

Case Report | DOI: https://doi.org/10.31579/2834-5029/006
BUDD CHIARI SYNDROME: A Rare Medical Condition with Variable Outcome in Pregnancy- Case Report and Review of Literature
1Department of High-risk pregnancy and Perinatology, KIMSHEALTH, Trivandrum, India.
2Department of Obstetrics and Gynecology, KIMSHEALTH, Trivandrum, India
3Department of Medical Gastroenterology, KIMSHEALTH, Trivandrum, India
*Corresponding Author: Nina Navakumar, Department of High-risk pregnancy and Perinatology, KIMSHEALTH, Trivandrum, India
Citation: Navakumar N., Vijayalekshmi R, Ambat R., Vidyalekshmy R, Khan T., Kareem H. (2022) BUDD CHIARI SYNDROME: A Rare Medical Condition with Variable Outcome in Pregnancy- Case Report and Review of Literature. International Journal of Biomed Research. 1(2): DOI: 10.31579/2834-5029/006
Copyright: © 2022, Nina Navakumar, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 October 2022 | Accepted: 07 November 2022 | Published: 16 November 2022
Keywords: hepatic venous outflow; inferior vena cava; its pro-thrombotic
Abstract
BCS is a condition where there is obstruction to hepatic venous outflow due to thrombosis of the hepatic vein or inferior vena cava. The prevalence of BCS during pregnancy and puerperium ranges from 3.8 to 21.5% [1]. However, the incidence of pregnancy in a woman diagnosed with BCS is unknown due to its rarity. As BCS is commonly encountered in women of childbearing age group, pregnancy poses a challenge. Traditionally pregnancy was discouraged in these women due to its pro-thrombotic state. However, with the increased use of anticoagulation and decompressive procedures, successful pregnancy outcomes have been observed. Despite management of this condition with a multidisciplinary team, pregnancy outcome in our case was unfavourable. Recent studies showed that good maternal outcome could be achieved with current treatment modalities and close surveillance of BCS during pregnancy. The reported maternal outcomes in patients with treated and stabilized BCS are favourable, and foetal outcomes beyond 20 weeks gestation are good
Introduction
The currently accepted definition of primary BCS is hepatic outflow obstruction regardless of the cause or level of obstruction. BCS is characterized by hepatic venous outflow obstruction at any level from the small hepatic veins to the atriocaval junction [1]. According to the European Group for the Study of Hepatic Vascular Diseases, BCS is defined as HVOO at any level from the small hepatic veins to the junction of the IVC and the right atrium, regardless of the cause of the obstruction. Cardiac etiologies of hepatic congestion or veno-occlusive disease (sinusoidal obstruction syndrome) are not included in this definition. 0.2 and 2 per 1 million population in general population during the 3rd -4th decade with preponderance for females and 6.8 percent cases are associated with pregnancy and post partum [1]. High index of clinical suspicion is needed for diagnosis. Well defined guidelines are lacking for management in pregnancy.
Case Discussion
36-year-old Maldivian woman G4A3 with history of 3 first trimester abortions came at 19 weeks of gestation for second opinion of her ultrasound which showed early onset severe fetal growth restriction (-4 SD), echogenic bowel and oligohydramnios (Figure:1). She is a known case of chronic hypertension and Primary antiphospholipid syndrome with thrombocytopenia. On further evaluation she was diagnosed to have secondary Idiopathic thrombocytopenic purpura since 4 years and was on Tab Prednisolone 40 mg , she also had Type 2 diabetes mellitus since 4 years; sugars were controlled with oral hypoglycemic drugs. She was diagnosed with Budd Chiari Syndrome with inferior vena cava stenosis five years ago when she presented with abdominal distension and ascites. Inferior vena cava stenting was done at that time. She had one episode of pulmonary embolism diagnosed 2 years ago with CTPA when evaluated for sudden onset dyspnea ; managed with Rivaroxaban, LMWH and low dose aspirin along with inferior vena cava filter insertion and later on continued with warfarin anticoagulation.
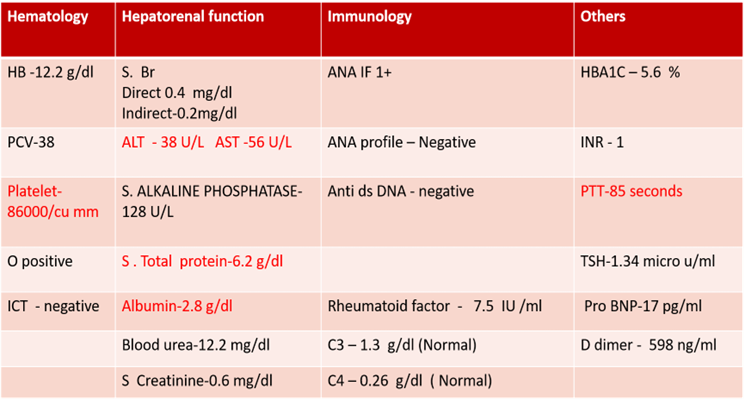
At time of first visit she had fatigue and dyspnea with slight limitation of physical activity since 6 months ( NYHA 2) . Investigation showed platelet of 81000 cells/mm3, liver function mildly deranged with Aspartate Transaminase – 56 IU/L and Alanine Transaminase – 38 IU/ML and lupus anticoagulant positive with prolonged APTT(Table:1). Ultrasound abdomen with doppler showed right hepatic vein thrombosis with normal sized liver and spleen and no ascites; Inferior vena cava filter in upper retro hepatic segment(Figure :2). Maternal echo showed features of pulmonary hypertension which could be due to recurrent thromboembolism. Warfarin changed to LMWH at 5 weeks of gestation.She was on therapeutic dose of low molecular weight heparin, oral Prednisolone 40 mg and Ecospirin 75 mg once daily, Metformin 500 mg, ἀ methyl dopa 500 mg and Nifedipine 10 mg(BP-140/90 mm Hg). After extensive counselling with multidisciplinary team approach including senior obstetrician, maternal-fetal medicine specialist, gastroenterologist, critical care specialist, hematologist ,rheumatologist, cardiologist and endocrinologist. Couple opted for medical termination of pregnancy in view of severe pulmonary artery hypertension and guarded fetal prognosis. LMWH changed to UFH 5000 and in Obstetric ICU with continuous cardiac monitoring MTP done with mifepristone and misoprostol .UFH stopped 6 hours prior to misoprostol and she expelled and abortus of weight 130gm. Placental histopathological examination did not show any abnormality and abortal karyotyping was also normal
Post MTP bleeding was within normal limits .Day 1 -Platelet count – 53000 / cumm . LFT – S. Direct Bilirubin – 1.2, Indirect Bilirubin- 0.6 ALT – 71 AST – 107 .LMWH was restarted after 4 hours of expulsion à 60 mg s/c Q24H. Day 2: Platelet count dropped to 37000 , hence LMWH 40 mg s/c Q24 H was given on alternate days .IV Methyl prednisolone pulse dose 1 g was given in view of falling platelet count. Inj Romiplostim 250 microgram s/c Q24H was also started . Day 3: Platelet count improved to 40,000. Day 5 she complained of acute onset of severe epigastric pain which was found to be non-specific . USS with doppler + CT angiogram did not show any new thrombus . Interventional radiologist opined for Venography if pain persists. Pain became symptomatically better with anlgesics and antacids . She discharged on Day 7 with Platelet count – 50000 on Prednisolone 40 mg od,Aspirin 75 mg ,Warfarin 3 mg od ,Inj LMWH 40 mg s/c Q24H ;and was reviewed with platelet count and PT-INR after 3 days and explained need for compliance of medications and long term follow up.



Discussion
Though BCS in pregnancy favourable outcome has been reported with a live birth rate of 75% in our case we had unfavourable outcome. We assume it could be due to multiple co-morbidities -hypertension , diabetes mellitus, immune thrombocytopenic purpura which were not with optimal control at time of conception, associated primary antiphospholipid syndrome which itself is associated with severe uteroplacental insufficiency, BCS itself was not in remission and was in advanced stage as she had pulmonary arterial hypertension as a life threatening complication at time of presentation . Hence we can infer from this case that optimal comorbidity control, multidisciplinary team input, BCS in remission without complications at time of conception , proper management of APS are warranted with maternal and fetal surveillance during pregnancy and postpartum. Also we need to emphasise on long tem follow up
Although a brief discussion of this clinical phenomenon first appeared in a book by Budd in 1845 , Lambron in 1842 is said to have reported the first case. In 1899, Chiari collected 10 cases and reported three personal cases and presented the first thorough clinicopathologic description of the syndrome, including the hypothesis that the underlying mechanism was endophlebitis of the hepatic veins. It presented with classical triad of abdominal pain, hepatomegaly and ascites. BCS is classified into primary due to endoluminal thrombosis and secondary due to external compression. BCS could be due to prothrombotic conditions like myeloproliferative diseases, thrombophilias, antiphospholipid antibody syndrome, paroxysmal nocturnal hemoglobinuria (PNH), Sjogrens syndrome, Sarcoidosis, Behcets disease, malignancy, sepsis, obesity, nephrotic syndrome , obesity or external compression due to tumor, hepatic cyts, blunt trauma [2].
Clinical features depends on anatomical site of thrombosis, etiology, speed of occlusion and severity of liver dysfunction [3]. BCS could be asymptomatic(6%), acute(41%), chronic(42%) or fulminant(8%). Investigation to find out the primary cause include USS abdomen with doppler, CT scan abdomen, MRI scan ,Hepatic venography and liver biopsy in selected cases [4]. Specific investigations include for myeloproliferative disorder – Janus tyrosine kinase-2 mutation in granulocytes of peripheral blood, CALR mutation testing if JAK 2 negative, bone marrow biopsy if both are negative ;thrombophilia screen which includes APLA screening ; for PNH- flow cytometry of peripheral blood cells for CD 55 and CD 59 deficient clones; discovery of a single risk factor should not preclude the testing for others ; thromboelastography to detect hypercoagulability even if specific defects are not found. Management includes multidisciplinary care and treating the underlying condition .Treatment modalities mainly include therapeutic anticoagulation , percutaneous angioplasty with stenting , decompression by trans jugular intrahepatic portosystemic shunting (TIPS)/ non-shunt surgeries and liver transplantation. Classical BCS patients commonly undergo TIPS (classical BCS: 4%62% vs HVC- BCS: 1%-4.5%) and liver transplantation (9%-55% vs 0%1%) [1]. Trans jugular intrahepatic portosystemic shunting (TIPS) is an artificial connection within the liver between the inflow portal vein and the outflow hepatic vein. It has lower morbidity and mortality rate than surgery and hence is a preferred approach; adopted as first step in patients who initially present with acute hepatic failure [6]. Liver transplantation is the only treatment available in fulminant form and is done if patient worsens despite aggressive medical and radiological therapy [7].Prognosis depends on liver and renal dysfunction; with treatment BCS has 75% survival at 5 years [8].
BCS in pregnancy
It could be a new diagnosis or pre-existing disease . New onset BCS in pregnancy presents as an acute disorder with hepatic vein obstruction. Acute major venous obstruction results in rapid deterioration with portal hypertension , variceal bleeding and fulminant hepatic failure . Delay in diagnosis or treatment results in irreversible liver damage and high mortality rate [9]. Managementin pregnancy needs multi disciplinary input. One-fifth women with Budd-Chiari syndrome (BCS) have primary infertility and hence conceive when BCS is treated [9]. BCS cannot be considered a contraindication to pregnancy in stable patients with a well controlled disease. The reported maternal outcomes in patients with treated and stabilized BCS are favourable, and foetal outcomes beyond 20 weeks gestation are good but still we have to counsel about persistent risks of severe exacerbation during pregnancy. Patients with known varices or portal hypertension need a pre pregnancy gastroscopy to assess severity.
Maternal effects include intra hepatic cholestasis pre eclampsia , abruption ,post partum hemorrhage [10] .Maternal mortality is not reported to be increased in controlled disease, but morbidity increase.Fetal effects like prematurity,fetal growth restriction,fetal distress,still birth can be due to poor control of underlying prothrombotic disorders [7] and uteroplacental insufficiency .
Treatment consists of therapeutic dose of anticoagulation (heparin), low dose aspirin prophylaxis against pre-eclampsia , continue pregnancy safe drugs. In ever visit specifically ask and look for signs and symptoms of flare of BCS .Warfarin > 5mg need to be changed to LMWH at the earliest, not later than 6 weeks. Medical Gastroenterology follow up every 4 weeks and monthly full blood count ,liver function test ,coagulation screen Antepartum surveillance includes serial growth scans from 24 weeks, watch for hypertension ,OGD for variceal surveillance during second trimester. Endoscopic variceal ligation is the treatment of choice in pregnancy if indicated for oesophageal varices and also ẞ blockers like propranalol and nadolol can be used in pregnancy. Patients with TIPS need regular abdominal ultrasound to ensure patency every 4 weeks. Birth plan to be given at 32- 34 weeks with MDT input from – Senior obstetrician, maternal -fetal medicine specialist, gastroenterologist, hematologist, critical care specialist, anesthetist ,neonatologist and other specialities as indicated. Intrapartum management includes to stop LMWH 24 hours before and UFH 12 hours of planned induction or regional anesthesia .Continuous fetal monitoring.Cut short second stage with assisted vaginal delivery [7] and we need to avoid methyl ergometrine Cesarean section to be considered for obstetric indications / large esophageal varices due to risk of bleeding and thrombosis. Special precautions to be taken in patients with portal hypertension due to large pelvic venous collaterals and postoperative ascites .Vascular surgery team should be involved .Literature review though not much shows there is increase rate of cs (70%) and live birth rate is approximately 62.5 % [11]. Postpartum periods also needs continued monitoring to avoid dehydration , early mobilization and intermittent pneumatic compression stockings . Therapeutic anti coagulation can be restarted 6 hours after vaginal delivery and 12 hours of CS ;LMWH can be bridged with warfarin until INR 2-3 achieved and emphasise on long term follow with gastroenterologist and haematologist. Appropriate contraceptive options include Copper intrauterine contraceptive devices, progesterone only contraceptives.
Conclusion
Managing pregnancy with BCS is a challenge. Close monitoring, adequate anticoagulation, monitoring of fetal growth and the liver condition along with a multidisciplinary approach lead to successful outcomes.
References
- Budd-(2020) 481 Lamia Y.K. Haque, Joseph K. Lim et al Chiari Syndrome An Uncommon Cause of Chronic Liver Disease that Cannot Be Missed Clin Liver Dis 24 453–
View at Publisher | View at Google Scholar - (2009) Pregnancy in women with known and treated Budd–Chiari syndrome: Maternal and fetal outcome Journal of Hepatology 51 47-54
View at Publisher | View at Google Scholar - Lamia Y.K. Haque, Joseph K. Lim; (2020) Budd-Chiari Syndrome An Uncommon Cause of Chronic Liver Disease that Cannot Be Missed Clin Liver Dis 24 453–481
View at Publisher | View at Google Scholar - Current knowledge in pathophysiology and management of Budd-Chiari syndrome and non-cirrhotic non-tumoral splanchnic vein thrombosis – Seminar Journal of Hepatology
View at Publisher | View at Google Scholar - In the INSPIRE collaboration study
View at Publisher | View at Google Scholar - (2019) Current knowledge in pathophysiology and management of Budd-Chiari syndrome and non-cirrhotic non-tumoral splanchnic vein thrombosis – Seminar Journal of Hepatology Feb
View at Publisher | View at Google Scholar - Faisal Khan, Ian Rowe, (2017) Outcomes of pregnancy in patients with known Budd-Chiari syndrome Observational study Bill Martin World J Hepatol July 28; 9(21): 945-95
View at Publisher | View at Google Scholar - Lamia Y.K. Haque, MD, MPHa (2020) Budd-Chiari Syndrome An Uncommon Cause of Chronic Liver Disease that Cannot Be Missed Clin Liver Dis 24 453–481
View at Publisher | View at Google Scholar - Weirong Ren, Liang LI (2015) Prevalence of Budd-Chiari Syndrome during Pregnancy or Puerperium: A Systematic Review and Meta-Analysis Hindawi Publishing Corporation Gastroenterology Research and Practice Volume, Article ID 839875.
View at Publisher | View at Google Scholar - (2016) Waltraut M. Merz, MD, PhD, Anna M. Ru¨land, MD, Valeria Hippe. Medicine CLINICAL CASE REPORT Pregnancy in Budd-Chiari Syndrome Case Report and Proposed Risk Score
View at Publisher | View at Google Scholar - (2022), March, Weigers et al Pregnancy outcomes in women with Budd–Chiari syndrome or portal vein thrombosis – a multicentre retrospective cohort study, BJOG Volume 129, Issue 4
View at Publisher | View at Google Scholar
