

Research Article | DOI: https://doi.org/10.31579/2834-8427/003
Attempts at Improving Maternal, Neonatal Outcome with Megathaimine
- S. Chhabra *
Obstetrics Gynaecology, Mahatma Gandhi Institute of Medical Sciences, India
*Corresponding Author: S. Chhabra, Obstetrics Gynaecology, Mahatma Gandhi Institute of Medical Sciences, India
Citation: S. Chhabra (2022). Attempts at Improving Maternal, Neonatal Outcome with Megathaimine. J. of Clinical Gynaecology and Breast. 1(1); DOI:10.31579/2834-8427/003
Copyright: © 2022 S. Chhabra, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 September 2022 | Accepted: 23 September 2022 | Published: 05 October 2022
Keywords: megathiamine; maternal neonatal; outcome advantages disadvantages
Abstract
Background
Various micronutrients are needed in pregnancy for growth of baby, preventionof disorders which affect mother and baby. Thiamineis one such micronutrient. Pregnantwomen have greaterrisk of deficiency. Research continues.
Objectives:
Study was conducted to know effects of high dose Thiamine ‘Megathiamine’ for prevention of pregnancy specific disorders, better maternal neonatal outcome so as to be able to use knowledge for maternal - neonatal health promotion even with limited resources as Thiamine does not cost much.
Material Methods
Study subjects were women with 14±2 weeks pregnancy who presented for prenatal care, had no medical, obstetric disorder at inclusion in study, no contraindication to Thiamine. End point was one week beyond birth. Study subjects,1200 women were divided into two Groups A, B. Each arm with 600 women was given Megathiamine or Placebo in triple blinded way. Women who received Megathiamine or Placebo (known only to pharmacologist not part of care providers ) were followed, up to one week post birth till there were 500 births in each arm .
Results
After completion of study and analysis of results, decoding revealed that anaemia was almost in double numbers in women who received Megathiamine than those who received Placebo(10 vs 5), Oligohydramnios, Fetal Growth Restriction(FGR) and Hypertensive Diseasesof Pregnancy (HDsP) were not different in both groups.In Megathaimine grouppreterm births and LBW were more than placebo 55 (38.4Percentage) vs 44 (33.88Percentage), respectively in Megathaimine, placebo groups. Admissions to Neonatal Intensive Care Unit (NICU) were more is Megathaimine group comparedto Placebo (45 (0.9Percentage) vs 23 (4.6Percentage).
Conclusion
Present study revealedthat Megathiamine had no benefitto mother or baby. Excessof Thiamine lead to ill effects in mothers, babies
Background
Various micronutrients are needed in pregnancy, not only for growth of the baby, but also for prevention of some pregnancy specific disorders which affect the mother as well as the baby. However pregnantwomen have greaterrisk of deficiencies.
So it is essential to know and supplement if the need be.
Thiamine is one such micronutrient needed for the mother as well as the baby. Thiamine is present in most multivitamin pills in a balanced way. In some places Thiamine is found in fortified grains such as cereals and bread, as well as Pasta, Legumes and Berries.
Thiamine mononitrate (Vitamin B1) is one of several nutrientswhich help in the functioning of the nervous system.
However Thiamine requirement is more duringpregnancy, specially during the third trimester of pregnancy, because of its sequestration by the foetus and placenta and the need during lactation (Butterworth,2001). The recommended daily intake of Thiamine for a pregnantwoman is 1.4 milligrams. The extra vitamin contributes not only to the mother’s nervous system, heart and muscle function, but also to unborn baby. In addition, Thiamine helps the pregnantwomen maintain their energy. Thiaminedeficiency may lead to pretermlabor or pretermprelabour rupture of membranes [PPLROM],hypertensive disorders of pregnancy (HDsP), Placental abruption etc (Aya mousa 2019).
Years back Borle(1981) reported low blood cell Thiamine concentration in mothers who had severe fetal growth restriction (FGR).
However in a study, it was revealed that, despite the high incidence of Thiamine deficiency in the Karenmothers, breast milk, Thiamine concentrations remainedwithin normal limits, suggesting preferential delivery of Thiamine to the milk at the expense of the mother (McGready, 2001). Earlier researchers recorded two fold higher concentrations of Thiamine and other water-soluble vitamins in umbilical cord blood than in maternal blood (Baker,1975). So research continues.
Objectives
Present study was conducted to know the effects of high dose Thiamine, Megathaimine in prevention of pregnancy specific disorders, best of maternal neonatal outcome and use the knowledge for trying best of maternal neonatal health even with limited resources.
Material Methods
The institute’s ethic’s committee’s approval was taken before initiation of study. Study subjects were women who presented with 14±2 weeks pregnancy for prenatal care and had no medical or obstetric disorder at the time of inclusion, no contraindications to Thiamine and plans to deliver at the study site. Consent was taken. Eligible women were given information about the study. Sufficient number of women were included to know the effects of supplement being given. End point was one week beyond birth. Study subjects were divided into cases and controls, and given Megathiamine or placebo in a triple blinded way. The woman, the drug provider, the investigator did not know which woman received Megathiamine and which one received placebo. Women were asked to take look alike capsules containing either Megathiamine or placebo filler with identity known only to the Pharmacologist who was keeping a confidential record of the code which was revealed to the research team after completion of the analysis of
the outcome of all the cases not knowing which were study or controls, which ever that could have been. Nothing was put on informed consent other than a vitamin capsule. Women took supplement capsule every day until one week after delivery. They were asked to bring their capsule containers during each antenatal visit. Treatment compliance was checked by the research assistant at 16, 20, 24, 28, 32 and 36-weeks antenatal visits and admission for birth by reviewing the woman's records, direct questioning and counting the number of remaining capsules. All events of the mothers during pregnancy and birth, including adverse outcome in the mothers and the babies were recorded. Baby’s birth weight and indication of admission to neonatal intensive care unit (NICU), if any, were also recorded. Any study subject could withdraw from the study at any stage of the trial and no further study medication was given. Similarly the researchers were also at liberty to drop a woman from the trial before completion of the study, if it was considered advisable because of non-compliance to advice or any other reason. Research assistant was also not part of the service providing team.
Of the total 1450 pregnant women registered, 1200 became study subjects as per the inclusion and exclusion criteria and received vitamin or placebo after getting divided into two groups, Group A and Group B. After this stage there were two arms with 600 women in each, arm keeping in mind the drop outs at various stages. After investigations 11 from A and 21 from B were excluded from the study as they were found to have medical disorders. All 1200 women who received capsules were followed, till there were 500 births in each arm. However after inclusion in between in Group A, 67 were lost to follow up and 522 women came for regular follow-up. Similarly in Group B, 59 were lost to follow-up and 520 pregnant women came for regular follow-up (Table I).
Registered 1450 excluded 250, at entry with inclusion criteria | Drug A | Drug B | |||
| No | % | No | % | ||
| 1 | Women who received Placebo or Meghathiamine | 600 | 600 | ||
| 2 | Women excluded from the study because of other reasons | 067 | 11.16 | 059 | 9.83 |
| 3 | Women whocame for follow up regularly | 522 | 87 | 520 | 86.67 |
| 4 | No. of women who did not come for follow up after theinitial inclusion | 011 | 1.83 | 021 | 3.5 |
| 5 | Total final studysubjects | 500 | 83.33 | 500 | 83.33 |
Table I Women Received Placebo / Megathiamine
The trial arm was comparable to the target arm which ever that could have been as it was triple blinded study. The analysis of the outcome of all the cases was done. Outcome comparison was made among both groups after decoding.
Results
During pregnancy in Group A in5 women and in Group B in 10 women anaemia was recorded. In Group A 21 and in Group B 20 women had FGR as well as oligohydramnios. In Group A 11 women had HDsP, 4 mild gestational hypertension (GH),5 severe GH and 2 mild pre-eclampsia. In Group B also in 10women HDsP were recorded, 2 mild GH, 6 severe GH and 2 mild Pre-eclampsia. Of 500 women in Group A, 49 (9.8 Percentage) had pretermlabour,34 (6.8 Percentage) delivered vaginally and 15 (3.0 Percentage had caesarean birth (CB).Overall 451(90.2 Percentage) had term births, 315 ( 69.84 Percentage) normal and 136 (30.15 Percentage) CB. Of 500 women ofGroup B, 59(11.8 Percentage) had preterm births,45 (9.0 Percentage) normal and 14 (2.8 Percentage) CB. 441 (88.2 Percentage) had term births,322 (73.01 Percentage)normal and 119 (26.98 Percentage)CB. In one woman of Group B placental abruption was recorded (Table II).
| OUTCOME | GROUP A 500 | GROUP B 500 | |||
| No | % | No | % | ||
| Preterm Births | 49 | 9.8 | 59 | 11.8 | |
| Vaginal | 34 | 06.8 | 45 | 09.0 | |
| CS | 15 | 03.0 | 14 | 02.8 | |
| Term Births up to date | 410 | 82.0 | 392 | 78.4 | |
| SpontaneousLabour | 369 | 64.0 | 296 | 59.2 | |
| 1. Vaginal | 261 | 52.2 | 257 | 51.4 | |
| 2. CS | 108 | 21.6 | 92 | 18.4 | |
| Induced Labour | 41 | 08.2 | 43 | 08.6 | |
| 1. Vaginal | 25 | 05.0 | 25 | 05.0 | |
| 2. CS | 16 | 03.2 | 18 | 03.6 | |
| Postdate Births | 41 | 08.2 | 49 | 09.8 | |
| Spontaneous Labour | 24 | 04.8 | 36 | 07.2 | |
| 1. Vaginal | 14 | 02.8 | 26 | 05.2 | |
| 2. CS | 10 | 02.0 | 10 | 02.0 | |
| Induced Labour | 17 | 03.4 | 13 | 02.6 | |
| 1. Vaginal | 13 | 02.6 | 9 | 01.8 | |
| 2. CS | 4 | 00.8 | 4 | 00.8 | |
| Total | 500 | 100.00 | 500 | 100.00 | |
Table II Maternal Outcome
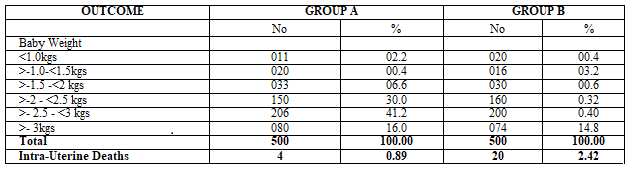
In the triple blinded study in which after decoding it was revealed that women of Group A received placebo and Group BMeghathiamine LBW babies were more in Megathiamine Group, 192 (38.4 Percentage) than placebo, 169 (33.88 Percentage) (P value 0.06500). Admissions to NICU for some or other reason were more in Megathiamine group than in Placebo (45 vs 23) (P value 0.002859). Similarly intrauterine deaths were also more in women who receivedMeghathiamine than Placebo (11(2.2 Percentage) vs 4(0.8 Percentage)(P value 0.03430). There were total of 15 ( 0.3 Percentage ) intrauterine deaths 4 ( 0.8 Percentage in Placebo group and 11 ( 2.2 Percentage) in Megathiamine Group (Table III ) .
Discussion
It is believed that Thiamine deficiency in pregnancy may be responsible for various disorders during pregnancy, because Thiamine functions as the co- enzyme, Thiaminepyrophosphate (TPP) for the metabolism of carbohydrates, branched-chain amino acids, Keto acids by dehydrogenase complexes also (McCormick, 1996, 1997). Thiamine-dependent enzymes are important for the maintenance of cellular energy metabolism, for lipid synthesis, and for nucleotide synthesis in the developing brain (Tylicki 2018). Immune system of the body is also dependent on Thiamine for engulfing and destroying the bacteria (Dhir 2019). It has been reported that Thiamine deficiency and alcohol intake during pregnancy lead to increased fetal deaths, and increased incidence of LBW babies (Bâ 2009). Cote d’lvoire,(2009) reported, that the vitamin supply during pregnancy prevented stillbirths which occured due to chronic alcoholism and different facets of malnutrition as Thiamine deficiency was found to be a potent risk factor for stillbirths. In a study done in Germany, it was revealed that mothers with pregnancies complicated by FGR had significantly lower Erythrocyte Thiamine concentrations than did mothers with a normal pregnancy (Heinze et al 1990). Reports of a high incidence of Thiamine deficiency during pregnancy and lactation were previously reported in India, Malaysia, and Ghana, where in some cases, the consumption of food rich in Thiaminase was also implicated (Neumann, 1979). In the study by Mc Gready et al (2001), visual alertness was found to be significantly better in infants of Thiamine-supplemented mothers than in those of unsupplemented mothers, but the sample size was considered to be too small to assess the association between Thiamine deficiency and the presence of FGR in these cases. Studies of the long-term effects of maternal Thiamine deficiency on human brain development in high-risk populations are still needed. McGready et al (2001) described high incidence of postpartum Thiamine Deficiency assessed by using the Erythrocyte Transketolase activation assay in a refugee camp. Up to 58% of the women were Thiamine deficient at 3 months postpartum despitethe distribution of ration of what appearedto be adequate dietary Thiamine supplements. However Thiamine supplementation was limited to women with peripheral neuropathyd uring pregnancy and those with other clinical signs of Beriberi.This nutritional policywas started whenit was recognized that Infantile Beriberiw as a major cause of infant mortalityin this population. The present study was a triple blindedstudy in which after decoding it was revealed that Group A women received placebo and Group B Meghathiamine. Anaemia was almost in double numbers in women who received Megathiamine compared to placebo (10 vs 5). Oligohydramnios, FGR and HDsP were not different in both the Groups. In Megathiamine Group, pretermbirths were more than placebo (55 vs 44). Major differences were in LBW and admission to NICU. Everyone needs Thiamine in their diet, but for pregnant women this nutrient is especially important. Naturalsources of Thiamine are generally considered safe. Pregnant women taking supplements should not take more than the daily recommended amount. It can do harm too.
References
- Butterworth RF. (2001) Maternal thiamine deficiency: still a problem in some communities. Am J Clin Nutr; 74:712-713
View at Publisher | View at Google Scholar - Mousa A, Naqash A, Lim S. (2019) Macronutrient and micronutrient intake during pregnancy: An overview of recent evidence. Nutrients;11(2):443.
View at Publisher | View at Google Scholar - Borle AB, (1981) Control, modulation and regulation of cell calcium. Rev. Physiol. Biochem. Pharmacol; 90:13.
View at Publisher | View at Google Scholar - McGready R, Simpson JA, Cho T et al (2001) postpartum thiamine deficiency in a Karen displaced population. Am JClinNutr; 74:808-13.
View at Publisher | View at Google Scholar - Baker H, Frank O, Thompson AD, et al. (1975) Vitamin profile of 174 mother and newborn at panurition. Am J ClinNutr;28 158-63.
View at Publisher | View at Google Scholar - (2009) Bâ A,Alcohol and B1 vitamin deficiency-related stillbirths. J Matern Fetal Neonatal Med. ;22(5):452-7.
View at Publisher | View at Google Scholar - McCormick, D.B. (1996). Co-enzymes, Biochemistry of. In: Encyclopedia of Molecular Biology and Molecular Medicine, Vol. 1. Meyers, R.A., ed. Weinheim: VCH, p. 396-406.
View at Publisher | View at Google Scholar - Tylicki A, Łotowski Z, Siemieniuk M, Ratkiewicz A (2018) Thiamine and selected thiamine antivitamins - biological activity and methods of synthesis.Biosci Rep.
View at Publisher | View at Google Scholar - Dhir S, Tarasenko M, Napoli E, Giulivi C. (2019) Neurological, Psychiatric, and Biochemical Aspects of Thiamine Deficiency in Children and Adults.Front Psychiatry. 2 4; 10:207.
View at Publisher | View at Google Scholar - Cote d’lvoire. (2009) Alcohol and B1 vitamin deficiency – related stillbirth. J Matern Fetal Neonatal Med; 22(5): 452-7,
View at Publisher | View at Google Scholar - Heinze T, Weber W, (1990) Determination of thiamine (vitamin B1) in maternal blood during normal pregnancies and pregnancies with intrauterine growth retardation. Z Ernahrunglwiss, 1990 29 : 39 46.
View at Publisher | View at Google Scholar - Neumann GC, Swendseid MF, Jacob M, Stiehm ER, Dirige OV (1979) Biological evidence of thiamine deficiency in young Ghanaian children. Am JClinNutr; 32: 99-104.
View at Publisher | View at Google Scholar
