

Review Article | DOI: https://doi.org/10.31579/2834-5029/016
Management of HBV/HIV Co-Infection
- Rehan Haider *
Riggs pharmaceutical, Department of Pharmacy, University of Karachi, Pakistan.
*Corresponding Author: Rehan Haider, Riggs pharmaceutical, Department of Pharmacy, University of Karachi, Pakistan.
Citation: Haider R., (2023), Management of HBV/HIV Co-Infection, International Journal of Biomed Research, 2(2): DOI:10.31579/2834-5029/016
Copyright: © 2023, Rehan Haider, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 March 2023 | Accepted: 28 March 2023 | Published: 04 April 2023
Keywords: liver/hepatitis; antiretroviral therapy; antiviral therapy; pathogenesis; reverse transcriptase inhibitors
Abstract
The prevalence and transmission routes of HBV co-infection in the HIV+ population vary substantially by geographic region. In the United States and Europe, the majority of HIV-positive gay men have evidence of past HBV infection, and 5–10% show persistence of HBs antigen, with or without replicative hepatitis B as defined by the presence of HBV DNA. Overall, rates of HBV/HIV co-infection are slightly lower among intravenous drug users compared to gay men and much lower among people infected through heterosexual contact. In endemic regions of Africa and Asia, the majority of HBV infections are transmitted vertically at birth or before the age of 5 through close contact within households, medical procedures, and traditional scarification. The prevalence among youth in most Asian countries has substantially decreased since the introduction of vaccination on a nationwide scale. In Europe, vaccination of children and members of risk groups is promoted and reimbursed by health care systems in most countries. The natural history of hepatitis B is altered by simultaneous infection with HIV. Immune control of HBV is negatively affected, leading to a reduction in HBs-antigen seroconversion. If HBV persists, the HBV DNA levels are generally higher in HIV-positive patients not on antiretroviral therapy. In addition, with the progression of cellular immune deficiency, reactivation of HBV replication despite previous HBs-antigen seroconversion may occur. However, after immune recovery due to antiretroviral therapy, He-antigen and HBs-antigen seroconversion occurs in a higher proportion of patients compared to HBV mono infected patients treated for chronic hepatitis B. In untreated HIV infection, faster progression to liver cirrhosis is reported for HBV/HIV-co-infected patients Moreover, hepatocellular carcinoma may develop at an earlier age and is more aggressive in this population.
Introduction
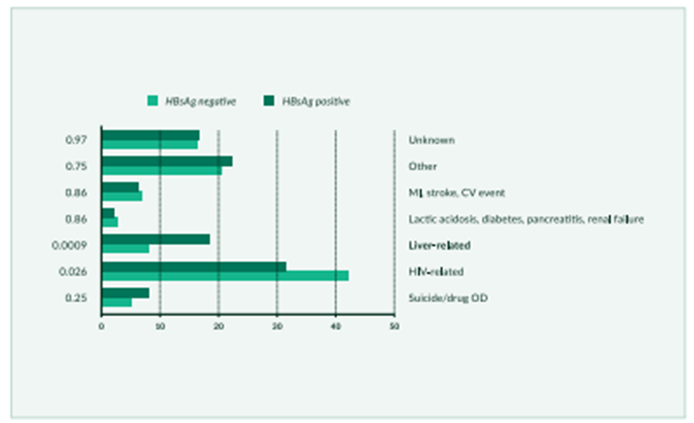
Being HBV-coinfected results in increased mortality for HIV-positive individuals, even after the introduction of effective antiretroviral therapy (ART), as demonstrated by an analysis of the Euro SIDA Study, which shows a 3.6-fold higher risk of liver-related deaths among HBsAg-positive patients compared to HBsAg negative individuals (Konopnicki 2005, Nikolopoulos 2009) [16] (Figure 1). In the Multicenter AIDS Cohort Study (MACS), an 8-fold increased risk of liver-related mortality was seen among HBV/HIV co-infected compared to HIV-mono infected individuals, particularly among subjects with low nadir CD4+ cell counts. Even at present, despite the widespread use of tenofovir, HBV/HIV coinfection is still associated with increased morbidity (Crowell 2014) [18], and liver-related deaths in HBV/HIV-infected patients still do occur (Rosenthal 2014) [19].The beneficial impact of treatment of HBV in HBV/HIV coinfection was first demonstrated by data from a large cohort showing a reduction in mortality with lamivudine treatment compared to untreated patients (Puoti 2004, Brau 2007)This result is even more remarkable because lamivudine is the least effective HBV polymerase inhibitor due to the rapid development of drug resistance. In general, because of its limited long-term efficacy, lamivudine monotherapy cannot be considered an appropriate therapy for either mono HBV infection or HBV/HIV coinfection.
In addition, two large cohort studies (EuroSIDA and MACS) plus data from HBV mono-infection studies showing a reduction in morbidity and mortality established the need to treat chronic hepatitis B in HBV/HIV-co-infected patients.
Treatment of chronic hepatitis B in HBV/HIV-co-infected patients on antiretroviral therapy
In the well-known, beginning hepatitis B therapy depends on the diploma of liver fibrosis and the HBV DNA level. however, as the artwork is now encouraged for all HIV sufferers unbiased of CD4-be counted to reduce HIV-associated morbidity and mortality and to prevent HIV transmission, all HBV/HIV-co-infected patients are considered eligible for art with the aid of cutting-edge hints (e.g., every 2016). The previous complicated recommendations for a way to deal with continual hepatitis B in patients without artwork are obsolete. As antiretroviral capsules which can be additionally lively towards HBV can commonly be used, interferon-based total treatment of HBV is now not often indicated. statistics within the literature for HIV-co-infected patients on interferon therapy for HBV infection are restrained and no longer very encouraging. In addition, intensified treatment research combining pegylated interferon with adefovir or intensifying TDF therapy with pegylated interferon for 12 months confirmed no boom in HBV seroconversion quotes (Ingiliz 2008. In widespread, tenofovir is the usual care for HBV in HIV-co-infected patients, because of its strong HBV polymerase hobby and antiretroviral efficacy. Tenofovir has been a protracted-acting and effective therapy in the giant majority of dealt with HBV/HIV-co-infected patients (van Bömmel 2004, Mathews 2009, Martin-Carbonero 2011, Thibaut, its antiviral efficacy isn’t impaired in HBV/HIV-coinfected as compared to HBV-mono infected sufferers. No conclusive pattern of resistance mutations has been recognized in research or cohorts (Snow-Lampart 2011). [28] These data are nonetheless legitimate at the cease of 2016. In idea, resistance might also arise in sufferers on lengthy-time period therapy, as with some other antivirals. For patients with HBV DNA <2000>
The potentially nephrotoxic effect of TDF is a concern. Although nephrotoxicity is rarely observed in HIV-negative patients treated with TDF monotherapy renal impairment has been more frequently reported in HIV-positive patients using TDF as a component in ART and may be associated in particular with the combined use of TDF and ritonavir-boosted HIV protease inhibitors (Mauss 2005, Fux 2007, Goicoechea 2008, In addition, the recently approved cytochrome P450 3A inhibitor cobicistat can also increase creatinine levels. Regular monitoring of renal function in HBV/HIV-co-infected patients, including estimated glomerular filtration rate (eGFR) and assessment of proteinuria, is necessary. In the case of a reduced eGFR, TDF should be substituted by TAF or should be dosed at a reduced frequency according to the label. In the case of significant proteinuria, TDF should also be replaced by TAF. Alternatively, in specific situations in the case of tenofovir-associated nephrotoxicity, tenofovir can also be replaced by entecavir.
Conclusion
The number of available HBV polymerase inhibitors for chronic hepatitis B has increased substantially over the last few years. In general, the choice is confined to two mostly non-cross-resistant classes, the nucleotide, and nucleoside compounds HBV/HIV co-infected patients, ART is indicated to treat both infections simultaneously. The HBV treatment of choice is tenofovir. Due to the rapid development of resistance when HBV is not fully suppressed HBV monotherapy with either lamivudine or emtricitabine should not generally be considered. A combination of tenofovir plus lamivudine or emtricitabine as a primary combination therapy has theoretical advantages over tenofovir alone, but studies supporting this concept have not been published to date. However, as tenofovir is combined with emtricitabine or lamivudine in most antiretroviral regimens today. This seems to be a more theoretical argument and not reflected by reality. In general, the treatment of HBV as a viral disease follows the same rules as HIV therapy, aiming at full suppression of the replication of the virus to avoid the development of resistance. Successful viral suppression of hepatitis B results in the inhibition of necro-inflammatory activity, reversion of fibrosis, and most importantly a decrease in the incidence of hepatic decompensation and hepatocellular carcinoma.
Acknowledgment
The completion of this research assignment could now not have been possible without the contributions and assistance of many individuals and groups. We're. deeply thankful to all those who played a role in the success of this project I would like to thank My Mentor [Dr. Naweed Imam Syed Prof branch of mobile Biology at the University of Calgary for their useful input and guidance for the duration of the research system. Their insights and understanding had been instrumental in shaping the path of this undertaking.
Authors' Contribution
I would like to increase our sincere way to all the members of our take a look at, who generously shared their time, studies, and insights with us. Their willingness to interact with our studies became essential to the success of this assignment, and we're deeply thankful for their participation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors declare no conflict-of-interest.
References
- Alter M. (2006). Epidemiology of viral hepatitis and HIV co-infection. J Hepatol; 44:69.
View at Publisher | View at Google Scholar - Konopnicki D, Mocroft A, de Wit S, et al. (2005), Hepatitis B and HIV: prevalence, AIDS progression, response to highly active antiretroviral therapy and increased mortality in the EuroSIDA cohort. AIDS; 19:593-601.
View at Publisher | View at Google Scholar - M, Puoti M, Camino N, Soriano V. (2003), Treatment of chronic hepatitis B in the human immunodeficiency virus-infected patient: present and future. Clin Infect Dis; 37:1678-1685.
View at Publisher | View at Google Scholar - Modi A, Feld J. (2007), Viral hepatitis and HIV in Africa. AIDS Rev; 9:25-39.
View at Publisher | View at Google Scholar - Shepard CW, Simard EP, Finelli L, Fiore AE, Bell BP. (2008), Hepatitis B virus infection: epidemiology and vaccination. Epidemiol, et al. Entecavir therapy for lamivudine-refractory chronic hepatitis B: improved virologic, biochemical, and serology outcomes through 96 weeks. Hepatology; 48:99-108.
View at Publisher | View at Google Scholar - Bods worth N, Donovan B, Nightingale BN. (1989), The effect of concurrent human immunodeficiency virus infection on chronic hepatitis B: a study of 150 homosexual men. J Infect Dis; 160:577-82.
View at Publisher | View at Google Scholar - Bodsworth NJ, Cooper DA, Donovan B. (1991), The influence of human immunodeficiency virus type 1 infection on the development of the hepatitis B virus carrier state. J Infect Dis; 163:1138-1140.
View at Publisher | View at Google Scholar - Hadler SC, Judson FN, O’Malley PM, et al. (1991), The outcome of hepatitis B virus infection in homosexual men and its relation to prior human immunodeficiency virus infection. J Infect Dis; 163:454-459.
View at Publisher | View at Google Scholar - Soriano V, Puoti M, Bonacini M. (2005), Care of patients with chronic hepatitis B and HIV co-infection: recommendations from an HIV-HBV international panel. AIDS; 19:221-240.
View at Publisher | View at Google Scholar - Schmutz G, Nelson M, Lutz T, et al. (2006), Combination of tenofovir and lamivudine versus tenofovir after lamivudine failure for therapy of hepatitis B in HIV-coinfection. AIDS; 20:1951-1954.
View at Publisher | View at Google Scholar - Piroth L, Pol S, Lacombe K, Miailhes P, et al. (2010), Management and treatment of chronic hepatitis B virus infection in HIV positive and negative patients: the EPIB 2008 study. J Hepatol; 53:1006-12.
View at Publisher | View at Google Scholar - Kosi L, Reiberger T, Payer BA, et al. (2012), Five-year on-treatment efficacy of lamivudine-, tenofovir- and tenofovir + emtricitabine-based HAART in HBV-HIV-coinfected patients. J Viral Hepat,19(11):801-810.
View at Publisher | View at Google Scholar - Puoti M, Torti C, Bruno R. (2006), Natural history of chronic hepatitis B in co-infected patients. J Hepatol; 44:65-70.
View at Publisher | View at Google Scholar - Puoti M, Bruno R, Soriano V, et al. (2004), Hepatocellular carcinoma in HIV-infected patients: epidemiological features, clinical presentation, and outcome. AIDS; 18:2285-2293.
View at Publisher | View at Google Scholar - Brau N, Fox R, Xiao P, et al. (2007), Presentation and outcome of hepatocellular carcinoma in HIV-infected patients: A US-Canadian multicenter study. J Hepatol; 47:527-537.
View at Publisher | View at Google Scholar - Nikolopoulos GK, Paraskevis D, Hatzitheodorou E, et al. (2009), Impact of Hepatitis B virus infection on the progression of AIDS and Mortality in HIV-infected individuals: a cohort study and meta-analysis. Clin Infect Dis; 48:1763-1771.
View at Publisher | View at Google Scholar - Thio C, Seaberg E, Skolsky R. (2002), HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter AIDS Cohort Study (MACS). Lancet; 360:1921-1926.
View at Publisher | View at Google Scholar - Crowell TA, Gebo KA, Balagopal A, et al. (2014), Impact of hepatitis coinfection on hospitalization rates and causes in a multicenter cohort of persons living with HIV. J Acquir Immune Defic Syndr. 65(4):429-37.
View at Publisher | View at Google Scholar - Rosenthal E, Roussillon C, Salmon-Céron D, et al. (2014), Liver-related deaths in HIV-infected patients between 1995 and 2010 in France: The Mortavic 2010 study in collaboration with the Agence Nationale de Recherche sur le SIDA (ANRS) EN 20 Mortalité 2010 survey. HIV Med.
View at Publisher | View at Google Scholar - Matthews GV, Manzini P, Hu Z, et al. (2011), Impact of lamivudine on HIV and hepatitis B virus-related outcomes in HIV/hepatitis B virus individuals in a randomized clinical trial of antiretroviral therapy in southern Africa. AIDS; 25:1727-1733.
View at Publisher | View at Google Scholar - Núñez M, Puoti M, Camino N, Soriano V. (2003), Treatment of chronic hepatitis B in the human immunodeficiency virus-infected patient: present and future. Clin Infect Dis; 37:1678-1685.
View at Publisher | View at Google Scholar - Ingiliz P, Valantin MA, Thibault V, et al. (2008), Efficacy and safety of adefovir dipivoxil plus pegylated interferon-alpha2a for the treatment of lamivudine-resistant hepatitis B virus infection in HIV-infected patients. Antivir Ther; 13:895-900.
View at Publisher | View at Google Scholar - Boyd A, Piroth L, Maylin S, et al. (2016), Intensification with pegylated interferon during treatment with tenofovir in HIV-hepatitis B virus co-infected patients. J Viral Hepat. 23(12):1017-1026.
View at Publisher | View at Google Scholar - Van Bömmel F, Wunsche T, Mauss S, et al. (2004), Comparison of adefovir and tenofovir in the treatment of lamivudine-resistant hepatitis B virus infection. Hepatology. 40:1421-1425.
View at Publisher | View at Google Scholar - Matthews GV, Seaberg E, Dore GJ, et al. (2009), Combination HBV therapy is linked to greater HBV DNA suppression in a cohort of lamivudine-experienced HIV/HBV-coinfected individuals. AIDS. 23:1707-15.
View at Publisher | View at Google Scholar - Thibault V, Stitou H, Desire N, Valantin MA, Tubiana R, et al. (2011), Six-year follow-up of hepatitis B surface antigen concentrations in tenofovir disoproxil fumarate treated HIV-HBV-co-infected patients. Antivir Ther. 16:199-205.
View at Publisher | View at Google Scholar - Plaza Z, Aguilera A, Mena A, et al. (2013), Influence of HIV infection on response to tenofovir in patients with chronic hepatitis B. AIDS. 27(14):2219-2224.
View at Publisher | View at Google Scholar - Snow-Lampart A, Chappell B, Curtis M, et al. (2011), No resistance to tenofovir disoproxil fumarate was detected after up to 144 weeks of therapy in patients mono infected with chronic hepatitis B virus. Hepatology. 53:763-773.
View at Publisher | View at Google Scholar - Lampertico P, Viganò M, Manenti E, Iavarone M, Sablon E, et al. (2007), Low resistance to adefovir combined with Lamivudine: a 3-year study of 145 Lamivudine-resistant hepatitis B patients. Gastroenterology. 133:1445-1451.
View at Publisher | View at Google Scholar - Berg T, Marcellin P, Zoulim F, et al. (2010), Tenofovir is effective alone or with emtricitabine in adefovir-treated patients with chronic hepatitis B virus infection. Gastroenterology, 139:1207-1217.
View at Publisher | View at Google Scholar - Ratcliffe L, Beadsworth MB, Pennell A, Phillips M, Vilar FJ. (2011), Managing hepatitis B/HIV co-infected: adding entecavir to Truvada (tenofovir disoproxil/emtricitabine) experienced patients. AIDS. 25:1051-1056.
View at Publisher | View at Google Scholar - Hosaka T, Suzuki F, Kobayashi M, et al. (2012), Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology.
View at Publisher | View at Google Scholar - Coffin CS, Stock PG, Dove LM, et al. (2010), Virologic and clinical outcomes of hepatitis B virus infection in HIV-HBV co-infected transplant recipients. Am J Transplant. 10:1268-1275.
View at Publisher | View at Google Scholar - Tateo M, Roque-Afonso AM, Antonini TM, et al. (2009), Long-term follow-up of liver transplanted HIV/hepatitis B virus co-infected patients: perfect control of hepatitis B virus replication and absence of mitochondrial toxicity. AIDS. 23:1069-1076.
View at Publisher | View at Google Scholar - Marcellin P, Heath Cote EJ, Buti M, et al. (2011), Tenofovir disoproxil fumarate versus adefovir dipivoxil for chronic hepatitis B. N Engl J, et al. Clinical and virological outcomes in HIV-infected patients with chronic hepatitis B on long-term nucleotide analogs. AIDS. 25:73-79.
View at Publisher | View at Google Scholar - Fung SK, Andreone P, Han SH, et al. (2005), Adefovir-resistant hepatitis B can be associated with viral rebound and hepatic decompensation. J Hepatol. 43:937:943.
View at Publisher | View at Google Scholar - Berg T, Marcellin P, Zoulim F, et al. (2010), Tenofovir is effective alone or with emtricitabine in adefovir-treated patients with chronic hepatitis B virus infection. Gastroenterology. 139:1207-1217.
View at Publisher | View at Google Scholar - Patterson SJ, George J, Strasser SI, et al. (2011), Tenofovir disoproxil fumarate rescue therapy following the failure of both lamivudine and adefovir digitoxin in chronic hepatitis B. Gut. 60:247-254.
View at Publisher | View at Google Scholar - Petersen J, Ratziu V, Buti M, et al. (2012). Entecavir plus tenofovir combination as rescue therapy in pre-treated chronic hepatitis B patients: An international multicenter cohort study. J Hepatol. 56(3):520-526.
View at Publisher | View at Google Scholar - Schmutz G, Nelson M, Lutz T, et al. (2006), Combination of tenofovir and lamivudine versus tenofovir after lamivudine failure for therapy of hepatitis B in HIV-coinfection. AIDS, 20:1951-1954.
View at Publisher | View at Google Scholar - Matthews GV, Avihingsanon A, Lewin SR, et al. (2008), A randomized trial of combination hepatitis B therapy in HIV/HBV co-infected antiretroviral naïve individuals in Thailand. Hepatology, 48:1062-1069.
View at Publisher | View at Google Scholar - Matthews GV, Seaberg E, Dore GJ, et al. (2009), Combination HBV therapy is linked to greater HBV DNA suppression in a cohort of lamivudine-experienced HIV/HBV-coinfected individuals. AIDS. 23:1707-1715.
View at Publisher | View at Google Scholar - Price H, Dunn D, Pillay D, et al. (2013), Suppression of HBV by tenofovir in HBV/HIV co-infected patients: a systematic review and meta-analysis. PLoS One. 8(7): e68152.
View at Publisher | View at Google Scholar - Lok AS, Trinh H, Carosi G, et al. (2012), Efficacy of entecavir with or without tenofovir disoproxil fumarate for nucleos(t)ide-naïve patients with chronic hepatitis B. Gastroenterology.143(3):619-628.
View at Publisher | View at Google Scholar - Agarwal K, Fung SK, Nguyen TT, et al. (2015), Twenty-eight-day safety, antiviral activity, and pharmacokinetics of tenofovir alafenamide for treatment of chronic hepatitis B infection. J Hepatol. 62(3):533-540.
View at Publisher | View at Google Scholar - Sax PE, Wohl D, Yin MT, et al. (2015), Tenofovir alafenamide versus tenofovir disoproxil fumarate, co-formulated with elvitegravir, cobicistat, and emtricitabine, for initial treatment of HIV-1 infection: two randomized, double-blind, phase 3, non-inferiority trials. Lancet. 385(9987):2606-2615.
View at Publisher | View at Google Scholar - Gallant J, Brunetta J, Crofoot G, et al. (2016), Efficacy and Safety of Switching to a Single-Tablet Regimen of Elvitegravir/Cobicistat/Emtricitabine/Tenofovir alafenamide in HIV-1/Hepatitis B-Coinfected Adults. J Acquir Immune Defic Syndr. 73(3):294-298.
View at Publisher | View at Google Scholar - Heathcote EJ, Marcellin P, Buti M, et al. (2011), Three-year efficacy and safety of tenofovir disoproxil fumarate treatment for chronic hepatitis B. Gastroenterology, 140:132-143.
View at Publisher | View at Google Scholar - Mauss S, Berger F, Flimann N, et al. (2011), Effect of HBV polymerase inhibitors on renal function in patients with chronic hepatitis B. J Hepatol. 55:1235-1244.
View at Publisher | View at Google Scholar - 50Mauss S, Berger F, Schmutz G. (2005), Antiretroviral therapy with tenofovir is associated with mild renal dysfunction. AIDS, 19:93-95.
View at Publisher | View at Google Scholar - Fux CA, Simcock M, Wolbers M, et al. (2007), Swiss HIV Cohort Study. Tenofovir use is associated with a reduction in calculated glomerular filtration rates in the Swiss HIV Cohort Study. Antivir Ther, 12:1165-1173.
View at Publisher | View at Google Scholar - Goicoechea M, Liu S, Best B, et al. (2008), California Collaborative Treatment Group 578 Team. Greater tenofovir-associated renal function decline with protease inhibitor-based versus non-nucleoside reverse-transcriptase inhibitor-based therapy. J Infect Dis. 197:102-108.
View at Publisher | View at Google Scholar - Mocroft A, Kirk O, Reiss P, et al. (2010), Estimated glomerular filtration rate, chronic kidney disease, and antiretroviral drug use in HIV-positive patients. AIDS. 24(11):1667-1678.
View at Publisher | View at Google Scholar
