

Research | DOI: https://doi.org/10.31579/2834-5010/029
Magnitude of Birth Asphyxia and Associated Factors Among Newborns Delivered at Public Hospitals in Hawassa City Administration, Sidama, Ethiopia, 2024*
1Yanet Liyana Health Science College, Hawassa, Ethiopia.
2Sidama Regional Health Bureau, Hawassa, Ethiopia.
3Adare General Hospital, Hawassa City Administration, Hawassa, Ethiopia.
*Corresponding Author: Derese Desalegn Buta, Yanet Liyana Health Science College, Hawassa, Ethiopia.
Citation: © 2025, Derese Desalegn Buta. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright: Derese D. Buta, Elsabet S. Hayesso, Ayalew S. Worassa, (2025), Magnitude of Birth Asphyxia and Associated Factors Among Newborns Delivered at Public Hospitals in Hawassa City Administration, Sidama, Ethiopia, 2024, International Journal of Clinical Therapeutics, 4(4); DOI:10.31579/2834-5010/029
Received: 04 August 2025 | Accepted: 20 August 2025 | Published: 26 August 2025
Keywords: associated factors; birth asphyxia; Ethiopia; hawassa city; magnitude; newborn
Abstract
Background: Globally, 23% of neonatal mortality occurred due to birth asphyxia, of which 31.6% occurred in Ethiopia. The effect of birth asphyxia is not limited only to death but also has a short and long term neuro development effect, including cognitive and motor disabilities which are almost untreatable. Therefore, current study was aimed to assess the magnitude and associated factors of birth asphyxia among newborns delivered at public facility in Hawassa City Administration, Sidama Regional State, Ethiopia, 2024.
Methods: A facility based cross sectional study was conducted from September 1 to November 1, 2024. Data was collected with Kobo Collect version 2023.1.2 and exported to SPSS version 25.0 for statistical analysis. Data quality measures ensured in each steps. Bivariate and Multivariable logistic regression analysis were computed and variables in bivariate analysis with the P-value < 0.25 were selected for multivariable analysis. Finally in multivariate analysis variables with P-value less than 0.05 considered as statistically significant with considering 95% confidence intervals.
Result: The magnitude of birth asphyxia among newborns at public hospitals in Hawassa city obtained as 25.7% (95% CI: 21.3% - 30.2%). Neonates born to mothers with anemia (AOR=2.72; 95% CI: 1.14, 6.51), mothers having preeclampsia (AOR=4.33; 95% CI: 1.49, 12.57), prolonged labor (AOR=5.37; 95% CI: 2.46, 11.71) and meconium-stained fluid (AOR=6.43, 95% CI: 3.46, 11.96) were found to be factors associated with birth asphyxia.
Conclusion and Recommendation: The overall magnitude of birth asphyxia at current study area was high. Maternal anemia, preeclampsia, prolonged labor and meconium-stained amniotic fluid were found as the most important factors influencing the occurrence of birth asphyxia. In order to alleviate the impact of birth asphyxia, it is essential to enhance the quality of antepartum and intra-partum care of mothers through the implementation of various strategies. Both governmental and non-governmental health institutions should work on antepartum and intra-partum care of mothers and improve service delivery.
Introduction
Background: Globally, most of neonatal mortality (75%) happened within one week of neonatal period and about 1 million newborns die within the first 24 hours. Preterm birth, infections and birth asphyxia were reported as the common causes of neonatal deaths (1).
Worldwide 23% of the neonatal deaths each year and about 29% of early neonatal deaths are ascribed to birth asphyxia. Birth asphyxia continued as the foremost cause of neonatal mortality as well as morbidity, particularly in the first week of life in low and middle-income countries (2, 3, 4). The occurrence of birth asphyxia in developed countries has been decreased considerably due to the advances in health care and it contributes only < 0>
Globally, significant number of babies (5-10 %) in each year need encouragement at birth to help them breathe easily like drying and stimulation, airway clearing or positioning), while 3%–6% need basic neonatal resuscitation (bag and mask ventilation) and <1>
In Ethiopia 2015, 31.6% of neonatal mortality was attributed to birth asphyxia (9). Similarly the result of study showed that regional prevalence of birth asphyxia in Ethiopia varies in the range between 3.1%- 32.9% (10, 11).
As indicated in different literatures, birth asphyxia is caused by antenatal, intra-natal, and fetal factors while intra-natal factors took the largest proportional risk factor, followed by antenatal and fetal factors respectively (12).
Factors like maternal chronic diseases like diabetes mellitus, hypertension and pre-eclampsia may affect placental vasculature and lead to reduced blood flow which lead to birth asphyxia. Factors which reduce placental blood flow like abruption of placenta, antepartum hemorrhage and chorioamnionitis are also linked to birth asphyxia (5). Another factors like maternal age, antenatal care, prim gravidity, breach presentation, home deliveries, maternal fever, resuscitation status, preterm baby, fetal distress and low birth weight are also stated as risk factors of birth asphyxia (6-9, 13).
Birth asphyxia is considerable public health important problem, as that understanding the magnitude and its contributing factors, in urban set up remained neglected, including current study areas.
Statement of the problem:
Despite the declining of neonatal mortality rate, the number of neonatal deaths increased by around 1 million deaths per year in Sub-Saharan Africa and around 338,000 under-five death occur due to birth asphyxia (2).
Ethiopia is among the countries with highest neonatal mortality rate, in the world, which is responsible for 29 deaths per 1000 live births and leads 9 times higher than that of developed countries, where the rate is 3 per 1,000 live births (14, 15).
As part of sustainable development goal (SDG) all countries targeting to reduce neonatal mortality rate to at least 12 deaths per 1,000 live births & under-five mortality to at least 25 deaths per 1,000 live births by 2030 (16). This was planned to be achieved through implementing better prevention and treatment strategies of the three leading causes; preterm births, severe infections and birth asphyxia as the key predictors (17).
Despite encouraging improvement seen in maternal as well as childcare in the past decade, birth asphyxia remained as the foremost cause of neonatal morbidities and mortality (18, 19, 20). With an increased percentage of institutional delivery, consideration has to shift toward the quality of service as lack of quality service would increase the magnitude of birth asphyxia (21). Evidences showed that the lack of skilled health workforce and vital medical equipment’s for resuscitation have been challenging properly intervention to reduce birth asphyxia in developing countries, including Ethiopia (22). Actually there were systematic review evidences towards birth asphyxia and its contributing factors, here in Ethiopia as well as global, however the problem persisted, and may need additional supporting evidences, especially in urban areas, where there is possible availability of trained manpower and medical devices. To the best of our knowledge yet, there is a lack of urban focused evidences for magnitude and determinants of birth asphyxia, especially where the current study has been conducted. Thus current study was aimed to assess the magnitude of birth asphyxia and its associated factors.
Conceptual Framework

Figure 1: Conceptual framework for factors affecting birth asphyxia: developed by principal investigators based on reviewed literatures (5, 10, 12, 15, 16).
Significance of the study
Understanding the magnitude of birth asphyxia among new-born and its contributing factors can help to strengthen better treatment outcomes and for further resource planning, prioritization as well as distribution. The findings of the current study will be also the availed evidence to hospitals, regional health bureaus, policy makers, non-governmental organizations and researchers for further intervention and implementation. The findings also may benefit local health facilities to adjust their healthcare deliveries, similarly it also helps to improve the maternal satisfactions.
Objectives
• To determine the magnitude of birth asphyxia among new-borns delivered at public hospitals in Hawassa city administration 2024.
• To examine factors that affect birth asphyxia among new-borns delivered at public hospitals in Hawassa city administration 2024
Methods and materials
Study area: The study was conducted at public hospitals found in Hawassa city, the capital city of Sidama region, with population of 436,992 according to projections of the central statistics of Ethiopia in 2020. The City is divided into eight sub cities and thirty two kebele/the smallest administrative unit. It has five governmental hospitals and thirteen health centers. Two hospitals namely Hawassa University Comprehensive Specialized and Adare General Hospitals were randomly included under current study.
During the study period, there were 980 and 1070 neonatal admissions annually at Adare General Hospital and Hawassa University Comprehensive Specialized hospital.
Study design and period: Facility based cross-sectional study was conducted from September 1, to November 1, 2024.
Source Population
All newborn-mother pair delivered at public hospitals in Hawassa city administration during the study period were considered as source population.
Study Population
All newborns delivered at Adare general hospital and Hawassa University comprehensive specialized hospital in Hawassa city administration during the study period were considered as study population.
Inclusion criteria
All newborns those delivered with gestational age 28 weeks or more were included in this study
Exclusion Criteria
All newborn-mothers pair with major congenital anomalies or syndromes, twin’s births and those with incomplete data/socio-demographic as well as clinical data/ were excluded from the current study.
Sample Size Determination
Sample Size for objective one
Sample size for the first objective was calculated by using single population proportion formula (n = [Z (α/2)2p (1-P)]/d2) by employing the following assumptions: desired precision (d) = 5%, confidence level = 95% (Ζα/2 = 1.96 value), considering the prevalence of 32.8% perinatal asphyxia among neonate admitted in Dilla University referral hospital(9).
Then, n = [Z (α/2)2p (1-P)]/d2
n= 1.962* 0.328 x (1-0.328)/ (0.05)2= 339
Hence, by adding 10% of non-response rate, the sample size for first objective was determined to be 373.
Sample Size for objective two
The sample size for the second objective was also calculated by taking more frequently observed associated factors for birth asphyxia. Such as PROM and parity using Epi info function and became 145 and 117 respectively (11, 14) (Table 1).
No |
Factors |
CI |
Power |
AOR |
Outcome Exposed (%) |
Sample Size |
Non response rate |
Total sample size |
1 |
PROM |
95% |
80 |
3.2 |
19.2 |
132 |
10% |
145 (14) |
2 |
Parity |
95% |
80 |
3.77 |
30.1 |
106 |
10% |
117 (11) |
Table 1: Sample size determination for second objective
Since calculated sample size for second objective was smaller than the sample size calculated for first objective. So, the final desired sample size for this study was taken as 373.
Sampling technique and procedure
Firstly random sampling was employed to select two public hospitals (Hawassa University Comprehensive Specialized Hospital and Adare general hospital) from the total of 5 public hospitals found in Hawassa city administration. Then, the average number of deliveries per month in each of the selected hospitals was calculated based on the number of mothers who gave birth in each of the selected hospitals prior to the survey. Based on this, the average number of deliveries per two months were 714 in Hawassa University Comprehensive Hospital (HUCH) and 406 in Adare general hospital respectively. By using proportional allocation formula 238 and 135 children were allocated and selected by using systematic random sampling method.
The first neonate was selected randomly by lottery methods. Then, another neonate was selected every three (K = 3) intervals until adequate sample size was achieved.
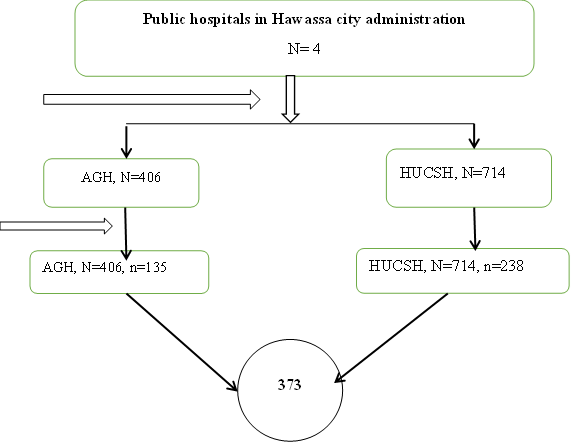
Figure 2: Schematic presentation of sampling procedure N-estimated number of delivery in 2 months, n-sample size allocated proportional to size
Dependent Variable
Birth Asphyxia (present/absent)
Independent Variables
• Socio demographic factors: age, residence, educational status, occupational status
• Antepartum related factors: NC, APH, DM, HTN, Anaemia, Preeclampsia, Parity
• Intra-partum related factors: prolonged labour, foetal presentation, Meconium Stained, C/S, instrumental delivery, obstructed labour
• Foetal related factors: sex of the neonates, foetal distress, gestational age, birth weight, resuscitations
Data Collection Instrument
Structured and pre-tested questionnaires were used to collect data from medical records with Kobo collect application. The questionnaire were developed through intensive search of literature review of related topics and were modified in to current study context to assess magnitude of birth asphyxia and associated factor in hospitals of Hawassa city administration. The questionnaire contains items to assess demographic factors, maternal and obstetric factors, fetal related factors and the outcome variable.
Data Collection Procedures
Four data collectors those with Bachelor of Science (BSc) in neonatal nurses and two master of public health (MPH) holders were involved for supervision and coordination of the whole data collection processes. One day training was given for data collectors and supervisors regarding significance of the study and truthful completion of the checklist and ethical considerations to standardize the data collection. The records of all study participants were selected according to the eligibility criteria and all available information on patient records were checked.
Data Quality Assurance
The questionnaire were prepared in English version and training was given for data collectors and supervisors regarding to the contents of questionnaire and responsibilities of them. Five percent of questionnaire were pre-tested in similar groups of study at Leku General Hospital, where out of study sites, two weeks prior to the actual data collection. Then, adjustments were made based on the findings of the pre-test.
Finally, the actually data collection were conducted by trained personnel’s and monitored with supervisors. Principal investigators were also involved in monitoring data on daily bases for completeness and overall quality of data collection.
Data Processing and Analysis
Data were collected and entered via Kobo collect version 2023.1.2 application and exported to SPSS version 25.0 for statistical analysis. Descriptive summary were used like frequencies, proportions, central tendency and dispersion to present study results.
Bivariate and Multivariable binary logistic regression analysis were computed to assess the association between the dependent and independent variables. All the variables during bivariate analysis with the P-value less than or equal to 0.25 were selected as candidate variables for multivariable analysis. Variance Inflation Factor (VIF) was used to identify the strengths of correlations between independent variables.
Then multivariable analysis were performed to check the association between dependent and independent variables and to adjust for all possible confounders. Variables with P-value less than 0.05 considered as statistically significant. An adjusted odds ratio with 95% confidence intervals (CI) was computed to identify the presence and strength of associations and statistical significance was declared as if p value < 0>
Operational Definitions
• Appearance, Pulse, Grimace, Activity, Respiratory score (APGAR):- Refers the results of an evaluation of a new born physical status, including heart rate, respiratory effort, muscle tone, response to stimulation and colour of skin.
• Birth asphyxia: - could be diagnosed when a new born with any of the sign of impaired breathing (not breathing or not crying, gasping, and < 30>
• Birth weight: - Low birth weight (<2500>2500).
• Preterm birth: -Any infant those borne before 37 weeks of gestational age.
• Fetal distress: - Fetal distress mean heart rate greater than 160 or less than 120/min between uterine contractions, with or without meconium-stained liquor
• Multiparty: - Recorded parity of >2.
• Meconium stained amniotic fluid (MSAF):- if the amniotic fluid was green/brown in color or mixed with meconium, or appears meconium stained on the baby.
• Prolonged labor: - when the labor, after the latent phase of first stage of labor, exceeds 12 hours in prim gravid or 8 hours in multipara mothers.
Results
Variables | Frequency | Percentage |
Age of the mother | ||
< 20> | 9 | 2.4 |
20-24 years | 99 | 26.5 |
25-29 years | 212 | 56.8 |
30-34 years | 47 | 12.6 |
>/= 35 years | 6 | 1.6 |
Educational status of the mother | ||
Primary school and below | 151 | 40.5 |
Secondary school | 141 | 37.8 |
College and above | 81 | 21.7 |
Occupational Status of the Mother | ||
Students | 25 | 6.7 |
House wife | 61 | 16.4 |
Government employee | 160 | 42.9 |
Non-governmental | 14 | 3.8 |
Self-employed | 63 | 16.9 |
Daily laborer | 50 | 13.4 |
Residence of the Mothers | ||
Rural | 27 | 7.2 |
Urban | 346 | 92.8 |
Religion | ||
Orthodox | 102 | 27.3 |
Protestant | 183 | 49.1 |
Catholic | 49 | 13.1 |
Muslim | 39 | 10.5 |
Estimated monthly income | ||
</= 2500 Birr | 110 | 29.5 |
2501-5000 Birr | 152 | 40.8 |
>/=5001 Birr | 111 | 29.8 |
Table 2: Socio-demographic characteristics of mothers delivered at the public hospitals in Hawassa city, Sidama regional state, Ethiopia, 2024
Ante-partum related characteristics of mothers
Among study participants, about 284 (76.1%) were multigravida and 233 (62.5%) were multiparous. Around 147 mothers (39.4%) had attended at least one antenatal care (ANC) visit, whereas only 96(25.7%) mothers had
received four or more ANC follow-ups during their pregnancy. About 44(11.8%) and 21(5.6%) of study participants had been diagnosed with anemia and preeclampsia respectively (Table 3).
Variables | Frequency | Percentage |
Gravidity | ||
Prim gravida | 89 | 23.9 |
Multigravida | 284 | 76.1 |
Parity | ||
Prim parous | 140 | 37.5 |
Multiparous | 233 | 62.5 |
ANC visit frequency | ||
One visit | 147 | 39.4 |
2-3 visits | 130 | 34.9 |
Four and above visits | 96 | 25.7 |
Maternal anemia | ||
Yes | 44 | 11.8 |
No | 329 | 88.2 |
Antepartum hemorrhage | ||
Yes | 18 | 4.8 |
No | 355 | 95.2 |
Preeclampsia | ||
Yes | 21 | 5.6 |
No | 352 | 94.4 |
Chronic Hypertension | ||
Yes | 9 | 2.4 |
No | 364 | 97. |
Chronic diabetes mellitus | ||
Yes | 373 | 100 |
No | 0 | 0 |
Gestational Diabetes Mellitus | ||
Yes | 373 | 100 |
No | 0 | 0 |
Table 3: Ante-partum related characteristics of mothers delivered at the public hospitals in Hawassa city, Sidama Regional State, Ethiopia, 2024
Intra-partum related characteristics of study participant
Of the participants included in the study, 236(63.3%) mothers gave birth through spontaneous vaginal delivery, while approximately 117(31.4%) mothers underwent cesarean section for delivery. Among the mothers who
took part in the study, around 61 (16.4%) experienced prolonged labor, while 36(9.7%) mothers encountered obstructed labor. Nearly one-fifth (25.5%), of the mothers in labor had stained amniotic fluid with either meconium or blood (Table 4).
Variables | Frequency | Percentage |
Duration of labour | ||
Prolonged | 61 | 16.4 |
Normal | 312 | 83.6 |
Mode of delivery | ||
SVD | 236 | 63.3 |
CS | 117 | 31.4 |
Instrumental | 20 | 5.4 |
Fetal presentation | ||
Vertex | 354 | 94.9 |
Non-vertex | 19 | 5.1 |
Obstructed labor | ||
Yes | 36 | 9.7 |
No | 337 | 90.3 |
Amniotic fluid | ||
Stained | 95 | 25.5 |
Clear | 278 | 74.5 |
Color of amniotic fluid | ||
Clear | 278 | 74.5 |
Meconium stained | 84 | 22.5 |
Blood stained | 11 | 2.9 |
Premature rupture of membrane (PROM) | ||
Yes | 63 | 16.9 |
No | 310 | 83.1 |
Table 4: Intra-partum related characteristics of mothers delivered at the public hospitals in Hawassa city, Sidama regional state, Ethiopia, 2024
Neonatal related characteristics of study participant
Among the newborns included in the study, 254 (68.1%) were female. In terms of gestational age, the majority of the newborns, 242 (64.9%) infants were born at full term, whereas 58 infants (15.5%) were born prematurely. Approximately 59 newborns (15.8%) experienced fetal distress during the time of birth (Table 5).
Variables | Frequency | Percentage |
Sex of the new born | ||
Male | 119 | 31.9 |
Female | 254 | 68.1 |
Gestational age | ||
Preterm | 58 | 15.5 |
Term | 242 | 64.9 |
Post term | 73 | 19.6 |
Fetal distress | ||
Yes | 59 | 15.8 |
No | 314 | 84.2 |
Table 5: Neonatal related characteristics of mothers delivered at the public hospitals in Hawassa city, Sidama regional state, Ethiopia, 2024
Magnitude of Birth Asphyxia among Newborns
The magnitude of birth asphyxia among newborns at public hospitals in Hawassa city was 25.7% (95% CI: 21.3% - 30.2%) (Figure2).
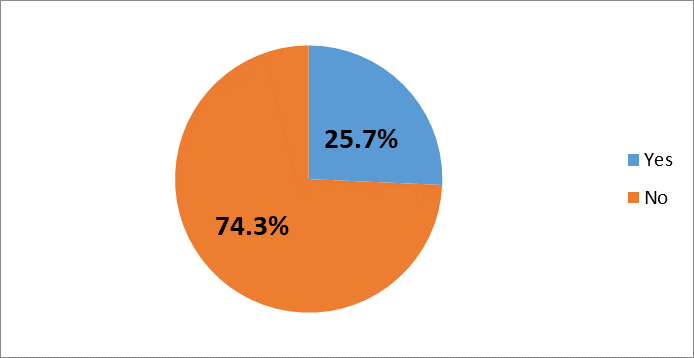
Figure 3: Magnitude of birth asphyxia among new-borns at the public hospitals in Hawassa city, Sidama regional state, Ethiopia, 2024
Factors associated with birth asphyxia
In the bivariate analysis, a total of nine variables with p-values less than 0.25 became eligible for multivariable logistic regression. After controlling for possible confounders in multivariable logistic regression, four variables such as maternal anemia, preeclampsia, duration of the labour, and meconium-stained amniotic fluid were obtained as determinants of birth asphyxia.
Neonates born to mothers with anemia were 2.72 times more likely to develop birth asphyxia compared with their counterpart (AOR=2.72; 95%
CI: 1.14, 6.51). The neonates born to mothers having preeclampsia were 4.33 times more likely to develop birth asphyxia compared with those born to mothers without preeclampsia (AOR=4.33; 95% CI: 1.49, 12.57). Newborns who were born from mothers with prolonged labor were 5.37 times more likely to develop birth asphyxia compared with mothers with normal labor (AOR=5.37; 95% CI: 2.46, 11.71). Newborns who had meconium-stained fluid 6.43 times more likely to develop birth asphyxia compared with their counterpart (AOR=6.43, 95% CI: 3.46, 11.96) (Table 6).
Variables | Birth asphyxia |
COR [95% CI] |
AOR [95% CI] | P-Value | |
No | Yes | ||||
Educational Status of the mother | |||||
Primary and below | 114 | 37 | 1 |
| |
Secondary school | 106 | 35 | 1.02(0.59, 1.73) | 1.56(0.76, 3.19) | 0.22 |
College and above | 57 | 24 | 1.29(0.71, 2.37) | 1.80(0.78, 4.14) | 0.17 |
Residence of the mother | |||||
Rural | 17 | 10 | 1.78(0.79, 4.03) | 0.79(0.21, 2.93) | 0.72 |
Urban | 260 | 86 | 1 |
| |
ANC Visit Frequency | |||||
One visit | 106 | 41 | 1 |
| |
2-3 visits | 103 | 27 | 0.68(0.39, 1.18) | 0.54(0.27, 1.10) | 0.08 |
Four and above | 68 | 28 | 1.07(0.30, 1.88) | 1.01(0.48, 2.14) | 0.98 |
Maternal anemia | |||||
Yes | 23 | 21 | 3.09(1.62, 5.90) | 2.72(1.14, 6.51)* | 0.024 |
No | 254 | 75 | 1 |
| |
Antepartum Hemorrhage | |||||
Yes | 7 | 11 | 4.99(1.88, 13.28) | 3.20(0.92, 11.09) | 0.067 |
No | 269 | 85 | 1 |
| |
Preeclampsia | |||||
Yes | 10 | 11 | 3.46(1.42, 8.42) | 4.33(1.49, 12.57)* | 0.007 |
No | 267 | 85 | 1 |
| |
Duration of the labour | |||||
Prolonged | 22 | 39 | 7.93(4.93, 14.39) | 5.37(2.46, 11.71)* | 0.0001 |
Normal | 255 | 57 | 1 |
| |
Meconium stained | |||||
Yes | 42 | 53 | 6.89(4.10, 11.59) | 6.43(3.46, 11.96)* | 0.0001 |
No | 235 | 43 | 1 |
| |
Fetal presentation | |||||
.Vertex | 272 | 82 | 1 |
| |
Non-vertex | 5 | 14 | 9.29(3.25, 26.56 ) | 3.24(0.86, 12.20) | 0.083 |
Table 6: Bivariate and multivariable logistic regression analysis between predictor variables and birth asphyxia among new-born delivered at public hospitals in Hawassa city administration, Sidama regional state, Ethiopia, 2024
COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval *P-Value <0>
Discussion
Current study found that the magnitude of birth asphyxia was 25.7% (95% CI: 21.3% - 30.2%). The result aligns with findings obtained in various regions of Ethiopia ranging from 22.1% to 29.9%, Kenya (29.1%) and Nigeria (30.1%) (5, 23, 24, 25, 26). However, the result of current study seems a higher prevalence compared to previous studies conducted in other several parts of Ethiopia those ranging from 3.1% to 19.9% and India (5.7%) and Indonesia (12.31%) (27, 28, 29, 30). Nevertheless, the current result is lower than findings from some of previous studies conducted in Southern Ethiopia (32.8%), Jimma (32.9%) and Bangladesh (56.9%) respectively (9, 31, 32). These variations might be due to differences in study settings, health service deliveries and gaps in community engagement concerning maternal health issues.
The result showed that maternal anemia was found to be significantly associated with birth asphyxia which is consistent with previous study conducted in Southern Ethiopia and India (31, 33). The possible justifications might be due to the effect of anemia on fetal development and birth.
Current study revealed that, preeclampsia was one of the factors that had a significant association with birth asphyxia. The odds of birth asphyxia among neonates from mothers with preeclampsia were more than four times compared with their counterpart. This finding is in line with the findings of previous study conducted in Ethiopia, Cameroon, Pakistan and Indonesia, (34, 35, 36, 37). The possible reason might be due to the fact that complications related with delivery such as preeclampsia may decrease the blood flow and oxygen supply to the infant and in turn lead to birth asphyxia.
Current findings revealed that prolonged labour increase the odds of birth asphyxia by more than five times compared with their counterparts. This finding is in line with results obtained from several parts of Ethiopia, Cameroon, Colombia and Sweden (24, 28, 34, 38). The possible explanation for this association could be the detail that prolonged labor is associated with fetal and maternal exhaustion and fetal distress can result birth asphyxia.
Meconium-stained amniotic fluid was also obtained as an independent factor of birth asphyxia. Newborn from mothers with history of meconium-stained amniotic fluid had more than six times more risk developing birth asphyxia compared with without history of meconium-stained amniotic fluid had. This is in line with previous studies done in several parts of Ethiopia, Bangladesh and Indonesia (25, 26, 31, 35, 37).The possible reason could be that meconium-stained amniotic fluid results in per-partum inhalation of meconium-stained amniotic fluid and filled smaller airways and alveoli in the lung, leading to mechanical obstruction of airways that can lead to limited gas exchange and birth asphyxia could occur.
Strengths of the study
Data quality measures taken in all steps. As its nature of cross sectional study data on all variables was only collected once, multiple outcomes and exposures could be studied
Limitation of the study
As the study was a cross-sectional base, founding causal relationship between the independent and outcome variables was difficult, and also as the study is facility base may hinders the generalizability of results for the whole community.
Conclusion and recommendations
The overall magnitude of birth asphyxia from current study obtained as high. Maternal anemia, preeclampsia, prolonged labor and meconium-stained amniotic fluid were found as the contributing factors influencing the occurrence of birth asphyxia.
In order to decrease the problem of birth asphyxia, it is important to improve the quality of antepartum and intra-partum care through the implementation of various strategies. All responsible bodies should work on those strategies focusing on preventing prolonged labor, maternal anemia, preeclampsia related challenges and promptly identifying obstetric complications and ensuring strict monitoring and follow-up of mothers during delivery. Governmental as well as non-governmental organizations should work integrate to tackle the predisposing factors of birth asphyxia.
List of abbreviations
ANC: Antenatal Care
AOR: Adjusted odds ratio
APGAR: Appearance, Pulse, Grimace, Activity, Respiration
EDHS: Ethiopian Demographic and Health Survey
HIE: Hypoxic- Ischemic Encephalopathy
MAS: Meconium Aspiration Syndrome
NBW: Normal Birth Weight
NICU: Neonatal Intensive Care Unite
NM: Neonatal Mortality
PNA: Prenatal Asphyxia
RDS: Respiratory Distress Syndrome
SDG: Sustainable Development Goal
WHO: World Health Organization
Ethical clearance
Research Ethical clearance was obtained from Institutional Review Board (IRB) of Yanet Liyana College of health science and permission was granted from Sidama Regional Health Bureau, Hawassa City Administration health department and sample hospitals after discussing and clarifying the objectives of the study and its importance’s towards improving child health. The benefit and harm of participating in this research were clearly described for each participants. After clarifying in the research, informed consent was obtained from all subjects and/or their legal guardians. All methods were carried out in accordance with relevant guidelines and regulations Privacy and confidentiality of participants’ information was ensured throughout the process.
Conflict of Interest:
All researchers declare that there is no conflict of interest and as that they have done each steps of current study with in agreement.
Acknowledgment
Above all, we thank the Almighty God for all. We would like to acknowledge Yanet Liyana College of health science, for granting ethical clearance for this research work. We would also like to extend our deepest gratitude to all health facilities those permit us to conduct the research and for their collaboration work and giving all information’s. Our sincere gratitude goes to data collectors and supervisors of the data collection. Last but not least our acknowledgement goes to study participants.
Authors’ details and contribution for the current study
DDB: Dr Derese Desalegn Buta (MPH, MBA, PhD): (ORCID iD https://orcid.org/0000-0002-7707-8389)
Sidama Regional Health Bureau, Health Extension Program and Primary Health Care advisor, Senior Public Specialist and health consultant, Researcher, student research advisor and lecturer, Yanet Liyana College of health science and Phama College of Health Science:
Supervises each and every steps of current study, proposal development, advice and test data collection tool, guide data collection steps, supervise and re-conduct data analysis and result writing part. Develop and finalize manuscript development.
ESH: Elsabet Shudura Hayesso (BSc, MPH-RH), Sidama Regional Health Bureau; participated in developing research proposal and data collection tool, train data collectors and supervisors, supervise data collection steps, did data cleaning, entry, analysis, result writing and finalizing the document.
ASW: Ayalew Sembeto Worassa (BSc, MPH), Adare General Hospital, Sidama Regional Health Bureau, post graduate student at Yanet Liyana College of Health Science
Idea generating, developing research proposal and data collection tool, train data collectors and supervisors, supervise data collection steps, did data cleaning, entry, analysis, result writing and finalizing the document.
Availability of data and materials
The datasets produced and/or analyzed throughout the current study are not openly accessible due to institutional regulation but would be obtainable from the authors for reasonable request.
Clinical number
No need of Clinical trial number as the current study is not clinical trial base study
Funding
There was no financial support for the current study obtained from anywhere and the researchers tried to cover it accordingly.
References
- World health organization (WHO). New-borns: reducing mortality, 2018 [cited 2018 December, 11,]. Available from: https://www.who.int/news-room/fact-sheets/detail/newborns-reducingmortality .
View at Publisher | View at Google Scholar - Liu L, Oza S, Hogan D, Chu Y, Perin J, Zhu J, et al. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. The Lancet. 2016; 388(10063):3027-35.
View at Publisher | View at Google Scholar - Lawn JE, Cousens S, Zupan J, Team LNSS. 4 million neonatal deaths: when? Where? Why? The lancet. 2005; 365(9462):891-900.
View at Publisher | View at Google Scholar - Lawn JE, Blencowe H, Oza S, You D, Lee AC, Waiswa P, et al. Every Newborn: progress, priorities, and potential beyond survival. The Lancet. 2014; 384(9938):189-205.
View at Publisher | View at Google Scholar - Ilah BG, Aminu MS, Musa A, Adelakun MB, Adeniji AO, Kolawole T. Prevalence and risk factors for perinatal asphyxia as seen at a specialist hospital in Gusau, Nigeria. Sub-Saharan African Journal of Medicine. 2015; 2(2):64.
View at Publisher | View at Google Scholar - Bhutta ZA. Paediatrics in the Tropics. . Manson’s Tropical Infectious Diseases,. 2014: 1197– 214.e2. doi:10.016/b978-0-7020-5101-2.00081-9
View at Publisher | View at Google Scholar - Wall SN, Lee AC, Niemeyer S, English M, Keenan WJ, Carlo W, et al. Neonatal resuscitation in low‐resource settings: what, who, and how to overcome challenges to scale up: International Journal of Gynaecology & Obstetrics. 2009; 107(Supplement):S47-S64.
View at Publisher | View at Google Scholar - FMOH. Neonatal Intensive Care Unit (NICU) Training Manual. 2015.
View at Publisher | View at Google Scholar - Health P AA, Melaku G, Abera GB. Prevalence and associated factors of perinatal asphyxia among newborns in Dilla University referral hospital, Southern Ethiopia 2019.
View at Publisher | View at Google Scholar - Selvakumar R, Vasanthamalar C, Deepthy SIJ. Incidence, Severity and Early Outcome of Hypoxic- ischemic Encephalopathy among New-borns Born in a Rural Tertiary Care Centre in Southern India DOI: 10.17354/ijss/2017/52. 2017; 5(8):63–6.
View at Publisher | View at Google Scholar - MS. NIRMALA.M.L. NO 40 4TH A Cross Near RAMAN COLLEGE, VINAYAKA NAGAR Rajiv Gandhi University of Health Sciences, Bangalore Karnataka Brief Resume of the Intended Work.
View at Publisher | View at Google Scholar - Tasew H, Zemicheal M, Teklay G, Mariye T, Ayele E. Risk factors of birth asphyxia among new-borns in public hospitals of Central Zone, Tigray, Ethiopia 2018. BMC research notes. 2018; 11(1):496.
View at Publisher | View at Google Scholar - Lee AC, Cousens S, Wall SN, Niemeyer S, Darmstadt GL, Carlo WA, et al. Neonatal resuscitation and immediate new-born assessment and stimulation for the prevention of neonatal deaths: a systematic review, meta-analysis and Delphi estimation of mortality effect. BMC public health. 2011; 11(3):S12.
View at Publisher | View at Google Scholar - WHO. Levels and Trends in Child Mortality. In.: United Nations Children’s Fund; 2018.
View at Publisher | View at Google Scholar - EDHS. Ethiopia Demographic and Health Survey: Central Statistical Agency Key Indicators Report. Addis Ababa, Ethiopia: October, 2016.
View at Publisher | View at Google Scholar - WHO:. World health statistics: monitoring health for the SDGs, sustainable development goals. . WHO Library Cataloguing-in-Publication Data. 2016: 1-136.
View at Publisher | View at Google Scholar - FMOH. Health sector transformation plan-I. 2016.
View at Publisher | View at Google Scholar - Alkema L, Chou D, Hogan D, Zhang S, Moller A-B, Gemmill A, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation InterAgency Group. The Lancet. 2016;387(10017):462
View at Publisher | View at Google Scholar - Aliyu I, Lawal T, Onankpa B. Prevalence and outcome of perinatal asphyxia: Our experience in a semi-urban setting. Trop J Med Res 2017; 20:161
View at Publisher | View at Google Scholar - Ellsbury DL, Clark RH, Ursprung R, Handler L, Dodd ED, Spitzer AR. A multifaceted approach to improving outcomes in the NICU: The pediatrix 100 000 babies’ campaign. Pediatrics 2016; 137:e20150389.
View at Publisher | View at Google Scholar - Manu A, Arifeen S, Williams J, Mwasanya E, Zaka N, Plowman BA, et al. Assessment of facility readiness for implementing the WHO/ UNICEF standards for improving quality of maternal and newborn care in health facilities experiences from UNICEF’s implementation in three countries of South Asia and Sub-Saharan Africa. BMC Health Serv Res 2018; 18:531
View at Publisher | View at Google Scholar - Mukhtar-Yola M, Audu LI, Olaniyan O, Akinbi HT, Dawodu A, Donovan EF. Decreasing birth asphyxia: Utility of statistical process control in a low-resource setting. BMJ Open Qual 2018; 7:e000231.
View at Publisher | View at Google Scholar - Erick Kiptui Kibai. Perinatal factors associated with birth asphyxia among neonates in maternity ward Kakamega county refferal hospital, Kenya. 2017.
View at Publisher | View at Google Scholar - Gebreheat G, Tsegay T, Kiros D, Teame H, Etsay N, Welu G, et al. Prevalence and Associated Factors of Perinatal Asphyxia among Neonates in General Hospitals of Tigray, Ethiopia, 2018. BioMed research international. 2018; 2018.
View at Publisher | View at Google Scholar - E.A. Lake et al. Magnitude of Birth Asphyxia and Its Associated Factors Among Newborns Delivered at Wolaita Sodo University Teaching and Referral Hospital, Southern Ethiopia, 2018. The Tropical Journal of Health Sciences. 2019; Vol 26 No 4.
View at Publisher | View at Google Scholar - Asfere WN, Yesuf A. Neonatal asphyxia and associated factors among neonates on labor ward at debre-tabor general hospital, Debre Tabor Town, South Gonder, North Centeral Ethiopia. Int J Pregn & Chi Birth. 2018; 4(6):208‒212. DOI: 10.15406/ipcb.2018.04.00128
View at Publisher | View at Google Scholar - Murali Krishnan P, Padarthi S. A Prospective Study on Intrapartum Risk Factors for Birth Asphyxia. IOSR Journal of Dental and Medical Sciences (IOSR-JDMS). 2016; 15(9).
View at Publisher | View at Google Scholar - Ibrahim NA, Muhye A, Abdulie S (2017) Prevalence of Birth Asphyxia and Associated Factors among Neonates Delivered in Dilchora Referral Hospital, in Dire Dawa, Eastern Ethiopia. Clinics Mother Child Health 14: 279. doi:10.4172/2090-7214.1000279
View at Publisher | View at Google Scholar - Amare Wudu and Birehanu. Predictors of Birth Asphyxia among New-borns in Public Hospitals of Eastern Amhara Region, North-eastern Ethiopia, 2022. Clinical Medicine Insights: Pediatrics. 2023. Volume 17: 1–10
View at Publisher | View at Google Scholar - Abdo et al. Prevalence and contributing factors of birth asphyxia among the neonates delivered at Nigist Eleni Mohammed memorial teaching hospital, Southern Ethiopia: a cross-sectional study. BMC Pregnancy and Childbirth. 2019; 19:536
View at Publisher | View at Google Scholar - Solayman, Hoque, Akber,.Prevalence of Perinatal Asphyxia with Evaluation of Associated Risk Factors in a Rural Tertiary Level Hospital Vol. 8, No.-1 (2017).
View at Publisher | View at Google Scholar - Jebessa Wayessa Z, Belachew T, Joseph J. Birth Asphyxia and Associated Factors among Newborns Delivered in Jimma Zone Public Hospitals, Southwest Ethiopia: A Cross-sectional Study. Journal of Midwifery and Reproductive Health. 2018; 6(2):1289-1295. DOI: 10.22038/JMRH.2018.10483
View at Publisher | View at Google Scholar - Yadav N, Damke S. Study of risk factors in children with birth asphyxia. International Journal Contemp Pediatr 2017; 4:518-26.
View at Publisher | View at Google Scholar - Chiabi A, NGUEFACK S, Evelyne M, NODEM S, MBUAGBAW L, MBONDA E, et al. Risk factors for birth asphyxia in an urban health facility in Cameroon. Iranian journal of child neurology. 2013; 7(3):46.
View at Publisher | View at Google Scholar - Molla M, Mekonnen A, Godie Y, Guadie Y, Birhanu D. Magnitude of Birth Asphyxia and Associated Factors among Newborns Admitted in Neonatal Intensive Care Unit at Government Hospitals in Addis Ababa, Ethiopia, 2021: Multicenter Cross-Sectional Study. Neonat Pediatr Med. 2022; 8: 246.
View at Publisher | View at Google Scholar - Aslam et al. risk factors of birth asphyxia. Italian Journal of Pediatrics.2014; DOI 10.1186/s13052-014-0094-2
View at Publisher | View at Google Scholar - Tri Adharia Sekarwati , Ninik Darsini, Dominicus Husada. Risk Factors for Neonatal Asphyxia Occurrence at General Hospital Dr. M. Soewandhie, Surabaya. Indian Journal of Public Health Research & Development, April 2020, Vol. 11, No. 04
View at Publisher | View at Google Scholar - A Sandström et al Durations of second stage of labor and pushing, and adverse neonatal outcomes: a population-based cohort study. Journal of Perinatology. 2017; 236 – 242
View at Publisher | View at Google Scholar
