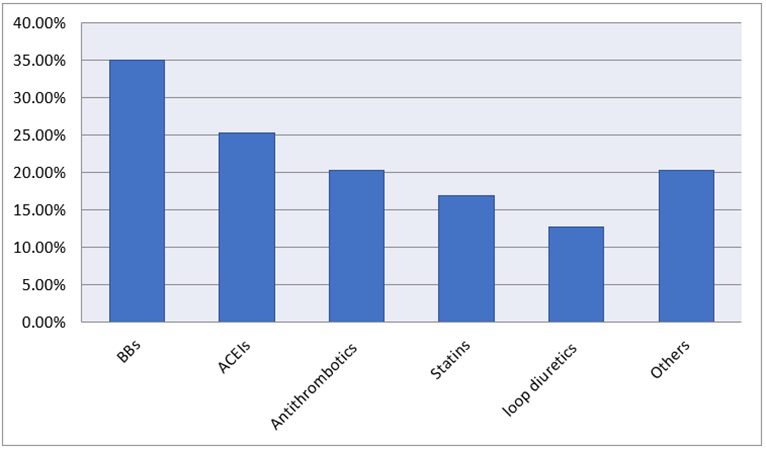
Others: Ferroussulphate (4.6%), Spironolactone (3.8%), digoxin (2.1%), thionamides (2.1%), antibiotics (1.7%), calcium channel blockers (1.7%), omeprazole (1.3%), cimetidine (0.8%), amiodarone (0.8%), antiTB (0.8%) and hydrochlorothiazide (0.4%)
Intervention, acceptance rate and outcome of intervention of medication related problems
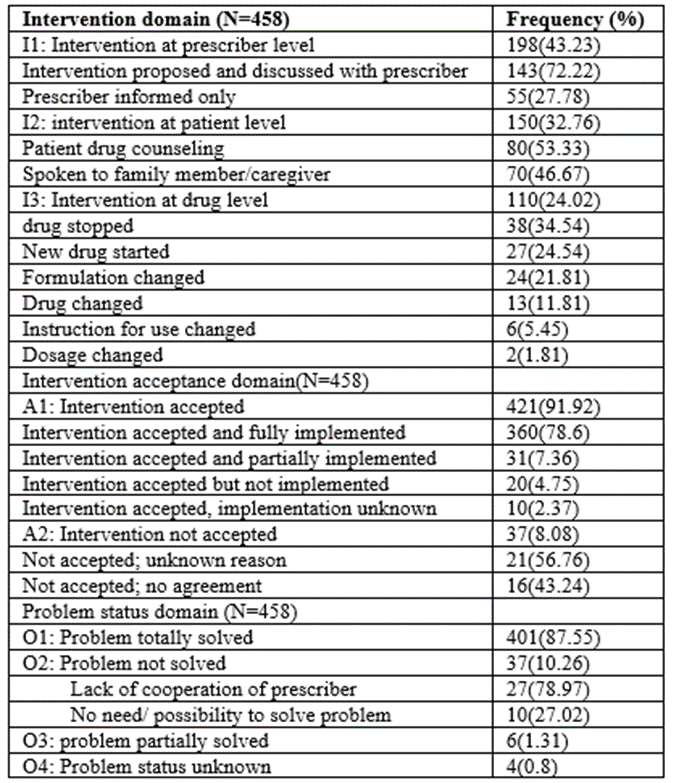
For the identified MRPs, a total of 458 intervention were delivered at different levels, out of these 198(43.23%) interventions were done at prescriber level, 421(91.92%) of them were accepted. After intervention, 401(87.55%) and 37(10.26%) of the problems were solved and not solved respectively (table 4).
Predictors of Medication related problems
In crude analysis using binary logistic regression: Sex, age, chat chewers, alcohol drinkers, comorbidity, hospital stay and polypharmacy were found to predispose HF patients for MRPs with statistically significant association. Independent predictors for encountered MRPs were identified using multivariate logistic regression, finally alcohol drinker (AOR; 3.25, 95% CI (1.46-7.23), P=0.004), prolonged hospital stay (AOR; 2.77, 95% CI 1.93-7.37, P=0.001), presence of comorbid condition (AOR: 2.59, CI 1.35-4.96, P=0.004) and polypharmacy (AOR; 2.94, 95% CI 1.54-5.61, P=0.02) were found to be independent predictors of MRPs.
According to our finding HF patients stay in hospital greater than 18 days are 2.77(AOR; 2.45, 95% CI 2.32-5.34) times at risk for MRPs than those stay in hospital less than 18 days, HF patients had comorbid condition were 2.59(AOR: 2.59, CI 1.35-4.96) times likely to encounter MRPs than those without comorbid condition. HF patients who Alcohol drinker was 3.25(AOR; 3.25, 95% CI (1.46-7.23) times likely to encounter MRPs than those not chew khat (Table 5).
| MRP Status | COR (95%CI) | p-value | AOR (95%CI) | p-value | |
Variable | Yes | No |
|
|
|
|
Sex | 88(56.1%) | 34(42.5%) |
| 0.049 | 1.17(0.56-2.45) | 0.681 |
Age group |
|
|
|
|
|
|
< 47> | 72(45.9%) | 34(42.5%) |
|
|
|
|
48-63 | 50(31.8%) | 21(26.3%) | 1.12(0.59-2.16) | 0.725 | 1.06(0.49-2.29) | 0.875 |
> 64 | 35(22.3%) | 25(31.2%) | 0.66(0.34-1.27) | 0.216 | 0.52(0.24-1.12) | 0.097 |
Residence | 110(70.1%) | 61(76.2%) | 0.73(0.39-1.35) | 0.32 |
|
|
Alcohol drinker | 50(31.8%) | 12(15%) | 2.648(1.316-5.33) | 0.006 | 3.25(1.46-7.23) | 0.004* |
Khat chewing | 24(15.3%) | 7(8.7%) | 1.88(0.77-4.58) | 0.16 | 1.48(0.49-4.41) | 0.478 |
Smokers | 28(17.8%) | 10(12.5%) | 1.52(0.69-3.31) | 0.29 |
|
|
Payment method |
|
|
|
|
|
|
Insurance | 49(31.2%) | 22(27.5%) |
|
|
|
|
Out of pocket | 108(68.8%) | 58(72.5%) | 0.84(0.461-1.52) | 0.56 |
|
|
Medication belief |
|
|
|
|
|
|
Positive belief | 92(58.6%) | 41(51.3%) |
|
|
|
|
Negative belief | 65(41.4%) | 39(48.7%) | 0.74(0.43-1.28) | 0.282 |
|
|
Comorbidity | 114(72.6%) | 32(40%) | 3.98(2.25-7.02) | <0> | 2.59(1.35-4.96) | 0.004* |
polypharmacy | 119(75.8%) | 32(40%) | 4.69(2.64-8.37) | <0> | 2.94(1.54-5.61) | 0.001* |
Duration of hospital stay |
|
|
|
|
|
|
<7days> | 72(45.9%) | 61(76.3%) |
|
|
|
|
≥7 days | 85(54.1%) | 19(23.7%) | 3.79(2.07-6.93) | <0> | 2.77(1.93-7.37) | <0> |
Table 5: Predictors of MRPs among heart failure patients at JMC, May 2020 to November 28, 2021
Discussion
Out of 231(60.15%) patients experienced MRPs, 56% of MRPs were found in males, which is similar with the result of two studies done in India. This might be due to increased medication use because of comorbid condition was higher in males and other various risk factors like smoking, alcoholism and chewing chats compared to females (34, 36). The prevalence of MRP was found to be 60.15% and average of MRPs per patient was 1.25+ 1.18, which was lower than study conducted at JUMC (83.5%) and 2.6 + 1.8, the difference could be due to setting difference where our study conducted in hospitalized patients in which senior physicians and clinical pharmacists are available more frequently than being at ambulatory(30).However, it is almost in line with study conducted at TASH (65.5%) (23) and GUH 63.4% or average 1.17 + 1.1 per patient (41). Moreover, study done on hospitalized heart failure patient at JUMC in 2014 showed that MRPs was about 91% (41). This difference from current study could be due to there were no clinical pharmacists’ ward (when clinical pharmacists were not involved in the ward) in the previous study.
The most common DRPs in our study were treatment effectiveness related problem (55.46%) and the least was ADE occurrence (21.57%). Of the treatment effectiveness related problem, suboptimal drug treatment and untreated indication were about 28% and 25% respectively. This finding was in line with study conducted in Barcelona which showed that suboptimal drug therapy (31%) and probability of ADE occurrence (16%) (40). In contrary to this finding, study conducted at JUSH in 2014 showed that treatment effectiveness related was about 83%, of which suboptimal drug therapy and untreated indication were about 55% and 27% respectively (29). Whereas, study conducted at TASH treatment effectiveness related problem (39%) was lower than our findings (28). Furthermore, study done in USA on outpatient heart failure showed that treatment effectiveness related problem was about 36.8%(37). The discrepancy could be due to difference in classification of MRPs, study setting, where studies done at JUMC, TASH and USA were at ambulatory clinic at which senior physicians, residents and clinical pharmacists less frequently available than in medical wards.
About 91% of patients were compliant to medication which was comparable with study done in Netherlands (98.6%) (39). Non-adherence was about 9%, which was in line with studies done at ambulatory care of JUSH (9%), Harar 12 % (25), Barcelona and Spain (14%) (29,37). However, study done at TASH showed that, non-compliance was about 45% (30). The difference could be due to difference in compliance assessment method and in our study, patients may be more access to information about medication from health professional and caregiver. In our study, one third of MRPs was due to inappropriate drug selection and about 21% was dose selection related problem. Indication (need additional drug therapy) was about 60
Conclusion
Our study showed that, the prevalence of MRPs was high among HF patients at JMC. The most common identified MRPs were treatment effectiveness related problems which mainly includes suboptimal effect of drug and untreated indication. Prolonged hospital stay, comorbidity and polypharmacy were found to be independent predictors of MRPs. Clinical intervention acceptance rate and implementation including totally solved outcome of intervention were high.
List of acronyms and abbreviations
ACEIs: Angiotensin converting enzyme inhibitors
ADR: Adverse drug reaction
AHA: American heart association
ARB: Angiotensin receptor blocker
BBs: Beta blockers
BMQ: Belief about medication questionnaire
CP: Clinical pharmacist
CVD: Cardiovascular disease
MRP: Medication related problems
ESC: European Society of Cardiology
ESTG: Ethiopian Standard treatment guideline
HF: Heart Failure
ICU: Intensive care unit
JMC: Jimma Medical Center
MRA: Mineralocorticoid receptor antagonist
NSAID: Non-steroidal anti-inflammatory drugs
PCNE: Pharmaceutical care Network Europe
TASH: UK: United Kingdom
Acknowledgment
We would like to thank Jimma University, data collectors and all study participants.
Competing Interests
All authors have no competing interests with the material presented in this manuscript
Funding
This research was funded by Jimma University Institute of health. The funding body had no any role in the design of the study, data collection, and analysis, interpretation of data and in writing the manuscript.
Authors’ contributions
W.A. and T.G wrote the main manuscript, prepared tables and figures. W.A and T.G have made substantial contributions to the conception, design of the work, the acquisition, analysis and interpretation of data. All authors also have drafted the work, substantively revised it and approved the submitted version. All authors read and approved the final manuscript.
Availability of data and materials
Readers who will require data and materials of the current study can communicate and get from the corresponding author with a reasonable request.
References
- Jessup M, Drazner MH, Book W, Cleveland JC, Dauber I, et al. (2017). 2017 ACC/AHA/HFSA/ISHLT/ACP Advanced Training Statement on Advanced Heart Failure and Transplant Cardiology. Journal of the American College of Cardiology. 69(24):2977-3001.
View at Publisher | View at Google Scholar - Ponikowski P, Anker SD, AlHabib KF, Cowie MR, Force TL, et al. (2014). Heart failure: preventing disease and death worldwide. ESC Heart Failure. 1(1):4-25.
View at Publisher | View at Google Scholar - Savarese G, Lund LH. (2017). Global public health burden of heart failure. Cardiac Failure Review. 3(1):7.
View at Publisher | View at Google Scholar - Beezer J, Al Hatrushi M, Kurdi A, Forsyth P. (2020). Polypharmacy definition and prevalence in heart failure: a systematic review. Heart Failure Reviews. 1-28.
View at Publisher | View at Google Scholar - Cipolle RJ, Strand LM, Morley PC. (2012). Pharmaceutical care practice: the patient-centered approach to medication management: McGraw Hill Professional.
View at Publisher | View at Google Scholar - Dall Agnol R. (2019). Intervenções Decorrentes Do Acompanhamento Farmacoterapêutico De Pacientes Pediátricos Durante O Tratamento Quimioterápico Na Internação Hospitalar.
View at Publisher | View at Google Scholar - Srikanth A. (2017). Assessment of drug related problems and its associated factors among medical ward patients in university of gondar teaching hospital, northwest Ethiopia: a prospective cross-sectional study. Journal of Basic and Clinical Pharmacy. 8.
View at Publisher | View at Google Scholar - Knafl GJ, Riegel B. (2014). What puts heart failure patients at risk for poor medication adherence? Patient preference and adherence. 8:1007.
View at Publisher | View at Google Scholar - Franco BB, Mclean G, Mair FS, Roger VL, Guthrie B, et al. (2017). Comorbidity and polypharmacy in chronic heart failure: a large cross-sectional study in primary care. British Journal of General Practice. 67(658): e314-e20.
View at Publisher | View at Google Scholar - Al-Azzam SI, Alzoubi KH, AbuRuz S, Alefan Q. (2016). Drug-related problems in a sample of outpatients with chronic diseases: a cross-sectional study from Jordan. Therapeutics and clinical risk management. 12:233.
View at Publisher | View at Google Scholar - Mentz RJ, Felker GM. (2013). Noncardiac comorbidities and acute heart failure patients. Heart Failure Clinics. 9(3):359-367.
View at Publisher | View at Google Scholar - Unlu O, Levitan EB, Reshetnyak E, Kneifati-Hayek J, Diaz I, et al. (2020). Polypharmacy in older adults hospitalized for heart failure. Circulation: Heart Failure. 13(11): e006977.
View at Publisher | View at Google Scholar - Handayany GN, Husain N, Kurniati Y. (2020). Research Study of Management of Drug Related Problems (DRPS) in Patients with Congestive Heart Failure (CHF). Systematic Reviews in Pharmacy. 12(1):1452-1458.
View at Publisher | View at Google Scholar - Adem F, Abdela J, Edessa D, Hagos B, Nigussie A, et al. (2021). Drug-related problems and associated factors in Ethiopia: a systematic review and meta-analysis. Journal of Pharmaceutical Policy and Practice. 14(1):1-24.
View at Publisher | View at Google Scholar - Georgiev KD, Hvarchanova N, Georgieva M, Kanazirev B. (2019). The role of the clinical pharmacist in the prevention of potential drug interactions in geriatric heart failure patients. International Journal of Clinical Pharmacy. 41(6):1555-1561.
View at Publisher | View at Google Scholar - Yates L, Valente M, Wadsworth C. (2020). Evaluation of pharmacist medication review service in an outpatient heart failure clinic. Journal of Pharmacy Practice. 33(6):820-826.
View at Publisher | View at Google Scholar - West LM, Williams JB, Faulkenberg KD. (2019). The impact of pharmacist-based services across the spectrum of outpatient heart failure therapy. Current Treatment Options in Cardiovascular Medicine. 21(10):1-21.
View at Publisher | View at Google Scholar - Viktil KK, Blix HS. (2008). The impact of clinical pharmacists on drug‐related problems and clinical outcomes. Basic & Clinical Pharmacology & Toxicology. 102(3):275-280.
View at Publisher | View at Google Scholar - Dixon-Woods M, Baker R, Charles K, Dawson J, Jerzembek G, et al. (2014). Culture and behaviour in the English National Health Service: overview of lessons from a large multimethod study. BMJ Quality & Safety. 23(2):106-115.
View at Publisher | View at Google Scholar - Mannesse CK, Derkx F, De Ridder M, Man In't Veld A, Van der Cammen T. (2020). Contribution of adverse drug reactions to hospital admission of older patients. Age and Ageing. 29(1):35-39.
View at Publisher | View at Google Scholar - Salvi F, Marchetti A, D’Angelo F, Boemi M, Lattanzio F, et al. (2012). Adverse drug events as a cause of hospitalization in older adults. Drug Safety. 35(1):29-45.
View at Publisher | View at Google Scholar - Ernst FR, Grizzle AJ. (2001). Drug-related morbidity and mortality: updating the cost-of-illness model. Journal of the American Pharmaceutical Association. 41(2):192-199.
View at Publisher | View at Google Scholar - Al Hamid A, Aslanpour Z, Aljadhey H, Ghaleb M. (2016). Hospitalisation resulting from medicine-related problems in adult patients with cardiovascular diseases and diabetes in the United Kingdom and Saudi Arabia. International Journal of Environmental Research and Public Health. 13(5):479.
View at Publisher | View at Google Scholar - Tegegne GT, Gelaw BK, Defersha AD, Yimam B, Yesuf E. (2014). Drug therapy problem among patients with cardiovascular diseases in Felege Hiwot referral Hospital, Northeast, Bahir Dar Ethiopia. IAJPR. 4:2828-2838.
View at Publisher | View at Google Scholar - Gelchu T, Abdela J. (2019). Drug therapy problems among patients with cardiovascular disease admitted to the medical ward and had a follow-up at the ambulatory clinic of Hiwot Fana Specialized University Hospital: The case of a tertiary hospital in eastern Ethiopia. Sage Open Medicine. 7:2050312119860401.
View at Publisher | View at Google Scholar - Gizaw K, Dubale M. (2017). Drug related problems and contributing factors among adult ambulatory patients with cardiovascular diseases at Gebretsadik Shawo General Hospital, Bonga, South west Ethiopia. Journal of Natural Sciences Research. 7(1):9-16.
View at Publisher | View at Google Scholar - Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, et al. (2013). Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circulation: Heart Failure. 6(3):606-619.
View at Publisher | View at Google Scholar - Seid E, Engidawork E, Alebachew M, Mekonnen D, Berha AB. (2020). Evaluation of drug therapy problems, medication adherence and treatment satisfaction among heart failure patients on follow-up at a tertiary care hospital in Ethiopia. PLOS one. 15(8): e0237781.
View at Publisher | View at Google Scholar - Niriayo YL, Kumela K, Kassa TD, Angamo MT. (2018). Drug therapy problems and contributing factors in the management of heart failure patients in Jimma University Specialized Hospital, Southwest Ethiopia. PLOS one. 13(10): e0206120.
View at Publisher | View at Google Scholar - Peterson C, Gustafsson M. (2017). Characterization of drug-related problems and associated factors at a clinical pharmacist service-naive Hospital in Northern Sweden. Drugs-Real World Outcomes. 4(2):97-107.
View at Publisher | View at Google Scholar - Abraham RR. (2014). Drug related problems and reactive pharmacist interventions for inpatients receiving cardiovascular drugs. International Journal of Basic Medical Sciences and Pharmacy. 3(2).
View at Publisher | View at Google Scholar - Hsu W-T, Shen L-J, Lee C-M. (2016). Drug-related problems vary with medication category and treatment duration in Taiwanese heart failure outpatients receiving case management. Journal of the Formosan Medical Association. 115(5):335-342.
View at Publisher | View at Google Scholar - Biradar SM, Indu P, Kalyane N, Ambali AP, Naikwadi A, et al. (2017). Impact of drug-related problems and clinical pharmacist interventions on therapeutic outcomes of the patients admitted to a tertiary care hospital. International Journal of Medical Science and Public Health. 6(5):867-873.
View at Publisher | View at Google Scholar - Shareef J, Sandeep B, Shastry C. (2014). Assessment of drug related problems in patients with cardiovascular diseases in a tertiary care teaching hospital. Journal of Pharmaceutical Care. 70-76.
View at Publisher | View at Google Scholar - Mohammed S, Poudel S, Laloo F, Madhur A, Robert R, et al. (2017). Assessment of drug-related problems in a tertiary care teaching hospital, India. Asian J Pharm Clin Res. 10:310-313.
View at Publisher | View at Google Scholar - Westberg SM, Derr SK, Weinhandl ED, Adam TJ, Brummel AR, et al. (2017). Drug therapy problems identified by pharmacists through comprehensive medication management following hospital discharge. Journal of Pharmacy Technology. 33(3):96-107.
View at Publisher | View at Google Scholar - Gastelurrutia P, Benrimoj SI, Espejo J, Tuneu L, Mangues MA, et al. (2011). Negative clinical outcomes associated with drug-related problems in heart failure (HF) outpatients: impact of a pharmacist in a multidisciplinary HF clinic. Journal of Cardiac Failure. 17(3):217-23.
View at Publisher | View at Google Scholar - Dempsey JT, Matta LS, Carter DM, Stevens CA, Stevenson LW, et al. (2017). Assessment of drug therapy-related issues in an outpatient heart failure population and the potential impact of pharmacist-driven intervention. Journal of Pharmacy Practice. 30(3):318-23.
View at Publisher | View at Google Scholar - Abdela OA, Bhagavathula AS, Getachew H, Kelifa Y. (2016). Risk factors for developing drug-related problems in patients with cardiovascular diseases attending Gondar University Hospital, Ethiopia. Journal of Pharmacy & Bioallied Sciences. 8(4):289.
View at Publisher | View at Google Scholar - Wendie TF, Angamo MT. (2020). Drug-Therapy Problems and Predictors among Hospitalized Heart-Failure Patients: A Prospective Observational Study. Drug, Healthcare and Patient Safety. 12:281.
View at Publisher | View at Google Scholar - Sharif-Askari NS, Sulaiman SAS, Sharif-Askari FS, Hussain AAS. (2015). Adverse drug reaction-related hospitalisations among patients with heart failure at two hospitals in the United Arab Emirates. International Journal of Clinical Pharmacy. 37(1):105-112.
View at Publisher | View at Google Scholar - Belayneh YM, Amberbir G, Agalu A. (2018). A prospective observational study of drug therapy problems in medical ward of a referral hospital in northeast Ethiopia. BMC Health Services Research. 18(1):1-7.
View at Publisher | View at Google Scholar - Aggarwal B, Pender A, Mosca L, Mochari-Greenberger H. (2015). Factors associated with medication adherence among heart failure patients and their caregivers. Journal of Nursing Education and Practice. 5(3):22.
View at Publisher | View at Google Scholar - Sharma S, Chhetri HP, Alam K. (2014). A study of potential drug-drug interactions among hospitalized cardiac patients in a teaching hospital in Western Nepal. Indian Journal of Pharmacology. 46(2):152.
View at Publisher | View at Google Scholar - Urbina O, Ferrández O, Luque S, Grau S, Mojal S, et al. (2015). Patient risk factors for developing a drug-related problem in a cardiology ward. Therapeutics and Clinical Risk Management. 11:9.
View at Publisher | View at Google Scholar - Murtaza G, Khan MYG, Azhar S, Khan SA, Khan TM. (2016). Assessment of potential drug–drug interactions and its associated factors in the hospitalized cardiac patients. Saudi Pharmaceutical Journal. 24(2):220-225.
View at Publisher | View at Google Scholar - Yusuff KB, Tayo F. (201). Frequency, types and severity of medication use-related problems among medical outpatients in Nigeria. International Journal of Clinical Pharmacy. 33(3):558.
View at Publisher | View at Google Scholar - Garedow AW, Mulisa Bobasa E, Desalegn Wolide A, Kerga Dibaba F, Gashe Fufa F, et al. (2019). Drug-related problems and associated factors among patients admitted with chronic kidney disease at Jimma University Medical Center, Jimma Zone, Jimma, Southwest Ethiopia: a hospital-based prospective observational study. International Journal of Nephrology.
View at Publisher | View at Google Scholar - Tigabu BM, Daba D, Habte B. (2014). Drug-related problems among medical ward patients in Jimma university specialized hospital, Southwest Ethiopia. Journal of Research in Pharmacy Practice. 3(1):1.
View at Publisher | View at Google Scholar - Sewagegn N, Fekadu S, Chanie T. (2015). Adherence to self-care behaviours and knowledge on treatment among heart failure patients in Ethiopia: the case of a tertiary teaching hospital. Journal of Pharmaceutical Care & Health Systems. 10:2376-419.
View at Publisher | View at Google Scholar - Anderson SL, Marrs JC. (2018). A review of the role of the pharmacist in heart failure transition of care. Advances in Therapy. 35(3):311-323.
View at Publisher | View at Google Scholar - Shah Jainam V, Patni Kalyani N, Deshpande Shrikalp S, Patel Varsha J. (2016). A Study of Role of Clinical Pharmacist in Medication Review and Patient Education. Inter J Pharm Sci Res. 7(3):160-167.
View at Publisher | View at Google Scholar - Celin A, Seuma J, Ramesh A. (2012). Assessment of drug related problems in stroke patients admitted to a South Indian tertiary care teaching hospital. Indian J Pharm Pract. 5(4):28-33.
View at Publisher | View at Google Scholar - Acheampong F, Nkansah FA, Anto BP. (2016). Drug-related problems and their clinical interventions in a Ghanaian teaching hospital. Safety in Health. 2(1):1-7.
View at Publisher | View at Google Scholar - Babelghaith SD, Wajid S, Alrabiah Z, Othiq MAM, Alghadeer S, et al. (2020). Drug-related problems and pharmacist intervention at a general hospital in the Jazan Region, Saudi Arabia. Risk Management and Healthcare Policy. 13:373.
View at Publisher | View at Google Scholar - Gökçekuş L, Mestrovic A, Basgut B. (2016). Pharmacist intervention in drug-related problems for patients with cardiovascular diseases in selected community pharmacies in Northern Cyprus. Tropical Journal of Pharmaceutical Research. 15(10):2275-2281.
View at Publisher | View at Google Scholar - Tsianou K, Giannakeas N, Tsipouras M, Tzallas A, Skamnelos A, et al. (2017). Accessing patient views about medication in chronic conditions using the Beliefs about Medicine Questionnaire (BMQ): a review study. J Drug Res Dev. 3(2):1-9.
View at Publisher | View at Google Scholar - Tox L. Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): national institute of diabetes and digestive and kidney diseases. (2012).
View at Publisher | View at Google Scholar - Hailu BY, Berhe DF, Gudina EK, Gidey K, Getachew M. (2020). Drug related problems in admitted geriatric patients: the impact of clinical pharmacist interventions. BMC Geriatrics. 20(1):1-8.
View at Publisher | View at Google Scholar - Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, et al. (2013). 2013 ACCF/AHA guideline for the management of heart failure: A report of the american college of cardiology foundation/american heart association task force on practice guidelines. Circulation. 128(16):240–327.
View at Publisher | View at Google Scholar - Ministry of Health of Ethiopia. (2016). Guidelines on Clinical and Programmatic Management of Major Non-Communicable Diseases. ResearchGate. 220.
View at Publisher | View at Google Scholar - Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, et al. (2016). 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J.
View at Publisher | View at Google Scholar
