

Review Article | DOI: https://doi.org/10.31579/2834-5029/075
Embolization of Urinary Bladder for the Treatment of Intractable Unresolving Visible Haematuria an Update
- Anthony Kodzo-Grey Venyo *
Department of Urology, North Manchester General Hospital, United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo, Department of Urology, North Manchester General Hospital, United Kingdom.
Citation: Grey Venyo AK, (2025), Embolization of Urinary Bladder for the Treatment of Intractable Unresolving Visible Haematuria an Update, International Journal of Biomed Research, 4(1): DOI:10.31579/2834-5029/075
Copyright: © 2025, Anthony Kodzo-Grey Venyo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 November 2024 | Accepted: 05 December 2024 | Published: 22 January 2025
Keywords: visible haematuria; unresolving blood in urine; selective angiography; embolization; CT scan
Abstract
Intractable visible haematuria is a severe, life-threatening condition which tends to be an emanation of many causes, some of which include an underlying malignant lesion mainly carcinoma of the prostate gland and urothelial cancer of the urinary bladder, inflammatory causes or radiotherapy associated cystitis as well medicament-induced cystitis, and sickle cell disease, and many other causes. The majority of cases of urinary bladder and prostatic-origin haematuria tend to be managed conservatively by irrigation with formalin, silver nitrate or alum solution, intra-vesical hydrostatic pressure, hyperbaric oxygen or endoscopic diathermy. Endoscopic resection of urinary bladder resection lesion with the undertaking of urinary diversion had traditionally been undertaken in scenarios in which conservative treatment had not been successful. The majority of patients who are afflicted by intractable visible haematuria tend to have a high surgical risk due to advanced age, various comorbidities and poor clinical status. Over a number of recent years, the undertaking of per-cutaneous, trans-catheter, arterial embolization of the urinary artery, in some cases, the internal iliac artery in difficult cases, and selective angiography of the vesical artery contemporaneously with super-selective embolization of a branch of the vesical artery that has been identified obviously upon the angiography, as, the source of bleeding has been promulgated as an attractive, minimal invasive, alternative option of treatment for patients who are suffering from visible haematuria from the urinary bladder that is not responding to conventional, non-invasive treatment. Most cases of embolization procedures to stop intractable haematuria has been undertaken under local anaesthesia successfully and most often the haematuria has settled, but at times there may be difficulties in the undertaking of the embolization procedure due to presence of complex pathological anatomy of the arterial blood supply of the vesical vascular system. Rare cases of recurrence of the haematuria develops and hence each patient who undergoes embolization of the urinary bladder supplying artery should be carefully observed. Complications that tend to ensue embolization procedures tend to be few but post-embolization procedure could occur. Considering that there not enough interventional radiologists in the world that could undertake embolization procedures especially within a number of developing countries, it would be necessary to train more interventional radiologists to undertake intricate procedures like embolization to stop bleeding from the urinary bladder.
Introduction
Intractable visible haematuria from the urinary bladder or prostate gland is known to be a potentially life-threatening event which often raises major treatment challenges. Some of the documented causes of severe haematuria include mainly unresectable urinary bladder carcinoma, radiation cystitis, cyclophosphamide-induced cystitis, transurethral resection of the prostate and prostate cancer. [1] In many patients, the vesical bleeding cannot be adequately controlled by conservative procedures, such as irrigation with formalin, silver nitrate or alum solution, intravesical hydrostatic pressure, hyperbaric oxygen or endoscopic diathermy. [1] [2] [3] The undertaking of radical surgery has not always been possible in view of the fact that the operative risk is high in this type of patient population. Selective angiography and super-selective embolization of the specific bleeding vessel or selective angiography with the undertaking of embolization procedures is a minimally invasive procedure which has emerging as a safe, effective means to control bladder or prostate bleeding and which is being undertaken by few trained interventional radiologists in selected radiology centres in the world. Vesical artery or prostatic artery embolization is occasionally indicated in these patients when all other measures to control the bleeding from the urinary bladder has not been successful. It has been pointed out that despite limited published experience with embolization of the blood supply to the urinary bladder, it had been documented by some authors that the success rate in 90% of patients is the confirm initial success associated when the vesical or prostatic arteries could be identified. [1] [4] [5] [6] [7] [8] [9] [10] Considering that embolization procedures are being carried out in few centres in the world, it would be envisaged that the majority of clinicians in the world would not be familiar with embolization procedures. The ensuing article has provided an update on embolization procedures that had been undertaken so far in the world to stop unresolving visible haematuria.
Aim
To provide an update on embolization to stop persistent bleeding in the form haematuria from the urinary bladder
methods
Internet data bases were searched including: Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: unresolving visible haematuria; intractable haematuria; persistent blood in urine. Fifty-one (51) references were identified which were used to write the article which has been divided into two parts: (A) overview which has discussed various aspects of haematuria in preparation for part (B) that includes miscellaneous narrations and discussion from some case reports, case series, and studies related to embolization of the urinary bladder in an attempt to stop haematuria.
Results
[A] Overview
Haematuria
General Statements / Definition
- Haematuria is a terminology that is used for presence of blood within urine
- Haematuria could be visualized with the eye and this type of blood within the urine is referred to as visible haematuria and visible haematuria has also been referred to as gross haematuria and visible haematuria has at times been referred to as gross haematuria
- Haematuria could also be detected upon testing of urine sample but not visible to sight and this type of haematuria is referred to as non-visible haematuria which is also termed microscopic haematuria
- Microscopic haematuria or non-visible haematuria is diagnosed based upon the finding of greater than (>) 3 red blood cells (RBCs) per high-power field of a non-contaminated sample of urine
- Hematuria could also be divided into (a) glomerular sourced haematuria and (b) non-glomerular cause of haematuria
- It is known that at times what may appear to be haematuria or blood within the urine is not haematuria in that at times myoglobin within urine which is referred to as myoglobinuria due to presence of rhabdomyocytes might simulate haematuria and sometimes bleeding from a non-urinary source for example menstruation in a female might portray to the individual the impression of blood within the urine.
- Hematuria may be associated with pain which is referred to as painful hematuria and this could indicate presence of urinary tract-infection (UTI) or nephrolithiasis or stone within the urinary tract.
- Hematuria could be painless for which the possibility of malignant tumour afflicting the urinary tract or hyperplasia, or a vascular cause would to excluded though a thorough and careful assessment.
- Gross haematuria is suspected when red or brown urine is present. Nevertheless, red or brown urine could also be due to causes other than blood including the following:
- Pigments from medications (for example, phenazopyridine, rifampicin) or foods (for example, beets)
- Metabolites that tend to be associated with other clinical conditions (for example, porphyria)
Some of the common causes of blood within urine.
It is known that blood could be found in the urine of young individuals as in the urine of adults and some of the known common causes of blood in the urine of younger adults and in older individuals has been summated as follows: [11]
- Younger adults [11]
- Urinary tract infection (UTI)
- Nephrolithiasis
- Older adults [11]
- Urinary tract infection (UTI)
- Neoplasm – a neoplastic lesion originating from anywhere in the urinary tract should be excluded
- Benign prostatic hyperplasia (BPH) in adult males.
- Any age group [11]
- Schistosomiasis (Bilharzia) This is the most common cause of haematuria that is found globally and most commonly found in Schistosomiasis endemic areas of the world along the confines of River Nile in areas including Egypt as well as in the confines of the Volta River in West Africa including Ghana
- This is the terminology that is used for manifestation of visible blood at the commencement or initiation of voiding which tends to subsequently clear towards the middle part and at the end of voiding.
- The manifestation of initial haematuria does indicate presence of diseases or source of the bleeding being confined to the urethra.
Types of hematuria that tend to be manifested [11]
- Initial hematuria
- Intervoid hematuria
- This refers to presence of blood between voiding only (voided urine is clear)
- This type of bleeding does indicate lesions within the distal urethra or meatus
- Total hematuria
- Total haematuria is a terminology that is used for presence of visible blood throughout the process of voiding
- This type of blood within urine does indicate the need to exclude disease of the kidneys, ureters, or urinary bladder
- Terminal hematuria
- Terminal haematuria is a terminology that is used for the manifestation of presence of visible blood towards the end of voiding ensuing the initial evidence of clear urine at the commencement of micturition
- Manifestation of terminal haematuria does indicate the bleeding emanating from either the neck of the urinary bladder or the prostatic urethra Gross hematuria
- This type of blood at the end of voiding of urine does suggest the lower urinary tract as the source or cause of the bleeding
- Microscopic hematuria
- Non-visible haematuria has tended to emanate within the kidney as a renal disease
- Presence of brown urine contiguous with red blood cell (RBC) casts and proteinuria indicates glomerular disease
- Clotted blood suggests the source of the clotted blood is below the kidneys
- Brown urine with RBC casts and proteinuria
Blunt Trauma [11] [12]
Kidney injuries – Kidney injuries tend to be manifested contemporaneously in association with the ensuing: [11]
- Sudden deceleration injury without any evidence of visible hematuria
- Visible Hematuria
- Microscopic Hematuria with Shock in association with systolic blood pressure that is less than (SBP<) 90 mm Hg
- The degree of hematuria does not correlate with significance of the kidney injury
Differential Diagnoses of Hematuria
Sources of hematuria [11]
- Urologic (lower tract)
- Any location
- Ureter(s)
- Urinary Bladder
- Prostate Gland
- Urethra
- Glomerular disease
- Non-glomerular disease
- Primary coagulopathy (for example, hemophilia)
- Pharmacological causes including taking of anti-coagulation medicaments
- Sickle cell disease
- Iatrogenic/post-procedure
- Genitourinary tract trauma
- Infection within the urinary tract
- Calculus within the kidney
- Erosion or mechanical obstruction by tumour
- Angiomyolipoma
- Dilatation of stricture
- Transitional cell carcinoma / urothelial carcinoma
- Vascular lesions or malformations
- Chemical or radiation cystitis
- Benign prostatic hypertrophy
- Prostatitis
- A rare sub-type of prostate tumour
- Urethral stricture / urethral stenosis
- Diverticulum of the urethra with or without a foreign body like a stone or at times a rare neoplasm within the diverticulum
- Foreign body
- Endometriosis (cyclic hematuria contemporaneously with menstrual pain)
- Renal (upper urinary tract) sources of Haematuria [11]
- Glomerulonephritis
- IgA nephropathy (Berger disease)
- Lupus nephritis
- Hereditary nephritis (Alport syndrome)
- Toxemia of pregnancy
- Serum sickness
- Erythema multiforme
- Interstitial nephritis
- Pyelonephritis
- Papillary necrosis: due to sickle cell disease, diabetes mellitus, non-steroidal anti-inflammatory drug usage
- Vascular: arteriovenous malformations, emboli, aortocaval fistula
- Malignancy
- Polycystic renal disease
- Medullary sponge disease
- Tuberculosis
- Kidney trauma
- Hematological causes [11]
- Myoglobinuria [11] - positive blood, no red blood cells (RBCs) in the urine: rhabdomyolysis
- Hemoglobinuria [11] - positive blood, no RBCs
- TTP / HUS
- DIC (disseminated intravascular coagulopathy)
- Mechanical valve emergency
- Hemolytic anemia
- Paroxysmal Nocturnal Hemoglobinuria
- Miscellaneous Causes of Haematuria [11]
- Eroding abdominal aortic aneurysm
- Malignant hypertension
- Loin pain–hematuria syndrome
- Renal vein thrombosis
- Exercise-induced hematuria
- Cantharidin (Spanish fly) poisoning
- Stings/bites by insects/reptiles having venom with anticoagulant properties
- Schistosomiasis
- Sickle Cell Trait
- Evaluation
- A full history taking and full general and clinical examination assessment including general examination, systematic examination looking for evidence of pallor, palpable abdominal and loin masses and tenderness, digital rectal examination assessment of the prostate gland, assessing the suprapubic region to exclude a mass or retention of urine as well as careful examination of the penis and external urethral meatus.
- History taking should including a history of past medical history including urinary tract infections, sexually transmitted disease, urethral and urinary tract trauma, presence of a known lesion in the kidney or urinary tract, recent travel abroad or living abroad, swimming in Schistosomiasis endemic area waters, medication history, history of sickle cell disease and any anticoagulant medications.
Macroscopic Hematuria - Approach to the assessment
The ensuing miscellaneous assessments and procedures tend to be undertaken when an adult manifests with visible haematuria:
Laboratory tests
- Urinalysis
- Urine microscopy could demonstrate abnormal RBC morphologies suggesting glomerular source of hematuria
- Microscopic hematuria associated with proteinuria does indicate the possibility of glomerular disease and requires further investigation (as an outpatient)
- There may be evidence in the urine features that may be indicative of urinary tract infection in the sample of urine
- Urine cytology may demonstrate possibility of urothelial neoplasm
- Urine dipstick may be undertaken quickly in some centers but has high false-positive rate [11] [13]
- Urine microscopy and culture – If it does appear as the individual patient might have urinary tract infection, urine specimen would be sent for microscopy and culture examination. In the scenario of Schistosomiasis, the urine specimen would demonstrate evidence of Schistosoma Haematobium during microscopy examination of the urine specimen.
- Full blood count and coagulation screen may be normal but if there is anemia or coagulopathy the results would demonstrate it and it would be investigated thoroughly and appropriate treatment would be provided to improve upon the general condition of the individual.
- Serum urea, creatine, and electrolytes, as well as liver function tests tend to be undertaken and the results would tend to be normal but if there is any abnormality found, it would be carefully assessed and an appropriate treatment would be provided to improve the general condition of the individual
- Serum prostate specific antigen levels tend to be undertaken in the older male group to ascertain the base line serum PSA level and to establish if the level is high to consider the possibility of adenocarcinoma of the prostate gland
Radiology Imaging
- Ultrasound scan of urinary tract: In small district hospitals especially within developing countries where facilities for CT scan or MRI scan are not available, ultrasound sound scan of the renal tract tend to be undertaken initially to ascertain if there is any abnormality within the renal tract and the patient would then be referred to a tertiary hospital for further assessment where CT scan of the urinary tract and pelvis would be undertaken
- Multi-phasic CT urography (hematuria protocol) is usually quickly undertaken to assess for pathology in the kidney and urinary collecting system [11] [14]
- A non-contrast phase is to visualize for stones or hydronephrosis
- A nephrographic phase demonstrates contrast-enhancing kidney parenchyma, which is useful for pyelonephritis and renal tumors
- A delayed excretory phase visualizes for urothelial and urinary bladder tumors
- Ultrasound useful for the assessment to exclude hydronephrosis and an abdominal aortic aneurysm
- Magnetic Resonance Imaging of the renal tract abdomen and pelvis may be undertaken in some specialist centres if the serum PSA is high.
- Flexible cystoscopy and/or kidney biopsies may be necessitated as follow-up procedures after the final disposition
Diagnosis
- The diagnosis tends to be based upon the results of the urine analysis:
- Isolated hematuria with dysmorphic red cells or red cells with a decreased mean corpuscular volume (MCV), would prompt the undertaking of an assessment for glomerulopathy (e.g., IgA nephropathy & Alport’s syndrome) [15]
- Isolated hematuria may be elusive. In some series, more than half of the patients do have non-visible hematuria with no definable cause [15]
Management
- If a cause for the hematuria is found it is then quickly treated
- Visible hematuria
- Visible haematuria is often associated with intra-vesicular blood clot formation and bladder outlet obstruction [11]
- Utilization of a triple-lumen urinary drainage catheter with intermittent or continuous bladder irrigation tends to be undertaken and if there are any blood clots in the urine, bladder wash outs tend to be undertaken to remove the blood clots [11]
- Adequate urinary drainage is always ensured; otherwise, the urologist is then consulted and the patient is then referred to the urology department
Disposition of the patient – (What to do for the patient)
Outpatient [11]
- Outpatient management would tend to be appropriate if the ensuing conditions are met:
- If the individual is hemodynamically stable without life-threatening cause of hematuria
- If the individual is able to tolerate oral fluids, antibiotics, and analgesics as indicated
- If the individual is able to pass or void urine easily
- If there is no significant anemia or no evidence of acute renal insufficiency
Referral Considerations [11]
- In the scenario of the patients being younger than (<) 40 years of age, then it would be recommended that the patients should be referred to the primary care provider for the undertaking of a repeat urine analysis (UA) within 2 weeks
- In the scenario of the patients being older than (>40) years of age with an associated risk factor for the development of urological cancer it would strongly recommend that: the patients should be referred to be seen and assessed by the urologist and the urology team based upon the two week wait urgent cancer referring system (urologist within 2 weeks)
- Some of the two-week wait urology risk factors include the ensuing: [11]
- Risk factors:
- Smoking history
- Occupational exposure to chemicals or dyes
- History of gross hematuria
- Previous urologic history
- History of recurrent UTI
- Analgesic abuse
- History of pelvic irradiation
- Cyclophosphamide utilization
- Pregnancy
- Known malignancy
- Sickle cell disease
- Proteinuria
- Renal insufficiency
- Risk factors:
- It has been recommended that the clinician should consider referring the patients to the nephrology team if there are signs depicting the likelihood and manifesting signs of glomerular hematuria such as concomitant or contemporaneous acute kidney injury (AKI), proteinuria, dysmorphic red blood cells (RBCs), red blood cell casts (RBC casts) [11]
Admission of patients on the same day. [11]
It has been advised that the clinician who has assessed the patients on the day should arrange emergency admission of the patient on the day if the ensuing factors are demonstrated on the day of the assessment(s):
- If the patient has manifested with intractable pain
- If the patient demonstrated evidence of intolerance of oral fluids and medicaments
- If there is clinical assessment of urinary bladder outlet obstruction
- If based upon the results of clinical assessment and laboratory blood and urine test results indicative of suspected or newly diagnosed glomerulonephritis
- If there is evidence of a high risk of the patient developing complications including: pulmonary oedema, volume overload, hypertensive emergency
- Pregnant women (hematuria could be associated with or accompany preeclampsia, pyelonephritis or obstructing nephrolithiasis
Hematuria (peds) https://wikem.org/wiki/Hematuria_(peds)
Haematuria in Children
Even though rare, visible haematuria may on uncommon occasions be experienced by children and the ensuing algorithms had been summated regarding the actions the clinician should take pursuant to the assessment of children who manifest with blood in the urine: [11]
Macroscopic Hematuria algorithm
- The clinician who has assessed children would be reminded that if a child manifests what appears to be visible blood within the urine, the clinician should ascertain or make sure that what appears to be hematuria is not myoglobin (for example, 2/2 rhabdomyolysis) or bleeding from a non-urinary source
- The clinician needs to have a high suspicion for rhabdomyolysis, which is the end result of or an emanation of any disease process which causes muscle cell (myocyte) lysis.
- Every clinician who assesses children who manifest with what appears to be haematuria or rhabdomyolysis should realise that rhabdomyolysis may have an obvious manifestation, such as traumatic 'crush' injury, or the presentation may be insidious, requiring a high clinical index of suspicion.
- The clinician needs to be aware that muscular pain or discomfort is common, but rhabdomyolysis could be associated with no symptoms or physical signs based upon clinical examination of the children.
- Diagnosis of rhabdomyolysis tends to be confirmed based upon the finding of elevated serum creatine kinase level in the patient’s biochemistry blood test results
- Fluid hydration is the mainstay of therapy for rhabdomyolysis
Definition of rhabdomyolysis
The ensuing brief summations had been made about rhabdomyolysis to remind every clinician who assesses children for the possibility of visible haematuria to enable every clinician to have a high index of suspicion to exclude rhabdomyolysis:
- Rhabdomyolysis may ensue any traumatic or medical injury to the sarcolemma (the myocyte cell membrane) of the skeletal muscle cells.
- The subsequent release of intracellular ions, myoglobin, creatine kinase (CK), and urates into the circulation results in electrolyte disturbances, acidaemia, disseminated intravascular coagulation, acute kidney injury (AKI), and multi-organ failure.
- The measurement of serum CK levels at more than 5 times the upper limit of normal or >1000 IU/L is utilised as a diagnostic criterion [17] [18] [19]
Common Causes of Haematuria in the Paediatric Age Group
In order that a clinician who assesses children could be aware of the common causes of haematuria in children, the common causes of blood in urine of children had been summated as follows: [16]
- Pediatric patients with haematuria could have any of these: [16]
- Glomerulonephritis
- Urinary Tract Infection (UTI)
- Congenital urinary tract abnormality
- Younger adults
- UTI
- Nephrolithiasis
- Any age
- Schistosomiasis (This condition is stated to be the most common cause of haematuria globally [16] This would be quite common in Schistosomiasis endemic areas of the world including areas around River Nile and Egypt and the Volta River in West Africa including Ghana)
Clinical Manifesting Features of Haematuria in the Paediatric age group
Types of hematuria
- Initial hematuria
- Blood at beginning of micturition with subsequent clearing
- Suggests urethral disease
- Intervoid hematuria
- Blood between voiding only (voided urine is clear)
- Suggests lesions at distal urethra or meatus
- Total hematuria
- Blood visible throughout micturition
- Suggests disease of kidneys, ureters, or bladder
- Terminal hematuria
- Blood seen at end of micturition after initial voiding of clear urine
- Suggests disease at bladder neck or prostatic urethra
- Gross hematuria
- Indicates lower tract cause
- Microscopic hematuria
- Tends to occur with kidney disease
- Brown urine with RBC casts and proteinuria
- Suggests glomerular source
- Clotted blood
- Indicates source below kidneys
Differential Diagnoses of Haematuria in the Paediatric Age Group. [16]
Pediatric Haematuria
Macroscopic Hematuria | Transient Microhematuria | Persistent Microhematuria |
Blunt abdominal trauma | Strenuous exercise | Benign familial haematuria |
Urinary tract infection | Congenital anomalies | Idiopathic hypercalciuria |
Nephrolithiasis | Trauma | Immunoglobulin A nephropathy |
Infections | Menstruation | |
Post streptococcal glomerulonephritis | Bladder catheterization | Alport syndrome |
High fever | Sickle cell trait or anaemia | |
Immunoglobulin A nephropathy | Henoch-Schonlein purpura | |
Hypercalciuria | Drugs and toxins | |
Sickle cell disease | Lupus nephritis |
Attribution License.
Look-Alikes (Conditions that simulate haematuria)Table 1: Reproduced from: [16] Under the Creative Commo
Conditions that simulate haematuria had been summated as follows: [16]
- Foods or medications
- For example, beets, rifampin, multivitamins, pyridium
- Uric acid crystalluria
- Gastrointestinal bleeding in children (peds)
- Vaginal bleeding
- Pre-pubertal vaginal bleeding
- Other causes of abnormally coloured urine
Evaluation
- Urinalysis
Management
- Treatment of blood in the urine in children does dependent upon finding the cause of the bleeding and treating the cause of the bleeding appropriately [16]
Disposition
- Dependent on cause – What the clinician does following full assessment of children who manifest with blood in urine depends upon the cause of the bleeding which the clinician finds. [16]
[B] Miscellaneous Narrations and Discussions from Some Case Reports, Case Series, And Studies Related to Angiography and Embolization to Stop Incessant Unresolving Haematuria
Loffroy et al. [1] made the ensuing iterations:
- Intractable hematuria from the urinary bladder or the prostate gland could be life-threatening and its management has remained to be a difficult clinical problem.
- Severe bleeding could arise as a result of radiation cystitis, carcinoma of the urinary, cyclophosphamide-induced cystitis, severe infection, transurethral resection of the prostate and prostate cancer.
- When irrigation of the urinary bladder through a three-way catheter and fulguration of the bleeding lesions fail to stop the hematuria, a life-threatening situation could develop, when blood transfusion fails to keep pace with the rate of blood loss.
- Patients who have massive uncontrollable hematuria are often elderly and unfit to undergo cystectomy as a treatment.
- Many urologists had had to manage this difficult problem, and many different treatments had been attempted and described, with varying degrees of success.
- Transcatheter arterial embolization of the vesical or prostatic arteries is occasionally indicated in these patients when all other measures have failed.
- There is limited published experience with this procedure, but success in 90% of patients had been reported when the vesical or prostatic arteries could be identified.
Tsitskari et al. [20] evaluated the feasibility, safety and long-term efficacy of super-selective trans-catheter arterial embolization for the management of intractable bladder bleeding. Tsitskari et al. [20] retrospectively analysed the records of 20 patients with intractable haematuria who had been referred urgently for selective arterial embolization after failed conventional therapy, between 2013 and 2018. They iterated that the primary outcomes were technical (cessation of extravasation and/or stasis of flow within the target vessel) and clinical (bleeding control) success. Secondary outcomes included complication and re-intervention rates. Tsitskari et al. [20] summated the results of their study as follows:
- Technical success was 90% which amounted to 18 cases out of 20 cases, as in 2 cases, embolization was not feasible.
- Super-selective embolization of the vesical arteries was feasible in 15 out of 18 cases which amounted to in 83.3% of the cases.
- Selective proximal occlusion of the anterior division of the internal iliac artery was undertaken in two cases which amounted to 11% of the cases and embolization of the anterior division after coil blockage of the posterior division was undertaken in one case which amounted to in 5% of the case.
- Bilateral and unilateral embolization was undertaken in 10 and 8 cases, respectively.
- The peri-procedural mortality rate was 5% which amounted to 1 patient out of 18 patients.
- One possible procedure-related death had occurred due to myocardial infarction ten days pursuant to the undertaking of non-target embolization of the buttocks and the anterior abdominal wall.
- The mean time follow up was 35 ± 15 months.
- Bleeding had reoccurred in three patients, which amounted to in 16.6% of the patients, all of them were successfully managed, one conservatively and two with further embolization.
- The clinical success of the embolization procedure was 85% which accounted for 17 cases out of 20 cases.
- During follow up 11 more patients died, due to underlying conditions that were not related to bleeding or the embolization procedure.
Tsitskari et al. [20] concluded that:
- Super-selective angiographic embolization is feasible, safe and effective to control refractory, life threatening bladder bleeding and should be considered as a first line treatment, as to obviate the need for emergency surgery.
Tsitskari et al. [20] provided a detailed summation of their study and background educative iterations and findings as follows:
- Intractable haematuria is a severe, as well as life-threatening condition.
- It may have a host of causes such as an underlying malignancy mainly prostate and bladder cancer, inflammatory causes or radiation and drug induced cystitis. [21]
- The majority of cases of urinary bladder and prostate gland haematuria are managed conservatively by irrigation with formalin, silver nitrate or alum solution, intra-vesical hydrostatic pressure, hyperbaric oxygen or endoscopic diathermy.
- Urinary bladder lesion resection with urinary diversion had traditionally been applied in cases in which conservative treatment had failed. [2]
- The majority of patients with intractable haematuria are of high surgical risk due to advanced age, various comorbidities and poor clinical status.
- Over the preceding decade percutaneous, trans-catheter, arterial embolization had been proposed as an attractive, minimal invasive, alternative treatment for patients suffering from bladder haematuria not responding to conventional, non-invasive treatment.
- Nonetheless, data regarding the safety and efficacy of the method had remain scarce. [1]
- They sought to assess the feasibility, safety and long-term efficacy of super-selective, trans-catheter, embolization of the vesical arteries for the management of intractable bladder haematuria in our institution.
Tsitskari et al. [20] undertook a retrospective study not requiring approval by the Hospital’s Ethics and Scientific Committee. The potential risks and benefits were explained and informed consent was obtained from all individual participants who were included in the study. Records of all the patients who were referred to the Interventional Radiology department for the management of intractable haematuria between 2013 and 2018, were retrospectively reviewed. Tsitskari et al. [20] iterated that in their institution, percutaneous embolization, was usually the preferred method of treatment for patients with haematuria non responsive to conservative measures due to its minimal invasiveness compared to surgical management. In total 20 patients which included 18 men that amounted 90% of the patients; whose mean age was 76 ± 4 years, who were treated with percutaneous trans-catheter arterial embolization were included in their study. The decision to undertake trans-catheter embolization was based upon clinical and laboratory evidence of continued bleeding despite adequate conventional therapy. The majority of the patients were noted to be hemodynamically stable and they were treated on an urgent basis. One patient had developed massive haematuria as well as hemodynamic instability while being treated conservatively and the patient was referred for embolization in the emergency setting. All the embolization procedures were undertaken under local anaesthesia, after obtaining right common femoral artery access via a 6-Fr vascular sheath. Initially pelvic angiography was undertaken utilising a 5 F pigtail catheter to delineate the pelvic arterial anatomy. Selective catheterization and angiography of the internal iliac arteries was then undertaken utilising a Tempo Aqua catheter (Cordis Europa N. V, Roden, The Netherlands) or a Sim 1 hydrophilic catheter (Progreat, Terumo Europe NV, Leuven, Belgium). Subsequently, the anterior division of the iliac artery was selectively catheterized and digital subtraction angiography (DSA) was undertaken (bilaterally) to adequately visualize vesical branches and demonstrate any pathological vascularity of the urinary bladder and/or a site of active extravasation. Based upon the angiographic findings super-selective catheterization of the vesical artery was undertaken utilising a 2.7Fr coaxial micro-catheter (Progreat®, Terumo Europe NV, Leuven, Belgium). Flow directed embolization was undertaken utilising microspheres or glue or both. When the main distal branches of the anterior division of the internal iliac artery could not be catheterized super-selectively, the catheter tip was left in the anterior division and embolization was then undertaken from that point using gelfoam or microspheres. The aim was bilateral, super-selective, embolization of the vesical arteries until stasis was achieved even if a clear bleeding site was not identified. Unilateral embolization was preferred only in cases in which selective DSA had identified an active extravasation from a specific terminal arteriole or the presence of a rather focalized than diffuse vascular pathology, or in cases where bilateral catheterization was not possible. With regard to definitions, outcomes, and follow-up assessment procedures, Tsitskari et al. [20] made the ensuing iterations:
- All study outcome measures were defined according to the SIR reporting standards. [22]
- The primary outcome measures included the ensuing: a. technical success defined as cessation of extravasation and/or stasis of flow within the target vessel on post-embolization DSA and b. clinical success defined as the resolution of signs or symptoms that prompted the embolization throughout the follow up period, without the occurrence of major complications.
- The secondary endpoints had included super-selective target vesical artery catheterization and embolization rates, procedure-related major and minor complication rates and re-intervention rates defined as the rate of additional embolization or open surgical procedures due to recurrence of haematuria.
- Follow up was assessed by the reviewing of the medical records of all patients and by telephone interview in case of missing data.
Tsitskari et al. [20] summated the results as follows:
- During the study period a total of 22 angiography procedures were undertaken (including re-interventions) for embolization of severe intractable bladder haematuria in 20 patients.
- The majority of the patients were adjudged to be at high operative risk due to advanced age and comorbidities as the underlying pathology was urinary bladder cancer (n = 16 patients), prostate cancer (n = 1), metastatic osteosarcoma of the urinary bladder (n = 1) and post irradiation cystitis (n = 2).
- The angiography findings included diffuse increased pelvic vascularity/neovascularity in 15 cases, active extravasation in two patients and localized hyper-vascular mass-like lesion in three patients.
- In one of the three patients who had mass-like lesions the presence of an AVF was also demonstrated.
- The technical success was 90% which accounted for in 18 cases out of 20 cases, as in 2 cases out of 20 cases which amounted to in 10% of the cases, embolization was found not to be technically feasible. In one patient catheterization of the internal iliac arteries was not achieved pursuant to many attempts due to severe atherosclerosis and tortuosity of the iliac arteries, while in the second case catheterization was not possible due to altered vascular anatomy following previous prostatectomy and partial bladder resection, which did not enable safe embolization. Both patients were managed conservatively and they died after 1 month and 2 months respectively.
- Super-selective distal embolization of the vesical arteries was undertaken in 15 out of 18 cases which amounted to in 83.3% of the cases using PVA foam particles (see figure 1) ranging from 100 to 500 μm (Cook Medical, UK) or PVA hydrogel particles ranging from 300 to 700 μm (Bead Block; Terumo Europe NV, Leuven, Belgium) or glue (GLUEBRAN®2,GEM S.r.l, LU,Italy) (see figure 2), or a combination of particles and glue.
- In 3 out of 18 patients which amounted to in 16.6% of the patients who had undergone trans-catheter embolization, super-selective catheterization of the vesical arteries was not feasible. Selective proximal Gelfoam sponge embolization of the anterior division of the internal iliac artery was undertaken in 2 out of these 3 patients while in one patient selective particle embolization was undertaken after coil protection of the posterior division.
- Embolization was undertaken bilaterally in 10 out of 18 patients which amounted to in 55.5% of the patients and unilaterally in 8 patients out of 18 patients which amounted to in 44.43% of the patients based upon the angiography imaging findings and technical feasibility. In 3 patients, bilateral embolization was desirable but not possible.
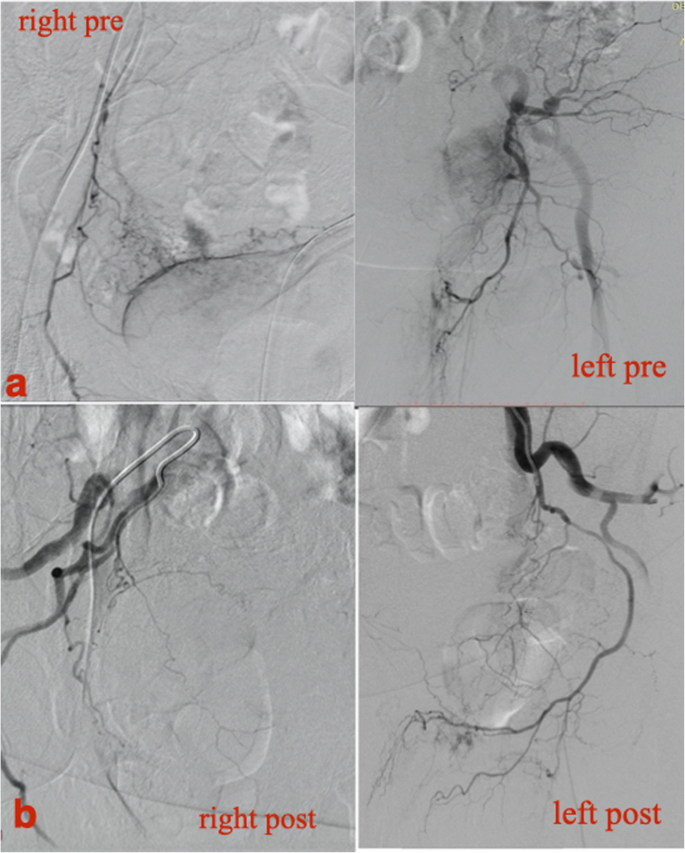
Figure. 1
Haemodynamically unstable 72-year-old, male patient with inoperable urinary bladder carcinoma and multiple episodes of haematuria not responding to conventional therapy. a. Selective DSA from the anterior division of the IIA bilaterally, demonstrating pathologic vascularity of the bladder. b Final DSA following micro-particle embolization (500-700 μm) demonstrating almost complete devascularization of the bladder. Patient remained asymptomatic without clinical relapse. Reproduced from: [20] under the CFigure. 2
Commons Attribution License.
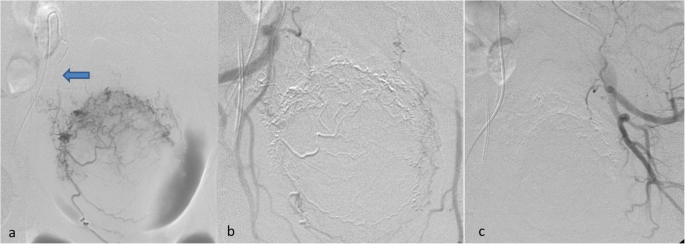
Figure. 2
responding to conventional therapy. a Super-selective DSA with a micro-catheter within the right superior vesical artery (blue arrow) demonstrating pathologic vascularization of the bladder. b and c DSA following bilateral superior vesical artery glue embolization demonstrating complete devascularisation of the bladder. No bleeding relapse occurred. Reproduced from: [20] Under the Creative Commons Attribution License.
- The mean follow-up period was 35 ± 15 months.
- The clinical success rate was 85% which amounted to success in 17 out of 20 cases, as there was one procedure-related death which occurred in 1 out of 18 patients which amounted to in 5% of the cases following the undertaking of non- target embolization of the buttocks and the anterior abdominal wall after proximal embolization of the anterior division of the internal iliac artery using embolic microspheres of 40 μm (Embospheres, Merit Medical Systems, Inc.) and coil embolization (Nester, Cook Medical) for the preservation of the posterior IIA division (see figure 3). This patient had developed ischemic changes at the anterior abdominal wall and buttock area (see figure 3) and died due to myocardial infarction 10 days subsequently.
- Bleeding recurrence was identified in 3 cases out of 18 cases, which amounted to 16.6% of the cases.
- In one patient re-bleeding had occurred 5 hours ensuing the initial embolization procedure and was controlled by repeated super-selective embolization.
- In the remaining two patients re-bleeding had developed 35 days and 43 days pursuant to the undertaking of the initial embolization procedure. One was successfully managed conservatively and the other with successful repeat super-selective embolization.
- During the follow up period 11 more patients died. Two of these patients died due to heart disease, one due to pulmonary embolism, one due to stroke and seven due to the underlying malignancy.
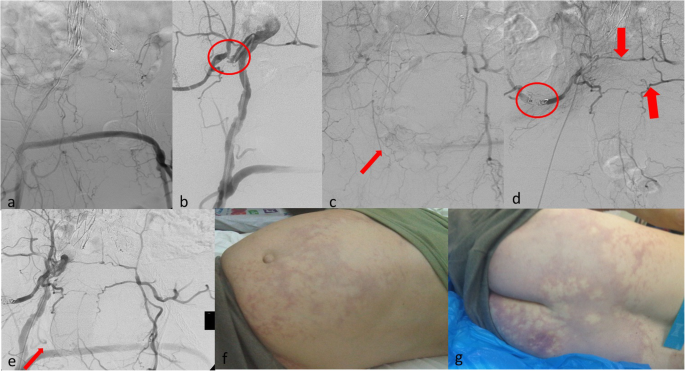
Figure. 3
Haemodynamically unstable 61-year-old male patient with history of inoperable bladder cancer, radiotherapy previous EVAR, fem-fem bypass graft and intractable haematuria not responding to any conservative method. a DSA depicting previous unilateral EVAR and extra-anatomic fem-fem bypass. b Selective catheterization of the right internal iliac artery (IIA) demonstrating a significant stenosis of its origin (circle). c DSA with the catheter at the origin of the IIA demonstrating a blush of contrast at the site of bleeding (arrow). d: As the anterior division of the IIA could not be selectively catheterized, protective coil embolization of the posterior division (circle) and life-saving particle embolization (40 μm for better penetration) from the origin of the IIA was performed. Note the anastomosis between the right and the left middle and lateral sacral arteries (arrows). e After the delivery of 1 vial of micro-particles no blush was evident (arrow). f and g 30 mins after embolization the patient developed severe pain and marked ischemia of the buttock and the anterior abdominal wall. He was managed by the anaesthesiology team and died of myocardial infarction 10 days after index procedure. Reproduced from: [20] Under the Creative Commons Attribution License.
- Minor complications were identified in 2 out of 18 cases which amounted to in 11% of the cases as two patients had experienced post embolization syndrome, which was managed conservatively only with analgesics and antipyretics and resolved within 10 days.
Tsitskari et al. [20] made the ensuing educative summating discussions:
- Refractory urinary bladder haemorrhage represents a major clinical problem which is treated upon an emergency basis.
- According to the literature, a variety of conservative measures that available for utilization had resulted in a response rate which had ranged from 50% to 100% [2] [21]
- Surgical treatment is associated with high morbidity and mortality in view of the fact that the majority of these patients suffer from serious comorbidities.
- Percutaneous, trans-catheter, arterial, embolization (TAE) is an alternative, minimally invasive treatment option which is associated with good results and a lower complication rate when compared to conventional surgical approach. [1]
- Review of the literature had revealed only few small case series or sporadic case reports which had reported results from endovascular embolization for severe haematuria. Most of these studies had supported the safety and efficacy of the technique in short and mid-term follow up and had presented a low complication rate. [1]
- Their presented outcomes had demonstrated that super-selective, vesical artery TAE is feasible in the majority of the cases and had achieved very satisfactory long-term clinical success rates of 85%.
- Rebleeding represents the weak point of the method and in their series rebleeding was encountered in 3 out of 18 patients which amounted to in 16% of the patients.
- Their results were in keeping with the lower reported rates which had ranged between 10% to 28%. [10]
- Earlier studies had described mainly non-selective unilateral internal artery embolization, which was associated with high complication and re-bleeding rate. [23] [24] [25]
- Overall, they had treated 10 patients that amounted to 55.5% of the patients with bilateral super-selective embolization of the vesical arteries and only one of these patients that amounted to 10% of the patients had suffered bleeding recurrence, 5 hours subsequently ensuing the initial TAE. As a result, the patient underwent second bilateral super-selective TAE using microspheres with successful clinical outcome. On the contrary 8 patients underwent unilateral embolization and rebleeding was noticed in 2 patients which amounted to in 25% of the patients, at 35 days and 43 days respectively, following the initial treatment. One was managed conservatively and one with further unilateral embolization of the same vessel. Bilateral approach seemed to have decreased the rate of early re-bleeding which is attributed to the rich collateral blood supply to the internal iliac artery. [9] [23] [24] [26] [27]
- They do argue that bilateral embolization might lead to more durable response even though it is hard to support it due to lack of technique standardization and the small number of patients treated.
- Super-selective embolization appeared to be associated with fewer complications. [24] [25] Delgal et al. [10] reported the safety and efficacy of super-selective embolization with particles in 11 patients. [10]
- They had also undertaken super-selective embolization with particles or glue or a combination of both without complications. The sole major complication in their case series that was encountered following TAE from the orifice IIA anterior division using microspheres after coil blockage of the posterior division. Selective distal catheterization of the anterior division was not feasible due to severe stenosis in its proximity. Few hours later the patient developed severe pain from gluteal and anterior abdominal wall necrosis. He died ten days later due to myocardial infarction. On a retrospect, this patient had a history of peripheral arterial disease, previous endovascular aortic aneurysm repair and fem-fem bypass, with a rich collateral network due to the underlying severe atherosclerosis that was over looked. Moreover, small sized particles of 40 μm were utilised aiming for better penetration. All the above had contributed to this disastrous complication could definitely be prevented if the angiographic findings were cautiously evaluated. The use of 300- to 500 μm particles would have certainly been a better choice, as it has been reported to decrease the complication rate given a lower risk of non-targeted embolization and/or tissue devascularisation. Surgery was not an option for this patient due to severe comorbidities.
- The use of different embolization materials had been reported like coils, glue, particles, alcohol and gelfoam without any actual benefit of a specific agent over another. Most of the authors had utilised particles regardless the selectivity of embolization. [10] [23]
- In the majority of the cases, they utilised particles, glue or a combination of both. There had been only few reports of embolization with utilization of cyanoacrylate glue in the literature. Delgal, et al., reported cyanoacrylate glue embolization of the feeding branch in patients with angiographic evidence of contrast extravasation. In this study, n-butyl-2-cyanocrylate glue mixed with ultra-fluid lipiodol (1:3 ratio) was used, alone or in combination with other embolic agents in 7 patients, regardless of the angiographic findings. There were no complications observed associated with the use of glue.
- Based upon the literature and the author’s opinion, bilateral super-selective approach, when possible, seemed to be the desired treatment option when no site of active bleeding is identified. Nevertheless, definite conclusions about the best technique and embolization agent to optimize the technique efficiency cannot be drawn yet. Unilateral embolization could be efficient in selected cases, especially when angiography demonstrates bleeding from a terminal arteriole or a focalized hypervascularity rather than diffuse disease. [10] An attempt to embolize one of the vesical arteries or even branches of the IIA should be made, as flow reduction could sometimes suffice as to stop the bleeding or incite clinical improvement.
- Limitations of their study included an inherent external validity bias, the small number of patients they had investigated due to the single-centre design and the lack of technique standardization. Moreover, the limited number of subjects that were included did not enable sub-group analysis as to identify possible factors influencing outcomes such as clinical presentation, embolic material, bilateral versus unilateral embolization etc. Finally, as this was a retrospective study some cases might have not been identified.
Tsitskari et al. [20] made the ensuing conclusions:
- Conclusively, according to the retrospective study, palliative, super-selective TAE was proven feasible, safe and effective in controlling refractory bladder bleeding.
- It is a life-saving procedure, less-invasive than surgery, which resulted in very satisfactory technical success, peri-procedural morbidity and mortality rates, as well as sustained long-term control of haematuria with low re-bleeding rates.
- The procedure should be considered as an alternative treatment option in selected patients not responding to conservative treatment, as to obviate the need for surgery.
- Nevertheless, as data in then literature had remained limited, further prospective comparative studies are needed in order to validate these results.
Taha et al. [28] undertook a study to establish the current evidence and assess the effectiveness and safety of selective trans-arterial embolization (STE) to control intractable bladder haemorrhage (IBH). Due to the rise in utilisation of STE in the treatment of IBH, Taha et al. [28] undertook a systematic review according to the Cochrane reviews guidelines and in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. Taha et al. [28] searched the literature which yielded 38 studies, of which 11 were excluded because of irrelevance of data. All included studies were observational cohort studies, with no randomisation or control groups apart from in relation to the materials used for embolization. The studies had been published between 1978 and 2016. There were 295 patients with an age range between 51 years and 95 years. The success rate had ranged from 43% up to 100%. The most reported complication was post-embolization syndrome, even though other complications were described such as mild transient gluteal claudication, nausea, and vomiting. Taha et al. [28] concluded that STE of the internal iliac artery is a safe and effective alternative technique to control severe IBH, and had been successfully applied over many years to treat urinary bladder haemorrhage associated with terminal pelvic malignancy.
Prasad et al. [27] used the patient characteristics, techniques used, and outcomes of 11 patients with lower urinary tract haemorrhage, who were treated with embolotherapy which they had summated on. The authors had focused upon bilateral super-selective embolization of the arterial supply to the urinary bladder and techniques to embolize multiple small vessels supplying the urinary bladder when the vascular anatomy was complicated and super-selective catheterization was not possible. The immediate success rate was 100%, with three later recurrences. One procedure was complicated by asymptomatic occlusion of the posterior division of the internal iliac artery. Prasad et al. {27] concluded that:
- Embolotherapy could provide at least short-term success adequate to improve quality of life for palliation with few complications.
Chen et al. [29] explored the effect of transcatheter arterial embolization (TAE) in controlling intractable, nontraumatic bladder haemorrhage in cancer patients. Chen et al. [29] undertook a literature review (PubMed and EMBASE), which was followed by a retrospective analysis of all cancer patients who had intractable haematuria from urinary bladder which were treated by TAE within their tertiary referral centre. Chen et al. [29] summated the results as follows:
- Within their institution, they had identified 27 consecutive cancer patients who underwent TAE for refractory visible haematuria from the urinary bladder.
- The systematic review had included 13 studies which had been published between 1981 and 2019.
- Within their local cohort, 27 patients were treated with 100% technical success, clinical success in 88.9%, no major complications, and rebleeding rate within the first month of 7.4%.
- In the systematic review cohort of 201 patients, there was technical success reported in 99.0%, clinical success in 80.9%, major complications in 5.5%, and a rebleeding rate within the first month of 4.5%. Bilateral embolization was undertaken in 81.1%, and embolization levels were mostly anterior division of internal iliac artery (73.7%) and vesical artery (23.2%).
Chen et al. [29] made the ensuing conclusions:
- TAE is effective and safe to control intractable haematuria from urinary bladder origin in cancer patients following failure of conservative management, providing effective temporary haemostasis.
Chen et al. [29] made the ensuing conclusions:
- For urinary bladder haemorrhage which is not suitable for surgery, TAE should be considered at an early stage.
- A literature review, followed by the undertaking of a retrospective analysis of all patients with intractable haematuria emanating from the urinary bladder which were treated by transcatheter arterial embolization within their tertiary referral centre, had demonstrated that trans-catheter arterial embolization is effective and safe to control intractable haematuria from the bladder.
- The major complication rate and rebleeding within the first month are acceptable.
Debernadinis et al. [30] made the ensuing iterations:
- Urinary bladder haemorrhage following radiotherapy is a serious complication in patients undergoing this treatment.
- Many methods had been proposed to control this particular situation; nevertheless, the results had been far from satisfactory, with the exception of drastic measures such as hypogastric artery ligation and radical cystectomy.
Debernadinis et al. [30] had recently used a method of super-selective embolization of the urinary bladder arteries which had enabled them to control severe intractable bleeding in a patient who was submitted to bladder radiotherapy for a transitional cell infiltrating carcinoma. Debernadinis et al. et al. [30] made the ensuing educative discussive iterations:
- Compared to selective embolization and other methods, the advantages of super-selective embolization include: a lower recurrence rate concerning bleeding, fewer side-effects and the possibility of using adaptable embospheres (150-1000 micron) which, on account of their marked plasticity, provide better occlusion of the vessels.
- For these reasons, super-selective embolization of the bladder arteries should be considered as the treatment of choice in intractable bladder haemorrhage.
Mohan et al. [31] evaluated the efficacy and outcome of super-selective vesical arterial embolization in the management of severe intractable haematuria secondary to haemorrhagic cystitis. Mohan et al. [31] retrospectively reviewed the medical records of nine patients with severe intractable haematuria who were treated with super-selective vesical artery embolization within their institution between March 2003 and February 2015. They summated the procedures of the patients as follows:
- There were six males and three females with a mean age of 56.1 years.
- Seven patients had transitional cell carcinoma (TCC) of urinary bladder and they had undergone transurethral resection of urinary bladder tumour and pelvic radiotherapy.
- One patient had synchronous renal pelvis and bladder TCC.
- One patient had aorto-arteritis and was receiving cyclophosphamide therapy and another patient had carcinoma cervix post-pelvic radiotherapy.
- Following the failure of conservative management, super-selective vesical artery catheterization and embolization was undertaken with 300-500-μ PVA particles in all patients. Coil embolization of inferior gluteal artery followed by particle embolization of vesical arteries was undertaken in one patient in whom superior, inferior vesical and inferior gluteal arteries were arising as a trifurcation.
Mohan et al. [31] summated the results as follows:
- The technical success rate was 100% with complete cessation of haematuria within 48 hours in all patients.
- No significant complications were identified, except for post-embolization syndrome in one patient, which had improved upon symptomatic treatment.
- During a mean follow-up period of 14.45 months and a follow-up which had ranged from 3 months to 28 months, one patient had mild recurrent haematuria at 2 months, which had resolved spontaneously.
Mohan et al. [31] made the ensuing conclusions:
- Super-selective vesical artery embolization is a safe and effective procedure in controlling intractable life-threatening haematuria in a select group of patients who have failed conventional treatment protocols.
- This procedure might be considered to be the treatment of choice since it usually obviates the need for the undertaking of emergency surgery in these severely ill patients.
Zhou et al. [32] evaluated the safety and efficacy of super-selective vesical artery embolization (SVAE) in the treatment of intractable haemorrhagic cystitis (HC) following hematopoietic stem cell transplantation (HSCT). Zhou et al. [32] retrospectively reviewed from January 2010 to December 2018, 26 patients with haematological malignant tumours who underwent SVAE for treatment of intractable HC following HSCT. Zhou et al. [32] reported that SVAE was undertaken with 300-500 μm gelatin-sponge particles initially. Zhou et al. [32] defined technical success as achieving bilateral SVAE for all the prominent vesical arteries. Zhou et al. [32] defined therapeutic efficacy as: Complete response (CR): macroscopic haematuria had completely disappeared on more than 2 consecutive days after SVAE; Partial response (PR): macroscopic haematuria had reduced after SVAE or briefly disappeared after SVAE but reappeared soon within 2 days; No response: no response to SVAE or haematuria which had been aggravated after the SVAE; Recurrence, was defined as macroscopic haematuria had relapsed on follow-up after achieving an initial CR. Zhou et al. [32] also registered the adverse events were also registered. Zhou et al. [32] summated the results as follows:
- There was a mean follow-up of 11.4 months and the follow-up had ranged between 0.5 months and 83.7 months.
- The mean interval for the onset of HC after HSCT was 39.7 ± 19.0 days, and mean duration of the haematuria before embolization was 14.9 ± 15.7 days.
- SVAE was found to be technically successful in all patients.
- Pursuant to the embolization, visible haematuria had regressed within 48 hours for all patients.
- The mean urine erythrocyte counts had dropped from 14,213.2 ± 20,999.0/uL before SVAE to 6072.9 ± 12,720.7/uL on 3d after SVAE (P = 0.002) and 3720.2 ± 8988.9/uL on 7 d after SVAE (P = 0.001), respectively.
- The haematuria had completely disappeared prior to discharge of the patients in 23 patients which amounted to in 88.5% of the patients, including 20 with one embolization and 3 with 2 embolization procedures and remaining 3 patients had PR.
- No major procedure-related complications were identified except for post-embolization syndrome in 8 patients, which had resolved with symptomatic treatment.
- On follow-up monthly, recurrence of haematuria was identified in 4 out of 23 patients which amounted to in 17.4% of the cases and these were managed conservatively in 2 patients and with repeat embolization in the remaining 2 patients.
Kim et al. [33] stated that intractable urinary bladder haemorrhage from pelvic malignancy could be potentially life-threatening and its management could be a challenging clinical problem. Kim et al. [33] evaluated the safety, efficacy, and clinical outcome of super-selective vesical artery embolization for the control of intractable urinary bladder haemorrhage from pelvic malignancy. Kim et al. [33] reported that between January 2010 and September 2018, 20 patients had undergone super-selective vesical artery embolization for intractable visible haematuria secondary to pelvic malignancy arising from or invading the bladder. Kim et al. [33] obtained the treatment details and clinical outcomes of the patients. Kim et al. [33] summated the results as follows:
- There were 12 men and 8 women whose mean age was 77 years.
- Bilateral embolization was undertaken in 10 patients and unilateral approach in 10 patients.
- Two patients died within four days ensuing the embolization due to underlying heart failure and systemic metastasis, respectively.
- The remaining 18 patients had a follow-up of longer than 30 days. Bleeding was controlled pursuant to the first embolization procedure in 17 out of 18 patients and after a repeat embolization in the remaining one patient.
- The mean follow-up period of 18 patients was 10.6 months (range = 1-77 months).
- Late recurrent haemorrhage lasting for 30 days or longer than 30 days after the embolization procedure was reported in 6 patients which amounted to in 33.3% of the patients. Five of these six patients underwent repeat embolization.
- There were no major complications related to the embolization.
Kim et al. [33] concluded that:
Palliative super-selective vesical artery embolization is a feasible, effective, and safe procedure to control intractable haematuria in patients who have pelvic malignancy.
Rodríguez-Patrón Rodríguez et al. [34] made the ensuing iterations:
- Bleeding secondary to severe vesical--prostatic pathology (mainly neoplastic disease and radiation cystitis) might be a serious clinical management problem due to its morbidity and associated increased resources demand in the form of admissions, transfusions and other measures.
- They had reviewed a series of patients who were embolized for this purpose, its efficacy, tolerability and adverse events.
Rodríguez-Patrón Rodríguez et al. [34] summated the patients and procedures as follows:
- They had reviewed 8 patients who had undergone hypogastric arteries embolization between July 1998 and December 2001, analysing the indications, efficacy and duration, tolerability, and consequences.
- Right femoral artery access was undertaken in all except one case that needed bilateral femoral accesses.
- Embolization was achieved by means of coils and particles. All procedures were performed under local anaesthesia.
Rodríguez-Patrón Rodríguez et al. [34] summated the results as follows:
- Nine (9) procedures were undertaken in 8 patients. 3 patients had manifested with visible haematuria due to radiation cystitis, 3 from prostatic carcinoma, and 2 with urethrorragy from urethral relapses after cystectomy.
- Seven out of nine (7/9) embolization procedures were effective in achieving immediate complete or almost complete bleeding control; in one case control was partial; another one had limited or no effect.
- Selective embolization of distal arteries was undertaken in 3 cases; all the remaining patients underwent direct hypogastric trunk embolization sparing the superior gluteal artery.
- Effect lasted between 1 month and 31 months. 4 patients died, 3 of them without haematuria, 1 because of an intercurrent disease, and the others from disease progression. 2 patients underwent posterior surgery, one due to recurrent haematuria, and the other, a case of urethral tumour, due to partial failure; partial cystectomy and urethrectomy were performed respectively. 2 patients needed administration of morphic derivatives after embolization, all the others were managed with magnesium metamizol. Only one patient was referred with mild transitory gluteal claudication.
Rodríguez-Patrón Rodríguez et al. [34] concluded that:
Percutaneous arterial embolization is an effective instrument to treat patients with haematuria or urethrorragy and severe lower urinary tract pathology in whom curative treatments are not applicable due to their general status, life expectancy, or tumour status.
Liguori et al. [23] determined the feasibility and efficacy of trans-arterial embolization (TAE) in haemorrhagic urological emergencies, and they assessed the perioperative morbidity, effect of timing of intervention on the requirement for blood transfusion, and the long-term follow-up. Liguori et al. [23] reported that between October 1997 and March 2009, 44 patients (30 men and 14 women; whose mean age was 79 years, and whose ages had ranged between 51 years 95 years with intractable haematuria secondary to advanced pelvic tumour arising from or invading the urinary bladder, who underwent internal iliac TAE. Twenty-four patients had transitional carcinoma of the urinary bladder, 12 had adenocarcinoma of the prostate gland, five patients had carcinoma of the uterus, one patient had cancer of the vagina, two patients had carcinoma of the rectum, three patients had carcinoma of the kidney, two patients had simultaneous carcinoma of prostate gland and urinary bladder, one patient had simultaneous carcinoma of prostate and kidney and one patient had haemorrhagic cystitis after radiotherapy. Liguori et al. [23] summated the results as follows:
- TAE of the internal iliac arteries had produced initial complete control of bleeding in 36 of the 44 patients which amounted to in 82% of the patients.
- At a mean (range) follow-up of 10.5 (1-97) months TAE there was noted to have achieved permanent control of bleeding in 19 patients which amounted to in 43% of the patients.
- A second TAE session was utilised in five patients which amounted to in 11% of the patients and it was successful in two of them.
- There were 24 patients which amounted to 55% of the patients who required a mean of 4 (1-17) transfusion units before embolization; only 13 (30%) required more blood products after TAE.
- The mean haematocrit level before and after TAE was 27% and 31% (P < 0001>
- During the follow-up there were no major complications related to TAE; minor complications were post-TAE syndrome in 12 (27%) patients, fever (11%), gluteus pain (14%), nausea (2%), and exterior genital oedema (5%).
- The 6 months and 12-months mortality rates were 66% (29 patients) and 18% (eight), respectively.
Liguori et al. [23] made the ensuing conclusions:
- TAE should be considered as an alternative less-invasive palliative measure and the treatment of choice in these situations.
- TAE should always be undertaken as a bilateral-embolization procedures, the catheter should be advance distally to the origin of the superior gluteal artery and the artery should be embolized with un-resorbable particles.
- Their study had confirmed the efficacy and safety of TAE in patients with pelvic malignancy, and had indicated that this technique should be considered before surgery.
- The procedure combines the benefits of a minimally invasive approach in decreasing the cost of surgery and operating time, while maintaining low blood loss and analgesia requirement.
Rastinehad et al. [9] assessed SAPE as an alternative treatment option in patients with refractory haematuria of prostatic origin. Rastinehad et al. [] undertook a retrospective analysis of charts from 10 patients. They stated that two patients were excluded from the analysis because of severe atherosclerotic disease which had prevented the undertaking of selective angiography of the pelvic vasculature. Therefore, 8 patients, whose mean age was 78.3 +/- 7.1 years with a history of refractory haematuria of prostatic origin were analysed by Rastinehad et al. [9] All of the patients had failed conventional therapy. The selective embolization procedures were undertaken between 2000 and 2006. Success was monitored with postembolization angiography and cessation of haematuria clinically. Rastinehad et al. [9] summated the results as follows:
- Out of the 8 patients, 6 had a history of adenocarcinoma of the prostate gland (mean Gleason Grade 7, range 5 to 9); 4 were previously treated with external beam radiotherapy.
- The remaining patient's histories were consistent with benign prostatic hypertrophy.
- SAPE was found to be technically successful in all 8 patients and had resulted in immediate cessation of visible haematuria.
- The mean follow-up post-embolization was 20.0 months and the follow-up had ranged between 1.5 months and 86.3 months.
- One patient had had developed visible haematuria 14 months ensuing the embolization that was attributed to a urinary bladder tumour recurrence.
- One patient who had T4 prostate cancer had a rectovesical fistula which he developed 1 month pursuant to his embolization procedure.
Rastinehad et al. [9] made the ensuing conclusions:
- SAPE results in cessation of refractory visible haematuria in patients with benign prostate hyperplasia and patients with prostate cancer which had been previously treated with radiotherapy.
- SAPE might be considered an effective treatment for visible haematuria in patients who have refractory visible haematuria regardless of the cause (radiation, cancer and/or hyperplasia).
Tarkhanov, et al. [35] made the ensuing background iterations:
- Embolization of bleeding due to locally advanced urinary bladder tumours is one of the most effective and minimally invasive methods, especially in cases of non-operative bleeding which does not react to conservative treatment.
- It has been iterated those severe complications are rare, but if they do occur, patient’s well-being would be at risk [36] [37]
- Complications could present as fever, pelvic pain, nausea (all of this is associated with postembolization syndrome and can be managed with NSAIDs).
- Minor complications could develop on first postprocedural days. It could be infection, urinary incontinence, retention of urine, prostatitis, soft tissue and penile ischemia. [37]
- All of the aforementioned conditions should be managed conservatively.
- Recently many case reports with positive outcome had been published. [5] [27] [36] [38] [39] [40]
- In their article they had described a case of tumour and encompassing urinary bladder tissue necrosis pursuant to urinary bladder arteries embolization due to visible haematuria.
Tarkhanov, et al. [35] reported a 58-year-old male, who had presented to a policlinic. He had manifested with dysuria, ischuria for several months and visible haematuria. He did not have physical symptoms of acute blood loss. The result of his serum Creatinine level was normal (68 mg/dL). He had ultrasound scan examination of his kidneys and urinary tract which demonstrated a solid urinary bladder mass that measured about 55 mm in diameter without signs of metastatic spread. The patient did not have any significant anaemia (HGB 117 g/l), but his haemoglobin (HGB) level had decreased from 143 g/l in two days.
Before his hospitalization additional imaging was undertaken which was reported as follows:
- MRI scan: presence of urinary bladder tumour that measured 63 mm with invasion of the right ureter with right hydrouretronephrosis .
- On nephroscintigraphy: nonfunctioning right kidney was found.
He had irrigation through a three-way catheter which was ineffective. He had conservative treatment of his haematuria (Транексам® (Tranexam), Obninsk, Russian Federation, tablets 500 mg 3 times per day) was ineffective. He had cystoscopy which was non-informative due to profuse haematuria, with multiple blood clots within in the urinary bladder. Pursuant to discussion with his referring physician it was decided to undertake selective embolization of the urinary bladder tumour due to potential life-threatening blood loss. He had a pre-operative CT-Angiography which showed significant neo-vascularisation of the neoplasm without obvious source of active bleeding. The patient underwent an embolization procedure: Right Common Femoral artery access was undertaken (Vascular sheath Prelude 5F, Merit Medical, USA., catheter Cobra C2 5F, Merit Medical, U.S.A.), bilateral superselective embolization of anterior division branches of Internal Iliac Arteries using microcatheter 2,4F (Progreat-α micro catheter, Terumo Corporation, Japan) and Avigo hydrophilic guidewire, Medtronic, USA). Superior and inferior-vesical arteries on both sides (see figures 4 and 5), left prostatic artery and left obturator arteries were embolized using 500 μm Embozene particles (Boston Scientific Corporation, USA) 1 vial per procedure (diluted with contrast media and saline in amount to stable suspension) to achieve subtotal stasis (near absence of contrast enhancement of distal parts of above-mentioned arteries), subtotal embolization of both anterior portions of Internal Iliac Arteries (notable ceasing of contrast flow from arising point) upon exit using gelfoam (Pfizer, USA) and Embozene suspension (self-made combination of Gelfoam particles about 20% of 10 ml syringe volume, mixed with Embozene spheres about 10% of syringe volume with contrast media and saline) (see figures 6 and 7). Such comprehensive embolization was undertaken as the departments dedicated medical facility with determined equipment was exclusive in terms of treating oncology patients and this particular patient could not be brought in time if the bleeding should re-occur at home.
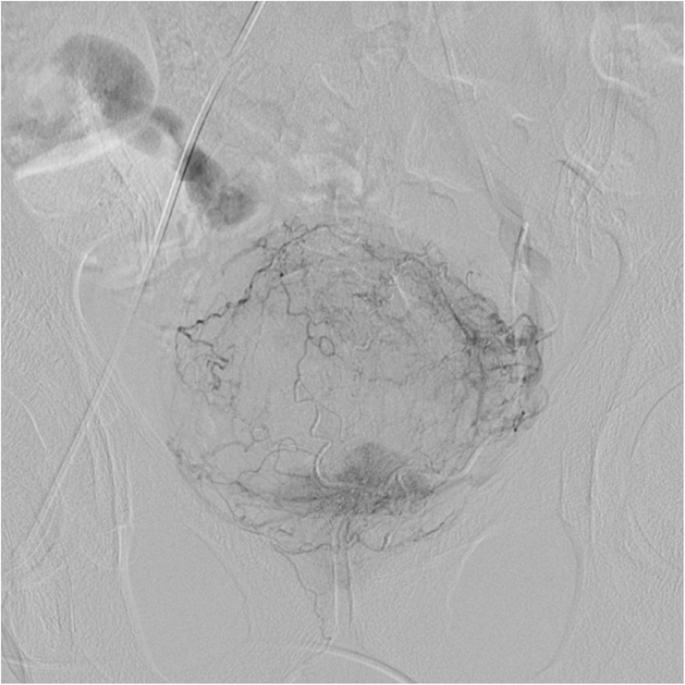
Figure. 4
Neovascularization in projection of tumour bed. Reproduced from; [35] Under the Creative Commons Attribution License.
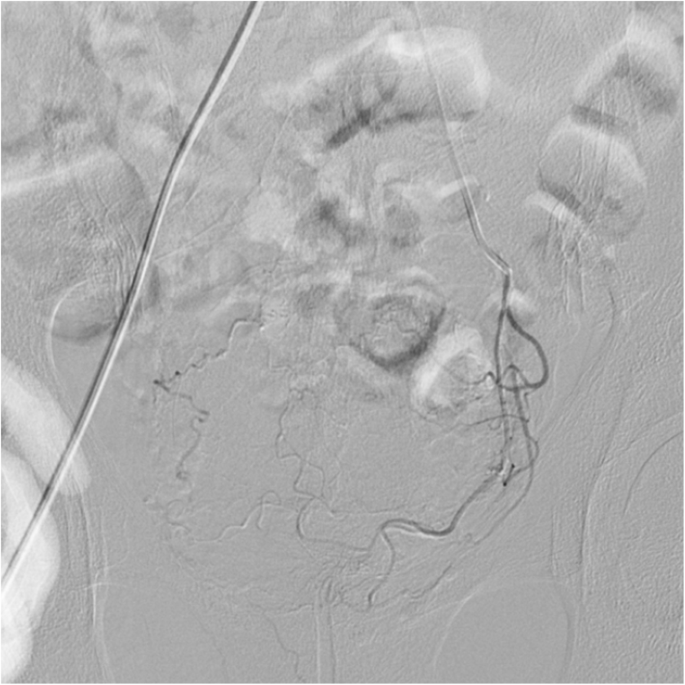
Figure 5
Finishing embolization on the left side. Reproduced from; [35] Under the Creative Commons Attribution License.
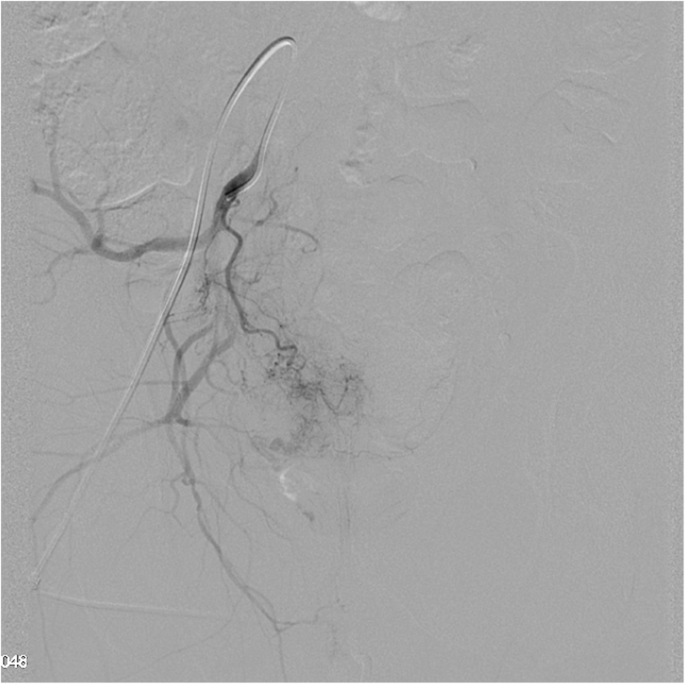
Figure 6
Finishing embolization on the right side.
Reproduced from; [35] Under the Creative Commons Attribution License.

Figure 7
Right side after finishing the procedure.
Reproduced from: [35] Under the Creative Commons Attribution License.
The procedures were undertaken under local anaesthesia using Lidocain 1%. Intravenous Fentanyl 0,2 mg (Fentanyl, Moscow endocrine factory, Moscow, Russia) was injected before embolization for analgesia during the procedure and programmed IV morphine pump connected following the procedure. Patient suffered from severe pelvic pain for 4 h after the procedure and mild pain in pelvic area for 2 days. Haematuria ceased on day 3 after the procedure. For planning further treatment transurethral biopsy of the mass was undertaken necrotic villous papillary tumour within lower semicircle of the urinary bladder was seen. Two days later the urologist diagnosed peritonitis. Upon ultrasound examination massive amount of free hyperechoic liquid, without gas was reported. Urgent exploratory laparotomy was undertaken which showed 3 to 4 l of free muddy smelly fluid within the abdominal cavity and total necrosis of the bladder wall. Sanation of abdominal cavity, necrectomy, cystostomy, and bilateral nephrostomy were undertaken. The patient deceased from multiple organ failure on day eight despite symptomatic treatment within the intensive care unit. An autopsy was undertaken which reported evidence of total necrosis of tumour with necrosis of underlying urinary bladder wall and multiple organ failure due to sepsis (see figures 8 and 9).
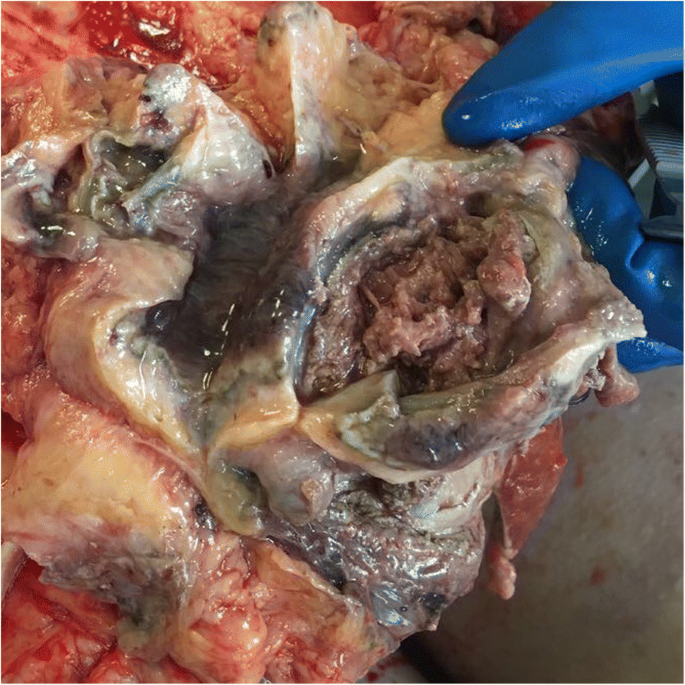
Figure 8.
Totally necrotized tumour and underlying bladder wall.
. Reproduced from: [35] Under the Creative Commons Attribution License.
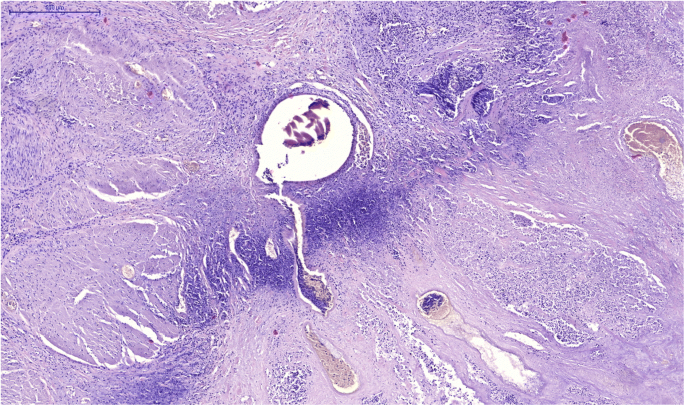
Figure 9
Microscopic view (normal muscle tissue, demarcation zone, tumour tissue and micro-embolus in vessel). Reproduced from: [35] Under the Creative Commons Attribution License.
Tarkhanov, et al. [35] made the ensuing educative discussions and conclusions:
- Chronic bleeding had been described in cases of most significant problems of oncology-urology.
- It has been pointed out that an oncology patient could face a permanent cascade of disbalance between pathways of coagulation. [41] [42] [43] [44]
- These patients are in slightly greater risk of bleeding without undergoing any surgical procedure and greater risk of bleeding in post-operative period.
- The most common cause of such complication could be a diffuse bleeding from traumatized tumour tissue surface after the undertaking of cystoscopy punch-biopsy.
- Conservative methods of bleeding control. [45]
- It is a complex scenario, because not each all patient from this cohort could survive cystostomy due to poor performance status.
- Recently, super-selective embolization had become the method of choice to control such bleeding.
- Besides, physicians choose embolization among other methods of treatment for acute bleeding: combined trauma with pelvic fractures, uncontrollable bleedings after gynaecological surgical operations and complications of radiotherapy (may be chronic as well). [46] [47] [48] [49] [50] [51]
- Usually, the sequence of actions entails the undertaking of bilateral diagnostic angiography of internal iliac arteries in order to determine a source of bleeding (arterial supply of bladder tumours could originate from superior and/or inferior vesical arteries, prostatic arteries, not infrequently it might be branches of internal pudendal artery, obturator arteries, [27] followed by super-selective embolization utilising various embolic agents. The most frequently-utilised agents are embolic spheres of different sizes, that could provide permanent tumour vessels occlusion (choosing spheres diameter depends on expected vessel penetration), but IRs also could employ or utilise polymorphic PVA agents (also permanent occlusion), gelfoam particles (temporary occlusion) or combinations of those. [27]
- Described methods of embolization are effective alternative to surgery.
- Embolization could be undertaken even in the in patients in shock and with high procedure success.
- The patient does not need special preparations.
- Despite obvious advantages and minimally invasive character of the procedure, in some cases embolization could lead to the development of serious complications.
- In a retrospective study of Matityahu et al., [47] the authors had reported 11% chance of complications, including one case of bladder necrosis from cohort of 98 patients. Serious complications were reported in all patients who had undergone bilateral embolization. [47]
- A major complication as urinary bladder necrosis was described within the first 4 weeks to 5 weeks pursuant to the embolization; [48] [49] nevertheless, they had found data of bladder necrosis in earlier post-operative period (two weeks after intervention). [49] [50]
- In their previous experience with over 40 embolization procedures of bleeding urinary bladder tumours they had utilised spherical calibrated BeadBlock (BTG) and EmboGold by Merit Medical particles they did not observe such complications with similar aggressive character of performed procedures.
- In their patient urinary bladder necrosis had developed within 10 post-embolization days.
- Factors that may contribute to the development of such life-threatening conditions include: tissue hypoperfusion and potential non-target embolization of non-involved in tumour supply bladder arteries, lack of good collateral flow due to patient abnormality such as atherosclerosis, hypovolemia due to developed sepsis.
- They had associated the aforementioned phenomenon with utilisation of strictly-calibrated microspheres with high concentration of particles per unit of volume (in comparison of non-strictly calibrated PVA particles or gelfoam).
- Strictly calibrated embolic agent is expected to have greater ability to penetrate the arteries with an exceptional dense filling capability, which can despite relatively large size of each sphere (500 μm) lead to complete tumour and some urinary bladder wall ischaemia. It seemed that strictly-calibrated microspheres do provide a desired haemostatic effect, but we have to carefully choose appropriate size of embolic agent according with vessel size of the target organ.
- Methods of embolization for bleeding control are firmly established in daily practice.
- Indisputable advantages of embolization therapy provide an opportunity to utilise it for patients with poor performance status, who cannot survive surgery or have contraindications to undergo general anaesthesia.
- Yet, even minimally-invasive treatment with overly aggressive approach could lead to life-threatening conditions.
- Such a potential complication needs to be discussed with the patient preceding the undertaking of the procedure and signing the informed consent.
- Each individual case requires a correct estimate of tumour blood supply and collateral flow followed by subtotal embolization of vessels feeding the tumour.
- Based upon described method of bladder tumour embolization utilising strictly-calibrated microspheres (EmboZene) they would recommend to avoid the use of particles sized 500μmor less, as it could lead to total necrosis of the tumour and encompassing urinary bladder tissue.
- In situations with less accessibility of catlabs for population from very remote locations, the goal is to find balance between significantly diminishing the flow within the tumour vessels in order to achieve stable haemostasis within the limits of single procedure, but not complete cessation of blood flow within the tumour bed in case of compromised collateral flow
Conflict of interest
Nil
Acknowledgement
Acknowledgements to:
- CVIR Endovasc. And Springer Nature for granting permission for reproduction of contents and figures from their Journal article under copyright of the Creative Commons Attribution License under ensuing copyright iterations: Rights and permissions Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made
- Wikipedia for granting permission for reproduction of contents and figures from their Journal article under copyright of the Creative Commons Attribution License
References
- Loffroy R, Pottecher P, Cherblanc V, Favelier S, Estivalet L, Koutlidis N, Moulin M, Cercueil JP, Cormier L, Krausé D. (2014). Current role of transcatheter arterial embolization for bladder and prostate hemorrhage. Diagn Interv Imaging. Nov;95(11):1027-1034.
View at Publisher | View at Google Scholar - Choong SK, Walkden M, Kirby R. (2000). The management of intractable haematuria. BJU international. Dec;86(9):951-959.
View at Publisher | View at Google Scholar - Capelli-Schellpfeffer M, Gerber GS. (1999). The use of hyperbaric oxygen in urology. The journal of Urology. 162(3):647-654.
View at Publisher | View at Google Scholar - Lang EK, Deutsch JS, Goodman JR, Barnett TF, Lanasa Jr JA, Duplessis GH. (1979). Transcatheter embolization of hypogastric branch arteries in the management of intractable bladder hemorrhage. The Journal of Urology. 1;121(1):30-36.
View at Publisher | View at Google Scholar - Carmignani G, Belgrano E, Puppo P, Cichero A, Giuliani L. (1980). Transcatheter embolization of the hypogastric arteries in cases of bladder hemorrhage from advanced pelvic cancers: follow up in 9 cases. The Journal of Urology. 1;124(2):196-200.
View at Publisher | View at Google Scholar - Carmignani G, Belgrano E, Puppo P, Cichero A, Quattrini S, Giuliani L. (1982) Treatment of massive hemorrhages due to inoperable pelvic neoplasms, by means of transcatheter embolization of the hypogastric arteries. Personal experience and review of literature. Minerva chirurgica. 37(15-16):1225-1234.
View at Publisher | View at Google Scholar - DS, Sibley GN, Doyle PT. (1988). Internal iliac artery embolisation for the control of severe bladder and prostate haemorrhage. British journal of urology. Jan;61(1):45-47.
View at Publisher | View at Google Scholar - Nabi G, Sheikh N, Greene D, Marsh R. Therapeutic transcatheter arterial embolization in the management of intractable haemorrhage from pelvic urological malignancies: preliminary experience and long‐term follow‐up. BJU international. 2003 Aug;92(3):245-247.
View at Publisher | View at Google Scholar - Rastinehad AR, Caplin DM, Ost MC, VanderBrink BA, Lobko I, Badlani GH, Weiss GH, Kavoussi LR, Siegel DN. (2008). Selective arterial prostatic embolization (SAPE) for refractory hematuria of prostatic origin. Urology. 1;71(2):181-184.
View at Publisher | View at Google Scholar - Delgal A, Cercueil JP, Koutlidis N, Michel F, Kermarrec I, Mourey E, Cormier L, Krausé D, Loffroy R. (2010). Outcome of transcatheter arterial embolization for bladder and prostate hemorrhage. The Journal of urology.;183(5):1947-1953.
View at Publisher | View at Google Scholar - Wikipedia the free encyclopedia. Hematuria
View at Publisher | View at Google Scholar - Mee SL, McAninch JW, Robinson AL, Auerbach PS, Carroll PR. (1989). Radiographic assessment of renal trauma: a 10-year prospective study of patient selection. J Urol. 141(5):1095-1098.
View at Publisher | View at Google Scholar - Leslie SW, Hamawy K, Saleem MO. (2024). Gross and Microscopic Hematuria.. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing;
View at Publisher | View at Google Scholar - Sharp VJ, Barnes KT, Erickson BA. (2013). Assessment of asymptomatic microscopic haematuria in adults. Am Fam Physician. 1;88(11):747-754.
View at Publisher | View at Google Scholar - Ingelfinger JR. (2021). Hematuria in Adults. N Engl J Med.;385(2):153-163. BMJ Best Practice Rhabdomyolysis
View at Publisher | View at Google Scholar - Poels PJ, Gabreëls FJ. (1993). Rhabdomyolysis: a review of the literature. Clin Neurol Neurosurg. ;95(3):175-92.
View at Publisher | View at Google Scholar - Kodadek L, Carmichael Ii SP, Seshadri A, Pathak A, Hoth J, Appelbaum R, Michetti CP, Gonzalez RP. (2022). Rhabdomyolysis: An American Association for the Surgery of Trauma Critical Care Committee Clinical Consensus Document. Trauma Surg Acute Care Open. 27;7(1):000836.
View at Publisher | View at Google Scholar - Tsitskari, M., Spiliopoulos, S., Konstantos, C. Palialexis, K, Reppas L, Brountzos E. (2020). Long-term results of super-selective trans-catheter embolization of the vesical arteries for the treatment of intractable bladder haematuria. CVIR Endovasc ; 3, 97.
View at Publisher | View at Google Scholar - Ghahestani SM, Shakhssalim N. (2009). Palliative treatment of intractable hematuria in context of advanced bladder cancer: a systematic review. Urol J. Summer;6(3):149-156.
View at Publisher | View at Google Scholar - Angle JF, Siddiqi NH, Wallace MJ, Kundu S, Stokes L, Wojak JC, Cardella JF. (2010). Quality improvement guidelines for percutaneous transcatheter embolization: Society of Interventional Radiology Standards of Practice Committee. Journal of Vascular and Interventional Radiology. Oct 1;21(10):1479-1486.
View at Publisher | View at Google Scholar - Liguori G, Amodeo A, Mucelli FP, Patel H, Marco D, Belgrano E, Trombetta C. (2010). Intractable haematuria: long‐term results after selective embolization of the internal iliac arteries. BJU international.;106(4):500-503.
View at Publisher | View at Google Scholar - Hietala SO. (1978). Urinary bladder necrosis following selective embolization of the internal iliac artery. Acta Radiologica. Diagnosis.;19(2):316-320.
View at Publisher | View at Google Scholar - Pisco JM, Martins JM, Correia MG. (1989). Internal iliac artery: embolization to control hemorrhage from pelvic neoplasms. Radiology.;172(2):337-339.
View at Publisher | View at Google Scholar - Ozono S, Okajima E, Hirao Y, Babaya K, Komada S, Matsuki H, Takahashi S, Ohishi H, Yoshioka T. (1988). Transcatheter arterial embolization of vesical artery in the treatment of invasive bladder cancer. European urology. 11;15(3-4):176-179.
View at Publisher | View at Google Scholar - Prasad V, Sacks BA, Kraus S, Clouse ME. (2009). Embolotherapy for lower urinary tract hemorrhage. Journal of Vascular and Interventional Radiology.;20(7):965-970.
View at Publisher | View at Google Scholar - Taha DE, Shokeir AA, Aboumarzouk OA. (2018). Selective embolisation for intractable bladder haemorrhages: A systematic review of the literature. Arab J Urol. 2;16(2):197-205.
View at Publisher | View at Google Scholar - Chen C, Kim PH, Shin JH, Yoon KW, Chung MS, Li HL, Hong B. (2021). Transcatheter arterial embolization for intractable, nontraumatic bladder hemorrhage in cancer patients: a single-center experience and systematic review. Jpn J Radiol.;39(3):273-282.
View at Publisher | View at Google Scholar - De Berardinis E, Vicini P, Salvatori F, Sciarra A, Gentile V, Di Silverio F. Superselective embolization of bladder arteries in the treatment of intractable bladder haemorrhage. Int J Urol.;12(5):503-505.
View at Publisher | View at Google Scholar - Mohan S, Kumar S, Dubey D, Phadke RV, Baijal SS, Kathuria M. (2019). Superselective vesical artery embolization in the management of intractable hematuria secondary to hemorrhagic cystitis. World J Urol. ;37(10):2175-2182.
View at Publisher | View at Google Scholar - Zhou C, Zhou CG, Wang B, Liu XL, Shi HB, Liu S. Superselective Vesical Artery Embolization for Intractable Hemorrhagic Cystitis Following Hematopoietic Stem Cell Transplantation: A Single-Center Retrospective Study in 26 Patients. Cardiovasc Intervent Radiol.;44(6):943-951.
View at Publisher | View at Google Scholar - Kim MS, Hong HP, Kang KA, Lee YR, Joo KJ, Cho YS, Lee YG. (2021). Superselective vesical artery embolization for intractable bladder hemorrhage related to pelvic malignancy. Acta Radiol.;62(9):1229-1237.
View at Publisher | View at Google Scholar - Rodríguez-Patrón Rodríguez R, Sanz Mayayo E, Gómez García I, Blazquez Sanchez J, Sanchez Corral J, Briones Mardones G, Pozo Mengual B, Escudero Barrilero A. (2003). Embolización de arterias hipogástricas como tratamiento paliativo del sangrado secundario a enfermedad vesical o prostática intratable [Hypogastric artery embolization as a palliative treatment for bleeding secondary to intractable bladder or prostate disease]. Arch Esp Urol.;56(2):111-118.
View at Publisher | View at Google Scholar - Tarkhanov A, Bartal G, Druzhin S, Shakhbazyan R, Grebenev E, Kartashov M. (2018). Bladder wall and surrounding tissue necrosis following bilateral superselective embolization of internal iliac artery branches due to uncontrollable haematuria related to bladder tumor: case report. CVIR Endovasc.;1(1):34.
View at Publisher | View at Google Scholar - Korkmaz M, Şanal B, Aras B, Bozkaya H, Çınar C, Güneyli S, Gök M, Adam G, Düzgün F, Oran I. (2016). The short- and long-term effectiveness of transcatheter arterial embolization in patients with intractable hematuria. Diagn Interv Imaging.;97(2):197-201.
View at Publisher | View at Google Scholar - Greenstein A, Merimsky E, Papo J, Braf Z. (1983). Douleur fessière persistante après embolisation des artères hypogastriques. Une complication inattendue [Persistent gluteal pain after embolization of the hypogastric arteries. An unexpected complication]. J Urol (Paris).;89(8):595-596.
View at Publisher | View at Google Scholar - Pereira J, Mancini I, Bruera E (2000). The management of bleeding in patients with advanced cancer. In: Portenoy RK, Bruera E, editors. Topics in palliative care, Vol. 4. New York: Oxford University Press. 163-183
View at Publisher | View at Google Scholar - Pereira J, Phan T. (2004). Management of bleeding in patients with advanced cancer. Oncologist.;9(5):561-570.
View at Publisher | View at Google Scholar - El-Assmy A, Mohsen T. (2007). Internal iliac artery embolization for the control of severe bladder hemorrhage secondary to carcinoma: long-term follow-up. Scientific World Journal. 7:1567-1574.
View at Publisher | View at Google Scholar - Fricke A, Ullrich PV, Cimniak AFV, Becherer C, Follo M, Heinz J, Scholber J, Herget GW, Hauschild O, Wittel UA, Stark GB, Bannasch H, Braig D, Eisenhardt SU. (2017). Levels of activated platelet-derived microvesicles in patients with soft tissue sarcoma correlate with an increased risk of venous thromboembolism. BMC Cancer. 7;17(1):527.
View at Publisher | View at Google Scholar - Salignac S, Walter A, Feugier P, Lecompte T, Lesesve JF. (2002). Une observation de tumeur solide en phase terminale: interprétation des anomalies biologiques (tests hématologiques) [Solid tumor in terminal phase: interpretation of biologic anomalies (hematologic tests)]. Ann Biol Clin (Paris).;60(1):96-100.
View at Publisher | View at Google Scholar - Kennedy AR, Maity A, Sanzari JK. (2016). A Review of Radiation-Induced Coagulopathy and New Findings to Support Potential Prevention Strategies and Treatments. Radiat Res.;186(2):121-140.
View at Publisher | View at Google Scholar - Zhu YW, Feng TB, Zhou XJ, Hu XL, Ding J, Zhu WY, Qian DP, Sun YW. (2016). Routine Hemostasis and Hemogram Parameters: Valuable Assessments for Coagulation Disorder and Chemotherapy in Cancer Patients. Chin Med J (Engl).;129(15):1772-1777.
View at Publisher | View at Google Scholar - Kolev K, Longstaff C. (2016). Bleeding related to disturbed fibrinolysis. Br J Haematol.;175(1):12-23.
View at Publisher | View at Google Scholar - Agolini SF, Shah K, Jaffe J, Newcomb J, Rhodes M, Reed JF 3rd. (1997). Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage. J Trauma.;43(3):395-399.
View at Publisher | View at Google Scholar - Matityahu A, Marmor M, Elson JK, Lieber C, Rogalski G, Lin C, Belaye T, Miclau T 3rd, Kandemir U. (2013). Acute complications of patients with pelvic fractures after pelvic angiographic embolization. Clin Orthop Relat Res.;471(9):2906-2911.
View at Publisher | View at Google Scholar - Ali A, Nabi G, Swami S, Somani B. (2014). Bladder necrosis secondary to internal iliac artery embolization following pelvic fracture. Urol Ann.;6(2):166-168.
View at Publisher | View at Google Scholar - Sieber PR. (1994). Bladder necrosis secondary to pelvic artery embolization: case report and literature review. J Urol.;151(2):422.
View at Publisher | View at Google Scholar - Sieber PR. (1994). Bladder necrosis secondary to pelvic artery embolization: case report and literature review. J Urol.;151(2):422.
View at Publisher | View at Google Scholar - Washington S, Osterberg EC, Elliott SP, Hittelman AB, Breyer BN. (2016). Acute Bladder Necrosis after Pelvic Arterial Embolization for Pelvic Trauma: Lessons Learned from Two Cases of Immediate Postembolization Bladder Necrosis. Case Rep Urol.;7594192.
View at Publisher | View at Google Scholar - El-Shalakany AH, Nasr El-Din MH, Wafa GA, Azzam ME, El-Dorry A. (2003). Massive vault necrosis with bladder fistula after uterine artery embolisation. BJOG. Feb;110(2):215-216.
View at Publisher | View at Google Scholar
