

Review | DOI: https://doi.org/10.31579/2834-5010/030
Future direction of Quality Improvement of Neonatal Intensive Care Units: A Short Narrative Review*
1Specialist neonatologist, Dubai Hospital, Dubai health, UAE.
2Specialist pediatrician, Al Jalila Children's Specialty Hospital, Dubai health, UAE.
*Corresponding Author: Reham Helmy Amin Saad, Specialist neonatologist, Dubai Hospital, Dubai health, UAE.
Citation: Amin Saad RH, Maryam A. Alsada, (2025), Future direction of Quality Improvement of Neonatal Intensive Care Units: A Short Narrative Review, International Journal of Clinical Therapeutics, 4(2); DOI:10.31579/2834-5010/030
Copyright: © 2025, Reham Helmy Amin Saad. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 March 2025 | Accepted: 17 March 2025 | Published: 31 March 2025
Keywords: quality improvement; future direction of qi; neonatal icu; neonatal outcomes
Abstract
Background: Quality improvement (QI) methods have the potential to improve outcomes and care processes for hospitalized patients. In the neonatal ICU (NICU), unit-based QI projects have resulted in lower rates of bronchopulmonary dysplasia, hospital-acquired infection, hypothermia on admission, delivery room intubations, and increased the use of mother’s own milk at discharge.
Methods: This rapid improvement in the outcomes brought care quality in neonatal intensive care unit (NICU) to the surface. Quality improvement (QI) involves safe, timely, effective, efficient, equitable, and patient centered care. In this review, we discuss the neonatal mortality worldwide, described the methods of QI with examples of NICU QI topics. Each NICU can voluntarily develop a QI project, but systematic support is essential.
Conclusion: the future direction of Quality Improvement (QI) in Neonatal Intensive Care Units (NICUs) is evolving rapidly, driven by technological advancements, data analytics, patient-centered care models, and a growing focus on health equity and safety. Here are the key emerging trends and future directions.
1.Neonatal mortality worldwide
Neonatal mortality is a worldwide problem and is identified as a priority focus of the World Health Organization (WHO). The Millennium Development Goals 4 (MDG4) set by the WHO aim at reducing the under five years’ old child mortality rate by two-thirds between 1990 and 2015, of which the neonatal mortality (number of deaths within 28 days per 1000 live births) forms a crucial part. (1,2) The neonatal mortality rate (NMR) forms an important part of the under-five mortality rates. Neonatal deaths refer to the number of infants who died during the first month of life; this period is considered the time of highest risk for child death. (1) Neonatal deaths can be subdivided into early and late neonatal deaths with early neonatal deaths occurring from birth to seven days and late neonatal deaths being from seven to 28 days. (3)
Worldwide, a decrease in neonatal mortality lagged when compared to the under five years’ old mortality rates in 2012, indicating the global newborn mortality rate decreased only by 37% from 33/1000 live births to 21/1000 live births, representing 44% of the total under-five mortality rate. (4) The current reality is that 2.9 million neonatal deaths still occur worldwide. (5) The percentage of deaths occurring in the neonatal period increased to 44% as reflected in the latest statistics available. However, this percentage does not include the 2.6 million stillbirths, of which 1.2 million (45%) occur during labour. Furthermore, of these deaths 99% occur in low- and middle-income countries. (5, 6)
2. Quality improvement in the NICU
Quality improvement (QI) methods have the potential to improve outcomes and care processes for hospitalized patients. In the neonatal ICU (NICU), unit-based QI projects have resulted in lower rates of bronchopulmonary dysplasia, hospital-acquired infection, hypothermia on admission, delivery room intubations, and an increased use of mother’s own milk at discharge. (7, 8) Previous research has elucidated the characteristics of highly functioning QI teams and defined the specific contextual variables associated with successful QI work. Successful QI teams routinely contain subject matter expertise, include experts in QI methodology, focus on continuously measuring improvement, and have strong team and organizational leadership. (9) Similarly, hospitals that successfully support improvement projects have been found to have supportive leadership, rigorous performance and data monitoring, and effective teamwork. (10) Successful QI work requires both capability (QI knowledge and expertise) and capacity (the pragmatic ability to produce results). Parental involvement is also a critical component of neonatal QI as families are one of the most important stakeholders in improving clinical outcomes. (11) The challenge for many units, including NICUs, in advancing QI work is developing an infrastructure that supports the development of successful QI teams within the individual units. Despite growing literature describing the characteristics and contextual facilitators of successful QI teams, little exists in the medical literature describing pragmatic steps to build QI infrastructure at the unit level.
3. What is quality improvement in the NICU?
In the early 2000s, a survey conducted in 12 major cities in the United States to determine whether adults without major medical conditions and children receiving outpatient care were receiving appropriate and timely treatment revealed the shocking result that only 54.9% of adults and 46.5% of children were receiving appropriate care. (12,13, 14). Since the early 2000s, the Institute of Medicine (IOM) has been at the forefront of the U.S. shared the need for policies for quality management in the complex healthcare system, and both the public and private sectors have invested in and systematically implemented quality management. (15) According to IOM, quality of care is "the degree to which individual health care services are provided in a manner that maximizes the likelihood of achieving a desirable outcome and is consistent with current medical knowledge. (16,17)
To provide appropriate healthcare, there are six quality dimensions that must be achieved. Healthcare must be safe for patients, timely, effectively delivered to ensure proper use and avoid overuse, efficient to prevent waste of medical equipment and tools, equitable, and patient centered. (12,17) Sometimes referred to simply as STEEEP, the acronym for these three dimensions, if healthcare is provided in accordance with STEEEP, patients will receive safer, more reliable, intensive, and more useful healthcare benefits. Donabedian9) proposed three indicators for assessing healthcare quality: structure, process, and outcomes. The structure includes facilities, equipment, services, and treatment personne. (7)
In the NICU, this includes nursing staff per patient, patient volume per area, number of isolation rooms, number of ventilators, immediate availability of imaging equipment, and the number of personnel capable of resuscitation. Process encompasses the entire range of activities from clinical to patient delivery. For example, in the NICU, this includes the extent of handwashing before patient contact, the time from birth to administering artificial surfactant for respiratory distress syndrome, the rate of timely screening for retinopathy of prematurity, the rate of maternal steroid administration before delivery of premature infants, and the rate of breastfeeding. Outcome indicators within the NICU include neonatal mortality, sepsis frequency, bronchopulmonary dysplasia frequency, retinopathy of prematurity frequency, cerebral hemorrhage frequency, and CLABSI frequency. (7, 18)
4. Quality Improvement Methods
Before undertaking quality improvement activities, a multidisciplinary team comprised of leaders from various fields is necessary. Most quality improvement activities are comprised of a representative group of individuals working on the project. The team leader is selected as the most knowledgeable individual within the project, and the team facilitator is comprised of individuals with extensive experience in quality improvement activities and familiarity with improvement methods. Other team members include critical care physicians as technical experts, administrative nurses as leaders of routine patient care, hospital administrators as administrative leaders, and clinical pharmacists and clinical nurse managers. (7)
Quality improvement activities can be implemented using various methods, including the Care model, the Lean model, Six Sigma, focus analyze-develop-execute (FADE), total quality management (TQM), and the plan, do, study, act (PDSA) cycle. However, the PDSA cycle, commonly used in the healthcare industry, consists of the following five steps (Figure 1). Know why improvement is needed (goal), Have a feedback mechanism to determine whether improvement is occurring (measurement), Create an effective change method to achieve improvement (change), Test the change before implementing it, Know and establish when and how to implement the change. (16,19)
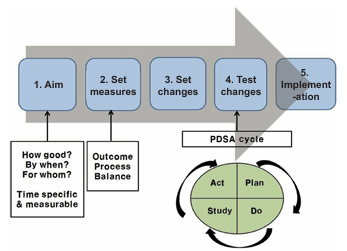
Figure 1: Methods of quality improvement. Abbreviation: PDSA, plan, do, study, act.
4.1. Goal Setting
Quality improvement goals include how well they will be achieved and by when. Goals should be specific, measurable, attainable, relevant, and timely (SMART). (16,19) For example, consider a NICU goal: "Reduce the NICU discharge readmission rate from 10% to 5% within the next six months," or "Increase the exclusive breastfeeding rate of newborns discharged from 50% to 80% by March 2019." To set such specific goals, it is necessary to collect current data in the target area, which serves as a baseline for assessing future improvements. (19)
4.2. Establishing Measurement Methods
Because improvement is not always achieved after attempting change, criteria are needed to determine whether to implement, implement, or discard the attempted change. To achieve this, a method for measuring data must be established. Determine measurement methods related to the objectives, but simple and practical methods are effective. Graphing the measured data is useful for visualizing the results. Depending on the content of the measurement, these can be categorized into outcome measures, process measures, and balance measures. (16,19) Outcome measures measure the desired final indicators, while process measures measure the steps or parts of the process for changing the outcome.
Balance measures determine whether changes intended to produce positive outcomes have had adverse effects in other areas. For example, with the goal of "Increasing the exclusive breastfeeding rate of newborns discharged from the neonatal unit from 50% to 80% by March 2019," if the following measurement methods were established as the exclusive breastfeeding rate at discharge (%), the time to first breastfeeding after delivery, the frequency of breastfeeding education provided by nurses to mothers, and the rate of readmission due to feeding problems, would be an outcome measure, and would be process measures, and would be a balance measure. Graphing the measurement data to view trends over time is very useful. (20, 21)
4.3. Change Planning
Because every problem has potential causes, exacerbating factors, and obstacles, before establishing changes for improvement, it is necessary to first analyze the underlying causes hindering change. While QI initiatives may bring about change, long-term changes that remain at the current level are merely reactive. Therefore, fundamental change may require a complete or partial overhaul of the system. This requires brainstorming within the QI team. Researching relevant literature on the QI topic or benchmarking successful practices can be helpful. Other changes in planning approaches include Fishbone diagrams (cause-and-effect diagrams), Driver diagrams, Force Field Analysis, and Process Mapping. Among these, the Fishbone diagram is a good example of a root cause analysis method (Figure 2). (16,19)
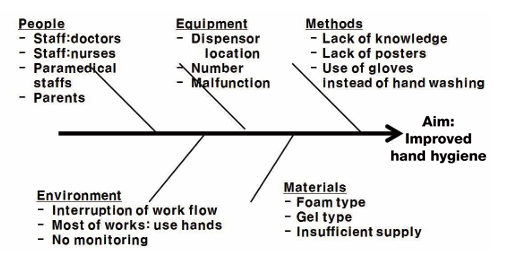
Figure 2: An example of fishbone diagram.
4.4. Testing Change
Because change attempts do not always lead to improvement, change must be put to the test. The PDSA cycle (Plan-Do-Study-Act) is a method for testing change (Figure 1). In the planning phase, we determine who will do what, when, and how to achieve our goals, and plan data collection. In the execution phase, we record any problems or unexpected events that arise while executing the plan and begin analyzing the data. In the analysis phase, we complete the data analysis, compare the data, and summarize any lessons learned.
In the action phase, we decide what changes to make and how to proceed with the next cycle. Even if we experience failure in the PDSA cycle, failure itself accelerates learning for change, so it is important to continue the PDSA cycle. Furthermore, if a single goal has multiple sub-goals, PDSA cycles for multiple QIs can be conducted simultaneously (Figure 3). (16,19)
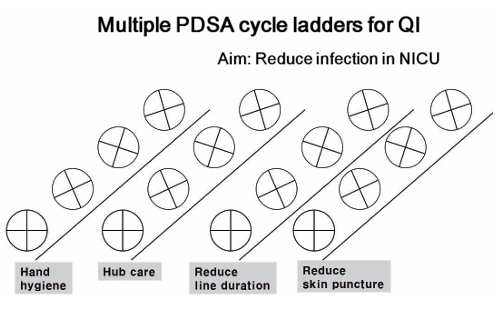
Figure 3: An example of multiple plans, do, study, act (PDSA) cycles. Abbreviations: NICU, neonatal intensive care unit; QI, quality improvement.
4.5. Establishing Changes
Additional efforts are needed to establish the changes created through the PDSA cycle in the system. Standardization and documentation of the changes are necessary. Training is necessary to familiarize daily staff with the changes, and support is needed to measure, manage, and maintain the level of training. (16, 19-26)
5. Quality Improvement Interventions and strategies for neonatal resuscitation
Structured improvement efforts have impacted numerous aspects of neonatal resuscitation and delivery room care. Most of the published QI reports related to NRP can be grouped into three general topic areas: prevention of hypothermia, delayed cord clamping, and optimizing respiratory care. Numerous interventions have been shown to reduce heat loss and improve temperature regulation, including use of radiant warmers, early removal of wet blankets, pre-warming surfaces, use of exothermic warming mattresses, use of plastic wraps or polyethylene bags, and control of ambient environment temperature. (27-30)
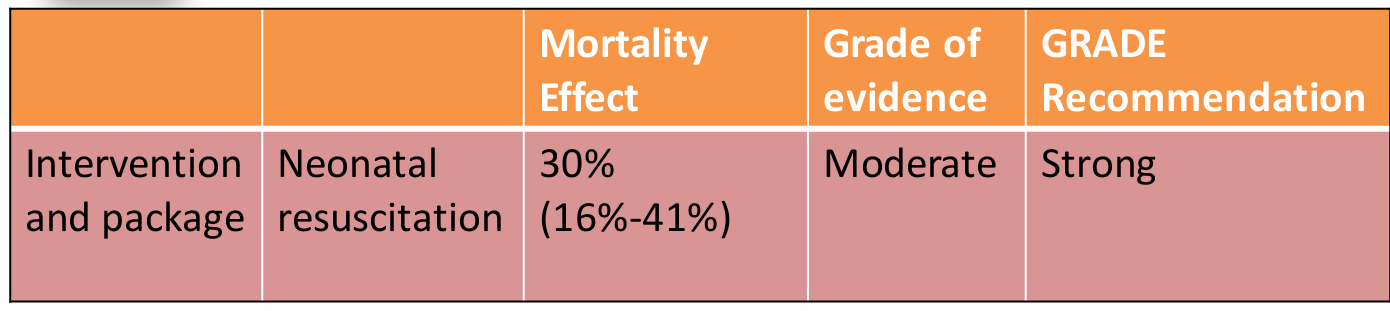
Table 1: Evidence of effect of neonatal resuscitation on intrapartum and neonatal outcomes.
Figure 4: Ustein formula of survival.
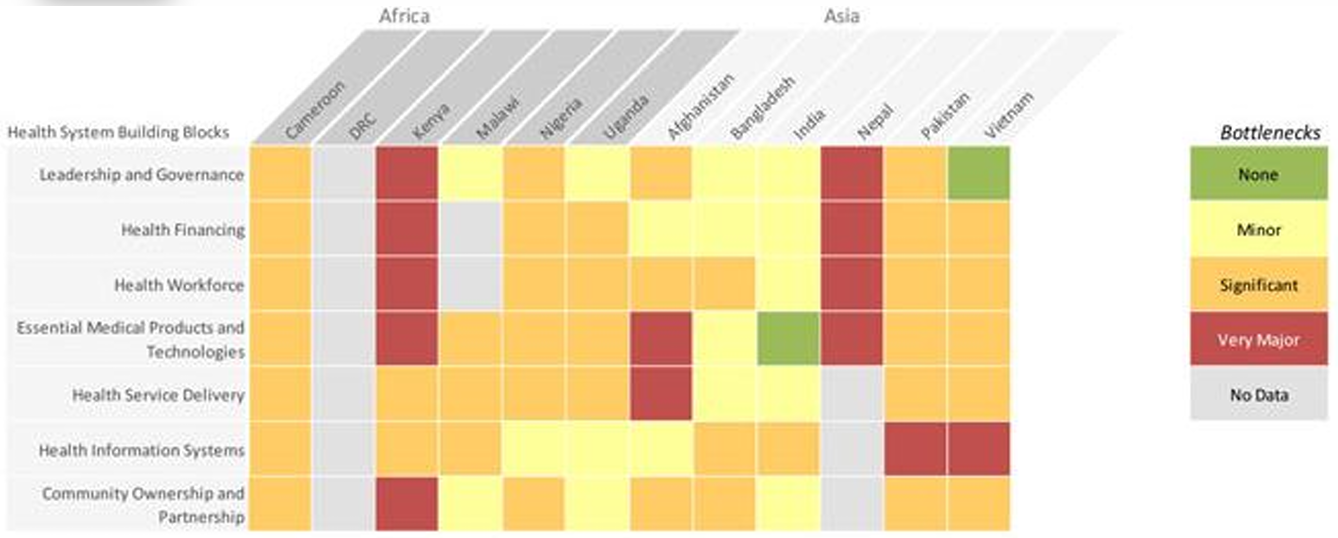
Figure 5: Health system bottlenecks for neonatal resuscitation.
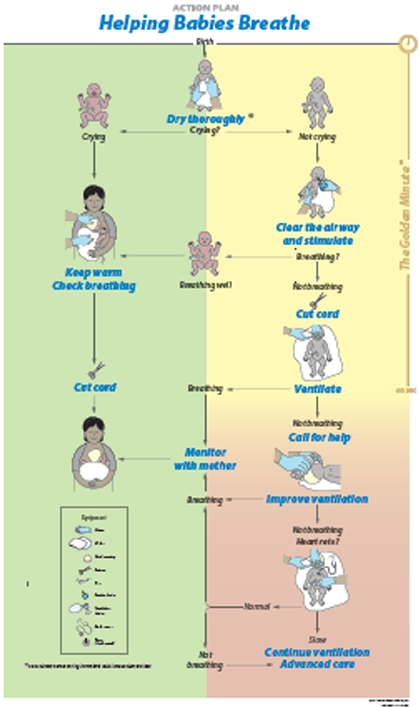
Figure 6: Intervention-Helping Babies Breathe Quality Improvement Cycle (HBB QIC).
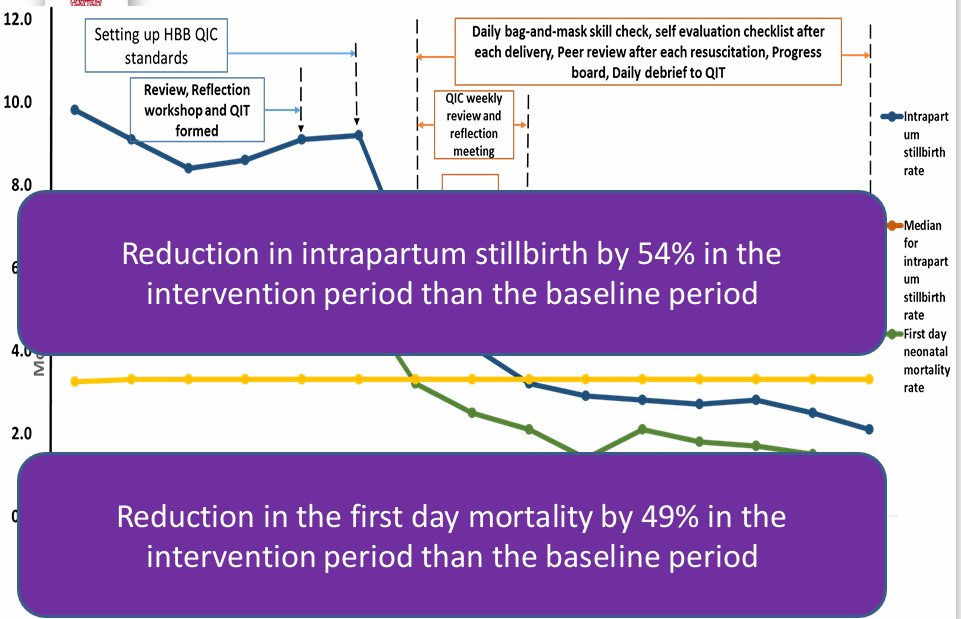
Figure 7: The intrapartum stillbirth rate, first day neonatal mortality rate monthly over time.
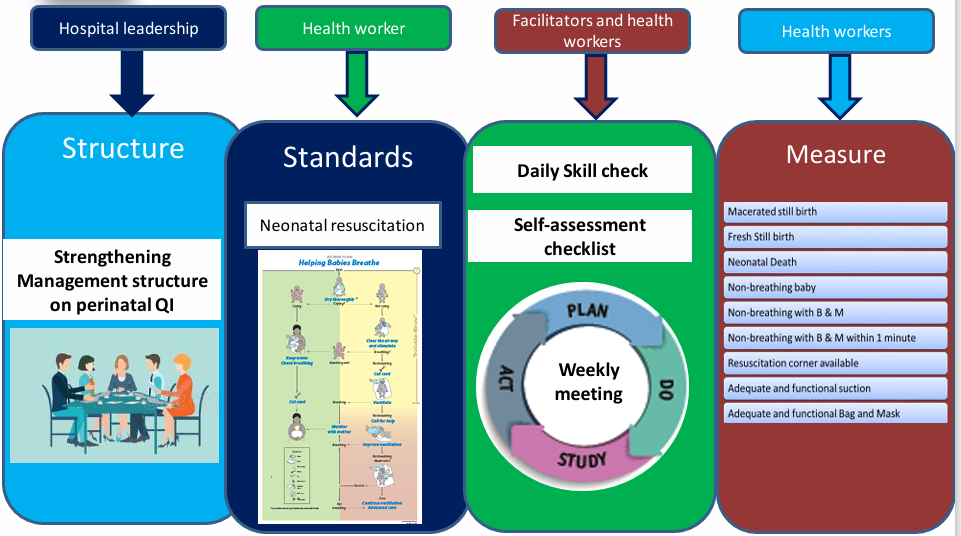
Figure 8: Quality improvement intervention.
6. Future Directions for NICU QI
While QI is a voluntary activity, systematic implementation by forming a multidisciplinary QI team is necessary to provide high-quality care to current NICU patients. When implementing QI for the first time, support from the hospital may be necessary for methodological aspects. An example of a large US hospital implementing NICU QI is the NICU CLABSI rate, central venous catheter bundle performance rate, hand hygiene rate, unplanned extubation rate, peripheral intravascular catheter infiltration/extravasation rate, hospital-acquired pressure injury rate, ventilator-associated event rate, breast milk mix-up rate, safety issues, mortality rate, and readmission rate within 7 days of discharge. The QI meeting is held periodically to discuss performance improvements. For each topic, the working group conducts a PDSA cycle and analyzes the data to determine the direction of change.
Currently, many NICU systems in Korea are inadequate, including the number of medical personnel, equipment, and the environment. Therefore, cooperation from the hospital may be necessary for QI initiatives. Furthermore, support from the hospital may be necessary for system improvements discovered during QI. Beyond individual QI initiatives within each NICU, collaborative QI management through a network is also necessary. International neonatal collaborative networks, such as the Vermont Oxford Network (VON), the Canadian Neonatal Network (CNN), and the California Perinatal Quality Care Collaborative (CPQCC), conduct QI-related research and provide baseline data on morbidity rates. (17, 18) Furthermore, the American Academy of Pediatrics (AAP) also has a Steering Committee.
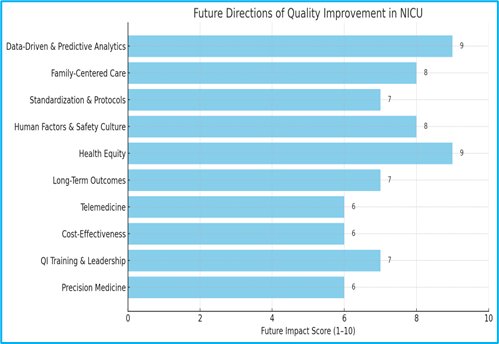
Figure 9: Future Directions for NICU QI.
The future direction of Quality Improvement (QI) in Neonatal Intensive Care Units (NICUs) is evolving rapidly, driven by technological advancements, data analytics, patient-centered care models, and a growing focus on health equity and safety. Here are the key emerging trends and future directions:
1. Data-Driven and Predictive Quality Improvement
- Real-time data integration: Use of electronic health records (EHRs), clinical dashboards, and real-time analytics to monitor key quality metrics.
- Predictive analytics & AI: Machine learning models to predict adverse events such as sepsis, necrotizing enterocolitis (NEC), or retinopathy of prematurity, enabling early intervention.
- Benchmarking: Participation in national databases (e.g., Vermont Oxford Network) to compare performance with peers and guide improvement.
2. Family-Centered and Developmental Care
- Emphasis on Family Integrated Care (FICare) and involving parents as partners in QI initiatives.
- Support for skin-to-skin contact (kangaroo care), breastfeeding support, and NICU parental education as QI metrics.
- Measuring parent satisfaction and outcomes as part of quality frameworks.
3. Standardization and Evidence-Based Protocols
- Development of standardized care bundles for common conditions (e.g., central line-associated bloodstream infections, ventilator-associated pneumonia).
- Use of clinical pathways and order sets to reduce variation in care.
4. Human Factors and Safety Culture
- Implementation of Just Culture principles to encourage error reporting and learning.
- Use of simulation-based training to improve team communication and response to critical events.
- Focus on team-based care, interprofessional collaboration, and safety checklists.
5. Health Equity and Disparity Reduction
- Stratifying NICU outcomes by race, ethnicity, and socioeconomic status to uncover disparities.
- Developing equity-focused QI initiatives, such as culturally sensitive care, language access services, and implicit bias training.
6. Neonatal Follow-Up and Long-Term Outcomes
- Expanding QI to include neurodevelopmental outcomes and follow-up care beyond NICU discharge.
- Integration with early intervention services and pediatric primary care for continuity of care.
7. Telemedicine and Remote Monitoring
- Using telehealth for family support, consultations, and education.
- Remote video monitoring for off-site quality assessments and family engagement in care rounds.
8. Sustainability and Cost-Effectiveness
- Emphasis on high-value care: balancing outcomes with costs.
- Evaluating the cost-benefit of QI initiatives to promote sustainable improvements.
9. QI Capacity Building and Leadership Development
- Training neonatal clinicians in QI methodology (e.g., PDSA cycles, Lean Six Sigma).
- Creating QI champions and embedding QI into residency and fellowship curricula.
10. Precision Medicine and Genomics
- Incorporating genetic screening and precision diagnostics into quality frameworks.
- Personalizing care plans based on genetic and metabolic profiles.
With the increase in high-risk newborns, NICUs have experienced significant growth both quantitatively and qualitatively. However, now is the time for qualitative growth to follow suit. QI activities within NICUs can be implemented through multidisciplinary teams, setting goals related to current priorities, and implementing a PDSA cycle. Leaders should understand that problems should not be blamed on individuals but rather should be addressed through systemic change. They should strive to establish systems through cooperation with hospitals when necessary. Maintaining QI through individual NICU and institutional efforts may be limited, and external support is essential. Where differences in quality persist across institutions, root cause analysis is necessary. Support for QI implementation training for healthcare professionals is also needed.
References
- Bradshaw D, Chopra M, Kerber K, et al. Every death count: Use of mortality audit data for decision making to save the lives of mothers, babies and children in South Africa. Lancet. 2008a;317(9620):1294–1304.
View at Publisher | View at Google Scholar - Bryce J, Daelmans B, Dwivedi A, et al. Countdown to 2015 for maternal, newborn, and child survival: The 2008 report on tracking coverage of interventions. Lancet. 2008;317(9620):1247–1257
View at Publisher | View at Google Scholar - Pattinson, RC. Saving babies 2008-2009: Seventh report on perinatal care in South Africa. Pretoria: Tshepesa Press; 2011.
View at Publisher | View at Google Scholar - World Health Organization. Every newborn: An action plan to end preventable deaths [homepage on the Internet]. 2014 [cited 2014 Aug 7]. Geneva: World Health Organization. www.EveryNewborn.org
View at Publisher | View at Google Scholar - Darmstadt GL, Kinney MV, Chopra M, et al. Who has been caring for the baby? Lancet [serial online]. 2014 [cited 2014 Jan 5]; 384:174–188. http://dx.doi.org/10.1016/S0140-6736(14)60458-x
View at Publisher | View at Google Scholar - Berkley S, Dybul M, Godal T, Lake A. Integration and innovation to advanced newborn survival. Lancet [serial online]. 2014 [cited 2014 Aug 14]; 384: e22–e23. http://dx.doi.org/10.1016/S0140-6736(14)60691-7
View at Publisher | View at Google Scholar - Bapat R, et al.A multidisciplinary quality improvement effort to reduce bronchopulmonary dysplasia incidence. J Perinatol. 2020;40(4):681–687.
View at Publisher | View at Google Scholar - Fugate K, et al. Improving human milk and breastfeeding practices in the nicu. J Obstet Gynecol Neonatal Nurs. 2015;44(3):426–438; quiz E414–425.
View at Publisher | View at Google Scholar - Brandrud AS, et al.Domains associated with successful quality improvement in healthcare - a nationwide case study. BMC Health Serv Res. 2017;17(1):648.
View at Publisher | View at Google Scholar - Taylor N, et al.High performing hospitals: A qualitative systematic review of associated factors and practical strategies for improvement. BMC Health Serv Res. 2015; 15:244.
View at Publisher | View at Google Scholar - Celenza JF, et al.Family involvement in quality improvement: From bedside advocate to system advisor. Clin Perinatol. 2017;44(3):553–566.
View at Publisher | View at Google Scholar - Institution of Medicine US, Committee on Quality of Health Care in America. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academy Press, 2001.
View at Publisher | View at Google Scholar - McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristofaro A, et al. The quality of health care delivered to adults in the United States. N Engl J Med 2003; 348:2635-45.
View at Publisher | View at Google Scholar - Mangione-Smith R, DeCristofaro AH, Setodji CM, Keesey J, Klein DJ, Adams JL, et al. The quality of ambulatory care deli referred to children in the United States. N Engl J Med 2007;357: 1515-23.
View at Publisher | View at Google Scholar - Kohn LT, Corrigan J, Donaldson MS. To err is human: building a safer health system. Washington, DC: National Academy Press; 2000.
View at Publisher | View at Google Scholar - Langley G, Moen R, Nolan K, Nolan T, Norman C, Provost L. The improvement guide: a practical approach to enhancing orga standardization performance. 2nd ed. San Francisco: Jossey-Bass Press, 2009.
View at Publisher | View at Google Scholar - Kim ES. Quality improvement in neonatal intensive care units. Neonatal medicine. 2018 May 30;25(2):53-7.
View at Publisher | View at Google Scholar - Donabedian A. Explorations in quality assessment and monitoring. The definition of quality and approaches its assessment. Vol. 1. Ann Arbor: Health Administration Press, 1980.
View at Publisher | View at Google Scholar - Institution for Healthcare Improvement. Open school [Internet]. Boston: Institution for Healthcare Improvement; c2018[cited 2018 May 21]. http://www.ihi.org/ education/ihiopenschool.
View at Publisher | View at Google Scholar - Provost LP, Murray S. The health care data guide: learning from data for improvement. San Francisco: Jossey-Bass Press, 2011.
View at Publisher | View at Google Scholar - Chawla D, Suresh GK. Quality improvement in neonatal care: a new paradigm for developing countries. Indian J Pediatr 2014; 81:1367-72.
View at Publisher | View at Google Scholar - Balakrishnan M, Raghavan A, Suresh GK. Eliminating undesirable able variation in neonatal practice: balancing standardization and customization. Clin Perinatol 2017; 44:529-40.
View at Publisher | View at Google Scholar - American Academy of Pediatrics Steering Committee on Quality Improvement and Management. Classifying recom Mendations for clinical practice guidelines. Pediatrics 2004; 114:874-7.
View at Publisher | View at Google Scholar - Isaac A, Saginur M, Hartling L, Robinson JL. Quality of reporting and evidence in American Academy of Pediatrics guidelines. Pediatrics 2013; 131:732-8.
View at Publisher | View at Google Scholar - Berwick DM. Era 3 for medicine and health care. JAMA 2016; 315:1329-30.
View at Publisher | View at Google Scholar - Ehret DY, Patterson JK, Bose CL. Improving neonatal care: a global perspective. Clin Perinatol 2017; 44:567-82.
View at Publisher | View at Google Scholar - McCall EM, Alderdice F, Halliday HL, Vohra S, Johnston L, Cochrane Neonatal Group. Interventions to prevent hypothermia at birth in preterm and/or low birth weight infants. Cochrane Database of Systematic Reviews. 1996 Sep 1;2018(2).
View at Publisher | View at Google Scholar - Roychoudhury S, Yusuf K. Thermoregulation: advances in preterm infants. Neo Reviews. 2017 Dec 1;18(12):e692-702.
View at Publisher | View at Google Scholar - Lawn JE, Kinney M, Lee AC, Chopra M, DonnayF, Paul VK, BhuttaZA, Bateman M, Darmstadt GL: Reducing intrapartum-related deaths and disability: can the health system deliver?IntJ GynaecolObstet2009, 107 Suppl1:S123-140, S140-122.
View at Publisher | View at Google Scholar - Enweronu-Laryea C, Dickson KE et al. Basic newborn care and neonatal resuscitation: a multicountry analysis of health system bottle necks and potential solutions. BMC Pregnancy Childbirth. 2015;15Suppl2: S4.
View at Publisher | View at Google Scholar
