

Case Report | DOI: https://doi.org/10.31579/2835-8295/037
A Case Report of Spontaneous Superficial Temporal Artery Hemorrhage following COVID-19 Infection
- Med Leonard B. Goldstein *
- Kelly Frasier,
- CRC Camilla Herbin,
- James Keane
Assistant Vice President for Clinical Education Development.
*Corresponding Author: Med Leonard B. Goldstein, Assistant Vice President for Clinical Education Development.
Citation: Leonard B. Goldstein, Kelly Frasier, CRC Camilla Herbin, James Keane (2023), A Case Report of Spontaneous Superficial Temporal Artery Hemorrhage following COVID-19 Infection, International Journal of Clinical Reports and Studies, 2(5); DOI:10.31579/2835-8295/037
Copyright: © 2023, Leonard B. Goldstein. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 September 2023 | Accepted: 26 September 2023 | Published: 29 September 2023
Keywords: covid-19; coronavirus disease; world health organization; hypertension; headache
Abstract
Post-COVID syndrome and COVID-19 have been related to autonomic changes and the appearance of endothelial dysfunction. Current research has discovered vasculitis-like occurrences in patients previously without evidence of endothelial dysfunction or autoimmune states. Additionally, COVID-19 and post-COVID syndrome have been hypothesized to induce flares of vascular dysfunction. Here, we present a patient with a large hematoma of the right scalp following spontaneous superficial temporal artery hemorrhage after uncontrolled hypertension, tachycardia, and generalized weakness three months after COVID-19 infection. This patient’s bleed was successfully managed with a pressure bandage and did not require neurosurgical embolization; moreover, he had no prior hemorrhages or indications for vessel rupture. Our case study represents a patient with chronic changes in blood pressure and heart rate following a prior COVID-19 infection that led to a large superficial scalp hematoma over the right frontotemporal bone with active extravasation from the right superficial temporal artery.
Introduction
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a global pandemic causing mild or severe respiratory symptoms. COVID-19 presents with a wide spectrum of clinical manifestations including myalgia, cough, dyspnea, fever, diarrhea, vomiting, nausea, hypertension, and headache. Although respiratory symptoms typically predominate, multiple organ dysfunction may occur and patients with current or recent COVID-19 infection may also experience heightened risk of bleeding, typically due to a high incidence of thromboembolic complications1. As of August 2023, there have been more than 770 million confirmed cases of COVID-19 and over 6.9 million deaths reported to the World Health Organization (WHO)2.
Data continues to emerge stating that COVID-19 affects patients long after the acute phase comes to an end, leaving many with “long COVID”, which is also referred to as post-COVID syndrome or post-acute COVID-19 syndrome. Long COVID is a serious global problem and includes a variety of symptoms and ongoing health problems that may last for weeks to years after initial COVID-19 infection. The World Health Organization (WHO) defines “long COVID” (post COVID-19) as “a clinical condition that occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis”3. Previous national study reports found COVID-19 has a direct association with hypertension4, in addition to complications of COVID-19 tied directly to vascular disorders4,5. Recent evidence suggests that hypertension and diseases related closely to hypertension (i.e., spontaneous hemorrhage) may occur as sequelae of COVID-19 after the acute phase of infection. Multiple studies reported elevated blood pressure and excess burdens of hypertension as post-acute sequelae of COVID-194,6,7.
Currently, many case studies have identified spontaneous bleeds thought to be attributed to COVID-19 infection, post-COVID syndrome, or long COVID. These documented bleeds have included, but are not limited to, spontaneous hemothorax, subdural hematomas, intracerebral hemorrhage, spontaneous muscle hematoma, a massive retroperitoneal hematoma due to spontaneous left inferior epigastric artery hemorrhage, spontaneous intraperitoneal hemorrhage, spontaneous adrenal hemorrhage, and spontaneous epidural hematoma of the cervical spine. Here, we discuss a patient with spontaneous hemorrhage of the right superficial temporal artery leading to a large superficial scalp hematoma. The patient had no history of hypercoagulability, anticoagulation usage, or trauma. Similar to other patients documented to have spontaneous hemorrhage following COVID-19 infection, our patient also developed new-onset, uncontrolled hypertension following a COVID-19 infection three months prior. This case study represents an additional spontaneous, unprovoked hemorrhage to the superficial temporal artery following uncontrolled hypertension with long COVID symptomatology.
Case Study
A 50-year-old male presented to our medical step-down unit (MSDU) via the emergency department (ED) for a large, right-sided head swelling, headache, and lightheadedness without loss of consciousness. His past medical history included gout and new-onset hypertension following a COVID-19 infection that had occurred three months prior. Upon arrival to the ED, his blood pressure was 188/81, indicating hypertensive urgency. His initial hemoglobin was 12.6 with a baseline of approximately 14. Over the next three days, his hemoglobin dropped from 12.6 to 12.4 to 11.3. On day two of hospitalization, his hemoglobin dropped to 11.4. Additionally, he had a potassium of 3.3, chloride of 96, AST of 92, AST of 130, and ALP of 149. Sed rate was slightly elevated at 30. WBC remained between 6.8 and 8.6. EKG showed sinus tachycardia at 143 bpm and borderline T wave abnormalities.
Of particular interest, our patient developed new-onset, uncontrolled hypertension and tachycardia following his COVID-19 infection three months prior. He had been unable to successfully manage his hypertension and tachycardia since his COVID-19 infection even after seeing his primary care doctor multiple times for medication adjustments. Our patient’s post-COVID syndrome included paroxysmal hypertension with a systolic value 20-45 above his baseline and a heart rate that increased from the 70s to 110-140 bpm post-COVID-19 infection. Our patient also dealt with weakness, fatigue, lethargy, and malaise after he recovered from COVID. Due to having a new onset of autonomic dysregulation with blood pressure and heart rate, our patient made multiple lifestyle changes over the months since his COVID-19 infection. He made healthy dietary changes, eliminated foods high in fat or oil, started exercising more regularly, and began meditating for stress control. He also started taking amlodipine 7.5 mg every day for additional blood pressure management with his new onset of post-COVID symptoms. The patient had no history of hypercoagulability, anticoagulation usage, or trauma.
The patient first arrived to the ED from work stating he was sitting at his computer and felt a little shaky when he stood up and noticed a large area of swelling to the right side of his head. He then started to notice a headache but denied dizziness or blurred vision. He had swelling to the right temporal lobe, approximately 9cm x 6.5cm in diameter with fluctuance. His extraocular movements and cerebellar function were normal. Initially, his systolic blood pressure was between 146-174, and
he was given IV labetalol and IV morphine IV for pain. Of note, his history included previous CyberKnife surgery for a left-sided arteriovenous malformation one year prior that two neurosurgeons documented were unrelated to the current hemorrhage. The patient’s frontotemporal region continued to enlarge with increasing headache and lightheadedness. The patient denied any trauma to the area. He denied vision changes, difficulty breathing, chest pain, or any focal neurologic deficits. Neurosurgery’s diagnosis concluded as spontaneous hematoma formation of unknown etiology.
Upon arrival, CT of the head showed a large right frontotemporal scalp hematoma with hematocrit levels suggesting recent/active hemorrhage, no acute intracranial hemorrhage or extra axial collection, and left temporal encephalomalacia and gliosis likely related to prior treatment/ischemic insult with superimposed acute ischemia. CTA of the head/neck showed patent intracranial arteries without significant stenosis, occlusion, or aneurysm, a small amount of internal cerebral venous drainage, and a large superficial scalp hematoma over the right frontotemporal bone with active extravasation from the right superficial temporal artery. Both right and left internal carotid arteries showed no hemodynamically significant stenosis by NASCET criteria.
Of note, this patient had never had a spontaneous bleed like this before or any autoimmune diseases that would lead to vascular compromise. The patient’s home medications prior to his hospitalization included amlodipine 7.5 QD (started after COVID-19 infection), melatonin 3mg QHS, allopurinol 100mg QD, lorazepam 0.5mg BID PRN, and supplemental potassium.
The patient was admitted to MSDU for further monitoring, and neurosurgery recommended his systolic blood pressure (SBP) be kept below 140. Neurosurgery had been consulted for possible embolization for temporal artery hemorrhage. Upon arriving to the MSDU from the ED, the patient was afebrile and hypertensive with SBP in the 170s. He was neither hypoxic nor tachypneic. He required a Cardene drip between 5-10 mg/hr for over 24 hours to maintain a resting SBP below 140.
During the following two days, the patient’s systolic blood pressure began to slowly decrease with the Cardene drip and addition of Amlodipine and Lisinopril. The pressure bandage applied by neurosurgery controlled the extravasation of blood, and the progression of swelling became stable. The patient was eventually transferred to a general medicine floor before discharge and close follow-up with his primary care provider. Upon discharge, the patient was instructed to follow up for hematoma of scalp, hypertensive emergency, arterial hemorrhage, and uncontrolled hypertension.

Image 1: An approximately 4cm x 4cm healing hematoma (previously 9cm x 6.5cm) in the temporoparietal region of the right scalp with fluctuance and a surrounding ring of non-blanching erythema
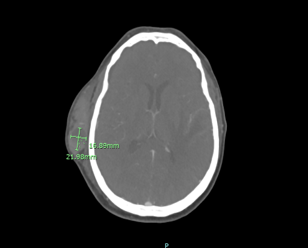
Image 2: CT Head Angiogram. Large superficial scalp hematoma over the right frontotemporal bone with active extravasation from the right superficial temporal artery 2.3 cm x 1.7cm
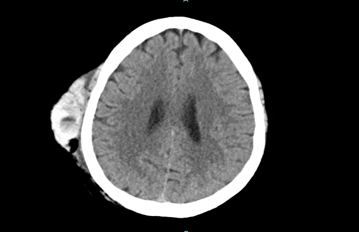
Image 3: CT Head Non-Contrast. Large right frontotemporal scalp hematoma
Discussion
There remains a substantial body of knowledge yet to be garnered from the novel coronavirus, particularly with respect to potential protracted consequences, which will become increasingly apparent as time elapses and larger datasets become available. Patients are currently presenting with a diverse array of post-COVID symptoms, necessitating both recognition and comprehensive documentation to facilitate the identification of potential trends. While there have been numerous reports detailing the impact of COVID-19 on pre-existing hypertension and other cardiovascular disorders, there is notably less information on the emergence of new-onset hypertension and subsequent endothelial dysfunction following COVID-19 infection. However, data has been collected on the increased likelihood of developing new-onset hypertension or worsening hypertension with post-COVID syndrome8. Additionally, multiple case reports and case studies have shown diverse arterial spontaneous hemorrhage. Emerging data underscores the capacity of COVID-19 to affect individuals beyond the acute phase, often referred to as "long COVID" or post-acute COVID-19 syndrome. The analysis of long COVID data allows for better understanding in this particular case the association between long COVID-induced uncontrolled hypertension and spontaneous vessel hemorrhage.
The pathophysiology of long COVID is uncertain. COVID-19 infection and its long-term effects are likely to be highly influenced by factors such as age and sex, not unlike hypertension and other forms of vascular dysfunction. The SARS-Cov-2 virus that causes COVID-19 uses angiotensin-converting-enzyme 2 (ACE2) as a cellular entry receptor by binding its spike protein there and gaining access to cells that express this enzyme9. The renin-angiotensin-aldosterone-system (RAAS) is highly regulated by a variety of molecules including ACE2, so therefore this virus can increase ACE2 activity and ultimately drive this process which paradoxically should decrease blood pressure through systemic and local vasodilation10. In sum, this system functions by the macula densa sensing either low intra-tubular sodium concentration or receiving sympathetic input to activate renin. Renin then stimulates the conversion of angiotensinogen to angiotensin I in the liver, and the accumulation of angiotensin-I increases angiotensin-converting-enzyme (ACE) activity to form angiotensin-II in the lungs. Angiotensin II stimulates aldosterone release which functions to vasoconstrict and therefore increases blood pressure. Alternatively, both angiotensin-I and angiotensin-II can be converted to other substrates via ACE2 which act to decrease blood pressure, namely, Ang(1-7) and Ang(1-9), respectively.
Hypertension is widely accepted as a risk factor for more severe manifestations of COVID. There have also now been several studies that may suggest COVID-19 infection as a cause or precipitating factor for new-onset hypertension. In a study by Akpek et al., 153 patients were evaluated in the acute phase at a follow-up appointment after a COVID-19 infection11. These patients were not previously diagnosed with hypertension, nor were their blood pressures elevated at the time of infection diagnosis. Out of 153 patients, 18 had new-onset hypertension with statistically significant increases in both systolic (120.9 ± 7.2 vs 126.5 ± 15.0 mmHg, P <.001) and diastolic BP (78.5 ± 4.4 vs 81.8 ± 7.4 mmHg, P <.001), with a mean follow-up time of 31.6 ± 5.0 days11. In a much larger systematic review and meta-analysis of available data, Zuin et al. evaluated greater than nineteen million individuals and identified 758,698 patients with confirmed COVID-19 infection with a mean length of follow-up of 6.8 months12. They determined that patients who were status post COVID-19 infection had a higher risk of developing new-onset hypertension compared to the general population, and this risk increases with male sex, age, and concurrent malignancy12. These findings further perpetuate the need for primary prevention against COVID, as well as close follow up after infection to monitor for hemorrhagic complications.
A retrospective study by Delalić et al. of 199 participants conducted between January 2021 and January 2022 analyzed the frequency of newly diagnosed or worsened existing hypertension based on the patient's phase of COVID-19 infection (acute, sub-acute, chronic, “long COVID”)13. This study found that post-COVID arterial hypertension affected 1 in 6 of their population studied13. Although this is limited by sample size, additional studies of this nature should be carried out in order to determine more definitive associations. Multiple case reports and case series have also been published on arterial dysfunction with reported hemorrhage due to acute or long COVID infection. Additional studies are needed to determine any link or causality between post-COVID syndrome, long COVID, and spontaneous hemorrhage in the weeks to months following COVID-19 infection in patients with no prior history of hypercoagulable states, anticoagulant use, or trauma.
Because SARS-CoV-2 has the propensity to bind ACE2, it decreases its availability to participate in natural homeostatic mechanisms, competing with angiotensin-II, thereby blunting its effects of vasodilation and anti-inflammation, further promoting hypertension, inflammation, and fibrosis. This downregulation of ACE2 also increases bradykinin that can activate the bradykinin B2 receptor and promote vasoconstriction. In people with pre-existing comorbidities, especially those which disrupt endothelial homeostasis such as hypertension, diabetes mellitus, and chronic kidney disease, COVID-19 has been associated with higher rates of complications and worse outcomes14. It has been remarkably difficult to isolate risk factors which would predispose individuals to more severe forms of COVID-19 infection, as patients typically have multiple comorbidities. Several studies have evaluated the association between hypertension and severity of COVID-19 infection, although they have not yet proved causation due to confounding of other comorbidities. In addition, men have been found to have on average higher levels of plasma ACE2 which could further demonstrate the increased disruption and their susceptibility to endothelial dysfunction caused by SARS-CoV-2 interference10.
Thromboembolic complications, both venous and arterial, have been noted to have increased incidence in patients with COVID-19 infection. The mechanism of endothelial dysfunction in COVID-19 remains unclear, although several hypotheses have been proposed. Endothelial cells expression of ACE2 predisposes them to damage by the virus, which then allows for increased permeability and could potentially explain the risk for respiratory dysfunction in the case of increased permeability of alveoli precipitating acute respiratory distress syndrome (ARDS) with COVID-19 infections. Ackermann et al. performed molecular and microscopic analyses of seven cases of COVID-19 lungs at biopsy, which demonstrated endothelial cell injury with intracellular virus, disrupted membranes, thrombosis with microangiopathy, and new vessel growth15. Thus, endothelial dysfunction may serve as an indicator for disease severity and risk of endothelial complications with major clinical consequences. Endothelial dysfunction seen specifically with acute COVID-19 infection and long COVID has been hypothesized as the culprit of various vasculopathies attributed to history of viral infection. The tendency towards hemorrhage may be due to endothelial dysfunction and unregulated inflammation creating a weakening within the vessel wall, making the vessel more likely to develop an area of compromised integrity and hemorrhage when coupled with longstanding, uncontrolled hypertension15. Furthermore, a deposition of immune complexes has been identified inside vascular walls, leading to a highly inflammatory state16. Immune complexes within the vasculature trigger an immune response that can cause a state of increased inflammation and compromise of vascular wall integrity.
Multiple case reports have documented cases of spontaneous hemorrhages thought to be linked to acute COVID-19 infection or post-COVID syndrome. Many of these cases reiterate the point that while ample research has been published on how hypercoagulable states are linked to COVID-19 infections, very little has been studied regarding bleeding manifestations associated with COVID-19. For instance, two cases of spontaneous muscle hematoma have been associated with COVID-1917. One case of spontaneous epidural hematoma of the cervical spine following a recent COVID-19 infection was also reported in a patient who had no prior history of coagulopathy, use of anticoagulants, or history of trauma18. Multiple instances of spontaneous brain hemorrhages have been reported following a COVID-19 infection. Multiple spontaneous intracerebral hemorrhages have been cited, in addition to a spontaneous intramedullary hematoma and a spontaneous brainstem hemorrhagic stroke19,20,21,22. Additional case studies also represent cases of spontaneous intraperitoneal hemorrhage, spontaneous retroperitoneal hematoma with spontaneous injury to the inferior epigastric artery, giant chest wall hematomas, and multiple documented cases of spontaneous hemothorax following COVID-19 infection23,24,25,26,27. Cases continue to be documented regarding spontaneous hemorrhagic bleeds following acute COVID-19 infection or long COVID with little research conducted on the association between hemorrhagic activity and previous COVID-19 infection. As cases of spontaneous hemorrhage continue to be found in correlation with COVID-19 infection in patients with no history of coagulopathy, trauma, or use or anticoagulants, associations must be further investigated to diagnose, treat, and prevent this type of spontaneous vascular dysregulation.
Conclusion
This case study represents a patient with post-COVID syndrome experiencing chronic changes in blood pressure and heart rate following a COVID-19 infection that led to a large superficial scalp hematoma over the right frontotemporal bone with active, spontaneous extravasation from the right superficial temporal artery. The patient had no history of hypercoagulability, anticoagulation usage, or trauma. Long COVID and post-COVID syndrome have been analyzed to contribute to worsening or new-onset hypertension, in addition to spontaneous hemorrhage attributed to endothelial dysfunction leading to vasculitis and vasculopathies. While multiple case reports have documented various locations of spontaneous hemorrhage attributable to long COVID, this is the first case study reported of spontaneous hemorrhage of the superficial temporal artery following COVID-19 infection. There is increasing and documented evidence for spontaneous hemorrhage following COVID-19 infection, and healthcare providers should be alerted to new-onset or worsening hypertension in post-COVID patients with the risk of developing spontaneous hemorrhage or vascular complications in the post-COVID course of disease.
References
- Guan WJ, Ni ZY, Hu Y, et al. (2020), Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med, 382 pp. 1708-1720.
View at Publisher | View at Google Scholar - World Health Organization (WHO). 2023. WHO Coronavirus (COVID-19) Dashboard. Retrieved on 7 September, from https://covid19.who.int.
View at Publisher | View at Google Scholar - World Health Organization (WHO). A clinical case definition of post COVID-19 condition by a Delphi consensus, 6 October 2021. https://apps.who.int/iris/bitstream/handle/10665/345824/WHO-2019-nCoV-Post-COVID-19-condition-Clinical-case-definition-2021.1-eng.pdf?sequence=1&isAllowed=y. Accessed 25 Dec 2022.
View at Publisher | View at Google Scholar - Shibata S, Kobayashi K, Tanaka M, et al. (2022). COVID-19 pandemic and hypertension: an updated report from the Japanese Society of Hypertension project team on COVID-19. Hypertens Res:1–12.
View at Publisher | View at Google Scholar - Magadum A, Kishore R. (2020). Cardiovascular manifestations of COVID-19 infection. Cells. 9:2508.
View at Publisher | View at Google Scholar - Daugherty SE, Guo Y, Heath K, et al. (2021). Risk of clinical sequelae after the acute phase of SARS-CoV-2 infection: retrospective cohort study. BMJ;373: n1098.
View at Publisher | View at Google Scholar - Saeed S, Tadic M, Larsen TH, Grassi G, Mancia G. (2021). Coronavirus disease 2019 and cardiovascular complications: focused clinical review. J Hypertens.; 39:1282–1292.
View at Publisher | View at Google Scholar - Charfeddine S, Ibn Hadj Amor H, et al. (2021). Long COVID 19 Syndrome: Is It Related to Microcirculation and Endothelial Dysfunction? Insights From TUN-EndCOV Study. Front. Cardiovasc. Med. 8:745758.
View at Publisher | View at Google Scholar - Matsumoto C, Shibata S, Kishi T, et al. (2023). Long COVID and hypertension-related disorders: a report from the Japanese Society of Hypertension Project Team on COVID-19. Hypertens Res 46, 601–619
View at Publisher | View at Google Scholar - Beyerstedt S, Casaro EB, Rangel ÉB. (2021). COVID-19: angiotensin-converting enzyme 2 (ACE2) expression and tissue susceptibility to SARS-CoV-2 infection. Eur J Clin Microbiol Infect Dis. May;40(5):905-919. doi: 10.1007/s10096-020-04138-6. Epub. PMID: 33389262; PMCID: PMC7778857.
View at Publisher | View at Google Scholar - Akpek M. (2022). Does COVID-19 Cause Hypertension? Angiology, 73(7), 682–687.
View at Publisher | View at Google Scholar - Zuin M, Rigatelli G, Bilato C, et al. (2023). Risk of Incident New-Onset Arterial Hypertension After COVID-19 Recovery: A Systematic Review and Meta-analysis. High Blood Press Cardiovasc Prev 30, 227–233.
View at Publisher | View at Google Scholar - Delalić Đ, Jug J, & Prkačin, I. (2022). ARTERIAL HYPERTENSION FOLLOWING COVID-19:
A RETROSPECTIVE STUDY OF PATIENTS
IN A CENTRAL EUROPEAN TERTIARY CARE CENTER. Acta clinica Croatica, 61(Suppl 1), 23–27.
View at Publisher | View at Google Scholar - Kornilov S, Lucas I, Jade K, Dai CL, Lovejoy JC, Magis AT. Plasma levels of soluble ACE2are associated with sex, metabolic syndrome, and its biomarkers in a large cohort, pointing to a possible mechanism for increased severity in COVID-19. Critical care. 2020; 24:452.
View at Publisher | View at Google Scholar - Ackermann M, Verleden SE, Kuehnel M, et al. (2020). Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N Engl J Med.
View at Publisher | View at Google Scholar - Frasier KM, Gallagher-Poehls C, Cochrane M, et al. (2023) Secondary Vasculitis Attributable to Post-COVID Syndrome. Cureus 15(8): e44119.
View at Publisher | View at Google Scholar - Rogani S, Calsolaro V, Franchi R, et al. (2020). Spontaneous muscle hematoma in older patients with COVID-19: two case reports and literature review. BMC Geriatr 20, 539
View at Publisher | View at Google Scholar - Lim SW, & Wong E. (2020). Spontaneous Epidural Hematoma of the Cervical Spine in an Elderly Woman with Recent COVID-19 Infection: A Case Report. The American journal of case reports, 21, e926784.
View at Publisher | View at Google Scholar - Sabouri M, Rezvani M, Aminmansour B, Sourani A, Baradaran Mahdavi S. (2022). Spontaneous intramedullary hematoma in a patient with COVID-19 infection: A case report. Clin Case Rep. 10:e05387.
View at Publisher | View at Google Scholar - Sourani A, Rezvani M, Foroughi M, Baradaran Mahdavi S. (2022). Spontaneous intramedullary hematoma following COVID-19 vaccination: A case report. Clin Case Rep. 10: e06743.
View at Publisher | View at Google Scholar - Flores G, Kumar JI, Pressman E, et al. (2020). Spontaneous Brainstem Hemorrhagic Stroke in the Setting of Novel Coronavirus Disease 2019 – A Case Report. Cureus 12(10): e10809.
View at Publisher | View at Google Scholar - Leasure AC, Khan YM, Iyer R, et al. (2021). Intracerebral hemorrhage in patients with covid-19. Stroke, 52(7).
View at Publisher | View at Google Scholar - Reisi-Vanani V, Lorigooini Z, Dayani MA, et al. (2021). Massive intraperitoneal hemorrhage in patients with COVID-19: a case series. J Thromb Thrombolysis 52, 338–344.
View at Publisher | View at Google Scholar - Abrashev H, Ananiev J, Georgieva E. (2023). Case Report: Spontaneous Left Inferior Epigastric Artery Injury in a COVID-19 Female Patient Undergoing Anticoagulation Therapy. Journal of Clinical Medicine. 12(5):1842.
View at Publisher | View at Google Scholar - Fuentes-Martín Á, Cilleruelo Ramos Á, Soro-García J, Matilla González JM. (2022). Spontaneous giant chest wall hematomas in COVID-19 patients: case report. Shanghai Chest 6:15.
View at Publisher | View at Google Scholar - Friedman A, & Ulrich M. (2023). Case report: Spontaneous hemothorax following anticoagulation for microthrombi in severe COVID pneumonia. Respiratory medicine case reports, 44, 101864.
View at Publisher | View at Google Scholar - Mohan SA, Fadzaily ZS, & Abdullah Hashim SH. (2022). Spontaneous Haemothorax in a Patient with COVID-19. Case reports in medicine, 2022, 8275326.
View at Publisher | View at Google Scholar
