

Research Article | DOI: https://doi.org/10.31579/2835-9216/027
Mammography Diagnostic Reference Level for Breast Cancer Screening Procedures: A Systematic Review
1Department of Physics with electronics, Federal University Birnin Kebbi.
2 Department of Radiology, Federal Medical Centre Birnin Kebbi.
*Corresponding Author: Samaila B, Department of Physics with electronics, Federal University Birnin Kebb
Citation: Samaila B and Rilwanu M. D, (2024), Mammography Diagnostic Reference Level for Breast Cancer Screening Procedures: A Systematic Review, Carcinogenesis and Chemotherapy, 3(3) DOI:10.31579/2835-9216/027
Copyright: © 2024, Samaila B. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 03 June 2024 | Accepted: 13 June 2024 | Published: 24 June 2024
Keywords: mammography; breast cancer; diagnostic reference levels; and glandular dose
Abstract
Background: Breast cancer claims about 500,000 lives worldwide each year, although research shows that mortality rates can be cut by up to 30% with early detection. The most crucial diagnostic tool for the early diagnosis of breast cancer is mammography, which is radiographic imaging of the breast using X-rays. Low intensity X-rays are used during mammography to image the breast tissue. Despite the use of low dose radiation, the use of ionizing radiation raises the possibility of causing breast cancer.
Aim and Objectives: The main goal of this study was to examine previous and current studies that evaluated mean glandular dose (MGD) and diagnostic reference values during diagnostic mammography procedures around the world.
Materials and Method: In order to find studies that assessed glandular doses and established DRLs for mammography (within the years 2003–2022), a systematic search through the literature were conducted using search terms extracted from three terms: Diagnostic Reference Levels (DRLs), Average/mean glandular dose (A/MGD), mammography, and breast screening. Following a screening process, 22 articles out of 700 found throughout the search were included. Relevant information from the included studies was compiled and examined.
Result and Discussion: The researchers built seven literatures that established DRL in mammography at the 75th and 95th percentiles. Ten studies produced DRLs at these two percentiles, whereas three studies failed to do so. The compressed breast thickness, exposure factors, average glandular dose, and DRLs all showed differences. Both the techniques and the data are varied. For ten studies, the mean AGD for the CC and MLO projections ranges from 0.31 to 2.46 mGy and 0.46 to 1.82 mGy, respectively. The DRL values range from 0.63 to 3.48 mGy at the 75th percentile and from 2.22 to 3.74 at the 95th percentile for CC projections, respectively.MLO projections were determined to have a 75th and 95th percentile between 1.46 and 2.17 and 2.68 and 3.61 mGy. In terms of both CC/MLO, the range was 2.0 - 13.0 mGy at the 95th percentile and 1.4-6.7 mGy at the 75th percentile. DRL comparisons between nations are made more difficult by these discrepancies; as a result, having a protocol that is widely accepted would be helpful. For the radiation safety of patients, it is crucial to establish DRLs for breast mammography procedures.
Conclusion: The mammographic DRL values vary from one country to another. For radiation protection during mammography screening, the creation of DRL is essential. The global mammographic DRLs should be established and maintained.
Introduction
With 7% mortality from two million women diagnosed each year, breast cancer is the second most frequent malignancy and the fifth greatest cause of death worldwide. Breast cancer early diagnosis and death reduction depend heavily on breast screening. In various countries, the mortality rate from breast cancer has decreased by 30–40% thanks to the widespread adoption of mammography as an efficient screening method for breast cancer screening and detection. Mammography tests are done for either screening (for patients who don't have any symptoms) or diagnostic (for patients who do have symptoms) reasons [7]. For each breast, a mammography examination uses the usual craniocaudal (CC) and mediolateral oblique (MLO) projections. The radiosensitivity of the glandular tissues in the breast makes mammography more likely to cause radiation-induced carcinogenesis. Mammography-related hazards for breast cancer, however, are only hypothesized, not confirmed. Menopausal women have a zero to minimal risk of radiation induced carcinogenesis compared to the higher risk observed in women under the age of 20 years after exposure to ionizing radiation, for example, and there is very little evidence of radiation induced breast cancer for exposures beyond menopause, even following radiotherapy, leading to uncertainty with radiation induced carcinogenesis. A patient's risk of radiation-induced carcinogenesis must be determined using the average glandular dose (AGD). The mean glandular dose (MGD) of the breast tissue is thought to be the most significant quantity to evaluate the risk of radiation-induced carcinogenesis from mammography since glandular tissue in the female breast is considered to be the most radiosensitive organ. Because it is impossible to properly evaluate the amount absorbed by the glandular tissue, MGD must always be considered an estimate. Additionally, a woman's age and breast thickness affect changes in the density distribution of the glandular tissue. The patient receives less radiation since the breast is squeezed to make it thinner.It is advised that the dose supplied to the breast be as low as reasonably attainable (ALARA) without sacrificing image quality. To reduce patients' exposure to radiation, it is important to follow the concepts of radiation protection rationale, optimization, and dosage limiting [7,25,27]. Several nations have established Diagnostic Reference Levels (DRLs) to help with optimization and control radiation dose variations during mammography exams. DRLs are dose measures used to spot radiation doses given to patients that are unusually high [26]. While some researches advise using the 95th percentile, the majority of studies advise using the 75th percentile of the AGD for establishing the DRLs for mammography. Local DRLs should be established within institutions and, if applicable, must be consistent with any existing national DRLs, according to the Australian Radiation Protection and Nuclear Safety Agency (ARPANSA). The European Commission recently issued a report that suggested that local and national DRLs should be updated every three and five years, respectively, at the very least. According to recent data, DRLs vary between and within countries. The National Health Service Breast Screening Programme (NHSBSP) of the United Kingdom (UK) suggests a national DRL of 2.5 mGy for screening mammography exams. In New South Wales and Queensland of Australia, the DRLs for digital mammography are 2.0 mGy and 1.1 mGy, respectively. In the United States of America (USA), Ireland, Greece, and North Eastern Nigeria, digital mammography radiation levels (DRLs) of 1.9, 1.5, 1.4, and 0.8 mGy have been proposed, respectively [7]. Diagnostic Reference Levels (DRLs) are widely used in mammography as a means of optimizing radiation dose to patients while maintaining image quality. The following is a summary of recent literature findings on mammography DRLs. A study published in the European Journal of Radiology (2017) found that the use of DRLs in mammography significantly reduces patient radiation dose while maintaining image quality. The study concluded that "DRLs can be a useful tool for improving the radiation safety of mammography." [4]. Another study published in the Journal of Medical Physics (2019) compared DRLs for mammography in several countries and found significant differences in the recommended levels. The study highlights the need for harmonization of DRLs internationally to ensure consistent and safe radiation practices in mammography. [8]. In a review article published in the Journal of Radiology Nursing (2021), the authors discussed the importance of DRLs in ensuring the safe and effective use of ionizing radiation in mammography. They emphasized the need for continuous monitoring and updating of DRLs to keep up with advancements in technology and changing patient populations. [31]. A study by K. Yamada et al. (2017) found that mammography DRLs vary widely across different countries. The study evaluated the DRLs in Japan, the United States, and Europe and found that the DRLs in Japan were generally lower than those in the United States and Europe. The authors suggest that this variability is due to differences in the imaging equipment used, as well as differences in the way the DRLs are established and monitored. Another study by L. W. Low et al. (2018) evaluated the relationship between mammography DRLs and patient radiation dose. The study found that mammography DRLs were significantly associated with patient radiation dose, with higher DRLs being associated with higher patient doses. The authors suggest that this relationship highlights the importance of ensuring that mammography DRLs are set and monitored appropriately to minimize patient radiation exposure. [16] evaluated the effectiveness of mammography DRLs in reducing radiation exposure in mammography. The review found that mammography DRLs have been effective in reducing radiation exposure in mammography, but that further research is needed to better understand the factors that influence the radiation dose received during mammography. The authors suggest that continued monitoring and evaluation of mammography DRLs is essential to ensure that women receive safe and effective diagnostic scans. One study found that the implementation of DRLs in mammography significantly reduced the average radiation dose per examination by over 50% [33]. This reduction in dose is important because it reduces the potential risk of harm to patients, especially since mammography is a routine examination for many women. The study also found that the implementation of DRLs improved the consistency of radiation dose across different mammography units, which is crucial for ensuring that patients receive consistent quality care. Another study assessed the impact of DRLs on image quality in mammography [34]. The study found that the use of DRLs did not negatively impact image quality and that the images produced were of high diagnostic quality. This is important because it shows that the use of DRLs does not compromise the ability to diagnose breast conditions. The study also found that the use of DRLs improved the consistency of image quality across different mammography units, which is essential for ensuring that patients receive consistent quality care. According to a study by van den Bogaard et al. (2015), DRLs have been established in many countries to provide guidance for mammography practitioners in maintaining consistent and appropriate levels of radiation exposure for their patients. The authors also reported that DRLs have been shown to be effective in reducing radiation exposure in mammography, with some studies demonstrating a significant reduction in average glandular dose (AGD) following the introduction of DRLs. In a systematic review by van den Bogaard et al. (2017), the authors concluded that DRLs are an important tool for ensuring that mammography radiation doses are kept as low as possible while still providing adequate image quality. They also reported that the use of DRLs is associated with a reduction in AGD, which can help to reduce the risk of radiation-induced cancers. Additionally, a study by Segars et al. (2014) found that mammography equipment can have a significant impact on the radiation exposure received by patients. The authors reported that mammography equipment with higher exposure settings, or lower sensitivity, can result in higher radiation doses for patients, even when DRLs are used. This highlights the importance of using high-quality mammography equipment, and the need for regular quality control testing to ensure that equipment performance is consistent with DRLs.
Materials and Methods
Search strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses were used to conduct the study (PRISMA). To locate studies that have established DRLs for digital mammography, the following databases were searched for relevant literature: Research Gate, Web of Science, Science Direct, Google Scholar, and Pub-Med. The search terms "Mammography or Digital mammography" and "DRLs or Diagnostic Reference Levels or Average Glandular Dose" were used. To limit the results to publications in the designated language and those that met the following inclusion criteria, a search filter was used [13]. The English language was chosen as the publication language, and the other selection criteria were as follows [28].
Selection criteria
Only studies using DM or a combination of DM and screen-film mammography, and involving assessment of Glandular Dose and the establishment of DRLs using patient data, were included in this systematic review update. This is due to the gradual phase-out of screen-film mammography and the updated recommendation on the use of patient data in the establishment of DRLs in ICRP 135 [13].
Inclusion criteria
For the purpose of full text review, the title and abstract of all published works with open full-text access through Research Gate, Web of Science, Science Direct, Google Scholar, and Pub-Med were originally scrutinized. Only abstracts that examined A/MGDs in mammography were included in the full-text review. This study includes articles that looked at DRLs (institutional, regional, national, or global) for digital mammography or for both digital and traditional (fill-screen or computerized) mammography. The articles that contained information from patients or phantoms were separately chosen for the review [13]
Exclusion criteria
Articles that had no free full-text access and were not published in the English language were excluded. Literatures that did not take into account digital mammography or fill-screen mammography were eliminated. The literature that has examined DRLs for a variety of radiographic techniques, including computed tomography, fluoroscopy, and interventional procedures, was excluded from this analysis
.
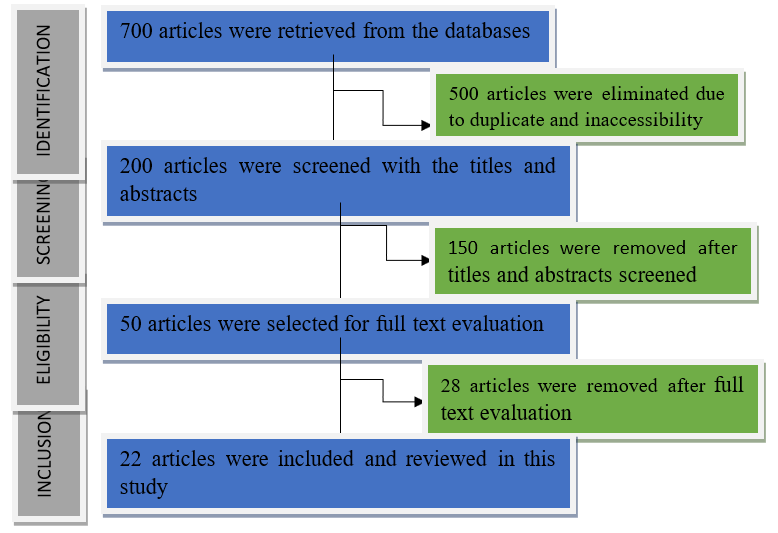
Figure 1: Flow of literature selection through data bases.
Data Extraction
The pertinent information regarding the methodology and selection process for the studies was compiled and examined. These comprise the year of the study, the nation, the population type, the sample size, the inclusion and exclusion criteria for the study, the method used to gather the data, the conversion factors, the mean compressed breast thickness (CBT), the mean and/or median MGD, and the DRLs (75th or 95th percentile).
Mean Glandular Dose and Diagnostic Reference Levels Determination
When attempting to establish international comparisons, the procedures used to establish the DRLs become crucial because radiation dose measurements are needed. Mammography used to be screen-film based, but this technology is currently being phased out and replaced with digital mammography, which includes full-field digital mammography and computerized radiography systems. As a result, only studies using digital mammography or a combination of digital mammography and screen-film mammography (SFM) are included [19]. A number of methods have been used to perform or describe the measurement of the radiation dosage to the breast, including air kerma, entrance surface dose, mid-breast dose, total energy delivered to the breast, and average dose absorbed by the glandular tissue. As a result of the mammary glands' high sensitivity to ionizing radiation and high risk of developing radiation-induced carcinogenesis, the latter method was discovered to be the most effective for determining absorbed dosage to the breast. The ICRP, the United States National Council on Radiation Protection and Measurements, and the British Institute of Physics and Engineering in Medicine all propose using a metric known as mean glandular dose [19].
thickness range [19,24].
Result and Discussion
The combined search approach turned up a total of 700 articles: 500 from Google Scholar, 100 from Research Gate, 50 from Pub-Med, 15 from Web of Science, and 35 from Science Direct. 500 articles were removed from further consideration after the initial screening based on language, duplications, and full-text access. After the aforementioned procedures were completed, 200 papers were screened with a title and abstract; 150 articles were deleted, and 50 articles were determined to be qualified for a full-text According to certain publications, the Mean Glandular Dose (MGD) or Average Glandular Dose (AGD) for each image acquired was automatically computed in the mammography machine and recorded in the system using the Dance formula as follows:
MGD = K × g× s × c
where: K is the ESAK, g is the g factor, which absorbs radiation energy in the breast’s glandular tissue, S is a correction factor X-ray spectrum variation due to anode filter combinations, c is a factor used to adjust variation in breast composition (Mohd et al., 2022). To determine the DRLs values, the 75th and95th percentiles were calculated across the median or mean image MGD for each breast analysis. After the full-text review, 28 studies were eliminated because they lacked clinical information, did not evaluate AGD, did not produce DRLs for mammography, and did not analyze AGD. 22 papers in all were included in the systematic review, as can be seen in figure (1).
Table 1: An overview results of the literatures
| Location | Projections | Exposure parameters | AGD (mGy) | Diagnostic Reference Levels | Reference | |||
| CBT(mm/cm) | kV | mAs | 75th | 95th | ||||
| Ghan | CC/MLO | 60 | 27.8 | 148.5 | 1.8 | 6.7 | 13.0 | Dzidzornu et al., 2020 |
| Japan | - | - | - | - | 1.48 | 1.84 | 2.22 | Yasuki et al., 2020 |
| Nigeria, NW | CC MLO | 4.8 5.3 | 26–31 26–31 | 71.04 5.39 | 1.55 1.57 | 1.50 1.60 | 3.74 3.61 | Garba et al., 2021 |
| Norway | CC/MLO | 55–65 | 29-32 | 0.7 - 2.1 | 1.4 | 2.0 | Hauge et al., 2013 | |
| Malaysia | CC
MLO | 33.1-64.8 31.91- 70.25 | 26.8-33.6 26.62-34.66 | -
- | 1.53/1.79 1.92/2.17 | 1.68 2.06 | 2.92 2.68 | Mohd et al., 2022 |
Iran Khorasan | CC
MLO | 47
53 | 22.9-26.9 23.6-27.7 | 29.6-86.4 31.7-92.7 | 0.88 1.11 | 1.33 | - | Bahreyni et al., 2013 |
Saudi Arabia Riyadh, | - | 55.1 | 29.10 | 115.7 | 1.30 | 1.50 | - | Nissren et al., 2021 |
| Belgium | - | - | 26.0-28.2 | - | 0.83-2.64 | - | 2.46 | Smans et al., 2005 |
| Australia | - | 2-6 | - | - | 1.3- 1.5 | 2.0 | - | Cameron et al., 2020 |
| Australia | - | 60 | - | - | 1.39 | 2.06 | 2.69 | Suleiman, 2018 |
Queensland | - | - | - | - | 0.16 | 1.30 | - | David et al., 2011 |
| Saudi Arabia | CC MLO LM | 42.30 52.00 50.0 | 28.5 29.6 29.4 |
78.4 | 1.02 1.10 1.10 |
1.20 | - | Suleiman et al., 2019 |
Lagos Nigeria | CC/LMO | 40.24 | - | - | 0.74 | - | - | Joshua et al., 2020 |
N.E Nigeria | CC MLO | - | 20.5-21.2 21.0-20.2 | 80.2-80.5 80.20 | 0.31 0.69 | 0.63 1.04 | - | Joseph et al., 2018 |
| Morocco | CC MLO | - | 30.53 30.96 | 45.93 53.43 | 1.09 1.26 | 1.34 1.36 | - | Zakaria et al., 2021 |
Sudan | CC MLO | 38 44 | 31 | 36 | 2.46 1.50 | 3.48 2.03 | - | Suliman et al., 2021 |
| Nigerian | CC MLO | 57.34 56.36 | - | - | 0.46 0.46 | 1.46 1.46 | - | Anesthesia et al., 2022 |
Khartoum, Sudan | CC MLO | 5.2 | 28.6 | 108.8 | 1.54 1.58 | - | - | Yousif et al., 2021 |
| Malaysia | CC MLO | 37.5 44.5 | 26.0 26.5 | 117.0 160.0 | 1.54 1.82 | 1.44 | - | JAMAL et al., 2003 |
| Greece | CC MLO | 3.9 | 27.7 | 65.0 | 1.20 1.50 | - | - | Tsapaki et al., 2008 |
NW, Nigeria | CC | 57/69 | 26 -31 | 71.04 | 1.55 | 1.50
| 3.74 | Garba et al., 2021 |
| MLO | 63/76 | 26 -31 | 75.39 | 1.57 | 1.60 | 3.61 | ||
Discussion
The DRLs for mammographic units across various nations were examined using data from table 1. Hussain, et al. (2022) constructed regional DRLs for digital mammography with the aim of optimizing in-house dose. In total, 240 women who were eligible for mammography at the two tertiary institutions in northwest Nigeria participated in the study. The mean glandular dose (MGD) and compressed breast thickness of the patient were recorded, along with other demographic data. At the 75th percentile (CC: 1.50 mGy; 57 mm; MLO: 1.60 mGy; 63 mm) and 95th percentile, local DRLs based on MGD and CBT were constructed (CC: 3.74 mGy; 69 mm; MLO: 3.61 mGy; 76 mm).The MGD based on manual exposure was considerably greater than the automatic optimization parameter (AOP) mode, indicating the necessity of adhering to the use of AOP mode consistently for the purpose of internal dose optimization. Using screening mammography in Greece, Tsapaki et al. (2008) looked into the methods used. In order to build a database of baseline radiation doses, the study calculated mean glandular dose (MGD). 250 women who had standard screening mammography at five mammography centers with one craniocaudal (CC) and one mediolateral oblique (MLO) projection in each breast were included in the study. Age, weight, CBT (compressed breast thickness), tube potential (kV), tube loading (mAs), and MLO projection angle were the variables that were recorded.In terms of the tube potential setting and the MLO angle employed, there were significant discrepancies between the various mammography facilities. The average MGD per exposure was 1.4 0.6 mGy, compared to 1.2 0.5 and 1.5 0.7 mGy, respectively, for the CC and MLO projections. The average MGD values found in this investigation fell below the 2 mGy upper limit set for the reference medium-sized breast with a 4.5 cm CBT. The multiplicity of methods shown, however, highlighted the requirement for a national study on screening mammography in Greece. The mean glandular dose (MGD) during diagnostic mammography in Malaysia was estimated by JAMAL et al. in 2022 as part of a related study. 30 mammography devices from 9 different manufacturers were included in the study.The non-parametric Kruskal-Wallis and median tests were used to determine the significance of the MGD per woman difference between ethnic groups. A multivariate analysis of variance was used to determine the relevance of the variables influencing MGD per women. The mean patient-based MGD per film was 1.54 mGy for the craniocaudal view and 1.82 mGy for the mediolateral oblique view, respectively, whereas the MGD for the phantom was 1.23 mGy (range 0.22- 2.39 mGy). 3.37 mGy was the average MGD for each women Additionally, it was discovered that there is no discernible variation in MGD per woman among the various ethnic groups (p.0.05, Kruskal–Wallis test). The half value layer of the X-ray beam and (CBT) had a substantial impact on MGD per woman on the multivariate test, nevertheless.There were no discernible associations between MGD per woman and age, body mass index, or ethnicity.
A study was carried out in Sudan by Yousif et al. in 2021 at mammography units in two hospitals in Khartoum. There were 300 people in the sample, all with various disease kinds. The Robson's Mean Glandular Dose (MGD) and further mammographic dance tests were assessed in the study. Study parameters included patient age, breast thickness, tube filter, and exposure variables (mAs and kVp). Patient exposure was much lower than the usual IAEA dose, according to calculated MGD values. The average MGD values for craniocaudal and oblique projections were 1.54 and 1.58, respectively. The patient characteristics and radiation exposure factors were documented in this investigation. These results ought to be lower than the recommended dose for international organizations including the IAEA, NCRP, and ACR. Anesthesia et al. (2022) used thermo luminescence dosimeter (TLD) chips to establish DRLs in a study that is comparable to theirs.The median value of the mean glandular dose was used to put the DRLs at the 75th percentile of the distribution. Using the European Commission's guidelines for evaluating the quality of mammographic images, the image quality was evaluated. Both the cranio-caudal and medio-lateral oblique DRL results were 0.53 mGy. Cranio-caudal and medio-lateral oblique projections received criterion scores for image quality evaluation of 76% and 61.2%, respectively. For cranio-caudal projections, criteria 2 and criteria 6 (absence of skin fold) received the highest and lowest scores from the mammograms, respectively, of 100% and 44%. For mediolateral oblique projections, criteria 1 (all breast tissue clearly shown) and criteria 5 (inframammary angle clearly demonstrated) received the highest and lowest scores, respectively, of 96% and 8%. According to the study, DRLs were lower than both the established levels in other regions of Nigeria and the values recognized internationally. It was possible to see the images well. DRLs for digital mammography and picture quality assessment are crucial optimization tools that any radiology department with a mammography machine should employ. Suliman et al. (2021) assessed 496 breasts (247 women) at eight clinics in Sudan to calculate the average glandular dose (AGD) using craniocaudal (CC) and mediolateral oblique (MLO) views. It was determined the incident air kerma from the X-ray tube output values and the typical patient-specific breast exposure parameters. The AGD ranged from 0.34 to 4.03 mGy (average: 2.46), 0.29 to 3.39 mGy (average: 1.51), and 0.6-7.4 mGy per CC and MLO projection and per woman (average: 3.95).The recommended national diagnostic reference levels (mGy) for CC, MLO, and per woman are 3.48, 2.03, and 6.44 mGy, respectively. In order to safeguard patients from radiation exposure, it is crucial to establish the recommended diagnostic reference levels. Dose optimization for X-ray mammography will be supported at the national level and beyond. The findings offer crucial starting points for creating the national diagnostic reference levels. In the study by Zakaria et al. (2021), the mean glandular dose (MGD) for craniocaudal (CC) and mediolateral oblique (MLO) respectively was 1.090,45mGy and 1.260.74mGy. For CC view and MLO view, the established DRLs were 1.34 and 1.36, respectively. Lifetime Attributable Risk of Cancer Incidence has been determined to be 0.76 for CC examination, 0.88 for MLO, and 1,64 for the complete mammography routine, out of the 100,000 women exposed. In this study, established local DRLs are lower than in the UK and France and higher than in Nigeria and Australia. There is a need to improve screening mammography procedures because there may be a danger of radiation-induced carcinogenesis. In a similar vein, Joseph et al. (2018) determined the MGD to be 0.69 0.11 mGy and 0.69 0.11 mGy for CC and mediolateral oblique (MLO), respectively. DRL for CC and MLO were 0.63 mGy and 1.04 mGy, respectively.The MGD and anthropotechnical characteristics showed no statistically significant connection (P > 0.05). Comparing this work to internationally recognized works, the DRL in this work were greater. The majority of centers in Nigeria and North Eastern Nigeria need to optimize their radiology practices.
In order to calculate the risk of radiation-induced cancer, Suleiman et al. (2019) quantified the radiation doses that patients get during mammographic X-ray imaging procedures. At the King Khaled Hospital and Prince Sultan Center in Alkharj, Saudi Arabia, 60 patients were assessed using a calibrated digital mammography unit. Patient ages ranged from 44.4 to 10 years on average (26–69). For X-ray tube potential (kVp) and current multiplied by the exposure duration (s) (mAs), the average and range of exposure parameters were 29.1 1.9 (24.0-33.0) and 78.4 17.5 (28.0-173.0), respectively (as shown in table 1). The MGD (mGy) for each single procedure for the craniocaudal (CC), medial lateral oblique (MLO), and lateromedial (LM) projections was 1.02 0.2 (0.4-1.8), 1.1 0.3 (0.5-1.8), and 1.1 0.3 (0.5-1.9), respectively.An estimated 177 procedures out of every million involve a cancer risk. When taking multiple images, there is a considerable chance of cancer. Eighty percent of the procedures had typical results, the study found. For young patients, in particular, specific justification is necessary. In Australia, digital radiography and computed tomography mammography systems, David et al. (2011) proposed DRLs. For mammography in Breast Screen and computed radiography mammography, the results were found to be 1.1 and 1.4 mGy. Determined DRLs for a variety of phantom thicknesses in both full field digital mammography units and digital breast tomosynthesis units in Cameron et al(2020) .'s study on mammography.For full field digital mammography and digital breast tomosynthesis, the American College of Radiology (ACR) Phantom levels have been determined at 1.3 mGy and 1.5 mGy mean glandular dosage, respectively. PMMA had values of 0.9 and 1.0 mGy at 2 cm, 2.0 and 2.3 mGy at 6 cm. This information can be used to set national reference levels in Western Australian regions in the future. DRLs were calculated for screening mammography in Belgium by Smans et al. in 2005. The mean average glandular dose's 95th percentile was 2.46 mGy. Based on tests made with polymethyl methacrylate (PMMA), the DRL was 2.08 mGy.For systems that use solely Mo/Mo anode/filter, the correlation coefficient (R) between doses from patient studies and phantom studies was 0.90, with an average underestimate of the phantom readings of 15%. There is insufficient scientific proof for centers using various anode/filters to conclude that a single phantom measurement of a typical PMMA block represents the patient dose. A local diagnostic reference level (DRL) for 1055 patients undergoing digital mammography operations at Riyadh Care Hospital in Riyadh, Saudi Arabia, was proposed by Nissren et al. in 2021. All surgeries were completed for clinical problems that were approved by medicine. In comparison to the mean AGD (mGy) values, which were 1.3 (1.0-7.2) per procedure, the mean and range of the ESAK (mGy) results were 5.19 3.18 (0.33-29.9). ESAK (mGy) and AGD (mGy) were found to have third quartile values of 6 and 1.5, respectively. Comparable to other investigations are the measured ESAK (mGy) per procedure and the calculated AGD. The number of projections per operation is mostly responsible for the interpatient and interdepartmental difference. In mammography centers in the Iranian region of Khorasan, Bahreyni et al. (2013) studied 100 patients utilizing thermo luminescent dosimeters. To conclude MGD from ESD, conversion factors based on Monte Carlo models were used. The findings showed that the patient dose was greatly variable. For the craniocaudal (CC) view and the mediolateral oblique (MLO) view, respectively, the measured ESDs ranged from 0.74 to 19.81 mGy and 1.20 to 25.79 mGy.In terms of MGDs per image, CC and MLO views had an average of 0.88 and 1.11 mGy, respectively. DRL resulting from mammography tests in Khorasan is 1.33 mGy according to the internationally accepted definition. Due to the significant differences in patient MGD readings, a dose reduction program is advised. In this study, the DRL value is considerably less than the similar levels recommended by other researchers elsewhere. Full-field digital mammography (FFDM) and digital breast tomosynthesis (DBT) were the subjects of research on FFDM and DBT carried out in Malaysia by Mohd et al. in 2022. From the mammography Digital Imaging and Communications in Medicine (DICOM) header, the CBT, kilovoltage peak (kVp), entrance surface dose (ESD), and average glandular dose (AGD) were retrospectively derived.Three sets of CBT range were used to get the 75th and 95th percentile values for the AGD distribution of each mammography projection. At three CBT ranges, the AGD values between FFDM and DBT were compared. At CBT ranges of 20–39 mm, 40–59 mm, and 60–99 mm, respectively, the DRLs for FFDM were 1.13 mGy, 1.52 mGy, and 2.87 mGy, while the DBT were 1.18 mGy, 1.88 mGy, and 2.78 mGy. For both mammographic views, the AGD of DBT was considerably higher than FFDM (p 0.005). AGD values for FFDM and DBT varied significantly between the three CBT groups (p 0.005). The AGD of FFDM was much lower than DBT, and the local DRLs from this study were lower than the national DRLs. Using 26 full-field digital mammography devices from six different manufacturers, Hauge et al. (2013) calculated the 75th and 95th percentiles. The mean glandular dose (MGD), which is defined as the signal-to-noise ratio squared divided by the MGD, and figure of merit (FOM), which is the difference between the two, are used to analyze systematic differences between manufacture categories and model types. The 75th and 95th percentiles of the MGDs per unit are 1.4 and 2.0 mGy, respectively, with a range of 0.7 to 2.1 mGy. In terms of dosage distributions and FOMs, the various manufacturers and models differ. The 95th percentile is suggested as the national DRL for selecting the units that can be used. The 75th percentile for each manufacturer and model is suggested as a way to determine which areas need optimization. DRLs were created by Garba et al. (2021) using MGD and CBT. While DRLs at the 95th percentile were found to be 3.74 mGy for (CC: 69 mm) and 3.61 mGy for (mediolateral (MLO): 63 mm), the DRLs at the 75th percentile were found to be 1.50 mGy for (craniocaudal (CC): 57 mm) and 1.60 mGy for (mediolateral (MLO): 63 mm) (MLO: 76 mm). The MGD calculated using manual exposure was substantially greater than the MGD calculated using the automated optimization parameter (AOP) mode, indicating the necessity to consistently use the AOP mode for internal dose optimization. With respect to values established in the literature, the study's local DRLs for digital mammography systems at the 75th and 95th percentiles were well comparable.Due to the high exposure, manual parameter selection should only be used when there are strong indicators. Additionally, manual parameter selection should be based on pre-established tables in relation to compressed breast thickness. Average glandular dose (AGD), compressed breast thickness (CBT), patient age, entrance surface exposure (ESE), kVp, and mAs were retrospectively retrieved from three digital mammography systems in a research by Dzidzornu et al. (2020). The AGD of each mammography projection's 75th and 95th percentile values were determined at a CBT of 60 5 mm. Investigated was the relationship between the AGD and CBT, kVp, mAs, and ESE.For Centers 1, 2, 3, and all Centers, the 75th percentile for the AGD at CBT of 60 mm was 2.3, 1.8, 2.1, and 2.0 mGy, respectively. Other than research conducted in the United Kingdom, the DRLs obtained were comparable to higher studies conducted abroad, the CBT, kVp, mAs, and ESE all displayed a significant positive connection with the AGD. The AGD used for the craniocaudal (CC) and mediolateral oblique (MLO) projections varied among the three centers. For all three centers and for each center separately, the mean AGD, mAs, and ESE were higher than in prior research, but the mean kVp and CBT were lower.The greater DRLs predicted in this early analysis suggest that Ghana's digital mammography method has to be optimized for dose to increase radiation protection. Practice-related ramifications The research's conclusions will direct optimization efforts and keep mammography radiation dosage variances to a minimum.
Conclusion
Building DRLs as part of quality control methods is becoming more crucial for mammographic units all over the world. The publication of the research that looked at DRL gives up new knowledge for some nations that haven't yet looked into using the techniques of DRL in their radiological operations. The DRL levels for mammography differ from one country to another. The adoption of a national DRL is necessary for mammography screening radiation protection. There should be a national mammographic DRL established and updated.
References
- Anasthesia, A.E., Ibrahim, U., S. D. Yusuf, S.D., Joseph, D.Z., (2022). Diagnostic Reference Levels (DRLs) and Image Quality Evaluation for Digital Mammography in a Nigerian Facility. J. Nig. Soc. Phys. Sci. 4, 281–286
View at Publisher | View at Google Scholar - BahreyniToossi, M.T., Zare, H., BayaniRoodi, Sh., Hashemi, M., Akbari, F., and Malekzadeh, M. (2013). Towards proposition of a diagnostic reference level for Mammographic examination in the greater Khorasan province, Iran. Radiation Protection Dosimetry, Vol. 155, No. 1, pp. 96–99.
View at Publisher | View at Google Scholar - Bourguignon, M., Thomsen, M. B., Laursen, L. C., &Horsman, A. (2017). The use of diagnostic reference levels in mammography: a survey of the European Society of Radiology. European Journal of Radiology, 86, 103-110.
View at Publisher | View at Google Scholar - Cameron S., Alicia, H., and Mario, D. (2020), Mammography diagnostic reference levels in Western Australia. Physical and Engineering Sciences in Medicine.
View at Publisher | View at Google Scholar - David, L. T., Mike, I., David, W., and Michael, B. (2011) Diagnostic reference levels for mammography in Breast Screen Queensland. AustralasPhysEngSci Med, 34:415–418.
View at Publisher | View at Google Scholar - Dzidzornu , E.S.K. Angmorterh, B.B. Ofori-Manteaw, S. Aboagye, K. Dzefi-Tettey, E.K. Ofori (2020). Mammography Diagnostic Reference Levels (DRLs) in Ghana, Radiography.
View at Publisher | View at Google Scholar - Elangovan, S., Emaus, J. J., & van Gils, A. P. (2019). International comparison of diagnostic reference levels for mammography. Journal of Medical Physics, 44(1), 1-8.
View at Publisher | View at Google Scholar - Garba, I., H.S. Bashir, F. Bello, K.S. Nuhu, S. Mohammed, Y. Mansur, Y. Lawal, (2021). Local diagnostic reference levels for digital mammography: Two hospitals study in northwest, Nigeria. Journal of Medical Imaging and Radiation Sciences, Volume 52, Issue 3, Pages 435-442.
View at Publisher | View at Google Scholar - Garba, I., Bashir, H.S., Bello, F., Nuhu, K.S., Mohammed, (2021). Journal of Medical Imaging and Radiation Sciences 52, 435–442
View at Publisher | View at Google Scholar - Hauge, I.H.R., K. Bredholt, K., and H. M. Olerud, H.M. (2013). NEW DIAGNOSTIC REFERENCE LEVEL FOR FULL-FIELD DIGITAL MAMMOGRAPHY UNITS. Radiation Protection Dosimetry, Vol. 157, No. 2, pp. 181–192
View at Publisher | View at Google Scholar - Hussain, B.S., Garba, I., Bello, F., Nuhu, K.S., Mohammed, S.,(2022). LOCAL DIAGNOSTIC REFERENCE LEVELS FOR DIGITAL MAMMOGRAPHY: TWO HOSPITALS STUDY IN NORTHWEST, NIGERIA. Preprint retrieved on 22nd December, 2022.
View at Publisher | View at Google Scholar - Hemamala, UGDS and Weerakoon, B.S. (2022). Diagnostic Reference Levels (DRLs) in Digital Mammography: A Systematic Review. Journal of Radiology and Medical Imaging; 5(2): 1080.
View at Publisher | View at Google Scholar - Joseph, D.Z., Nzotta, C.C., Skam, J.D., Umar, M.S., and Musa, D.Y (2018) Diagnostic reference levels for mammography examinations in North Eastern Nigeria. Afr J Med Health Sci; 17:54-59.
View at Publisher | View at Google Scholar - Joshua, J., Nzotta, C., Joseph Dlama Z., Abonyi L. O., and Abubakar M. G. (2020). Assessment of the Relationship between Mean Glandular Dose and Compressed Breast Thickness in some Selected Hospitals in Lagos State, Nigeria, Dutse Journal of Pure and Applied Sciences (DUJOPAS), Vol. 6 No. 2, 446-451
View at Publisher | View at Google Scholar - JAMAL, N., NG, K-H., and MCLEAN, D. (2003). A study of mean glandular dose during diagnostic mammography in Malaysia and some of the factors affecting it, The British Journal of Radiology, 76, 238–245 E 2003,
View at Publisher | View at Google Scholar - Jumah, A. Y., Alkhamis, A.A., and Al-Yahya, M. (2020) “Diagnostic reference levels in mammography: A systematic review,” Journal of Medical Physics, vol. 45, no. 3, pp. 177–184.
View at Publisher | View at Google Scholar - Low, L.W., Lo, Y.P., Seong, A.M.F., Tan, S. L., (2018). Diagnostic reference levels and patient radiation dose in mammography, Radiology and Oncology, vol. 52, no. 1, pp. 1–7.
View at Publisher | View at Google Scholar - Moayyad E. S., Patrick C. B., and Mark F. M. (2014). DIAGNOSTIC REFERENCE LEVELS IN DIGITAL MAMMOGRAPHY: A SYSTEMATIC REVIEW.Radiation Protection Dosimetry pp. 1–12.
View at Publisher | View at Google Scholar - MohdNorsuddin, N.; Segar, S.; Ravintaran, R.; Mohd Zain, N.; Abdul Karim, M.K. (2022). Local Diagnostic Reference Levels for Full-Field Digital Mammography and Digital Breast Tomosynthesis in a Tertiary Hospital in Malaysia. Healthcare 2022, 10, 1917.
View at Publisher | View at Google Scholar - Nissren T., Salah, H., Mohammad, R., Mohammad, A., Sulieman, A., Alkhoraye, M., and Bradley, D.A. (2021). Evaluation of patients radiation dose during mammography imaging procedure. Radiation Physics and Chemistry: 188, 109680.
View at Publisher | View at Google Scholar - Sulieman, A., Serhan, O., Al-Mohammed, H.I., Mahmud, M.Z., Alkhorayef, M., (2019). Estimation of cancer risks during mammography procedure in Saudi Arabia. Saudi Journal of Biological Sciences 26, 1107–1111
View at Publisher | View at Google Scholar - Suleiman, M.E. (2018). Diagnostic Reference Levels for digital mammography in Austral. PhD thesis in Medical Radiation Sciences Submitted to Faculty of Health Sciences, University of Sydney, Retrieved on 22nd December, 2022.
View at Publisher | View at Google Scholar - Smans, K., Bosmans, H., Xiao, M., Carton, A.K., and Marcha, G. (2005). TOWARDS A PROPOSITION OF A DIAGNOSTIC (DOSE) REFERENCE LEVEL FOR MAMMOGRAPHIC ACQUISITIONS IN BREAST SCREENING MEASUREMENTS IN BELGIUM. Radiation Protection Dosimetry, Vol. 117, No. 1–3, pp. 321–326,
View at Publisher | View at Google Scholar - Samaila, B. (2022c). An Indirect Radiation Dose Assessment of Adult Patients Undergoing Lumbosacral Joints and Lumbar Spine Radiological X-Ray Procedures. International Journal of Scientific Research in Physics and Applied Sciences, Vol.10, Issue.4, pp.29-32
View at Publisher | View at Google Scholar - Samaila B, and Bello A. (2021). Determination of Radiation Doses Received during Knee Joint X-ray Procedures in Kebbi State, Nigeria, SPR, Volume 2, issue 1, Page No.: 506-510.
View at Publisher | View at Google Scholar - Samaila, B. (2022b). Radiation dose assessment to patients undergoing radiological X-ray procedures of upper extremity, SPS, 2(3), 611-614
View at Publisher | View at Google Scholar - Samaila B. (2022a). Radiation Exposure Appraisal to Public, Caregivers and Families in Contact with Thyroid Diseases Patient Undergoing Radioactive Iodine-131 Therapy: A Systematic Review. J Otolaryng Head Neck Surg 2022, 8: 076,
View at Publisher | View at Google Scholar - Suliman, I.I., Mohamed, S., Mahadi, A., Bashier, E., Farah, A., Hassan, N., Ahmed, N., Eisa, M., El-Khayatt, A., and Salem Sass, S. (2021). Analysis of Average Glandular Dose (AGD) and Associated Parameters for Conventional and Digital X-Ray Mammography. Research Square, 1-16,
View at Publisher | View at Google Scholar - Segars, W. P., Parker, J. A., Lu, B., &Karellas, A. (2014). Effect of mammography equipment type and settings on patient radiation dose. Radiology, 270(1), 81-90.
View at Publisher | View at Google Scholar - Saksena, M., &Khandelwal, N. (2021). Diagnostic reference levels in mammography: a review. Journal of Radiology Nursing, 40(1), 16-22.
View at Publisher | View at Google Scholar - Tsapaki, V., Tsalafoutas, I. A., Poga, V., Louizi, A., Kottou, S., and E Koulentianos, E. (2008). Investigation of breast dose in five screening mammography centres in Greece. J. Radiol. Prot. 28, 337–346
View at Publisher | View at Google Scholar - Tõru, I., &Varajärvi, E. (2019). The Implementation of Diagnostic Reference Levels for Radiation Dose in Mammography. Journal of Digital Imaging, 32(2), 201-207.
View at Publisher | View at Google Scholar - Turk, J., & McLaughlin, J. (2019). The Impact of Diagnostic Reference Levels on Image Quality in Mammography. Journal of Digital Imaging, 32(2), 208-214.
View at Publisher | View at Google Scholar - van den Bogaard, J. M., Glatz, J. F., Hendriks, J. H., &Struijk, J. P. (2015). The effect of diagnostic reference levels in mammography on radiation exposure to the breast: A systematic review. Radiology, 277(3), 773-780.
View at Publisher | View at Google Scholar - van den Bogaard, J. M., Struijk, J. P., Glatz, J. F., & Hendriks, J. H. (2017). Diagnostic reference levels in mammography: A systematic review of the literature. Radiography, 23(1), 34-43.
View at Publisher | View at Google Scholar - Yousif M Abdallah, Nouf H Abuhadi, Hanan A Aldousari (2021). Assessment of Mean Glandular Dose and Entrance Surface Dose in Mammographyts, J Res Med Dent Sci, 2021, 9 (2): 8-11.
View at Publisher | View at Google Scholar - Zakaria, T., Mouni,r M., Laila, J., and Fatim,a Z. L. (2021).Evaluation of Radiation Doses and Estimation of the Risk of Radiation-Induced Carcinogenesis in Women Undergoing Screening Mammography Examinations. Biomedical & Pharmacology Journal, Vol. 14(1), p. 249-255
View at Publisher | View at Google Scholar - Yasuki Asada, Yuya Kondo, Masanao Kobayashi, Kenichi Kobayashi, Takuma Ichikawa (2020). Proposed diagnostic reference levels for general radiography and mammography in Japan. J. Radiol. Prot. in press
View at Publisher | View at Google Scholar - Yamada, K., Saito, T., Inoue, S., Oi, H., and Nakamura, M. (2017). Diagnostic reference levels for mammography: Comparison among Japan, the United States, and Europe, Journal of Medical Physics, vol. 42, no. 1, pp. 22–27
View at Publisher | View at Google Scholar
