

Research Article | DOI: https://doi.org/10.31579/2834-5029/024
Cerebrovascular Disease
- Rehan Haider *
Riggs Pharmaceuticals Karachi, Department of Pharmacy University of Karachi, Pakistan.
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals Karachi, Department of Pharmacy University of Karachi, Pakistan.
Citation: Rehan Haider, (2023), Cerebrovascular Disease, International Journal of Biomed Research, 2(4): DOI:10.31579/2834-5029/024
Copyright: © 2023, Rehan Haider. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 June 2023 | Accepted: 30 June 2023 | Published: 10 July 2023
Keywords: cerebrovascular disease; ischemic stroke; hemorrhagic stroke; transient ischemic attack (TIA); high blood pressure; smoking
Abstract
The cerebrovascular disorder is a broad term encompassing various situations that affect the blood vessels in the brain. It is a major cause of morbidity and mortality worldwide, often leading to stroke or brief ischemic attack (TIAs). This summary aims to provide a concise overview of cerebrovascular disorders, their threat factors, pathophysiology, scientific presentation, and available treatments.
Cerebrovascular sickness can develop due to numerous causes, including atherosclerosis, embolism, and vascular malformations. Threat elements, such as high blood pressure, diabetes, smoking, and excessive cholesterol levels, contribute to the improvement and development of the disease. The pathophysiology involves disruption of blood flow to the mind, leading to ischemia, neuronal harm, and subsequent neurological deficits.
The clinical presentation of cerebrovascular ailments varies depending on the particular circumstances and affected mental regions. Stroke, characterized by sudden focal neurological deficits, is the most unusual manifestation. TIAs regularly referred to as "mini-strokes are gifts with transient signs and symptoms that resolve within 24 hours. Unusual symptoms include weakness or paralysis of the limbs, speech difficulties, visible disturbances, and cognitive impairment.
Control of cerebrovascular disorders involves both acute interventions and lengthy-time preventive measures. Acute treatment focuses on the fast healing of blood wafers to the affected mind tissue through thrombolytic therapy, endo vascular procedures, or surgical interventions. Long-term management emphasizes chance factor modification via way-of-life changes, medications, and interventions including carotid endarterectomy or angioplasty. Improvements in diagnostic strategies, together with magnetic resonance imaging (MRI), computed tomography (CT), and cerebral angiography, have improved the accuracy of the analysis and guided treatment choices. Additionally, ongoing research has explored novel healing goals consisting of neuroprotective agents, antiplatelet treatment plans, and stem cell-based interventions.
Introduction
Epidemiology of stroke in widespread
Cerebrovascular sickness (CVD) is the main cause of morbidity and mortality. It is an incredibly widespread disorder with approximately seven-hundred 000 strokes taking place every year in the u... Of these, 500 000 are first-time events, whilst 200 000 are recurrent events [1]. Stroke is the third leading cause of loss of life in America, following heart disease and all types of cancers. As a result, a girl is more than twice as probably to die from a stroke than she is from breast most cancers, and one and a half of instances as likely as from lung cancer [2]. furthermore, it's miles the primary purpose indexed for discharge diagnosis for patients discharged from hospitals to chronic care centers. In total, the price of stroke to health care devices in us turned to $sixty-two.7 billion in the yr 2007 [1]. information in different international locations is much like the ones seen inside the United States. The Oxford Vascular has a look at [3], which compiled stroke facts for all and sundry within the county of Oxford shire, demonstrated a typical prevalence of 1.62 strokes in step with one thousand patients per 12 months. The WHO MONICA observe looked at 21 populations in 11 countries, 10 ecu countries in addition to China, and located an occurrence of 125 – 361/one hundred 000 sufferers in guys and 61 – 194/one hundred 000 in ladies [4].
Diabetes as a risk factor for stroke
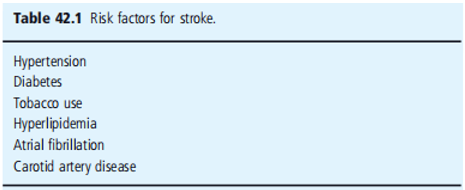
There is strong evidence that type 1 (T1DM) or type 2 (T2DM) diabetes mellitus is a strong risk factor for ischemic cerebrovascular disease (Table 42.1). Observational studies have demonstrated an association between these two diseases. A model created from data from the Framingham Heart Study showed that diabetes confers an increased relative risk of 1.4 in men and 1.72 in women [5]. The Honolulu Heart Study showed that diabetes increases the risk of thromboembolic stroke between two - and three-fold over those without the disease in Japanese men living in Hawaii [6].
The effect of diabetes is stronger among ethnic minorities in the USA. The Greater Cincinnati and Northern Kentucky Stroke The study found that as a sole risk factor, diabetes increased the odds ratio for having an ischemic stroke by 2.1 in Caucasians; however, in African - Americans that odds ratio was increased by 2.7. These results were obtained across all age cohorts [7]. Similarly, the Northern Manhattan Study found that diabetes was a stronger risk factor for ischemic stroke among African-Americans and Caribbean Latinos than among Caucasians. In these ethnicities, diabetes increased the stroke risk by 1.8 and 2.1, respectively, partly because of the increased prevalence of the disease.
The proportion of strokes that could be directly attributable to diabetes as a risk factor was 14% among African Americans and 10% among Caribbean Latinos [8]. The Copenhagen City Heart Study found a difference in the effects of diabetes between men and women. Thus, diabetes increased the relative risk of first stroke, incident stroke, and hospital admission for stroke among men by 1.5 – 2, and among women, the same relative risks were increased by 2 – 6.5 [9].
In addition to its effects as the sole risk factor, diabetes exacerbates the effects of other risk factors. Thus, in patients with isolated systolic hypertension, diabetes confers an additional risk of ischemic stroke or transient ischemic attack (TIA).
Stroke in patients with diabetes
Epidemiologic studies have shown that ischemic stroke occurs at a younger age in patients with diabetes. They are also more likely to be African American. Among other risk factors, those with diabetes Patients with ischemic stroke are more likely to have hypertension and hyperlipidemia and to have experienced myocardial infarction (MI) in the past [7]. Furthermore, diabetes increases the risk of death due to stroke. In a prospective study in a Finnish cohort, men had an increased relative risk of 6 for mortality from ischemic stroke, whereas women had a relative risk of 8.2. These relative risks were higher than those for systolic blood pressure (BP), smoking, or total serum cholesterol. In this cohort, the proportion of stroke deaths directly attributable to diabetes was 16% in men and 33.3% in women [10].
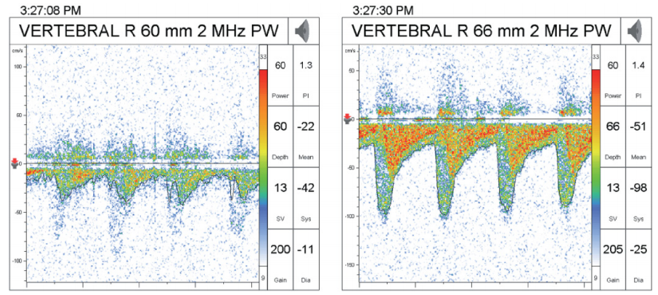
In terms of stroke subtype, diabetes is most commonly associated with lacunar infarcts. These are small, deep infarcts in the territory of a single penetrating arterial branch. Conversely, patients with demonstrable microvascular diseases had the highest prevalence of diabetes. Similarly, lacunar disease is more likely to be associated with diabetes than hemorrhage at the same location (Figure 42.1) [11 – 14]. Diabetes is associated with both extra cranial and intracranial stenosis. In one study of 510 patients referred for asymptomatic carotid bruits, only 200 had extra cranial stenosis on Doppler examination. 66 had asymptomatic intracranial stenosis, of whom 37 had concurrent extra cranial stenosis. Of the patients with intracranial stenosis, 19 had diabetes (Figure 42.2) [15].
TIA is much less common in people with diabetes than in those now not having the disease. this will imply that patients with diabetes are more likely to provide with a finished infarct instead of
reversible ischemia [16]; but, patients with diabetes who do a gift with TIA are much more likely to move directly to full-blown ischemic stroke within the next 2 days as expected by using the ABCD2 score. This score stratifies patients with TIA through the following factors: age > 60 years, BP greater than 140/90 mmHg, medical capabilities of motor or speech involvement, duration of more than 60 minutes, and diabetes [17]. Diabetes is a risk factor for coronary artery ailment (CAD), and therefore for MI and the subsequent development of atrial fibrillation. In a large retrospective study of the relationship between diabetes and atrial fibrillation or atrial flutter, diabetes was found to be a robust independent predictor of atrial arrhythmias in an assessment of over 850 000 charts over a ten-year length. The percentage ratio of diabetes was 2.13, with a 95% confidence interval (CI) of 2.10 – 2. sixteen [18]. In contrast, atrial fibrillation has been repeatedly validated as a sturdy risk factor for cardioembolic stroke, with an expected 75 000 strokes per year attributable to arrhythmia [19]. Moreover, diabetes increases the risk of cardiac embolization. The CHADS2 score is a proven approach to stratifying the chance Cardioembolic stroke in patients with atrial fibrillation. It assigns one factor every for the presence of congestive coronary heart failure (CHF), hypertension, age greater than 75 years, diabetes, and points for previous stroke or TIA. The growth of each factor was related to a 1. Five-fold increased risk of stroke. Diabetes by myself would increase the risk of stroke in a patient with atrial fibrillation from 1.9 to 2.8 [20]. While the CHADS2 score is not perfect, and attempts have been made to make it more precise [21], it has the benefit of being very easy to use, thus guiding non-stroke practitioners towards using anticoagulation in the appropriate section of the population.
In large observational studies, there has not appeared to be an association between diabetes and hemorrhagic strokes. In contrast, in the Hemorrhagic Stroke Project, a case–control study of young patients with intracerebral and diabetes conferred an adjusted odds ratio of 2.4. The risk factor with the greatest impact was hypertension, which outweighed the contribution of diabetes by more than two-fold [22].
Intermediate hyperglycemia and other risk factors
Although it is well established that diabetes is a strong risk factor for ischemic stroke, forms of intermediate hyperglycemia are not as indicated as risk factors. Selvin et al. [23] looked at people with and without diabetes in the Atherosclerosis Risk in Communities (ARIC) trial and compared hemoglobin A 1c (HbA 1c) levels drawn at a specified visit, not necessarily related to at the time of the incident stroke. With increasing tertile of HbA 1c across the normal distribution within each group, the risk of stroke increased in both those with diabetes and those without the disease, although only in those with diabetes, the difference was statistically significant [23]. In contrast, Myint et al. [24] abstracted data from the European Perspective Investigation into Cancer (EPIC) on HbA 1c Levels in patients without known diabetes and correlated these data with stroke chance. on this populace, it become the handiest after HbA 1c ranges had been better than 7. 0% (fifty-three mmol/mol) that an extended hazard of stroke was validated, in comparison to sufferers with HbA 1c less than 5. 0% (31 mmol/mol). for the reason that those sufferers are the maximum possible to have undiagnosed diabetes, this finding may not implicate continual hyperglycemia by myself as the number one risk thing for stroke [24].
Insulin resistance (IR), another form of diabetes, has also demonstrated conflicting proof an affiliation with stroke. The ARIC investigated hyperinsulinemia in those without diabetes and determined a slight growth within the hazard of stroke of 1.19 with each increase of 50 pmol/L of fasting insulin. After adjustment for other risk factors along with age, systolic BP, and smoking, the growth in chance now becomes less well described [25].
Weight problems, a proxy for insulin resistance and intermediate hyperglycemia, have also been related to stroke through numerous epidemiologic studies. As an example, the Copenhagen city heart the study observed that frame mass index (BMI) became independently related to an accelerated risk of stroke [26]. similarly, the Nurses’ fitness study observed, as anticipated, a multiplied chance of stroke with increasing BMI, with a relative chance of stroke of two.37 (95% CI 1.60 – three.50) visible in patients with BMI > 32 kg/m 2 [27]; however, ARIC was not able to demonstrate any dating between BMI and stroke, or between waist: hip ratio, a better dimension of belly weight problems, and stroke [25]. similarly, whilst adjustment for cardiovascular dangers was done, the relative danger of BMI for stroke was once again attenuated. even though those personal forms of intermediate hyperglycemia have not conclusively been proven to predispose people to stroke, a constellation of diseases, together known as metabolic syndrome, has been reported. The combination of hypertension, hyperlipidemia, IR, and stomach weight problems creates an environment that is relatively at risk for vascular damage and ischemic sequelae.
In a Finnish cohort, metabolic syndrome in the absence of diabetes or cardiovascular disease (CVD) was related to stroke with a relative risk of approximately 2, after adjustment for more than one other risk factor [28]. In addition, a cohort from the ARIC has a look at those who likewise turned free of diabetes, coronary heart disease (CHD), or stroke and had an improved hazard of 1.5 – 2. zero for ischemic stroke. In addition, when separating each hazard issue, there seemed to be a synergistic impact from the aggregate of the relative dangers inherent in each issue [29].
Pathophysiology of ischemic stroke in diabetes
Diabetes predisposes patients to vascular thrombi-bi-occlusive events in several ways. Accelerated atherosclerosis occurs in both large and medium-sized vessels. There is a disordered endothelial response and the blood of patients with diabetes is hypercoagulable [30].
Carotid intimate-media thickness (cIMT) is a useful proxy for early atherosclerosis because it is easily measured using Doppler imaging. Furthermore, cIMT is associated with primary stroke, with an increased relative risk per standard deviation (0.163 mm) of 1.57 in patients who had not had a previous stroke [31]. It also predicts recurrent stroke, with each 0.1 mm of increase in cIMT were associated with an increased risk of 18% [32]. Diabetes is associated with an increased cIMT. The IR atherosclerosis Study demonstrated an increase in common cIMT in patients with chronic diabetes, but not in those with newly diagnosed diabetes. Nor was there an association with Internal cIMT [33]. Conversely, patients with diabetes and stroke have been found to have greater cIMT. In one study of 438 Japanese patients with T2DM, common cIMT was significantly higher in those who had a stroke, even after adjustment for age, BMI, and smoking status [34]. Similarly, in a Czech cohort, cIMT increased in stroke patients with diabetes [35].
Atherosclerosis also affects the ability of the endothelium to release nitric oxide (NO), a potent vasodilator. Diabetic blood vessels either reduce NO production or alter NO metabolism. In addition to its vasodilating effects, NO protects against platelet aggregation and enables the blood vessels to withstand ischemic conditions. With decreased NO activity, the vessel tends towards vasoconstriction, with a predictably poor response to ischemia. Stroke patients have been demonstrated to have decreased NO levels in the circulating blood, along with increased peroxynitrite (ONOO), a reactive oxygen species. These results were particularly true for larger strokes. Because the measurements were performed for acute stroke, these levels are likely to represent the outcome of ischemia rather than the cause; however, the correlation supports the role of decreased NO in the effects of stroke [36]. The cerebral vasculature has a diminished response to the inhibition of NO synthase (NOS). In a small study of men with diabetes treated with a synthetic NOS inhibitor, NG - mono methyl - L - arginine (L - NMMA), the blood flow through the internal carotid artery was significantly lower than that in control subjects treated similarly [37].
As further indirect evidence of the role of NO in stroke, 3 - hydroxy - 3 - methyl - glutaryl coenzyme A (HMG-CoA) reductase inhibitors (statins) have multiple beneficial effects beyond their most common effect of lowering plasma cholesterol. Among these effects are increased expression of endothelial NOS and decreased activity of Rho-kinase, a pro-constrictor enzyme [38]. Statins have been demonstrated to lower the risk of recurrent stroke in multiple large studies [39 – 41]. Whether the social effect of statins in stroke is due to their cholesterol-lowering effect, their ability to stabilize atherosclerotic plaques, their effects on vascular function, or more likely a combination of all of the above is very difficult to separate.
In addition to the aforementioned predisposing factors, the blood of patients with diabetes is hypercoagulable. Studies have demonstrated increased thrombin generation [42], prothrombin fragments, and thrombin-anti-thrombin III complexes [43]. Furthermore, elevated pro thrombotic levels are significantly associated with macroangiopathic complications. Thrombus formation is further promoted by platelet hyper reactivity in the blood of patients with diabetes. In patients with metabolic syndrome, platelets have been shown to have increased activity both through closure time as measured by the platelet function analyzer (PFA - 100), increased fi fibrinogen binding after exposure to ADP, implying activation of the GPIIa/IIIb receptors, and expression of activated ligands on the platelet surface [44]. In full-blown diabetes, platelets are hyper reactive, as measured by light transmittance aggregometry and the expression of surface ligands [45].
Thus, a person with diabetes has a vascular environment that is highly susceptible to thrombotic-occlusive complications. With early atherosclerosis and a disordered endothelial response, these conditions are predisposed to thrombophilia. Blood, in its hypercoagulable state, e combined with platelets that are highly active in themselves, is far more likely to form clots.
Lacunar strokes are caused by damage to smaller parenchymal vessels. The most common cause is micro atheroma, as demonstrated in the pathologic case series published by Fisher [46 – 48], the neurologist responsible for naming lacunar syndromes. Lipohyalinosis and fibrinoid necrosis also cause micro angiopathy, and both are most commonly found in chronic hypertension with severe acute BP elevations, as seen in hypertensive encephalopathy [49,50].
Primary prevention of stroke in the patient with diabetes
Primary prevention of stroke is of paramount importance, as the disability from stroke and health care costs associated with the acute and chronic care of stroke are extensive. The approach Prevention in patients with diabetes is a multifactorial necessity. Medical therapy aimed at achieving normoglycemia is fundamental. The Diabetes Control and Complications Trial (DCCT) investigated intensive insulin regimens, including subcutaneous insulin injections and external insulin pumps, in patients with T1DM. The goal for treatment was HbA 1c levels of less than 6.05% (42 mmol/mol). The comparison group had no goals outside of the prevention of hyperglycemia or hypoglycemia [51]. The intensive treatment group achieved a reduction in the combined endpoints of nonfatal MI or stroke, cardiac death, or revascularization by 57%. Most of this improvement was associated with a decrease in HbA 1c [51]. Among oral hypoglycemic agents, metformin has been shown to decrease diabetes-related endpoints, including stroke, by 32% and diabetes-related mortality, including stroke, by 42% when compared with conventional therapy. Furthermore, it was more effective in reducing these outcomes when compared with other intensive therapies, such as sulfonylureas (e.g., chlorpropamide or glibenclamide) or insulin. It should be noted that the HbA 1c levels were similar between the treatment groups, and so the benefits were not explicable based on improved glycemic control [52].
Rosiglitazone, a thiazolidinedione, has been associated with an increased risk of MI and death from cardiovascular causes. Stroke was not assessed separately in the meta-analysis reporting these findings. [53]. In a more recent multicenter, open-label trial directly assessing the effect of rosiglitazone on cardiovascular outcomes, the use of rosiglitazone was associated with a non-significant reduction in stroke (HR 0.72, 95% CI 0.49 – 1.06) [54]. Pioglitazone, another medication in the same class, was not associated with worse cardiovascular outcomes, including stroke, and reduced the secondary outcomes of all-cause mortality, non-fatal MI, and non-fatal stroke by 16% [55]. The UK Prospective Diabetes Study (UKPDS) failed to show any reduction in macro vascular complications of T2DM despite an 11% reduction in HbA 1c in the intensive treatment group.
Microvascular complications such as retinopathy and neuropathy are significantly reduced [56]. A 10-year follow-up study of the same cohort after attempts to maintain treatment differences showed that the original treatment cohort had persistent decreases in microvascular complications, as well as in MIs and deaths from any cause, but not CVA [57]. Thus, glycemic control, in patients with T2DM has not been linked to a reduction in the risk of stroke.
Given how susceptible people with diabetes are to other vascular risk factors, such as hypertension and hyperlipidemia, the therapeutic regimen must also address these states. In In treating hypertension in people with diabetes, the classes of medications with effects on the renin-angiotensin system appear to have the greatest benefit. The Hypertensive Old People in Edinburgh (HOPE) trial examined patients with vascular disease (including CAD or stroke) or diabetes plus one other cardiovascular risk factor, such as hypertension, tobacco use, or elevated low-density lipoprotein levels. In this high-risk population, ramipril, an angiotensin-converting enzyme inhibitor (ACEi), decreased the risk of death from cardiovascular causes with a relative risk of 0.74 and reduced the risk of stroke with a relative risk of 0.68. As the mean reduction in BP was 3/2, the benefits were not attributed to the BP-lowering effect of the medication. The effect was whether the patients had had a stroke before enrollment [58].
The Losartan Intervention for Endpoint Reduction in Hypertension (LIFE) trial examined patients with diabetes, hypertension, and left ventricular hypertrophy. The participants were treated with either losartan, an angiotensin receptor blocker (ARB), or atenolol. Although, once again, both medications achieved the same reduction in BP, the primary endpoint of cardiovascular mortality, MI, or nonfatal stroke was reduced with a relative risk of 0.76 in the Losartan group. Notably, in this trial, only 40% of participants achieved a systolic BP of less than 140 mmHg, implying that further benefits would likely accrue with more intensive management [59]. The latest trial of in-intensity multifactorial clinical control in patients with diabetes and micro albuminuria confirmed a discount in all-cause mortality, cardiovascular mortality, and aerobic vascular activities. The habitual modified into designed to gain the following desires: HbA 1c tiers of a whole lot much less than 6.5% (48 mmol/mol), fasting standard serum cholesterol levels of a lot less than one hundred seventy-five mg/dL (4. five mmol/L), systolic BP lots less than a hundred thirty mmHg and diastolic BP a good deal less than eighty mmHg. The stroke was no longer modified into a pre-specified endpoint in this commentary; however, there were six strokes in six patients inside the huge scientific institution, assessment with 30 strokes in 18 patients in the management enterprise [60].
whilst an antiplatelet treatment is suggested for the number one prevention of CAD, the Anti-Thrombotic Trialists’ Collaboration meta-evaluation did not display a giant development in Number one prevention of ischemic stroke in patients with diabetes. Not unusual, there were nearly 5000 sufferers treated with aspirin, with the best at a 7% discount in extreme vascular events. The confidence c language becomes enormous and sufficient to consist of a possible 25% hazard discount, quite a number that is steady with the prevention of secondary stroke in this population. it can be in this populace at an excessive chance, that the capability giants of prophylactic aspirin outweigh the hemorrhagic headaches [61]. most of the early trials of anti-thrombotic medicines have been performed first-rate on guys. inside the women s fitness examination, a study accomplished among lady fitness specialists with no history of coronary or cerebrovascular illness, low-dose aspirin (one hundred mg each unique day) becomes associated with a 17% chance discount in stroke, a result of a 24% threat reduction in ischemic stroke and a non - sizable increase in hemorrhagic stroke. the one finding had been particularly said in girls older than age 65 at the time the enrollment, in addition to the subgroup with diabetes [62].
Treatment of acute stroke in the patient with diabetes
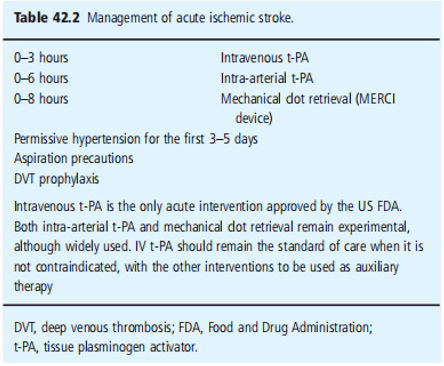
Treatment of acute stroke is limited by the vulnerability of the neuron to ischemic insult. With lower cerebral blood flow (CBF), the parenchyma is less likely to recover from even short durations of ischemia. With CBF less than 2 hundred mL/kg of tissue, neurologic disorder begins to appear; however, it is not until CBF falls beneath a hundred mL/kg of tissue irreversible ischemia occurs, in a count of mins [63]. Thrombolysis has been confirmed to be powerful within the Treatment of acute stroke, as long as the medication is given within the first three hours after symptom onset, as defined by using the final time the affected person changed into seen at their neurologic functional baseline (Figure 42.2). The countrywide Institute of Neurologic disorders (NINDS) trial of intravenous tissue plasminogen activator (t-PA) demonstrated a 30 – 50% increased likelihood of minimum or no disability three months after treatment. The thrombolysis turned associated with a 6.4% chance of symptomatic intracranial hemorrhage, but mortality facts at 3 months were no longer statistically exclusive between the treatment and placebo companies [64]. primarily based on this trial, treatment with intravenous t - PA has emerged as the same old of care in this early duration. whilst the latest records from the ECASS-III trial endorse that it isn't always the handiest safe however clinically effective to a lesser degree in a pick organization of patients to offer intravenous t-PA in the window between three and 4.5 hours, this has no longer yet grown to be a trendy exercise. In addition, patients with diabetes who had a preceding stroke based on records or imaging were excluded from the trial [65].
Thrombolysis in patients with diabetes and acute stroke is not as successful as that in the general population. In one collection of 27 patients treated with intravenous t-PA, none of the patients with diabetes achieved recanalization of the occluded artery as measured by transcranial Doppler [66]. The collection was not sufficiently large to illustrate a good-sized difference. In every other study examining which elements would possibly expect principal neurologic improvement in patients treated with intravenous tPA, there was a trend toward patients with diabetes being much less likely to reap that development [67].
Past intravenous thrombolysthromboly, an intra-arterial bio-lysishavesh beeperi-stroke then tested in patients up to 6 h after the onset of stroke signs. The Prolyse in Acute Cerebral Thromboembolism II (PROACT II) trial showed that patients treated with intra-arterial urokinase had a 58% relative risk reduction to reap minimum or no purposeful disability 90 days after remedy. Mortality prices were comparable, and recanalization fees notably increased with medication [68]. Cutting-edge tips guide the use of intra-arterial thrombolysis inside the length between three and 6 h; however, the medication has not been authorized by the USA Federal Drug Administration (FDA) for this indication [69]. In a single case series of 100 patients who underwent intra-arterial thrombolysis with urokinase, diabetes was related to poor useful final results at three months. It became no longer associated with symptomatic intracranial hemorrhage [70], but because diabetes is independently related to worse effects following acute ischemic stroke, it is not clear whether these facts have any indicated clinical exercise. Hyperglycemia at the time of stroke remedy is related to worsened effects. In a series of seventy-three patients dealt with intravenous t - PA, age, diabetes, admission glucose extra than one hundred forty mg/dL (7.8 mmol/L), and early re-occlusion on transcranial Doppler imaging had been significantly associated with worsened functional final results as defined by a rating of extra than three on the modified Rankin scale, however, after
logistic regression, the most effective hyperglycemia remained as an unbiased predictor of terrible final results. In particular, it was related to a larger infarct length, a lesser degree of neurologic improvement, and worse clinical outcomes of recanalization changed into finished.
Similarly, baseline hyperglycemia is associated with a greater probability of taking place in symptomatic intracranial hemorrhage after intravenous thrombolysis. There appears to be a dose –between the stages of serum glucose and the likelihood of hemorrhage. This became, in particular, real whilst levels had been > 11.1 mmol/L (two hundred mg/dL), where 25% of patients had symptomatic intracranial hemorrhage. In a repeat analysis substituting the presence of diabetes for glucose tiers, diabetes was related with an odds ratio of 36.1 for all hemorrhages and seven. forty-six for symptomatic hemorrhage. moreover, both the sufferers who acutely worsened and the one's patients who showed a lack of improvement at 24 hours had been times more likely to have accelerated their blood glucose levels at baseline. Hyper acute worsening in patients treated with both intravenous and intra-arterial thrombolysis, or both, was not extraordinarily associated with intracerebral hemorrhage and lack of recanalization; however, it was also associated with higher serum glucose levels. With each increase in 50 mg/dL glucose, the odds ratio for worsened final results was 1.50, and the odds ratio for mortality was 1.38. Even in the patients who did obtain recanalization, higher blood glucose expected worse effects.
in addition, serum glucose greater than a hundred and 44 mg/dL, as well as cortical involvement and time to treatment had been impartial predictors of lack of improvement at 24 hours after remedy with intravenous thrombolysis. The chance ratio for hyperglycemia was 2.89. Moreover, lack of development at 24 h predicted negative purposeful outcomes at three months.
even as those statistics are understandably disheartening, they ought to by no means be taken to suggest that patients with diabetes and acute stroke have to not get hold of thrombolysis, nor that these patients do now not benefit from the remedy. moreover, it is not clear whether the hyperglycemia that is seen in patients with acute stroke and diabetes is secondary to the ischemic insult as a stress response, or rather part of the continual diabetic state, and for that reason merely a complicating factor. interestingly, one look tested how chronic hyperglycemia differed from brief hyperglycemia in useful outcomes in addition to mortality. while hyperglycemia was a gift at baseline and 24 hours after admission, it was inversely related to neurologic development within the first 7 days, 30-day functional outcome, and 90-day negligible dependence at the same time, persistent hyperglycemia was positively associated with increased mortality at 90 days, and parenchymal hemorrhage. When hyperglycemia was absent at baseline but present 24 hours after admission, it was likewise inversely associated with 90-day negligible dependence and was positively associated with death and parenchymal hemorrhage. In this study, baseline hyperglycemia alone (without persistence at 24 h) was not associated with poor outcomes. These data suggest that it may not be the stress response hyperglycemia that causes damage in acute stroke settings. Intensive treatment of hyperglycemia may be associated with improved outcomes, as demonstrated in the cardiac literature for MIs. A small pilot study found that hyperglycemic patients could be treated with insulin infusions safely, but the numbers were too small to compare the functional outcomes at 1 month. The use of insulin drips in another study to maintain glucose levels at 5.0 – 7.2 mmol/L (90 – 130 mg/dL) in patients with acute ischemic stroke, started no later than 12 h after the onset of symptoms, was associated with a trend towards better functional outcomes and minimal or no neurologic symptoms as measured by the National Institutes of Health (NIH) stroke scale. There were hypoglycemic episodes in the group treated with continuous infusion, but the majority of the patients were asymptomatic. However, further studies on this subject are required.
Hyperglycemia, as defined by serum glucose > 400 mg/dL, was a contraindication for inclusion in the NINDS trial for some of the reasons above, as well as that extreme hyperglycemia, can cause focal neurologic deficits that mimic stroke. Current guidelines recommend starting aggressive glycemic control if serum glucose is > 200 mg/dL while acknowledging that levels A level > 140 – 185 mg/dL may be harmful. While it may be reasonable to attempt to reduce the glucose level and determine whether any focal symptoms improve or resolve, and then treat with bio-lysis if no improvement is seen, this approach has yet to be tested. In terms of oral hypoglycemics in the acute stroke setting, one study looked at the role of sulfonylureas taken pre-stroke and during acute hospitalization. The effect of sulfonylureas on ATP-sensitive Kir6.2 potassium channels, which are regulated by the sulfonylurea receptor 1 (SUR1) receptor, such as pancreatic β-cells, which are open only during ischemic episodes, causing cell death. Theoretically, then, treatment with sulfonylureas is neuroprotective during ischemia. Although the numbers were small, and patients with more severe strokes (NIH stroke scale greater than 9) were excluded, patients on medication were more likely to have a decrease of four points on the NIH stroke scale or a score of 0 and were more likely to achieve excellent functional recovery at discharge. This effect was particularly noticeable in the non-lacunar stroke cases.
Further, care for the acute stroke patient is best handled in a certified ed stroke unit, with multidisciplinary care from a team consisting of vascular neurologists, stroke-trained registered Nurses, physical therapists, occupational therapists, and speech and swallowing specialists. This resulted in a 25% reduction in mortality. BP management in acute ischemic stroke is a topic of ongoing debate. gift-day thinking though helps the idea of permissive High blood strain within the Ave peri-stroke the duration. maximum vascular neurology lists would possibly allow the blood pressure to remain untreated until the systolic BP rises > 220 mmHg or diastolic BP > 120 mmHg. The period over which permissive hypertension has to be allowed is controversial. Generally, BP is left untreated for 3–5 days after stroke [69]. The general public with clinical complications after stroke has a disability associated with neurologic deficits. Consequently, deep venous thrombosis (DVT) and aspiration pneumonitis are two complications that stroke patients want to prevent. Prevention of DVT is achieved via subcutaneous anticoagulation with heparin or low-molecular-weight heparin with or without external compressive devices. Treatment initiation is commonly performed immediately upon admission, irrespective of infarct size. One unblinded examination examined heparin as opposed to enoxaparin and determined a discount in thrombosis with low molecular weight heparin. Prevention of aspiration is complex. Protection of the airway is often compromised in the acute period after stroke. Not unusual suctioning and positioning allow you to save your aspirations.
Swallow critiques should be undertaken before oral vitamins are initiated in any affected person in whom dysphagia is suspected. Placement of nasogastric tubes (NGT) is often required for nutrients, and patients frequently require percutaneous endoscopic gastrostomy (PEG) tubes for prolonged provision of vitamins. Hydration is vital, both intravenously earlier than the enteral entry is set up, or through NGT or PEG tubes to prevent dehydration and electrolyte abnormalities. Antibiotics need to be started in any patient suspected of having contamination, and the fever has to set off a competitive look for a source. Hyperthermia itself causes neurological deterioration, and antipyretic should be administered.
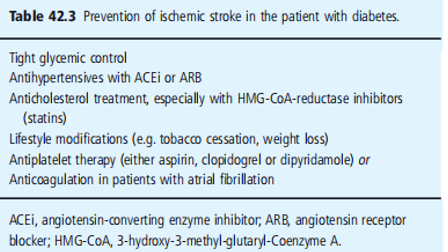
Secondary prevention of stroke in diabetes the management of patients with diabetes after stroke was similar to that of primary prevention, as outlined above (Table 42.3).
The seventh report of the Joint National Committee on the Prevention and Treatment of Hypertension recommends that people with diabetes should be maintained a BP < 130>
In sufferers who've had ischemic stroke secondary to extract cranial carotid stenosis, carotid endarterectomy remains the desired treatment of choice for carotid artery stenosis extra than 70% (figure 40.3). For levels of stenosis of 50% – 70%, the benefits of surgery are a good buy smaller, and choices to deal with will rely on the trouble rate at close by institutions. Carotid artery stenting for symptomatic carotid artery stenosis is still being studied. to date, except there is a huge hazard of going through the surgical operation, together with clinically massive cardiac disease or pulmonary disease, contralateral carotid artery occlusion, or records of preceding radical neck surgical treatment or neck radiation remedy, carotid endarterectomy remains maximum desirable. In such excessive-risk situations, carotid artery stenting is not as accurate as surgical treatment.
Diabetes on my own is not always sufficient to categorize an affected person as a high danger.
People with diabetes and atrial inflammation, paroxysmal or in any other case, have to be anti-coagulated with warfarin to a purpose international Normalized Ratio (INR) of 2.0 – 3.0. The danger discount associated with anticoagulation treatment was 68%, with an absolute danger discount in the annual stroke charge ranging from 4.5% to 1.4%. This risk reduction is so strong that one takes a look at the anticipated that an affected character should fall 295 times in an unmarried 12 months for the chance of subdural hematoma secondary to trauma to outweigh the benefits of anticoagulation. There is no reason to assume that is distinct for patients with diabetes.
Research Method:
This study aimed to investigate the risk factors related to cerebrovascular ailments in a population-based total sample. A total of 1,000 contributors elderly 50-seventy-five years were randomly selected from numerous communities. Comprehensive medical opinions and interviews were conducted to accumulate facts on demographic traits, medical history, lifestyle factors, and laboratory measurements related to cerebrovascular ailment. The individuals were followed up for 5 years to evaluate the incidence of cerebrovascular events.
Result:
a few participants, a hundred and fifty advanced cerebrovascular diseases throughout the observation period. The occurrence rate was 15%, with a higher prevalence in men (62%) than in girls (38%). Statistical analysis revealed numerous threat factors associated with cerebrovascular sickness. These included age > 65 years, hypertension, diabetes, smoking, weight problems, and a sedentary lifestyle. The strongest predictor was hypertension, with members with hypertension displaying a threefold increase in cerebrovascular disorder threat compared to those without hypertension.
Discussion:
The results of this study verify the properly mounted chance elements for cerebrovascular ailments, namely age, hypertension, diabetes, smoking, obesity, and physical state of no activity. These findings are consistent with previous research, further validating the importance of addressing these modifiable threat factors in each of the number one and secondary prevention techniques.
The high incidence of cerebrovascular sickness among adult males warrants further research into capability gender-related variations in chance profiles and healthcare utilization. Additionally, the affiliation between a sedentary lifestyle and cerebrovascular disease emphasizes the importance of selling normal bodily activities as a part of complete prevention efforts.
While this study provides valuable insights into the risk elements related to cerebrovascular disorders, it is not always without limitations. The sample length and compliance with-up duration will be prolonged to improve generalizability and capture the long-term consequences. Moreover, the study depended on self-reported data for lifestyle elements, which might introduce take into account bias.
Conclusions:
Diabetes is a significant risk factor for ischemic stroke. Patients with diabetes who experience stroke tend to have more excessive signs and symptoms and worse consequences than those without diabetes. In addition, strokes in patients with diabetes are regularly difficult to deal with acutely. Although diabetes increases the likelihood of various stroke causes, the most common type observed in patients with diabetes is lacunar microvascular infarction. To prevent stroke in patients with diabetes, it is vital to actively manage concurrent excessive blood pressure and hyperlipidemia. Although cautious glycemic management may reduce the threat of stroke, the importance of hazard discounts is not as stated. Antiplatelet remedies play a critical role, and a single anti thrombotic agent is sufficient for ischemic stroke prevention. Hyperglycemia all through the acute segment following an ischemic stroke is related to poorer outcomes, and in-depth management might also enhance functional recovery, particularly in men.
Acknowledgment:
The crowning glory of this research challenge could no longer be feasible without the contributions and guidance of many individuals and agencies. we’re deeply grateful to all those who performed a position in the achievement of this mission We would also like to thank My Mentor Dr. Naweed Imam Syed Prof. Department of Cell Biology at the College of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their helpful input and guidance throughout this research. Their insights and understanding had been instrumental in shaping the direction of this challenge.
Declaration of interest:
I, at this second, declare that: I haven’t any pecuniary or another private hobby, direct or oblique, in any dependence that raises or can also boost a war with my duties as a supervisor of my workplace control.
Conflicts of Interest:
The authors declare that they have no conflicts of interest.
Financial support and sponsorship:
No Funding was received to assist with the preparation of this manuscript
References
- Tom T., Haase N., Rosamond W., Howard W.J., Rumsfeld J., (2006). Manolio the T and Other Facts on Coronary Heart Disease and Stroke - 2006 Update: Report at the Commission on the Facts of Belonging to Cardiovascular Diseases Stroke Facts Subcommittee. 113: e85 - e151.
View at Publisher | View at Google Scholar - Heron MP, Hoyert DL, Xu J, et al. (2004). Mortality: Preliminary information for 2006 National Critical Spokesperson for 2008 Statistics; 56: 16. 3.
View at Publisher | View at Google Scholar - Rothwell PMs, Coull AJ, Giles MF, Howard SC, Silver LE, et al. (2004). Changes in stroke prevalence, mortality, fatality, severity, and risk factors in Oxfordshire, England from 1981 to 2004 (Oxford Vascular Research). Lancet. 363: 1925–1933.
View at Publisher | View at Google Scholar - Thorvaldsen P, Asplund ok, Kuulaasma ok, Rajakangas AM, Shroll M. (1995). Stroke prevalence, mortality, and mortality from WHO MONICA Mission: Global fitness company, trend tracking and Determinants of cardiovascular disease. Stroke; 26: 361-367.
View at Publisher | View at Google Scholar - Wolf P.A., D'Agostino R.B., Belanger A.J., Kannel V.B. (1991). Opportunity Go: Take a look at Framing Ham's random profile. Stroke; 22: 312-318.
View at Publisher | View at Google Scholar - Rodriguez B.L., D'Agostino R., Abbott R.D., Kagan A., Berchfi el K.M., et al. (2002). Risk of in-hospital stroke in men: Explore heart disease programs in Honolulu and Framingham. Stroke; 33: 230-236.
View at Publisher | View at Google Scholar - Kissela B.M., Khoury J., Kleindorfer D., Wood D., Schneider A., et al. (2005). Epidemiology of Ischemic Stroke in Diabetic Patients: There are Cincinnati and Northern Kentucky strokes. Diabetes Departed in; 28: 355-359.
View at Publisher | View at Google Scholar - Sacco RL, Boden-Albala B., Abel G., Lin I.F., Elkind M., et al. (2001). Racial and Ethnic Differences in the Impact of Stroke Risk Factors: Take a look at the North Big Apple Punch. Stroke; 32: 1725-1731.
View at Publisher | View at Google Scholar - Almdal T., Sharlik H., Jensen A.S., Vestergaard H. (2004). Fair Type 2 diabetes is associated with coronary artery disease, stroke, and death. Arch Intern Med; 164: 1422-1426.
View at Publisher | View at Google Scholar - Tuomilehto J, Rasteni D, Jousilahti P, Sarti K, Vartiiainen E. (1996). Diabetes as a Cause of Stroke Death: An Opportunity Finnish middle-aged census. Stroke; 27: 210- 217.
View at Publisher | View at Google Scholar - Davis B.R., Vogt T., Frost P.H., Burlando A., Cohen J., et al. (1998). Stroke risk factors and stroke types in isolated people Systolic Hypertension: Systolic Hypertension in the Elderly Joint research organization. Stroke; 29: 1333-1340.
View at Publisher | View at Google Scholar - Grau A.J., Weimar K., Buggle F., Heinrich A., Gertler M., et al. (2001). Risk Factors, Outcome and Treatment of ischemic subtypes Stroke: German Stroke Fact Bank. Stroke; 32: 2559-2566.
View at Publisher | View at Google Scholar - Labovitz D.L., Boden-Albala B., Hauser V.A., Sakko R.L. (2007). Lacunar infarction or deep intracerebral hemorrhage: who gets what? northern Manhattan prosecutor. Neurology; 68: 606-608.
View at Publisher | View at Google Scholar - Horowitz D.R., Turim S., Weinberger J.M., Rudolf S.H. (1992). Mechanism with Lacunar Infarction. Stroke; 23: 325-327.
View at Publisher | View at Google Scholar - Elmore EM, Mosquera A, Weinberger J. (2003). The prevalence of asymptomatic intracranial large-vessel occlusive disease: the function of diabetes. J Neuro Imaging; 13: 224-227.
View at Publisher | View at Google Scholar - Weinberger J., Becerra V., Weisberg M.K., Jacobson J.H. (1983). Factors contributing to the occurrence of stroke in patients with atherosclerosis Vascular: location of diabetes. Stroke; 14: 709-712.
View at Publisher | View at Google Scholar - Johnston SC, Rothwell PM, Nguyen-Huynh MN, Giles MF, Elkins JS. et al. (2007). Checking and correcting estimates for forecasting Very early risk of stroke after transient ischemic attack. Lancet; 369: 283-292.
View at Publisher | View at Google Scholar - Movahed M., Hashemzadeh M., Jamal M.M. (2005). Diabetes mellitus is a strong unbiased threat of atrial fibrillation and flutter. to other cardiovascular diseases. International Cardiologist; 105: 315–318.
View at Publisher | View at Google Scholar - Sacco R.L., Adams R., Albers G., Alberts M.J., Benavente O., et al. (2006). Recommendations for stroke prevention in patients with ischemic disease Stroke or Transient Ischemic Attack: A Statement from the American Heart Association/American Stroke Medical Professional Council of Stroke Associations. Stroke; 37: 577-617.
View at Publisher | View at Google Scholar - Gage BF, Waterman ad, Shannon W, Boechler M, Rich MW, et al. (2001). Validation of medical classification schemes for predicting stroke: consequences from the National Registry of Atrial traumatic inflammation. JAMA; 285: 2864–2870.
View at Publisher | View at Google Scholar - Rietbrock S, Heeley E, Plumb J, van Staa T. (2008). Chronic atrial fibrillation: prevalence, occurrence, and prediction of stroke using the congestive coronary heart failure, hypertension, age > 75, diabetes mellitus, and earlier stroke or brief ischemic attack (CHADS2) threat stratification scheme. Am Heart J; 156: 57–64.
View at Publisher | View at Google Scholar - Feldmann E, Broderick JP, Kernan WN, Viscoli CM, Brass LM, et al. (2005). Essential threat elements for intracerebral hemorrhage in the young are modifiable. Stroke; 36: 1881–1885.
View at Publisher | View at Google Scholar - Selvin E, Coresh J, Shahar E, Zhang L, Steffes M, et al. (2005). Glycemia (hemoglobin A1c) and incident ischaemic stroke: the Atherosclerosis risk in communities (ARIC) looks at. Lancet Neurol; 4: 821–826.
View at Publisher | View at Google Scholar - Myint PK, Sinha S, Wareham NJ, Bingham SA, Luben RN, et al. (2007). Glycated hemoglobin and chance of stroke in human beings without known diabetes inside the European prospective research into most cancers (EPIC) - Norfolk prospective population look at a threshold relationship? Stroke; 38: 271–275.
View at Publisher | View at Google Scholar - Folsom AR, Rasmussen ML, Chambless LE, Howard G, Cooper LS, et al. (1999). Prospective institutions of fasting insulin, body fat distribution, and diabetes with the threat of ischemic stroke. Diabetes Care; 22: 1077–1083.
View at Publisher | View at Google Scholar - Lindenstr ø m E, Boysen G, Nyboe J. (1993). Threat factors for stroke in Copenhagen, Denmark. II. lifestyles fashion factors. Neuro epidemiology; 12: 43–50.
View at Publisher | View at Google Scholar - Rexrode KM, Hennekens CH, Willett WC, Colditz GA, Stampfer MJ, et al. (1997). A prospective study of frame mass index, weight change, and risk of stroke in girls. JAMA; 277: 1539–1545.
View at Publisher | View at Google Scholar - Kurl S, Laukkanen JA, Niskanen L, Laaksonen D, Sivenius J, et al. (2006). Metabolic syndrome and the threat of stroke in center-aged men. Stroke; 37: 806–811.
View at Publisher | View at Google Scholar - McNeil AM, Rosamond WD, Girman CJ, Golden SH, Schmidt MI, et al. (2005). The metabolic syndrome and 11 - yr hazard of incident cardiovascular disorder in the Atherosclerosis risk in groups study. Diabetes Care; 28: 385–390.
View at Publisher | View at Google Scholar - Air EL, Kissela BM. (2007). Diabetes, metabolic syndrome, and ischemic stroke. Diabetes Care; 31: 3131–3140.
View at Publisher | View at Google Scholar - Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE. (1997). Not unusual carotid intima-media thickness and danger of stroke and myocardial infarction: the Rotterdam look at. Circulate. 96: 1432–1437.
View at Publisher | View at Google Scholar - Tsivgoulis G, Vemmos okay, Papamichael C, Spengos K, Manios E, et al. (2006). Common carotid intima-media thickness and the danger of stroke recurrence. Stroke; 37: 1913–1916.
View at Publisher | View at Google Scholar - Wagenknecht LE, D’ Agostino R Jr, Savage PJ, O’ Leary DH, Saad MF, et al. (1997). period of diabetes and carotid wall thickness: the Insulin Resistance Atherosclerosis examination. Stroke; 28: 999–1005.
View at Publisher | View at Google Scholar - Matsumoto okay, Sera Y, Nakamura H, Miyake S. (2002). Correlation between not unusual carotid artery wall thickness and ischemic stroke in sufferers with kind 2 diabetes mellitus. Metabolism; 51: 244–247.
View at Publisher | View at Google Scholar - Chlumsky J, Charvat J. (2006). Echocardiography and carotid sonography in diabetic sufferers after cerebrovascular assaults. J Int Med Res; 34: 689–694.
View at Publisher | View at Google Scholar - Taffi R , Nanetti L , Mazzanti L , Bartolini M , Vignini A , et al. (2008). Plasma degrees of nitric oxide and stroke final results. J Neurol; 255: 94–98.
View at Publisher | View at Google Scholar - Nazir FS, Alem M, Small M, Connell JM, Lees KR, et al. (2006). Blunted reaction to systemic nitric oxide synthase inhibition in the cerebral flow of sufferers with type 2 diabetes. Diabet Med; 23: 398–402.
View at Publisher | View at Google Scholar - Laufs U, Endres M, Stagliano N, Amin - Hanjani S, Chui DS, et al. (200). Neuro protection is mediated by using changes in the endothelial actin cytoskeleton. J Clin makes investments; 106: 15–24.
View at Publisher | View at Google Scholar - Plehn JF, Davis BR, Sacks FM, Rouleau JL, Pfeffer MA, et al. (1999). Reduction of stroke prevalence after myocardial infarction with pravastatin: the cholesterol and Recurrent events (CARE) look at. Stream; 99: 216–223.
View at Publisher | View at Google Scholar - Sever PlayStation, Dahl ö f B, Poulter NR, Wedel H, Beevers G, et al. (2003). Prevention of coronary and stroke events with atorvastatin in hypertensive patients who've common or decreased-than-average cholesterol concentrations within the Anglo - Scandinavian Cardiac effects Trial – Lipid reducing Arm (ASCOT - LLA): a multicenter randomized controlled trial. Lancet; 361: 1149–1158.
View at Publisher | View at Google Scholar - Amarenco P, Bogousslavsky J, Callahan a third, Goldstein LB, Hennerici M, et al. (2006). High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med; 355: 549–559.
View at Publisher | View at Google Scholar - Aoki I, Shimoyama okay, Aoki N, Homori M, Yanagisawa A, et al. (1996). Platelet - Structured Thrombin Era in Sufferers with Diabetes Mellitus: Effects of Glycemic Control on Coagulability in Diabetes. J Am Coll Cardiol; 27: 560–566.
View at Publisher | View at Google Scholar - Yamada T, Sato A, Nishimori T, Mitsuhashi T, Terao A, et al. (2000). Significance of hyper coagulability over hyperglycemia for vascular complications in kind 2 diabetes. Diabetes Res Clin Pract; 49: 23–31.
View at Publisher | View at Google Scholar - Serebruany VL, Malinin A, Ong S, Atar D. (2008). Sufferers with metabolic syndrome showcase better platelet interest than those with conventional danger elements for vascular illness. J Thromb Thrombolysis; 25: 207–213.
View at Publisher | View at Google Scholar - Angiolillo DJ , Fernandez - Ortiz A , Bernardo E , Ram í rez C , Sabat é M , et al. (2005). Platelet characteristic profiles in patients with type 2 diabetes and coronary artery sickness on blended aspirin and clopidogrel remedy. Diabetes; 54: 2430–2435.
View at Publisher | View at Google Scholar - Fisher CM. (1969). The arterial lesions underlying lacunes. Acta Neuropathology; 12: 1–15.
View at Publisher | View at Google Scholar - Fisher CM. (1978). Thalamic pure sensory strokes: a pathologic examination. Neurology; 28: 1141–1144.
View at Publisher | View at Google Scholar - Fisher CM. (1979) Capsular infarcts. Arch Neurol; 36: 65–73.
View at Publisher | View at Google Scholar - Chester EM, Agamanolis DP, Banker BQ, Victor M. (1978). Hypertensive encephalopathy: a clinicopathologic observation of 20 cases. Neurology; 28: 928–939.
View at Publisher | View at Google Scholar - Rosenberg EF. (1940). The thoughts in malignant high blood pressure: a clinicopathologic have a observe. Arch Neurol; 65: 545.
View at Publisher | View at Google Scholar - Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, et al. (2005). In-depth diabetes remedy, and cardiovascular ailment in sufferers with kind 1 diabetes (DCCT). N Engl J Med; 353: 2643-2653.
View at Publisher | View at Google Scholar - UKPDS have a look at the group. (1998). Impact Of Extensive Blood-Glucose Manipulation with Metformin on Headaches in Obese Patients with Kind 2 Diabetes (UKPDS 34). Lancet; 352: 854–865.
View at Publisher | View at Google Scholar - Nissen SE, Wolski okay. (2007). Impact Of Rosiglitazone at The Risk of Myocardial Infarction and Loss of Life from Cardiovascular Causes. N Engl J Med; 356: 2457–2471.
View at Publisher | View at Google Scholar - Home PD, Pocock SJ, Beck - Nielsen H, Curtis PlayStation, Gomis R, et al; (2009). File has a Look at The Crew. Rosiglitazone Evaluated for Cardiovascular Effects in Oral Agent Combination Remedy for Kind 2 Diabetes (file): a multicenter, randomized, open-label trial. Lancet; 373: 2125–2135.
View at Publisher | View at Google Scholar - Wilcox R, Bousser MJ, Betteridge DJ, Schernthaner G, Pirags V, et al. (2007). Results of pioglitazone in sufferers with type 2 diabetes without or with preceding stroke: effects from PRO active (prospective Pioglitazone scientific Trial in Macro vascular occasions 04). Stroke; 38: 865–873.
View at Publisher | View at Google Scholar - UKPDS. (1998). Intensive Blood-Glucose Control with Sulfonylureas or Insulin as Compared with Traditional Remedies and The Chance of Complications in Sufferers with Kind 2 Diabetes (UKPDS 33). Lancet; 352: 837–853.
View at Publisher | View at Google Scholar - Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. (2008). 10 - yr observation - of extensive glucose manipulation in kind 2 diabetes. N Engl J Med; 359: 1577–1589.
View at Publisher | View at Google Scholar - Coronary Heart Results in Prevention Assessment Take a Look at Investigators. Consequences of an Angiotensin-Changing Enzyme Inhibitor, Ramipril, on Aerobic Vascular Occasions in High-Hazard-Patients. N Engl J Med; (2000). 342: 145–153.
View at Publisher | View at Google Scholar - Dahl ö f B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, et al. (2002). Cardiovascular morbidity and mortality inside the Losartan Intervention for Endpoint reduction in hypertension look at (lifestyles): a randomized trial in opposition to atenolol. Lancet; 359: 995–1003.
View at Publisher | View at Google Scholar - Gaede P, Lund - Andersen H, Parving HH, Pedersen O. (2008). Impact of a multifactorial intervention on mortality in kind 2 diabetes. N Engl J Med; 358: 580–591.
View at Publisher | View at Google Scholar - Antithrombotic Trialists’ Collaboration. (2002). Collaborative meta-evaluation of randomized trials of antiplatelet therapy for prevention of demise, myocardial infarction, and stroke in excessive chance patients. Br Med J; 324: 71–86.
View at Publisher | View at Google Scholar - Ridker PM, cook NR, Lee IM, Gordon D, Gaziano JM, et al. (2005). A randomized trial of low-dose aspirin within the number one prevention of cardiovascular ailment in women. N Engl J Med; 352: 1293–1304.
View at Publisher | View at Google Scholar - Latchaw RE, Yonas H, Hunter GJ, Yuh WT, Ueda T, et al. (2003). Recommendations and suggestions for perfusion imaging in cerebral ischemia: a scientific declaration for healthcare specialists using the writing institution on perfusion imaging, from the Council on Cardiovascular Radiology of the American coronary heart affiliation. Stroke; 34: 1094–1104.
View at Publisher | View at Google Scholar - National Institute of Neurologic Issues and Stroke Rt-PA Stroke examine institution. Tissue plasminogen activator for acute stroke. N Engl J Med; (1995). 333: 1581 – 1587.
View at Publisher | View at Google Scholar - Hacke W, Kaste M, Bluhmki E, Brozman M, D á value A, et al. (2008). Thrombolysis using alteplase 3-4.5 hours after acute ischemia steel. N Engl J Med; 359: 1317-1329.
View at Publisher | View at Google Scholar - Tandberg Askevold E., Nass H., Thomassen L. (2007). Predictors of recanalization after intravenous thrombolysis in acute stroke. J stroke Cerebrovascular Diss; 16:21-24.
View at Publisher | View at Google Scholar - Brown D.L., Johnston K.S., Wagner D.P., Hayley E.K. ml. (2004). Prediction Basics Improvement of Neurological Condition with Intravenous Administration of Recombinant Tissue Plasminogen Activator for Stroke Treatment. Stroke; 35:147 -150.
View at Publisher | View at Google Scholar - Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, et al. (1999). Intra-arterial urokinase in acute ischemic stroke. PROACT You are looking at a randomized controlled trial. Yama; 282: 2003-2011.
View at Publisher | View at Google Scholar - Adams HP, Del Zoppo G., Alberts MJ, Bhatt D.L., Brass L., et al. (2007). Recommendations for Early Treatment in Adults with Coronary Artery Disease Stroke: Yankee Heart Guiding Principle / American Style Stroke Council Stroke Association, Scientific Cardiology Council on Cardiovascular Radiology and Interventional Interventions, Atherosclerotic peripheral vascular disease and good care Impact on interdisciplinary operational enterprise research. Steel; 38: 1655–1711.
View at Publisher | View at Google Scholar - Arnold M, Schroth G, Nedeltchev K, Loher TJ, Stepper F, et al. (2002). Intra-arterial thrombolysis in 100 patients with acute stroke due to middle cerebral artery occlusion. Stroke; 33: 1828-1833.
View at Publisher | View at Google Scholar
