

Research Article | DOI: https://doi.org/10.31579/2834-5029/018
Adoption of Artificial Intelligence in The Ugandan Health Sector: A Review of Literature
- Alex Mirugwe *
School of Public Health, Makerere University, Kampala, Uganda.
*Corresponding Author: Alex Mirugwe, School of Public Health, Makerere University, Kampala, Uganda.
Citation: Alex Mirugwe, (2023), Adoption of Artificial Intelligence in The Ugandan Health Sector: A Review of Literature, International Journal of Biomed Research. 2(3): DOI: 10.31579/2834-5029/018
Copyright: © 2023, Alex Mirugwe. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 April 2023 | Accepted: 24 April 2023 | Published: 01 May 2023
Keywords: artificial intelligence; health; machine learning; deep learning; fuzzy logic
Abstract
This paper presents a comprehensive literature review on the application of artificial intelligence techniques in Ugandan healthcare and the medical industry. Recently, the data generated in the health domain has exceeded the human cognitive capacity to analyze it effectively. Several approaches have been suggested to address this problem but, in several studies, Artificial Intelligence has been found to be the best and the most effective solution as far as speed, accuracy, robustness, and reliability are concerned. We searched AI health related peer-reviewed articles in ScienceDirect, Springer, PubMed, arXiv, IEEE Xplore, MedRxiv, PLOS, Wiley Online Library, BioMed Central, bioRxiv, and Scopus published between 2012 and 2022. This literature survey covered 38 research papers, and the review showed that the most applied AI subfields are statistical learning, machine learning, and deep learning. The paper highlights the challenges, gaps, and opportunities required to improve and advance the application of AI in the Ugandan healthcare industry. We believe this study will help researchers and policymakers to foster AI innovations better.
1. Introduction
In this information era, the amount of data being generated in every sector of the economy is growing exponentially [1]. This explosion of data is also being witnessed in the health sector. Today, the health industry is generating as much as 30% of the global data volume [2]. A patient is believed to be generating close to 80 megabytes of data in imaging and electronic health-related data annually [3]. This data may include demographics, laboratory tests, treatment, pharmacy, encounters, diagnosis, and many other health-trackable variables.
This data being generated has exceeded the human cognitive capacity to store and analyze it effectively. In a number of studies, AI has proved to be a great solution to this problem [4–6]. According to Bengio et al. [7], AI is a technological force with the greatest potential to transform several industries. AI-enabled systems can quickly analyze vast amounts of data, learn from it, and perform predictions onto which important decisions can be made [8]. AI-powered systems may not replace physicians, but they will help them achieve better results or make better medical decisions.
Broadly, AI is a branch of computer science that aims at developing systems that mimic human intelligence [9]. AI was inspired by the functioning of human brain neurons, and it includes the basics of sensing and objects recognition that empowers machines with intellectual capabilities of performing activities with precision as good as or even better than humans [10]. The most widely applied artificial intelligence techniques include machine learning, deep learning, natural language processing, fuzzy logic, expert systems, robotics, logical programming, and various hybrid systems that combine two or more AI techniques [11, 12].
The application of AI in medicine and healthcare delivery has surged in recent years, and it is getting into fields that were only thought to be the territory of human experts; with many discoveries being made in several areas, including medical imaging, bio-informatics, clinical informatics, electronic health records (EHRs), pharmaceutical developments, and public health informatics. This surge has mainly been attributed to the availability of vast amounts of data, an increase in the computation power, increased demand for more efficient technologies, and the development of novel state-of-the-art AI methods [13].
Papers on the topic of health AI applications have mounted substantially in recent years. Several scholars have written and published articles on its application’s benefits and highlight the potential to improve and advance health care delivery in Uganda [14–17]. In this paper, we review the progress and breakthrough made in Uganda in several medical fields, both in academics and industrial sectors, and then summarizes the challenges, gaps, and opportunities required to improve and advance the application of AI in the Ugandan healthcare industry. The paper will help readers to capture Uganda’s gradual development of health and medical AI-based systems during the last 10 years, from 2012 to 2022.
The following questions guided this study:
- How is AI been applied to Uganda’s health and medical industry?
- What are the challenges researchers and industrialists face in implementing AI in health?
- What is the AI-related programs being taught in Uganda’s academic institutions?
- What are the gaps and opportunities in implementing health-based AI?
2. Methods
This section discusses the research selection methodology and the reviews related to the application of artificial intelligence in healthcare and medicine. We adopted a two-phase research methodology approach for this study:
a comprehensive review of research articles dealing with “health AI-based applications in Uganda” and a second phase focused on analyzing the state (challenges, gaps, and opportunities) of AI application in Uganda’s health industry.
Study Design
In this study, we provided a comprehensive review of the AI healthcare and medical-based literature that has been conducted in Uganda.
Search Strategy
We conducted a rigorous literature review in several bibliographic repositories to find research articles related to artificial intelligence in the Ugandan health sector. To generate reliable evidence in this review paper, we searched nine repositories covering most computer science, medical, and health journals and conferences. These databases are ScienceDirect, Springer, PubMed, arXiv, IEEE Xplore, MedRxiv, PLOS, Wiley Online Library, BioMed Central, bioRxiv, and Scopus.
While searching these databases, we used several keywords. These included “machine learning”, “health informatics”, “artificial intelligence”, “biomedical”, “clinical decision support”, “computer vision”, “natural language processing”, “fuzzy logic”, “deep learning”, “Monte Carlo”, “Genetic algorithms”, “supervised learning”, “unsupervised learning”, “neural networks”, “statistical modelling”, “robotics”, “autoencoders”, and “medical imaging” etc.
Inclusion Criteria
The papers selected for this study were selected based on the following criteria:
- Papers written in English and published between 2012 - 2022.
- The paper must have discussed the design and use of any AI technique in Uganda’s health care and medical domains.
- The paper evaluated the applicability or performance of new and existing artificial intelligence techniques.
- Papers with full accessible text.
Exclusion Criteria
The study excluded books, book chapters, posters, abstracts, and articles with less than five pages. Studies that used non-human datasets were also not included in this review.
Findings
This section summarizes the research papers in the area of AI health-based research in Uganda.
Search Findings
We identified 126 papers; 88 did not meet our selection criteria because of the reasons mentioned in Section 2.2.2. Overall, a total of 38 articles were included in this study. Kamulegeya et al. [14] carried out a study that assessed the diagnostic accuracy of an AI algorithm that was developed using a deep convolutional neural network (CNN) on Fitzpatrick 6 skin types (black-dark) dermatological conditions that were retrospectively extracted from a digital platform for the Medical Concierge Group, located in Kampala-Uganda. The overall diagnostic accuracy achieved in this study was very low, and this poor performance was attributed to low diversity in the images used to train the algorithms.
Mwikirize et al. [18] employed a hybrid deep learning neural network comprised of a convolutional neural network and long short-term memory recurrent units to train a model with 5000 frames from 42 video sequences. They proposed a method that automatically models temporal dynamics associated with needle tip motion, and it was more accurate than most of the state-of-the-art deep learning methods. Their study showed a great potential to improve needle tip localization in challenging clinical ultrasound-guided interventions. A study by Memon et al. [19] used statistical and machine-learning methods to analyze missing data in maternal health records at Kawempe National Referral Hospital, Uganda. The modelling was performed using Listwise deletion, Mode Imputation, Multiple Imputation by chained equations, Imputation using K-Nearest Neighbors, and Random Forest Imputation techniques, and they were able to find out that 5% of the critical data elements were missing.
Alobo et al. [20] utilized multivariate logistic regression to estimate the risk of maternal death at admission at Lacor Hospital in northern Uganda. Another study by Hughes et al. [21] investigated maternal risk factors, indications, and decision-to-delivery interval of the emergency cesarean section using Cox proportional hazards models and multivariate logistic regression models in Uganda.
Nakasi et al. [22] proposed an automated framework for the diagnosis of malaria parasites in thick blood smears images using pre-trained deep-learning faster regional convolutional neural network (faster R-CNN), single-shot multi box detector (SSD) and RetinaNet meta-architectures. Validation with faster R-CNN achieved the best accuracy results of a mean average precision of over 94%, and SSD provided the best model for mobile deployment.
Shanthi et al. [23] implemented an automated skin disease diagnostic algorithm using a convolutional neural network (CNN) to classify four different types of skin diseases (namely Acne, Keratosis, Eczema herpeticum, and Urticaria).
The algorithm achieved an accuracy of 98.6%. Another study by Onyutha et al. [24] utilized six deep learning and nine machine learning techniques to develop algorithms that can predict residual chlorine in drinking water. Their best performing model managed to explain 74% of the total variance in observed residual chlorine.
Farr et al. [25] applied a machine learning ensemble known as Super Learner to develop a prediction algorithm for tuberculosis screening in people living with HIV. The performance measures for sensitivity and specificity of 90% and 44%, respectively, were achieved in this study. Another study by Shete et al. used the Super Learner technique to evaluate the antibody responses to 28 M. TB antigens as a diagnostic tool for active TB patients in Uganda. They achieved a specificity and sensitivity of 88.6% and 90.6%, respectively.
Jacob and Habomugisha [27] developed a location intelligence system powered by machine learning to automatically map malaria mosquito habitats in domestic agro-pasture land ecosystems in Northern Uganda. This system was embedded in an unmanned aerial vehicle that was used to conduct seek- and-destroy activities. The proposed neural network achieved an outstanding detection performance of about 0.99.
Adil et al. [16] used an elastic-net regularized logistic regression model to develop an algorithm (GLMnet) for predicting individual treatment effects of neurosurgery for traumatic brain injury patients in Uganda. A total of 1766 patients were included in the study and they achieved areas under the receiver operating characteristic curve ranging from 83.1% for a single C5.0 ruleset to 88.5% for a random forest model, with the GLMnet at 87.5%. Mondo et al. [28] employed an artificial intelligence-generated algorithm to detect the left ventricular systolic function in a general cardiac clinic in Uganda. By using an optimal cutoff based on the AUCs, they achieved a sensitivity of 80.77% and specificity of 81.05% with a negative predictive value of 98.99%.
We could not explain other studies in detail due to space and time, but they were summarized in Table 1.
Author and year | AI application | Title |
Rezapour, Hansen [29] | Machine Learning | A machine learning analysis of COVID-19 mental health data. |
Nareeba et al. [30] | Machine Learning | Machine learning algorithm for identifying the predictors of childhood immunization in rural Uganda. |
Bisaso et al. [31] | Machine Learning | A comparative study of logistic regression-based Machine learning techniques for prediction of early virological suppression in antiretroviral initiating HIV patients |
Nshimiyimana and Zhou [32] | Machine Learning | Analysis of riskfactors associated withacute respiratory infections among under-five childrenin Uganda. |
Katushabe et al. [33] | Fuzzy Logic | Fuzzy Based Prediction Model for Air Quality Monitoring for Kampala City in East Africa |
Finnegan et al. [34] | Machine Learning | Deploying machine learning with messy, real-world data in low- and middle-income countries: Developing a global health use case |
Ouma et al. [35] | Statistical Modelling | Model-based small area estimation methods and precise district-level HIV prevalence estimates in Uganda |
Mafigiri et al. [36] | Statistical Modelling | HIV prevalence and uptake of HIV/AIDS services among youths (15–24 Years) in fishing and neighboring communities of Kasensero, Rakai District, South Western Uganda |
Igulot [37] | Statistical Modelling | Sexual and Gender-Based Violence and Vulnerability to HIV Infection in Uganda: Evidence from Multilevel Modelling of Population-Level HIV/AIDS Data |
Kabukye et al. [38] | Statistical Modelling | Assessment of organizational readiness to implement an electronic health record system in a low-resource settings cancer hospital: A cross-sectional survey |
Bbosa et al. [39] | Machine Learning | On the goodness of fit of parametric and non-parametric data mining techniques: the case of malaria incidence thresholds in Uganda |
Roberts, Matthews [40] | Statistical Modelling | Risk factors of malaria in children under the age of five years old in Uganda |
Nabyonga et al. [41] | Statistical Modelling | Health care seeking patterns and determinants of out-of-pocket expenditure for Malaria for the children under-five in Uganda |
Baik et al. [42] | Statistical Modelling | A clinical score for identifying active tuberculosis while awaiting microbiological results: Development and validation of a multivariable prediction model in sub-Saharan Africa |
Becker et al. [17] | Deep Learning | Detection of tuberculosis patterns in digital photographs of chest X-ray images using Deep Learning: feasibility study |
Coker et al. [15] | Machine Learning | A land use regression model using machine learning and locally developed low-cost particulate matter sensors in Uganda. |
Muyama et al. [43] | Deep Learning | Automated Detection of Tuberculosis from Sputum, Smear Microscopic Images Using Transfer Learning Techniques. |
Ndagire et al. [44] | Machine Learning | Modelling study of the ability to diagnose acute rheumatic fever at different levels of the Ugandan healthcare system. |
Kananura [45] | Machine Learning | Machine learning predictive modelling for identification of predictors of acute respiratory infection and diarrhea in Uganda’s rural and urban settings. |
Cummings et al. [46] | Machine Learning | Multidimensional analysis of the host response reveals prognostic and pathogen-driven immune subtypes among adults with sepsis in Uganda. |
Khalifa et al. [47] | Machine Learning | Implications of rapid population growth on survey design and HIV estimates in the Rakai Community Cohort Study (RCCS), Uganda. |
Mugisha et al. [48] | Mathematical Modelling | Mathematical modelling of COVID-19 transmission dynamics in Uganda: Implications of complacency and early easing of lockdown. |
Mbabazi et al. [49] | Mathematical Modelling | A Mathematical Model Approach for Prevention and Intervention Measures of the COVID–19 Pandemic in Uganda. |
Borquez et al. [50] | Mathematical Modelling | The Incidence Patterns Model to Estimate the Distribution of New HIV Infections in Sub-Saharan Africa: Development and Validation of a Mathematical Model. |
Rutaremwa et al. [51] | Statistical Modelling | Determinants of maternal health services utilization in Uganda. |
Table 1: Additional studies included in this study.
4. Discussion
4.1. Trends of AI application in the health industry
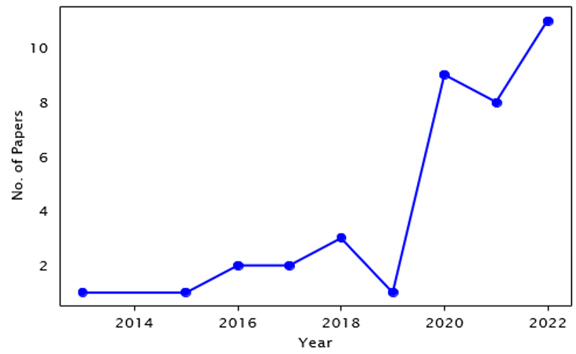
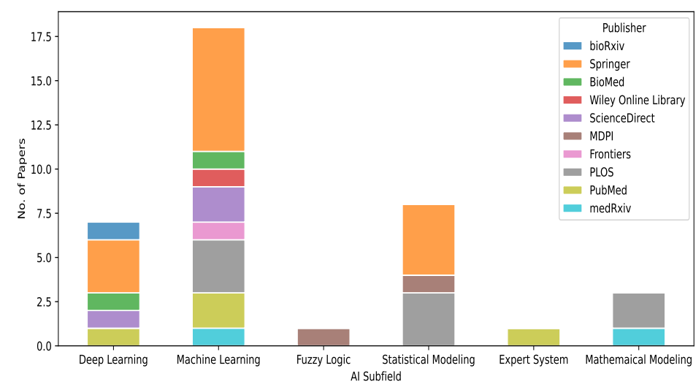
We analyzed the articles published in Uganda, and Figure 1 shows an increasing trend in the number of research papers published in the health and medical AI domain from 2012 onwards. In the 2010s, very few papers were published, but starting in the 2020s, the application of AI subfields in the health industrystarted picking up. Another key observation from the research trend is thatmachine learning is overtaking statistical modelling as the most applied AIsubfield, see Figure 2. This is because of its wide-ranging applicability, hence making it relevant for several healthcare and medical use cases. Of the different machine learning subfields, supervised learning techniques were the most commonly used in all the papers reviewed in this study.
- Challenges and Suggestions
The results of this study show that there are notable AI health-related activities in Uganda, though not yet at the same level as it is in other emerging African countries like Kenya, Nigeria, and Ghana. Several challenges have been presented in the reviewed papers, and we highlight some others below.
- Data accessibility and quality
AI-powered algorithms require large amounts of good-quality data if one is to get good performance [52]. The availability and accessibility of large clinical data are one of the biggest challenges in almost every article reviewed in this study. The low levels of digitization and electronic medical record systems usage in low-developing countries like Uganda make obtaining the required datasets for training and testing AI models challenging. In a number of reviewed studies, authors failed to obtain anticipated results due to lack of enough data or poor-quality data [16, 23, 34, 39]. Clinical data quality is mainly compromised by data noise (missing and incorrect values, data sparsity, and outliers), data heterogeneity, imbalanced data, and data redundancy [53].
To address this issue, the government and other stakeholders will need to invest more in developing and deploying electronic health record systems (EHRs) to improve clinical data digitization levels.
- Cost of AI implementations
Implementing an AI-based system does not come cheap as many associated activities and requirements are costly or even hard to obtain especially in developing countries like Uganda. Authors of the review papers highlighted the financial hardships faced in acquiring and annotating datasets [17, 24], hardware and computing resources [24, 43, 49], and system maintenance and upgrading [29, 42]. Modern AI-driven systems leverage deep learning neural networks that require very high computing hardware compared to traditional machine learning algorithms. Such modern computing hardware is not affordable for researchers in developing countries.
Challenges and Suggestions
- AI Deployment
Most of the AI systems reviewed in this study focused on training, validation, and testing of the models; they were never used or deployed beyond an academic setting [24, 29, 42, 43, 49]. This shows the wide gap between AI systems development and deployment in healthcare practice. But this slow uptake of AI systems in the industry is also attributed to the resistance from healthcare leaders across the global [54, 55].
- Policy and Ethical Issues
In Uganda, there are few protocols governing and guiding the implementation of AI in the healthcare industry. Very few of the reviewed articles even had ethical clearances to be conducted; this not only violates the research ethical guidelines but is also a danger to data privacy. Some authors described the existing ethical guidelines and policies for implementing healthcare and medical AI-powered systems as a challenge and an issue that requires much attention to address [30, 45, 50]. Globally, the available laws and policies have been out-paced by rapid technological advancements, and there is a need to revise them to ensure liability [56]. There is a need for the government of Uganda to establish laws and policies for the safety and regulatory oversight of AI.
- AI Skills Shortage
One of the major roadblocks to implementing and adopting AI in the Uganda health industry is the shortage of AI technical personnel with the experience and knowledge to develop, deploy, and operate AI-powered solutions effectively.
Research by Nagitta et al. [57] suggests that experienced AI experts are in short supply. This may explain why methods in most of the reviewed articles were not deeply explained, and even some papers lacked originality.
To address some of these issues, the governments and the health supporting partners will need to retrain or orient the existing healthcare professionals to fit the rapidly changing needs and also help train future health and medical workers. This will improve the perception, adaptability, and usage of AI in the healthcare industry. Academic institutions also need to introduce AI and health informatics-based programs like data science, biostatistics, machine learning, etc. Formal education, self-teaching, and on-job experience are considered the easiest ways to develop AI expertise [58]. Looking at Ugandan academic institutions, there are very few AI-focused degrees at both undergraduate and postgraduate levels (see Table A1 in Appendix A). Most of these degrees have one to three AI-related courses and mostly focus on introductory principles. The institutions should broaden these degrees to include more courses and a research component, allowing students to research AI-related topics as their thesis/dissertation.
5. Conclusion
5. Conclusion
The paper has highlighted the progress of how AI has been applied in the Ugandan healthcare and medical industry in the last ten years. We reviewed 38 research papers published between 2012 and 2022 in the major bibliographic repositories. In particular, the study summarized the challenges, gaps, and opportunities required to advance the application of AI. AI subfields, especially machine learning, deep learning, and natural language processing, hold tremendous promise to transform several healthcare and medical services in resource-constrained environments like Uganda. However, some AI subfields like machine learning, deep learning, and statistical modelling have been widely applied to address different clinical problems in Uganda, but some fields have not been studied at all. We did not find any study based on natural language processing and robotics subfields.
Acknowledgments
The content of this review paper is solely the responsibility of the author and does not necessarily represent the official views of the Makerere University School of Public Health.
Appendix
An AI-related Programs taught in Ugandan universities
Table A1 shows that several academic institutions are seeking to train students in AI-related fields at the postgraduate level. Though most of these courses offer basic AI and Data Science concepts.
References
- Nalubega T, Uwizeyimana DE. (2019). Public sector monitoring and evaluation in the Fourth Industrial Revolution: Implications for Africa. Africa’s Public Service Delivery and Performance Review. 7(1):1–12.
View at Publisher | View at Google Scholar - Gopal G, Suter-Crazzolara C, Toldo L, Eberhardt W. (2019). Digital transformation in healthcare–architectures of present and future information technologies. Clinical Chemistry and Laboratory Medicine (CCLM). 57(3):328–335.
View at Publisher | View at Google Scholar - Huesch MD, Mosher TJ. (2017). Using it or losing it? The case for data scientists inside health care. Nejm Catalyst. 3(3).
View at Publisher | View at Google Scholar - McCall B. COVID-19 and artificial intelligence: protecting health care workers and curbing the spread. The Lancet Digital Health.2020;2(4): e166–e167.
View at Publisher | View at Google Scholar - Shailaja K, Seetharamulu B, Jabbar M. (2018). Machine learning in health care: A review. In: 2018 Second international conference on electronics, communication and aerospace technology (ICECA). IEEE; p. 910–914.
View at Publisher | View at Google Scholar - Currie G, Hawk KE, Rohren E, Vial A, Klein R. (2019). Machine learning and deep learning in medical imaging: intelligent imaging. Journal of medical imaging and radiation sciences. 50(4):477–487.
View at Publisher | View at Google Scholar - Bengio Y, Courville A, Vincent P. (2013). Representation learning: A review and new perspectives. IEEE transactions on pattern analysis and machine intelligence. 35(8):1798–1828.
View at Publisher | View at Google Scholar - Haleem A, Javaid M, Khan IH. (2019). Current status and applications of artificial intelligence (AI) in medical field: An overview. Current Medicine Research and Practice. 9(6):231–237.
View at Publisher | View at Google Scholar - Dick S. (2019). Artificial intelligence.
View at Publisher | View at Google Scholar - Ellahham S, Ellahham N, Simsekler MCE. (2020). Application of artificial intelligence in the health care safety context: opportunities and challenges. American Journal of Medical Quality. 35(4):341–348.
View at Publisher | View at Google Scholar - Parishwad G, Bhardwaj R, Nema V. (1997). Estimation of hourly solar radiation for India. Renewable Energy. 12(3):303–313.
View at Publisher | View at Google Scholar - Maafi A, Adane A. (1989). A two-state Markovian model of global irradiation suitable for photovoltaic conversion. Solar & wind technology. 6(3):247–252.
View at Publisher | View at Google Scholar - Mirugwe A, Nyirenda J, Dufourq E. (2022). Automating Bird Detection Based on Webcam Captured Images using Deep Learning. In: Proceedings of 43rd Conference of the South African Insti. vol. 85; p. 62–76.
View at Publisher | View at Google Scholar - Kamulegeya LH, Okello M, Bwanika JM, Musinguzi D, Lubega W, et al. (2019). Using artificial intelligence on dermatology conditions in Uganda: A case for diversity in training data sets for machine learning. BioRxiv. p. 826057.
View at Publisher | View at Google Scholar - Coker ES, Amegah AK, Mwebaze E, Ssematimba J, Bainomugisha E. (2021). A land use regression model using machine learning and locally developed low-cost particulate matter sensors in Uganda. Environmental Research. 199:111352.
View at Publisher | View at Google Scholar - Adil SM, Elahi C, Gramer R, Spears CA, Fuller AT, et al. (2021). Predicting the individual treatment effect of neurosurgery for patients with traumatic brain injury in the low-resource setting: a machine learning approach in Uganda. Journal of Neurotrauma. 38(7):928–939.
View at Publisher | View at Google Scholar - Becker A, Bluthgen C, Sekaggya-Wiltshire C, Castelnuovo B, Kambugu A, et al. (2018). Detection of tuberculosis patterns in digital photographs of chest X-ray images using Deep Learning: feasibility study. The International Journal of Tuberculosis and Lung Disease. 22(3):328–335.
View at Publisher | View at Google Scholar - Mwikirize C, Kimbowa AB, Imanirakiza S, Katumba A, Nosher JL, et al. (2021). Time-aware deep neural networks for needle tip localization in 2D ultrasound. International Journal of Computer Assisted Radiology and Surgery. 16(5):819–827.
View at Publisher | View at Google Scholar - Memon SM, Wamala R, Kabano IH. (2022). Missing Data Analysis Using Statistical and Machine Learning Methods in Facility-Based Maternal Health Records. SN Computer Science. 3(5):1–15.
View at Publisher | View at Google Scholar - Alobo G, Reverzani C, Sarno L, Giordani B, Greco L. (2022). Estimating the Risk of Maternal Death at Admission: A Predictive Model from a 5-Year Case Reference Study in Northern Uganda. Obstetrics and Gynecology International.
View at Publisher | View at Google Scholar - Hughes NJ, Namagembe I, Nakimuli A, Sekikubo M, Moffett A, et al. (2020). Decision-to-delivery interval of emergency cesarean section in Uganda: a retrospective cohort study. BMC pregnancy and childbirth. 20(1):1–10.
View at Publisher | View at Google Scholar - Nakasi R, Mwebaze E, Zawedde A, Tusubira J, Akera B, et al. (2020). A new approach for microscopic diagnosis of malaria parasites in thick blood smears using pre-trained deep learning models. SN Applied Sciences. 2(7):1–7.
View at Publisher | View at Google Scholar - Shanthi T, Sabeenian R, Anand R. (2020). Automatic diagnosis of skin diseases using convolution neural network. Microprocessors and Microsystems. 76:103074.
View at Publisher | View at Google Scholar - Onyutha C, et al. (2022). Multiple Statistical Model Ensemble Predictions of Residual Chlorine in Drinking Water: Applications of Various Deep Learning and Machine Learning Algorithms. Journal of Environmental and Public Health.
View at Publisher | View at Google Scholar - Farr K, Ravindran R, Strnad L, Chang E, Chaisson LH, et al. (2018). Diagnostic performance of blood inflammatory markers for tuberculosis screening in people living with HIV. PloS one. 13(10): e0206119.
View at Publisher | View at Google Scholar - Shete PB, Ravindran R, Chang E, Worodria W, Chaisson LH, et al. (2017). Evaluation of antibody responses to panels of M. tuberculosis antigens as a screening tool for active tuberculosis in Uganda. PLoS One. 12(8): e0180122.
View at Publisher | View at Google Scholar - Jacob BG, Habomugisha P. (2021). Location Intelligence Powered by Machine Learning Automation for Mapping Malaria Mosquito Habitats Employing an Unmanned Aerial Vehicle (UAV) for Implementing “Seek and Destroy” for Commercial Roadside Ditch Foci and Real Time Larviciding Rock Pit Quarry Habitats in Peri-Domestic Agro-Pastureland Ecosystems in Northern Uganda. In: Sensemaking for Security. Springer. p. 133–148.
View at Publisher | View at Google Scholar - Mondo C, Attia Z, Benavente E, Friedman P, Noseworthy P, et al. (2020). External validation of an electrocardiography artificial intelligence generated algorithms to detect left ventricular systolic function in a general cardiac clinic in Uganda. European Heart Journal. 41(Supplement 2): ehaa946–1013.
View at Publisher | View at Google Scholar - Rezapour M, Hansen L. (2020). A machine learning analysis of COVID-19 mental health data. Scientific reports. 12(1):1–16.
View at Publisher | View at Google Scholar - Nareeba T, Wosu A, Kajungu D. (2020). Machine learning algorithm for identifying the predictors of childhood immunization in rural Uganda. International Journal of Infectious Diseases. 101:483.
View at Publisher | View at Google Scholar - Bisaso KR, Karungi SA, Kiragga A, Mukonzo JK, Castelnuovo B. (2018). A comparative study of logistic regression-based machine learning techniques for prediction of early virological suppression in antiretroviral initiating HIV patients. BMC medical informatics and decision making. 18(1):1–10.
View at Publisher | View at Google Scholar - Nshimiyimana Y, Zhou Y. (2022). Analysis of risk factors associated with acute respiratory infections among under-five children in Uganda. BMC Public Health. 22(1):1–10.
View at Publisher | View at Google Scholar - Katushabe C, Kumaran S, Masabo E. (2021). Fuzzy Based Prediction Model for Air Quality Monitoring for Kampala City in East Africa. Applied System Innovation. 4(3):44.
View at Publisher | View at Google Scholar - Finnegan A, Potenziani DD, Karutu C, Wanyana I, Matsiko N, et al. (2022). Deploying machine learning with messy, real-world data in low-and middle-income countries: Developing a global health use case. Frontiers in big Data. 5.
View at Publisher | View at Google Scholar - Ouma J, Jeffery C, Awor CA, Muruta A, Musinguzi J, et al. (2021). Model-based small area estimation methods and precise district-level HIV prevalence estimates in Uganda. PLOS one. 16(8): e0253375.
View at Publisher | View at Google Scholar - Mafigiri R, Matovu JK, Makumbi FE, Ndyanabo A, Nabukalu D, et al. (2017). HIV prevalence and uptake of HIV/AIDS services among youths (15–24 Years) in fishing and neighboring communities of Kasensero, Rakai District, South Western Uganda. BMC Public Health. 17(1):1–10.
View at Publisher | View at Google Scholar - Igulot P. (2022). Sexual and Gender-Based Violence and Vulnerability to HIV Infection in Uganda: Evidence from Multilevel Modelling of Population Level HIV/AIDS Data. Social Sciences. 11(7):301.
View at Publisher | View at Google Scholar - Kabukye JK, de Keizer N, Cornet R. (2020). Assessment of organizational readiness to implement an electronic health record system in a low- resource settings cancer hospital: A cross-sectional survey. PLOS one. 15(6): e0234711.
View at Publisher | View at Google Scholar - Bbosa FF, Nabukenya J, Nabende P, Wesonga R. (2021). On the goodness of fit of parametric and non-parametric data mining techniques: the case of malaria incidence thresholds in Uganda. Health and Technology. 11(4):929–940.
View at Publisher | View at Google Scholar - Roberts D, Matthews G. (2016). Risk factors of malaria in children under the age of five years old in Uganda. Malaria journal. 15(1):1–11.
View at Publisher | View at Google Scholar - Nabyonga J, Mugisha F, Okui AP, Musango L, Kirigia JM. (2013). Health care seeking patterns and determinants of out-of-pocket expenditure for malaria for the children under-five in Uganda. Malaria journal. 12(1):1–11.
View at Publisher | View at Google Scholar - Baik Y, Rickman HM, Hanrahan CF, Mmolawa L, Kitonsa PJ, et al. (2020). A clinical score for identifying active tuberculosis while awaiting microbiological results: Development and validation of a multivariable prediction model in sub-Saharan Africa. PLoS medicine. 17(11): e1003420.
View at Publisher | View at Google Scholar - Muyama L, Nakatumba Nabende J, Mudali D. (2019). Automated detection of tuberculosis from sputum smears microscopic images using transfer learning techniques. In: International Conference on Intelligent Systems Design and Applications. Springer; p. 59–68.
View at Publisher | View at Google Scholar - Ndagire E, Ollberding N, Sarnacki R, Meghna M, Pulle J, et al. (2022). Modelling study of the ability to diagnose acute rheumatic fever at different levels of the Ugandan healthcare system. BMJ open. 12(3): e050478.
View at Publisher | View at Google Scholar - Kananura RM. (2022). Machine learning predictive modelling for identification of predictors of acute respiratory infection and diarrhoea in Uganda’s rural and urban settings. PLOS Global Public Health. 2(5): e0000430.
View at Publisher | View at Google Scholar - Cummings MJ, Bakamutumaho B, Price A, Owor N, Kayiwa J, et al. (2022). Multidimensional analysis of the host response reveals prognostic and pathogen-driven immune subtypes among adults with sepsis in Uganda. Critical Care. 26(1):1–15.
View at Publisher | View at Google Scholar - Khalifa A, Ssekubugu R, Lessler J, Wawer MJ, Santelli J, et al. (2022). Implications of rapid population growth on survey design and HIV estimates in the Rakai Community Cohort Study (RCCS), Uganda. medRxiv.
View at Publisher | View at Google Scholar - Mugisha JY, Ssebuliba J, Nakakawa JN, Kikawa CR, Sematimba A. (2021). Mathematical modeling of COVID-19 transmission dynamics in Uganda: Implications of complacency and early easing of lockdown. PloS one. 16(2): e0247456.
View at Publisher | View at Google Scholar - Mbabazi FK, Gavamukulya Y, Awichi R, Olupot-Olupot P, Rwahwire S, et al. (2020). A mathematical model approach for prevention and intervention measures of the COVID–19 pandemic in Uganda. medRxiv.
View at Publisher | View at Google Scholar - Borquez A, Cori A, Pufall EL, Kasule J, Slaymaker E, et al. (2016). The incidence patterns model to estimate the distribution of new HIV infections in Sub-Saharan Africa: development and validation of a mathematical model. PLoS medicine. 13(9): e1002121.
View at Publisher | View at Google Scholar - Rutaremwa G, Wandera SO, Jhamba T, Akiror E, Kiconco A. (2015). Determinants of maternal health services utilization in Uganda. BMC health services research. 15(1):1–8.
View at Publisher | View at Google Scholar - Owoyemi A, Owoyemi J, Osiyemi A, Boyd A. Artificial intelligence for healthcare in Africa. Frontiers in Digital Health. 2020; 2:6.
View at Publisher | View at Google Scholar - Zhou L, Pan S, Wang J, Vasilakos AV. Machine learning on big data: Opportunities and challenges. Neurocomputing. 2017; 237:350–361.
View at Publisher | View at Google Scholar - He J, Baxter SL, Xu J, Xu J, Zhou X, et al. (2019). The practical implementation of artificial intelligence technologies in medicine. Nature medicine. 25(1):30–36.
View at Publisher | View at Google Scholar - Safi S, Thiessen T, Schmailzl KJ, et al. (2018). Acceptance and resistance of new digital technologies in medicine: qualitative study. JMIR research protocols. 7(12): e11072.
View at Publisher | View at Google Scholar - Petersson L, Larsson I, Nygren JM, Nilsen P, Neher M, et al. (2022). Challenges to implementing artificial intelligence in healthcare: a qualitative interview study with healthcare leaders in Sweden. BMC Health Services Research. 22(1):1–16.
View at Publisher | View at Google Scholar - Nagitta PO, Mugurusi G, Obicci PA, Awuor E. (2022). Human-centered artificial intelligence for the public sector: The gate keeping role of the public procurement professional. Procedia Computer Science. 200:1084–1092.
View at Publisher | View at Google Scholar - Butcher N, Wilson-Strydom M, Baijnath M. (2021). Artificial intelligence capacity in sub-Saharan Africa: Compendium report.
View at Publisher | View at Google Scholar
