

Short Communication | DOI: https://doi.org/10.31579/2835-8325/018
Zinc(Ⅱ)-induced Neuroimmunological Renal Chronic Kidney Disease Prevention and Suppressive Progression
- Tsuneo Ishida *
2-3-6, Saido, Midori-Ku, Saitama-Shi, Saitama-Ken, 〒336-0907, Japan
*Corresponding Author: Tsuneo Ishida, 2-3-6, Saido, Midori-Ku, Saitama-Shi, Saitama-Ken, 〒336-0907, Japan
Citation: Tsuneo Ishida, (2023), Zinc(Ⅱ)-Induced Neuroimmunological Renal Chronic Kidney Disease Prevention and Suppressive Progression, Clinical Research and Clinical Reports, 2(3); DOI:10.31579/2835-8325/018
Copyright: © 2023, Tsuneo Ishida. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 May 2023 | Accepted: 17 May 2023 | Published: 30 May 2023
Keywords: Zinc(Ⅱ); CKD prevention; Serum zinc and creatinine levels; Egfr; urinary protein excretion; Stage 5 ESRD; Zn2+ ions-centered coordinated pattern
Abstract
Zinc(Ⅱ) supplementation with 30 mg/day should become likely therapeutic chronic kidney disease (CKD) prevention implications with immense importance of CKD-associated immunological and neurological complications. Zinc induced neuroimmunological suppressive CKD progression with Stage 2 ~ 3A, 3B, zinc supplementation (30 mg/day) may be beneficial for nutritional status in CKD children and adolescents, and zinc could reduce urinary protein excretion composed of albumin and/or minimize proteinuria excretion in proteinuric CKD. In CKD 4-5 stage, risk of cardiovascular disease (CVD) become higher that zinc supplementation of 25 mg/day in zinc homeostasis has a beneficial effect for CVD in vascular dysfunction. Thus, zinc intake of 30 mg/day and serum zinc level of 60~76 μg/dL could slow down CKD Stage 4 progression. Zinc induced CKD Stage 5 (eGFR < 15) is involved that zinc is actively bound to several proteins that the decrease of circulating zinc levels in CKD is partly caused by renal losses of zinc, becoming zinc-deficiency with advanced stage CKD and ESRD in CKD. Serum zinc and serum albumin levels are 37.4 ± 5.4 and 2.6 ± 0.6 µg/dL, respectively, for as eGFR 6.6 (5.2–8.3). Zn intake of 45-75 mg/day and serum zinc level of ≤78.3 µg/dL are beneficial for HD and maintenance hemodialysis (MHD) patients, in which Zinc 15 mg/day and Selenium 50–70 μg/day that are recommended may be thought to prevent ESRD stage. Zinc induced NAD(P)H oxidase (Nox) activation occurring ROS generation in CKD cell involves assembly that ROS include the superoxide anion (O2•–), hydrogen peroxide (H2O2), and hydroxyl radicals (OH•), and in the kidney.
Zinc(Ⅱ) ions-binding protein molecular mechanism is involved that Zn2+ ions-several protein complexes coordinated binding model of ligands of such as albumin, a-macroglobulin and transferrin in several proteins had been found on the binding specificity by Zn2+ ions-centered tetrahedral geometric coordination, in which causing zinc-activated serine, histidine and aspartate hydrogen residues enhance renal function activity and resulting inhibition of CKD progression proceeds.
Introduction
COVID-19 pandemic affects high mortality rate among older adults and individuals suffering from chronic kidney diseases (CKD) [1]. Neuroimmune interaction in acute kidney injury (AKI) is closely associated with various disorders, inflammatory CKD in neuroimmunology propose, neuromodulation that center on the cholinergic anti- inflammatory pathway (CAP) [2]. Immunological roles and nervous systems are directly related to homeostasis of renal physiology [3].
CKD is typically identified with serum chemistry profile and urine studies or as an incidental finding that having therapeutic patients clinical symptoms such as gross hematuria, a sign of albuminuria, nocturia, flank pain, or decreased urine output and CKD steps as ①GFR less than 60 mL/min/1.73 m2, ②albuminuria (ie, urine albumin ≥30 mg per 24 hours or urine albumin-to-creatinine ratio [ACR] ≥30 mg/g), ③abnormalities in urine sediment, histology, or imaging suggestive of kidney damage, ④renal tubular disorders; or ⑤kidney transplantation [4]. The CKD Practice Guide of Nephrology recommendation referral meets any of the following 3 criteria: ①0.5 g/g creatinine or higher, or proteinuria (≧ 2+), ②an estimated glomerular filtration rate of less than 50 ml/min/1.73m2, or ③positive results (≧ 1+) for both proteinuria and hematuria tests [5].
While, zinc element is important essential for human body that zinc homeostasis and zinc deficiency, the recommended dietary allowance (RDA) for zinc is of 11 mg/day for men and 8 mg/day for women, lower zinc intake is recommended for infants (2–3 mg/day) and children (5–9 mg/day) [6]. Elemental toxic zinc plays important roles for cardiovascular disease (CVD), bone disorders and oxidative stress in complications of CKD [7].
The efficacy of zinc supplementation for adequate zinc nutriture on the immune integrity of young pregnant women, the aged or those with any of the many diseases is just applicable, in which zinc supplementation significantly reduces infectious disease and other many severe diseases and may well reduce the impact of many severe diseases by preventing the dismantling of the immune system [8]. Due to the fact that zinc is liable to be bound to proteins in the plasma [9], glomerular filtration and consecutive urinary excretion are limited [10] that the zinc-protein binding complexes function as Zn-protein enzymes in the human body.
In this semi-review article, zinc(Ⅱ) induced neuroimmunological renal functional activities for CKD prevention and regulatory CKD development with CKD Stage 2, Stage 3A,3B, Stage 4, and Stage 5, ESRD are investigated, and subsequently, zinc-induced binding renal CKD suppressive progression molecular mechanism is clarified.
2. CKD (chronic kidney disease) development
CKD was defined as an estimated glomerular filtration rate (eGFR) of less than 60 mL/min/1.73 m2. that the classification of CKD depending on GFR value consists of Stage 1 — normal GFR (above 90 mL/min/1.73 m2) with persistent microalbumin, Stage 2 — GFR 60–89 mL/min/1.73 m2 with persistent microalbumin, Stage 3 — GFR 30–59 mL/min/1.73 m2, Stage 4 — GFR 15–29 mL/min/1.73 m2, and Stage 5 — GFR below 15 mL/min/1.73 m2 or end-stage renal disease (ESRD) [11].
The other, CKD stages have 1, 2, 3, 4, 5 stages / First stage, middle stage, final stage / Mild stage, moderate stage, severe stage /
Zinc induced CKD stages of mild stage, moderate stage, and severe stage have the probability of CKD regression and mortality far exceeded the risk of progression or kidney failure that CKD regression may be at least as common as CKD progression or kidney failure for mild to severe CKD [12]. Thus, low dietary zinc intake for normal renal function may increase the risk of CKD development.
Accordingly, CKD was defined as an estimated glomerular filtration rate (eGFR) of less than 60 mL/min/1.73 m2. Stage 1 CKD; eGFR 90 or greater, Stage 2 CKD; eGFR between 60 and 89, Stage 3 CKD; eGFR between 30 and 59, Stage 4; eGFR between 15 and 29, and Stage 5 CKD; eGFR less than 15.
3. Zinc induced immunological and neurological CKD prevention
Zinc induced immunological CKD that reduced renal function resulting from CKD causes marked alterations in the immune system, including inflammation and acquired immunosuppression. The immunosuppressed state accounts determine the morbidity and the mortality that is associated with CKD thatthe immune dysregulation was previously attributed to the effects of hemodialysis of the loss of kidney functions on immune responses may affect general immunity [13]. The kidney disease has important immune-mediated concepts of systemic immune and autoimmune disorders, including systemic autoimmunity and vasculitis, immune complex-related serum sickness and complement disorders with normal Zn 40-90 μg/dL immunity status.
CKD patients suffer from several neurological complications, including dementia, cognitive impairment, motor abnormalities, depression, and mood and sleep disturbances. Further, peripheral nervous system, have been suggested to impair neurotransmission, and thereby contribute to the neurological complications in CKD that are warranted for investigating the role of individual uremic toxins in causing the neurological complications [14]. In addition, elemental toxic zinc status in CKD development is under without Zn deficiency and Zn excess that plasma zinc levels and serum zinc levels are 0.82 ±0.04μg/mL, 43.4 mg/dL (lower serum zinc levels), respectively, in which low plasma zinc levels in CKD patients and abnormal blood-zinc level are the result of anemia [15].
Zinc(Ⅱ) has many effective actions for its antioxidant, anti-inflammatory, immunomodulatory, and antiviral activities that health human body is maintained by having neuroimmunology with immune system and neurological pathology, in which zinc ions promote immune system responses, neurogenesis, and antioxidant effects. Zinc(Ⅱ) ions could prevent to CKD that zinc can prevent the oxidative stress and the inflammatory response, the intensification of the immune response [16]. Zinc deficiency (ZnD) is a risk factor for CKD progression with the recommended zinc dose ranges from 1.5 to 7.7 mmol/day or 1 mg/kg/day in which 30 mg/day of zinc supplementation may benefit in the medication and prevention of the CKD [17]. Renal effect of zinc-activated metallothionein is involved in a significant positive correlation between metallothionen and eGFR, which is possibly influenced by Zn [18]. As low zinc intake has a significantly increased risk of incident CKD, the mean daily zinc intake and zinc intake density are assumed to be adapted to 8.6 ± 3.4 mg and 4.4 ± 0.9 mg/1000 kcal, respectively [19].
Thus, CKD prevention research should become therapeutic implications in the CKD prevention with immense importance of CKD-associated immunological and neurological complications.
4. Zinc induced neuroimmunological suppressive CKD progression with Stage 2~ 3A, 3B at 80~60~39 eGFR
All stages of CKD are correlated with increased risks of cardiovascular morbidity, premature mortality, have multiple atherosclerosis risk factors of inflammation, oxidative stress, in which Zn supplementation is benefited the nutritional status of HD patients providing anti-inflammatory and antioxidant effects and the Cholinergic Anti-inflammatory Pathway (CAP) is a neuroimmune pathway, containing the neuroimmune circuit and kidney disease for treating kidney disease [20].
Zinc induced reduced plasma zinc level, serum creatinine concentration in stage 2, 3 of CKD progressing have an anti-fibrotic effect in the liver and lungs that zinc may reduce the risk of fibrosis in patients with CKD and delay CKD progression, in which fibrosis in CKD is a progressive process that worsens not only the kidneys but also the heart, leading to zinc deficiency caused necrosis of kidney cells and exacerbated fibrosis by increasing kidney inflammation [21].
Serum zinc is 52.8 µg/dL at eGFR 30-44 that the serum zinc level is shown to be at CKD 2~ 3A, 3B Stage [22]. Low dietary zinc intake may increase the risk of CKD development in individuals with normal renal function that the mean serum Zn concentration in patients on maintenance HD was significantly with the cut-off point of 70 µg/dL [23]. In the patients, plasma zinc and serum creatinine concentrations are reduced in patients with chronic renal failure and zinc deficiency may be related to the degree of renal insufficiency [24].
The effect of zinc intake on serum zinc level 76 mg/dL, eGFR 30-59 and serum creatinine concentration at CKD mild stage becomes that Zinc intake <11> [25]. The protective effect of zinc is an effective clinical approach to reduce progression of vascular calcification (VC) and cardiovascular disease (CVD) in patients with CKD that zinc supplement (ZnSO4) ameliorated the osteoinductive effects of uremic serum in VC and vascular smooth muscle cells (VSMCs) with CKD patients [26].
Patients excreting large amounts of urinary protein should be considered at high risk for renal disease progression, in which
the upper limit of normal for total urinary protein excretion is 150 mg/24 h and the normal amount of albumin excretion is <30>300 mg/day are considered overt proteinuria or macroalbuminuria. Zinc could reduce urinary protein excretion and/or minimize proteinuria excretion in an important proteinuric CKD [27].
Zinc may reduce proteinuria in CKD that zinc levels are lower in CKD and account for zinc imbalance in CKD, in which this factor of urinary zinc excretion may be involved that an increase in zinc’s binding to alpha2-macroglobulin may reduce the amount of ultra-filterable zinc [28, 29].
Thus, zinc-deficiency at Stage 2-3 is that urinary zinc excretion was significantly higher in CKD patients and zinc fractional excretion was stable in the early stage of CKD, then a sudden and strong increase was seen in stage 3 patients [30].
Accordingly, at Stage 2~3, zinc supplementation (30 mg/day) may be beneficial for nutritional status in CKD children and adolescents, in which zinc could reduce urinary protein excretion composed of albumin and/or minimize proteinuria excretion in a proteinuric CKD.
5. Zinc induced suppressive CKD progressing of Stage 4 at eGFR=29~15.
In CKD 4-5 stage, risk of CVD become higher that Zn supplementation in the process of recovery from CVDs would be most beneficial primarily for the prevention and appropriate dietary recommendations can attain sufficient levels of dietary Zn in daily diets and potentially diminish the risk of developing CVDs [31]. Zinc supplementation of 25 mg/day in zinc homeostasis has a beneficial effect for CVD in vascular dysfunction [32].
Zinc induced neuroimmunelogical suppressive CKD progression may be accomplished that CKD is slowly progressive and leads neph loss, end-stage renal disease and pre-dialysis. Zinc intake has been shown to occure increased urinary excretion that the effect of zinc supplementation on kidney function in advanced stage CKD and pre-dialysis CKD is needed to determine [33]. Plasma zinc and urine zinc contents decrease with CKD progressing that urine zinc-deficiency with urinary zinc excretion in CKD can be reduced and stopped in renal activity.
Zinc balance in uremic animals is primarily determined by nutritional zinc, in which the inverse association between urinary zinc excretion and uromodulin possibly points to an impaired tubular activity, which could partly account for zinc imbalance in CKD and zinc levels are lower in CKD by reduced renal zinc excretion [34].
Thus, zinc supplementation greater than 45 mg/day may be necessary to increase the serum zinc level in hemodialysis patients.
As zinc levels are lower in CKD, and not compensated by reduced renal zinc excretion and uromodulin possibly points which could partly account for zinc imbalance in CKD [28].
Accordingly, at CKD Stage 4, zinc intake of 30 mg/day and serum zinc level of 60~76 μg/dL could slow down CKD progression.
6. Zinc induced nutritional CKD Stage 5 (eGFR < 15>
At ESRD Stage, in order to optimize care for neurological and renal improved outcomes, considering with brain-kidney interactions may be necessary for renal function and outcomes after neurological injury [35]. Zinc supplementation benefits the nutritional status of maintenance hemodialysis (MHD), leads to an anti-inflammatory and anti-oxidative effect in MHD [36].
CKD on cerebrovascular and neurological complications has been identified to the factor the uraemic toxins accumulated in the blood in ESRD [37].
The causes of PEW in dialysis patient with nutritional problems in CKD Stage 5 are involved that morbidity and mortality in HD patients can be reduced, early administration of nutritional support and a rationalized timing of Oral Nutritional Supplement (ONS) consumption may improve the efficacy of nutritional support. The main perspectives for the treatment of PEW during dialysis may be the development of specific ONS for dialysis patients, a multimodal therapy including nutritional support, exercise, anabolic agents and the use of daily dialysis in selected HD patients [38].
Serum zinc (Zn) levels tend to be low in CKD patients that Zinc induced end-stage renal disease (ESRD) is involved in eGFR below 15 mL/min/1.73 m2 or ESRD that the mean Zn level was 59.6 μg/dl and the median eGFR was 20.3 ml/min/ 1.73 m2 [39].
Moreover, zinc supplementation reduces urinary albumin excretion and zinc supplementation may protect against the exacerbation of renal dysfunction, in which CKD is a significant risk factor for end-stage renal disease (ESRD) and cardiovascular disease (CVD) and prevention of CKD progression [39].
In addition, elemental toxic zinc plays a role for hemodialysis in CKD renal failure that serum zinc levels are 86.83 g/dL
before HD, 82.70 after HD, serum creatinine levels 12.46 before HD, 5.90 mg/dL after HD, in which reduction of serum zinc levels in CKD patients, increase of serum zinc levels in uremic patients after HD, and average blood concentrations of important trace elements like copper and zinc are recognized in hemodialysis patients [40].
Zinc induced ESRD functional activity is involved that Serum zinc concentration is baseline serum zinc levels: tertile, <45>, serum zinc and serum albumin levels are 37.4 ± 5.4 and 2.6 ± 0.6 µg/dL, respectively, in which Zinc 15 mg/day and Selenium 50–70 μg/day are recommended such as micronutrient supply in adult patients on hemodialysis and peritoneal dialysis and in children with hemodialysis patients aged between 5 and 18 years old, given daily zinc supplementation of 50–100 mg for 90 days found that serum zinc was significantly increased from 53.2 ± 8.15 to 90.75 ± 12.2 µg/dL (p= 0.001). In addition, serum zinc level in HD patient has been recommended as a serum zinc range (≤78.3 µg/dL) [22].
Thus, zinc can prevent ESRD, in which serum zinc range (≤78.3 µg/dL) and daily zinc supplementation of 50–100 mg for 90 days found that serum zinc was significantly increased from 53.2 ± 8.15 to 90.75 ± 12.2 µg/dL (p= 0.001), and Zinc 15 mg/day and Selenium 50–70 μg/day are recommended as micronutrient supply.
Accordingly, zinc intake of 45-75 mg/day and serum zinc level of ≤78.3 µg/dL are beneficial for HD and MHD patients, in which Zinc 15 mg/day and Selenium 50–70 μg/day that are recommended may be thought to prevent ESRD stage.
7. Zinc induced ROS generation in CKD progression
Zinc induced NAD(P)H oxidase activation occurring ROS generation in CKD cell involves assembly of enzyme’s membrane-associated subunits with cytosolic subunits that ROS are by-products of aerobic metabolism and include the superoxide anion (O2•–), hydrogen peroxide (H2O2), and hydroxyl radicals (OH•), and in the kidney, mitochondria and the NOX family are the major sources of endogenous ROS. For NADPH Oxidases, seven different NOX homologues have been characterized (NOX1–NOX5, DUOX1, and DUOX2) with different activation mechanisms, heterogeneous tissue distribution and subcellular localizations. NOX4 is the principal NOX isoform in the kidney [41]. NAD(P)H Oxidase is activated by ROS production in endothelial vascular smooth muscle and renal parenchymal cells that zinc induced NADPH oxidase activation can reduce chronic inflammation and oxidative stress in CKD [42]. The other, NADPH oxidases play a critical role in kidney damage and Nox2-containing NADPH oxidase plays a role in cyclosporine induced kidney damage, while Nox4-containing NADPH oxidase is involved in diabetes-induced kidney damage [43].
8. Zinc ions-proteins binding molecular mechanism with CKD suppressive development
Zinc induced zinc ions-proteins interaction complexes are formed that Zn2+ ions tend to bind many proteins by zinc ions-protein interaction in CKD blood. The zinc ions complexes may play important role that Zn2+ ions-protein complexes are liable to form for this Zn2+ ions-centered coordination pattern that the zinc-coordinating inhibitor of tetrahedral zinc sites is tetrahedrally coordinated binding to such as the catalytic triad of zinc-activated Serine, Histidine and Aspartate Hydrogen Residues.
Thus, Zinc(Ⅱ) ions-binding protein molecular mechanism is involved that Zn2+ ions-several protein complexes coordinated binding model of ligands of such as albumin, a-macroglobulin and transferrin in several proteins had been found on the binding specificity by Zn2+ ions-centered tetrahedral geometric coordination for this Zn2+ ions-centered coordination pattern that the decrease of circulating zinc levels in CKD is partly caused by renal losses of zinc, becoming zinc-deficiency in CKD, and possibly due to impairment in tubular reabsorption.
Accordingly, as mentioned above, zinc induced nutritional and neuroimmunological renal effects on CKD prevention and CKD suppressive development with CKD Stage 2~3, CKD Stage 4, and CKD Stage 5 ESRD, respectively, are represented in Table 1, including the zinc ions-binding molecular mechanism.
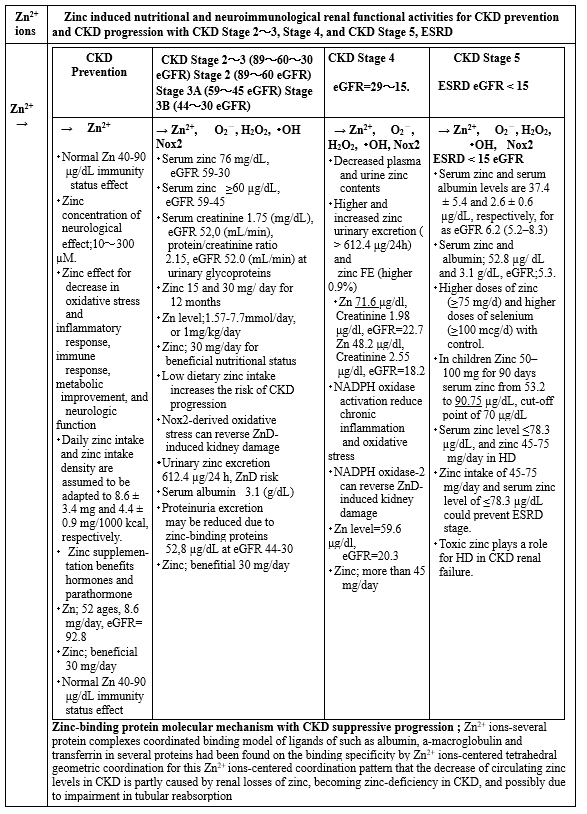
Table 1: Zinc induced neuroimmunological renal effects for CKD prevention and CKD suppressive development
Conclusions
Zinc(Ⅱ) induced nutritional, neuroimmunological renal activities for CKD prevention and suppressive CKD progression with CKD Stage 2, Stage 3A and 3B, Stage 4, and Stage 5, ESRD are elucidated, subsequently the zinc induced binding protein molecular mechanism has been clarified.
Zinc induced nutritional, immunological, and neurological CKD prevention is involved that zinc supplementation with 30 mg/day may benefit a metabolic improvement, a decrease in CVD, the neurologic function, and prevention of the CKD. The role of zinc in neurological diseases CKD prevention research should become likely therapeutic CKD prevention implications with immense importance of CKD-associated immunological and neurological complications.
Zinc induced nutritional, neuroimmunological suppressive CKD progression with Stage 2~3A,3B is involved that Zn supplementation is benefited the nutritional status of hemodialysis (HD) patients providing anti-inflammatory and antioxidant effects, containing the neuroimmune circuit with kidney disease. Zinc supplementation (30 mg/day) may be beneficial for nutritional status in CKD children and adolescents, in which at the level of urinary protein excretion, zinc could reduce urinary protein excretion composed of albumin and/or minimize proteinuria excretion in an important therapeutic management of proteinuric CKD.
Zinc induced neuroimmunelogical CKD suppressive progressing of Stage 4 is involved that CKD is slowly progressive and leads irreversible nephloss, end-stage renal disease and pre-dialysis. In CKD 4-5 stage, risk of CVD become higher that Zn supplementation in the process of recovery from CVDs would be most beneficial primarily for the prevention and appropriate dietary recommendations can attain sufficient levels of dietary Zn in daily diets and potentially diminish the risk of developing CVDs and zinc supplementation of 25 mg/day in zinc homeostasis has a beneficial effect for CVD in vascular dysfunction. Thus, zinc intake of 30 mg/day and serum zinc level of 60~76 μg/dL could slow down CKD progression.
Zinc induced CKD Stage 5 and ESRD Stage (eGFR < 15>
In addition, elemental toxic zinc plays a role for hemodialysis in CKD renal failure.
Thus, zinc intake of 45-75 mg/day and serum zinc level of ≤78.3 µg/dL are beneficial for HD and MHD patients, in which Zinc 15 mg/day and Selenium 50–70 μg/day that are recommended may be thought to be able to prevent ESRD stage, and elemental toxic zinc plays specially for HD in CKD renal failure.
Zinc induced NAD(P)H oxidase activation occurring ROS generation in CKD cell involves assembly that ROS include the superoxide anion (O2•–), hydrogen peroxide (H2O2), and hydroxyl radicals (OH•), and in the kidney, the NADPH oxidase (Nox) family are the major sources of endogenous ROS.
Zinc(Ⅱ) ions-binding protein molecular mechanism is involved that Zn2+ ions-several protein complexes coordinated binding model of ligands of such as albumin, a-macroglobulin and transferrin in several proteins had been found on the binding specificity by Zn2+ ions-centered tetrahedral geometric coordination. The decrease of circulating zinc levels in CKD is partly caused by renal losses of zinc, becoming ZnD in CKD, and possibly due to impairment in tubular reabsorption, in which causing zinc-activated serine, histidine and aspartate hydrogen residues enhance renal function activity and resulting inhibition of CKD progression proceeds.
Abbreviations
ACR=albumin-to-creatinine ratio, AKI=acute kidney injury, BMI=body mass index, BP=blood pressure, CAP=Cholinergic Anti-inflammatory Pathway, CKD=chronic kidney disease, CAPD=continuous ambulatory peritoneal dialysis, CRF= chronic renal failure, CRP=C-reactive protein, CVD=cardiovascular disease, DM=diabetes mellitus, DN=diabetic nephropathy, eGFR=estimated glomerular filtration rate, ESRD=end-stage renal disease, FE=fractional excretion, HD= hemodialysis, MHD=maintenance hemodialysis, NADPH= nicotinamide adenine dinucleotide phosphate, Nox=NADPH oxidase, ONS=oral nutritional supplement, OS=oxidative stress, PEW=Protein-Energy Wasting, PSD=postsynaptic density, RCTs= randomized controlled trials, RDA=recommended dietary allowance, ROS=reactive oxygen species, VC=vascular calcification, VSMCs=vascular smooth muscle cells, ZnD=zinc deficiency.
Conflicts of Interest
The author declares there is no conflicts of interest.
Sources of funding: No source funding for this article, author's own expenses.
References
- Hassan Askari, Nima Sanadgol, Asaad Azarnezhad, Amir Tajbakhsh, Hossein Rafiei, et al. (2021). kidney diseases and COVID-19 infection: causes and effect, supportive therapeutics and nutritional perspectives Heliyon, 7:1-15.
View at Publisher | View at Google Scholar - Hong Xu, Sara Garcia-Ptacek, Annette Bruchfeld, Edouard L. Fu, Taher Darreh Shori, Bengt Lindholm, Maria Eriksdotter, and Juan Jesus Carrero. (2023). Association between cholinesterase inhibitors and kidney function decline in patients with Alzheimer’s dementia Kidney International, 103:166-176.
View at Publisher | View at Google Scholar - Sho Hasegawa, Tsuyoshi Inoue, Reiko Inagi. (2019). Neuroimmune interactions and kidney disease Kidney Research Clinical Practice, 38(3): 282-294.
View at Publisher | View at Google Scholar - Teresa K. Chen, Daphne H. Knicely, Morgan E. Grams. (2019). Chronic Kidney Disease Diagnosis and Management: A Review JAMA. 322(13): 1294-1304.
View at Publisher | View at Google Scholar - Kunitoshi ISEKI. (2011). Role of Urinalysis in the Diagnosis of Chronic Kidney Disease (CKD) JMAJ, January/February, 54(1): 27-30.
View at Publisher | View at Google Scholar - Paun S, Tudosie M, Petris R, Macovei R. (2015). The effects of Zinc on human body, including on renal failure and renal transplantation Journal of Medicine and Life, 137-140.
View at Publisher | View at Google Scholar - Adwalia Fevrier-Paul,Adedamola K Soyibo, Sylvia Mitchell, Mitko Voutchkov. (2018). Role of Toxic Elements in Chronic Kidney Disease Journal of Health & Pollution, 8:20: 1-6.
View at Publisher | View at Google Scholar - Pamela J. Fraker,3 Louis E. King, Tonya Laakko and Teresa L. Vollmer. (2000). The Dynamic Link between the Integrity of the Immune System and Zinc Status, J. Nutr. 130:1399-1406.
View at Publisher | View at Google Scholar - Barnett JP, Blindauer CA, Kassaar O et al. (2013). Allosteric modulation of zinc speciation by fatty acids. Biochim Biophys Acta, 1830: 5456-5464.
View at Publisher | View at Google Scholar - King JC, Shames DM, Woodhouse LR. (2000). Zinc homeostasis in humans. J Nutr, 130: 1360-1366.
View at Publisher | View at Google Scholar - Stanisław Niemczyk, Longin Niemczyk, Katarzyna Romejko-Ciepielewska. (2012). Basic endocrinological disorders in chronic renal failure Polish Journal of Endocrinology, 63(3): 250-257.
View at Publisher | View at Google Scholar - Ping Liu, Rob R. Quinn, Ngan N. Lam, Huda Al-Wahsh, et al. (2021). Progression and Regression of Chronic Kidney Disease by Age Among Adults in a Population-Based Cohort in Alberta, Canada Nephrology, 4(6): 1-13.
View at Publisher | View at Google Scholar - Christian Kurts, Ulf Pallnzer, Hans-Joachim Anders and Andrew J.Rees. (2013). The immune system and kidney disease: basic concepts and clinical implications Immunology, 13: 739-755.
View at Publisher | View at Google Scholar - Muhammed Khairujjaman Mazumder, Rajib Paul, Pallab Bhattacharya & Anupom Borah. (2019). Neurological sequel of chronic kidney disease: From diminished Acetylcholinesterase activity to mitochondrial dysfunctions, oxidative stress and inflammation in mice brain Scientific Reports, 9(1): 1-22.
View at Publisher | View at Google Scholar - Sen-Shyong Jeng, and Yen-Hua Chen. (2022). Association of Zinc with Anemia Nutrients. 14:1-18.
View at Publisher | View at Google Scholar - L. C. Neto, M. R. Bacci, L. C. Sverzutt, M. G. Costa1, B. C. A. Alves, F. L. Fonseca. (2016). The Role of Zinc in Chronic Kidney Disease Patients on Hemodialysis: A Systematic Review Health, 8: 344-352.
View at Publisher | View at Google Scholar - Xiuli Zhang, Dan Liang, Xu Lian, Zhi-Hong Chi, Xuemei Wang, Yue Zhao and Zhang Ping. (2016). Effect of zinc deficiency on mouse renal interstitial fibrosis in diabetic nephropathy Molecular Medicine Reports, 14: 5245-5252.
View at Publisher | View at Google Scholar - Moritz Schanz, Lea Schaaf, Juergen Dippon, Dagmar Biegger, Peter Fritz et al. (2017). Renal effects of metallothionein induction by zinc in vitro and in vivo BMC Nephrology, 1:1-8.
View at Publisher | View at Google Scholar - Young Su Joo, Hyung Woo Kim, Sangmi Lee, Ki Heon Nam, Hae-Ryong Yun, Jong Hyun Jhee et al. (2021). Dietary zinc intake and incident chronic kidney disease Clinical Nutrition, 40:1039-1045.
View at Publisher | View at Google Scholar - Yasuna Nakamura, and Tsuyoshi Inoue. (2020). Neuroimmune Communication in the Kidney JMA Journal, 3(3):164-175.
View at Publisher | View at Google Scholar - Yi Xie, Fei Liu, Xiaojing Zhang, Yanyan Jin, Qiuyu Li, Huijun Shen, Haidong Fu, Jianhua Mao. (2022). Benefits and risks of essential trace elements in chronic kidney disease: a narrative review Ann Transl Med, 10(24): 1-25.
View at Publisher | View at Google Scholar - Tatsunori Toida, Reiko Toida, Shou Ebihara, Risa Takahashi, Hiroyuki Komatsu, Shigehiro Uezono, Yuji Sato and Shouichi Fujimoto. (2020). Association between Serum Zinc Levels and Clinical Index or the Body Composition in Incident Hemodialysis Patients Nutrients, 12: 1-11.
View at Publisher | View at Google Scholar - Simin Dashti-Khavidaki, Hossein Khalili, Seyedeh-Maryam Vahedi, Mahboob LessanPezeshki. (2010). Serum Zinc Concentrations in Patients on Maintenance Hemodialysis and its Relationship with Anemia, Parathyroid Hormone Concentrations and Pruritus Severity Sauji J. Kidney Diseases and Transplantation, 21(4): 641-645.
View at Publisher | View at Google Scholar - P. Gill, F. Fagiol. E. De Paoli Vital. A. Farinel. (1985). Is Zinc Status a Problem in the Dietary Treatment of Chronic Renal Failure? Nephron, 40: 382.
View at Publisher | View at Google Scholar - Yiying Zhang, Yan Liu and Hongbin Qiu. (2018). Association between Dietary Zinc Intake and Hyperuricemia among Adults in the United States Nutrients,10: 1-12.
View at Publisher | View at Google Scholar - Jakob Voelkl, Rashad Tuffaha, Trang T.D. Luong, Daniel Zickler, Jaber Masyout, Martina Feger, Nicolas Verheyen, Florian Blaschke, Makoto Kuro-o et al. (2018). Zinc Inhibits Phosphate-Induced Vascular Calcification through TNFAIP3-Mediated Suppression of NF-kB J Am Soc Nephrol 29: 1636-1648.
View at Publisher | View at Google Scholar - Biff F. Palmer. (2007). Proteinuria as a Therapeutic Target in Patients with Chronic Kidney Disease American Journal of Nephrology, 27: 287-293.
View at Publisher | View at Google Scholar - Katerina Damianaki, Joao Miguel Lourenco, Philippe Braconnier, Jean-Pierre Ghobri et al. (2020). Renal handling of zinc in chronic kidney disease patients and the role of circulating zinc levels in renal function decline Nephrol Dial Transplant, 35(7):1163-1170.
View at Publisher | View at Google Scholar - Mahmoud Parham, Massoud Amini, Ashraf Aminorroaya and Esfandiar Heidarian. (2008). Effect of Zinc Supplementation on Microalbuminuria in Patients with Type 2 Diabetes: A Double Blind, Randomized, Placebo-Controlled, Cross-Over Trial Review of Diabetic Studies, 5: 102-108.
View at Publisher | View at Google Scholar - Alice Bonanni, Irene Mannucci, Daniela Verzola, Antonella Sofia, Stefano Saffioti et al. (2011). Protein-Energy Wasting and Mortality in Chronic Kidney Disease Int. J. Environ. Res. Public Health, 8: 1631-1654.
View at Publisher | View at Google Scholar - Joachim Jankowski, Jürgen Floege, Danilo Fliser, Michael Böhm, Nikolaus Marx. (2021). cardiovascular disease in Chronic Kidney Disease Pathophysiological Insights and Therapeutic Options Circulation, 143: 1157-1172.
View at Publisher | View at Google Scholar - Marija Knez and Maria Glibetic. (2021). Zinc as a biomaker of cardiovascular health frontiers in nutrition, 8:606878:1-7.
View at Publisher | View at Google Scholar - Shinya Nakatani, Katsuhito Mori, Tetsuo Shoji, and Masanori Emoto. (2021). Association of Zinc Deficiency with Development of CVD Events in Patients with CKD Nutrients, 13: 1-21.
View at Publisher | View at Google Scholar - AUL L. KIMMEL, DON W. WATKINS, ELIZABETH B. TELLER, Rsjiv KHANNA, STEFAN DOSA, and TERENCE M. PHILLIPS. (1988). Zinc balance in combined zinc deficiency and uremia Kidney International, 33: 1091-1099.
View at Publisher | View at Google Scholar - Sara Stern-Nezer. (2021). Chronic and End-Stage Kidney Disease in the Neurological Intensive Care Unit Journal of Stroke and Cerebrovascular Diseases, 30:9: 1-6.
View at Publisher | View at Google Scholar - Ling-Jun Wang, Ming-Qing Wang, Rong Hu, Yi Yang, Yu-Sheng Huang, Shao-Xiang Xian, and Lu Lu. (2017). Effect of Zinc Supplementation on Maintenance Hemodialysis Patients:A Systematic Review and Meta-Analysis of 15 Randomized Controlled Trials BioMed Research International, 1-12.
View at Publisher | View at Google Scholar - Sophie Liabeuf, Marion Pepin, Casper F.M. Franssen, Davide Viggiano, Sol Carriazo, et al. (2021). chronic kidney disease and neurological disorders: are uraemic toxins the missing piece of the puzzle? Nephrol Dial Transplant,37:33-44.
View at Publisher | View at Google Scholar - Anne-Elisabeth Heng and Noel J. M. Cano. (2010). Nutritional problems in adult patients with stage 5 chronic kidney disease on dialysis (both haemodialysis and peritoneal dialysis) Nephrology Dialysis Transplation (NDT), 3: 109-117.
View at Publisher | View at Google Scholar - Atsuyuki Tokuyama, Eiichiro Kanda, Seiji Itano, Megumi Kondo et al. (2021). Effect of zinc deficiency on chronic kidney disease progression and effect modification by hypoalbuminemia PLOS ONE, 16(5): 1-13.
View at Publisher | View at Google Scholar - Rajashri B. Bhogade,Adinath N. Suryakar, Nitin G. Joshi. (2013). Effect of Hemodialysis on Serum Copper and Zinc Levels in Renal Failure Patients European Journal of General Medicine, 10(3):154-157.
View at Publisher | View at Google Scholar - Maria V. Irazabal, and Vicente E. Torres. (2020). Review Reactive Oxygen Species and Redox Signaling in Chronic Kidney Disease Cells, 9(6):1-17.
View at Publisher | View at Google Scholar - Yonova, Trendafilov, Georgieva, Dimitrova, Arabadjieva and Velkova. (2018). Oxidative stress (OS) in chronic kidney disease (CKD): A mini review Nephrology and Renal Diseases, 3(3):1-3.
View at Publisher | View at Google Scholar - Mirandy S. Li, Sherry E. Adesina, Carla L. Ellis, Jennifer L. Gooch, Robert S. Hoover, and Clintoria R. Williams. (2017). NADPH oxidase-2 mediates zinc deficiency-induced oxidative stress and kidney damage Am J Physiol Cell Physiol, 312: 47-55.
View at Publisher | View at Google Scholar
