

Research Article | DOI: https://doi.org/10.31579/2835-835X/080
Warts: Review and Update
Anthony kodzo-grey venyo. Retired urologist; medical examiner member or the royal college of pathologists of london. United kingdom.
*Corresponding Author: Yahoo Vvarning, Anthony kodzo-grey venyo. Retired urologist; medical examiner member or the royal college of pathologists of london. United kingdom.
Citation: Yahoo Vvarning, (2025), Warts: Review and Update, Clinical Trials and Case Studies, 4(6); DOI:10.31579/2835-835X/080
Copyright: © 2025, Yahoo Vvarning. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 October 2025 | Accepted: 07 November 2025 | Published: 13 November 2025
Keywords: behaviours; human food matrices; staphylococcus aureus
Abstract
Warts, which are generally caused by human papillomavirus (HPV) infections, represent a common dermatological condition associated with a substantial impact upon individuals and healthcare systems within the world including developing countries. Warts afflict millions of individuals within developed and developing countries, and they tend to pose physical discomfort, psychological distress, as well as potential complications. Even though rarely life-threatening, warts could significantly impair the quality of life of afflicted individuals. The burden of warts does extend beyond clinical symptoms, with economic and humanistic implications. Costs that tend to be associated with diagnosis, treatment, and missed workdays attributable to visible warts could strain already limited healthcare resources and hinder socioeconomic development. Warts emanate from HPV infection, which are primarily transmitted via direct skin contact. Risk factors associated with warts include poor hygiene, immunosuppression, and coital behaviours, with genital warts linked to increased HPV-related cancer risk. While warts are considered to be generally benign, they could be associated with complications, including: pain, bleeding, secondary infections, as well as psychosocial distress. Untreated warts may be ensued by scarring and impact upon the individual’s mental well-being. Warts manifest in variety of forms, including: common, plantar, flat, and genital warts. Clinical diagnosis of warts has quite often tended to be straightforward, but biopsy of the warty lesion may be required for pathology examination in atypical cases to confirm the diagnosis of warts. Management options of warts include: non-pharmacological approaches (for example, cryotherapy, salicylic acid) and pharmacological treatments (for example, imiquimod, podophyllin). Monitoring parameters and patient education constitute part of effective management approach. Excision of warts does constitute effective management and confirmation of correct diagnosis of warts. It is important to appreciate the fact that warts could simulate a number of differential diagnoses including malignant lesions and hance correct diagnosis of warts is important for appropriate and correct management of patients afflicted by warts. education, vaccination programs, telemedicine, community engagement, local treatment modalities, training, data collection, stigma reduction, and partnerships.
Introduction
Warts are benign proliferations of skin and mucosa that are stated to be caused by the human papillomavirus (HPV). It has been iterated that at present, more than 100 types of HPV had been identified. [1,2] Certain HPV types are iterated to tend to afflict the skin at particular anatomic sites; nevertheless, warts of any HPV type may afflict any site. The primary clinical presentations of HPV infection include common warts, genital warts, flat warts, and deep palmoplantar warts (myrmecia). Less common documented presentations of HPV infection include the ensuing: focal epithelial hyperplasia (Heck disease), [3] epidermodysplaia verruciformis, as well as plantar cysts. It has been iterated that warts are transmitted by means of direct or indirect contact, and predisposing factors for the development of warts include disruption to the normal epithelial barrier. [1] It has been pointed out that the therapy of warts is difficult, with frequent failures and recurrences. Many warts, nevertheless, are known to resolve spontaneously within a few years even without treatment. [1] A small number of high-risk HPV subtypes had been iterated to be associated with the development of malignancies, including types 6, 11, 16, 18, 31, and 35. Malignant transformation of warts most commonly is encountered in patients with genital warts and in immunocompromised patients. [1] HPV types 5, 8, 20, and 47 had been stated to have oncogenic potential in patients with epidermodysplasia verruciformis. [1] It has been documented that warts could afflict any area on the skin and mucous membranes. The HPV virus is stated to infect the epithelium, and systemic dissemination of the virus does not emanate. [1] Viral replication is stated to occur within differentiated epithelial cells in the upper level of the epidermis; nevertheless, it has been pointed out that viral particles can be found within the basal layer. [1] The ensuing summations had been made regarding the aetiology of warts:
- Warts are caused by HPV, which is a double-stranded, circular, supercoiled DNA virus enclosed in an icosahedral capsid and comprising 72 capsomers.
- More than 100 types of HPV had been identified. The ensuing wart types and HPV types need to be known about:
- Common warts - HPV types 2 and 4 (most common), followed by types 1, 3, 27, 29, and 57
- Deep palmoplantar warts (myrmecia) - HPV type 1 (most common), followed by types 2, 3, 4, 27, 29, and 57
- Flat warts - HPV types 3, 10, and 28
- Butcher's warts - HPV type 7 (although some data suggest the association may be weak)
- Focal epithelial hyperplasia (Heck disease) - HPV types 13 and 32
- Cystic warts - HPV type 60
Warts are known to be widespread within the entire world. It has been iterated that even though the frequency of warts is not known, warts had been estimated to afflict about 7 percent to 12 percent of the population. [1] In school-aged children, the prevalence of warts is stated to be between 10 percent and 20 percent. [1] An increased frequency of warts had also been iterated to have been observed among immunosuppressed patients and meat handlers. [1]
It has been iterated that even though warts may afflict individuals of any race, common warts appear about twice as frequently in whites as in blacks or Asians. [4] Focal epithelial hyperplasia (Heck disease) has been stated to be more prevalent among American Indians and Inuit. [3] The male-to-female ratio approaches of warts has been stated to be 1:1. [1] It has been documented that warts can occur at any age. [] Warts are stated to be unusual in infancy and early childhood, with an increase in incidence among school-aged children, and a peak at 12 years to 16 years. [1,5]
It has been iterated that about 65 percent of warts disappear spontaneously within 2 years and that when warts resolve on their own, no scarring is visualised. [1] It has also been documented that scarring can occur as a result of different methods of treatment of warts. [1] It has furthermore been iterated that growth of periungual or subungual warts may emanate in permanent nail dystrophy. [1]
It has been iterated that failures of treatment of warts and wart recurrences are common, more so among immunocompromised patients [1]. It has furthermore been iterated that normal appearing peri-lesional skin may harbour HPV, which helps explain recurrences. [1]
It has been iterated that common warts usually tend to be asymptomatic; however, warts may cause cosmetic disfigurement or tenderness. [1] It has been stated that plantar warts could be painful, and extensive involvement of warts upon the sole of the foot might impair ambulation. [1] It has been iterated that malignant change in non-genital warts is rare; however, it has been reported and is termed verrucous carcinoma. [1,6-8] Verrucous carcinoma is stated to be regarded as a slow-growing, locally invasive, well-differentiated squamous cell carcinoma which may be easily mistaken for a common wart. [1] Warts, cancer can occur anywhere upon the skin but wart is most commonly encountered upon the plantar surfaces. [1] Even though this type of cancer rarely metastasizes, it can be locally destructive. [1] Considering that warts simulate various lesions of the body and one of the differential diagnosis of warts is a malignant lesion, it is important that clinicians all over the world should be familiar with the clinical features, management and outcome following treatment of warts. The ensuing article has been divided into two parts (A) Overview and (B) Miscellaneous narrations and discussions from some case reports, case series, and studies related to warts.
AIM
To review and update the literature on warts.
Method
Internet data bases were searched including: Google; Google scholar; Yahoo; and PUBMED. The search words that were used included: Warts, warty dyskeratoma, cutaneous warts, genital warts, and mucosal warts. Seventy-eight (78) references were identified which were used to write the article which has been divided into two parts: (A) Overview and (B) Miscellaneous narrations and discussions from some case reports, case series, and studies related to warts.
Results
[A] OVERVIEW
Definition / general statements
The ensuing general iterations had been made about warts which are also referred to as verrucae [9]
- A wart is stated to be a common viral infection of skin and mucosal epithelial cells [10]
- Wart is iterated to be caused by human papilloma virus (HPV) [10]
- Most wart infections are stated to generally clear within 2 years. [11]
Essential features
The essential features of warts had been summated as follows: [9]
- Warts are stated to be flesh coloured papules that tend to be associated with a rough surface or rough surfaces
- Warts are stated to be caused by HPV infection
- Common and plantar warts are stated to be caused by: HPV 1, 2, 4 and 7 [12]
- Genital warts are said to be caused by: HPV 6 and 11 [11]
- Hands and feet are documented common sites for the development of warts.
- Koilocytes are iterated to be a characteristic histological finding in the pathology examination of specimens of wart.
Terminology
Some of the terminologies that tend to be used for warts include the ensuing: [9]
- Verruca vulgaris: common wart
- Condyloma acuminata: genital warts
- Verruca palmaris / verruca plantaris: palmar / plantar warts
- Myrmecia: special type of palmoplantar wart
- Verrucae planae: Plane warts
Epidemiology
The epidemiology of wart had been summated as follows: [9]
- It has been iterated that wart constitutes 7% to 12% of the population, and children tend to be more afflicted by warts than adults. [13]
- It has been documented that genital warts are sexually transmitted infections (STIs)
- Most common STI in U.S.A is stated to affect about 40% of sexually active individuals [11]
Sites
The sites of the body afflicted by wart had been summated as follows: [9]
- Common warts: any site, especially hands, fingers, knees and elbows. [14]
- Palmar / plantar: These warts afflict the palms, and soles. [14]
- Flat / plane warts: These types of warts afflict dorsal hands, and face. [14]
- Genital warts: Genital warts are stated to afflict external genitals, perineum, perianal, groin, mons, vagina, urethra, anal canal [11]
- Oral warts: Oral warts are stated to afflict any oral surface. [11]
Pathophysiology
The pathophysiology of wart had been summated as follows: [9]
- Wart is stated to spread via direct contact (sexual, skin to skin / fomite)
- HPV is stated to invade the epidermal basal cells through micro-abrasions; induces hyperplasia and hyperkeratosis
- Most wart infections are stated to be cleared by immune response
- It has been iterated that in warts, the virus binds to the receptor and the virus is then internalized into the cell by endocytosis and then the viral genome enters the nucleus
- It has been iterated that E6 and E7 HPV proteins hijack the checkpoint mechanisms of the cell cycle and this is ensued by uncontrolled proliferation
- It has been documented that viral genome replication emanates with increased levels of the E1, E2, E4 and E5 proteins
- It has been iterated that in the terminally differentiated layer of epithelium L1 and L2 capsid proteins are expressed and viral particles are assembled
- It has been stated that the virions are sloughed off with the dead squamous cells of the host epithelium for further transmission. [15]
Aetiology
The aetiology of wart had been summated as follows: [9]
- It has been pointed out that more than 200 types of HPV exist. [12]
- It has also been iterated that common and plantar warts are caused by: usually HPV 1, 2, 4 and 7. [12]
- Plane warts are stated to be caused by: HPV 3, 10, 27 and 41
- Genital warts are stated to be caused by: 90% are caused by HPV 6 and 11. [11]
Clinical manifestations
The clinical features of wart had been summated as follows: [9]
- Common warts are stated to manifest with: hyperkeratotic flesh-coloured papules with pinpoint black dots (thrombosed capillaries). [12]
- Palmar / plantar warts are stated to manifest as: thick, deep endophytic papules with black dots. [12]
- Myrmecia: painful plantar wart with anthill appearance
- Mosaic: coalescence of several warts on plantar surfaces. [12]
- Flat / plane warts are stated to manifest with: light pink-brown, flat-topped papules. [12]
- Genital warts are stated to manifest with: smooth, sessile, raised, skin coloured to brown lobulated papules. [11]
- Genetic syndromes associated with warts had been summated as follows:
- Epidermodysplasia verruciformis: increased susceptibility to genus β HPV types
- Generalized polymorphic papules (flat wart-like appearance on the dorsal hands, neck, face and extremities)
- Scaly, pink macules, hypopigmented, guttate macules / patches and seborrheic keratosis-like lesions on forehead, neck, trunk. [16]
- WHIM syndrome: This syndrome is stated to be a rare primary immunodeficiency disorder which is characterized by warts, hypogammaglobinemia, infections and myelokathexis. [17]
- WILD syndrome: This syndrome is stated to entail an association between warts, immunodeficiency, lymphedema and dysplasia (anogenital). [17]
- Epidermodysplasia verruciformis: increased susceptibility to genus β HPV types
Diagnosis
The diagnosis of wart had been summated as follows: [9]
- The diagnosis of wart is stated to be usually undertaken or established as a clinical diagnosis
- It has been iterated that pathology examination of biopsy specimen of the lesion can confirm the clinical diagnosis of wart as well as rule out other entities. [12]
Factors of prognostication
The prognostic factors of wart had been summated as follows: [9]
- Majority of wart infections clear within 2 years. [11]
- Young age and non-Caucasian skin type are stated to enhance the resolution of warts. [13]
- Smoking, alcohol consumption, increased number of sexual partners and risky sexual behaviour are stated to increase the oncogenic risk of warts. [18]
Treatment
Treatment options of warts had been summated as follows: [9]
- Destructive therapies of warts had been documented to include the ensuing. salicylic acid, trichloroacetic acid, cryotherapy, silver nitrate, phenol, cantharidin, surgical interventions and lasers. [19]
- Antiproliferative agents include the ensuing: bleomycin, vitamin D analogs, podophyllin, podophyllotoxin and 5-fluro uracil. [19]
- Antiviral agents for the treatment of warts include the ensuing: cidofovir and retinoids [19]
- Immunotherapy for recalcitrant, recurrent or extensive warts had been stated to include the following: imiquimod, BCG vaccine, MMR vaccine, Candida antigen, vitamin D3 [19]
Gross description
Macroscopy pathology examination features of a wart had been summated as follows: [9]
- Flesh coloured or brown papules or plaques with rough surface tend to be seen upon gross examination of a wart specimen.
- Single or multiple warts tend to be seen.
Microscopic (histologic) description
Microscopy pathology examination of specimens of specimens of wart had been summated to demonstrate the ensuing: [9]
- Common warts (verruca vulgaris) [20]
- Hyperkeratosis, papillomatosis, hypergranulosis
- Columns of parakeratosis, especially over projecting dermal papillae
- Intracorneal haemorrhage
- Vacuolated superficial keratinocytes with pyknotic raisin-like nuclei (koilocytes)
- Koilocytes may not be seen in older lesions
- Koilocytes are not needed for the diagnosis
- Inward bending of rete ridges at borders of lesion (toeing in)
- Dilated capillaries in dermal papillae
- Projects above the plane of the epidermis
- Palmar / plantar warts (verruca palmaris and verruca plantaris). [20]:
- Similar to verruca vulgaris (clinical distinction based on location)
- Endophytic growth - greater proportion of the lesion lies beneath the plane of the epidermis
- Myrmecia warts: [21]
- Marked acanthosis
- Large eosinophilic intracytoplasmic inclusion bodies
- Plane warts (verrucae planae) [20]:
- Acanthosis and hyperkeratosis
- No papillomatosis or parakeratosis
- Vacuolization of the cells of the upper stratum spinosum and stratum granulosum with margination of keratohyalin granules
- Often have dyskeratotic keratinocytes
- Condyloma acuminatum (venereal / genital warts): [22]
- More massive acanthosis with bulbous rete ridges (condyloma means fist or knuckle)
- Koilocytes in the upper spinous layer
- Parakeratosis often in the valleys of the epithelium (crypt parakeratosis)
- Epidermodysplasia verruciformis [20]:
- Hyperkeratosis and hypergranulosis
- Acanthosis with small nests of large cells with pale blue-gray cytoplasm, clear nuclei and perinuclear halos
- May evolve to squamous cell carcinoma
Immunohistochemistry staining studies:
Immunohistochemistry staining studies of wart had been summated as follows: [9]
Positive stains
- IHC is stated to be not typically required for the diagnosis of a wart.
- Sporadic and focal staining with p16 stated to be seen in condyloma acuminatum [23]
Electron microscopy description
In cases of warts, it has been stated that electron microscopy examination of the lesion demonstrates the ensuing:
- Intracytoplasmic electron dense inclusions. [24]
Molecular / cytogenetics description
Molecular / cytogenetics study features of wart had been stated to demonstrate the following: [9]
- HPV: in situ hybridization tend to be found during molecular and cytogenetics studies.
Differential diagnoses
The differential diagnoses of wart had been summated to include the following: [9]
- Verruca vulgaris:
- Seborrheic Keratosis: This lesion is iterated to depict the ensuing features upon pathology examination.
- Variable combinations of hyperkeratosis, papillomatosis, acanthosis
- Horn pseudocysts
- No hypergranulosis, koilocytes or tiers of parakeratosis
- Seborrheic Keratosis: This lesion is iterated to depict the ensuing features upon pathology examination.
- Epidermal nevus: This lesion is iterated to depict the ensuing features upon pathology examination:
- Hyperkeratosis, papillomatosis, acanthosis
- No koilocytes or tiers of parakeratosis
- Acrochordon: This lesion is iterated to depict the ensuing features upon pathology examination.
- Pedunculated papule, epidermis often extends almost completely around a fibrovascular core
- Papillomatosis and acanthosis
- No koilocytes or tiers of parakeratosis
- Acanthosis nigricans: This lesion is iterated to depict the ensuing features upon pathology examination.
- Lesser degree of hyperkeratosis and papillomatosis tend to be visualised upon microscopy examination of the specimen.
- Acanthosis minimal or absent,
- Basal layer hyperpigmentation
- No koilocytes or tiers of parakeratosis
- Myrmecia:
- Molluscum contagiosum: This lesion is iterated to depict the ensuing features upon pathology examination:
- Crater filled with eosinophilic to basophilic intracytoplasmic inclusions (Henderson-Patterson bodies) that push the nucleus and numerous keratohyaline granules aside
- Molluscum contagiosum: This lesion is iterated to depict the ensuing features upon pathology examination:
- Condyloma acuminata:
- Bowenoid papulosis: This lesion is iterated to depict the ensuing features upon pathology examination.
- Atypical keratinocytes throughout the full thickness of the epidermis with several mitoses in metaphase
- Verrucous carcinoma: This lesion is iterated to depict the ensuing features upon pathology examination.
- Well differentiated SCC with pushing invasive border
- More mitoses and mild cytologic atypia
- Condyloma lata: This lesion is iterated to depict the ensuing features upon pathology examination:
- Condyloma lata are stated to be more-moist, in comparison with condylomata acuminata and may be ulcerated.
- Acanthosis with neutrophils in the epidermis
- Perivascular plasma cell infiltrate
- Spirochetes on dark field examination (and IHC) and reactive syphilis serology
- Bowenoid papulosis: This lesion is iterated to depict the ensuing features upon pathology examination.
[B] Miscellaneous Narrations and discussions form some case reports. Case series, and studies related to warts.
Cho et al. [18] made the ensuing iterations:
- At the moment condyloma acuminata afflicts about 1% of sexually active adults, and its incidence has been on the increase.
- The coexistence of genital warts (GW) and some cancers and an association between human papillomavirus (HPV) and many malignant tumours had been reported in the literature. In view of this they had undertaken a large national study to analyse the risk of malignancies among men and women with GW in Taiwan.
Cho et al. [18] reported that between January 2000 and December 2013, about 3 million individuals were reported to the National Health Insurance Research Database of Taiwan. Out of these reported individuals, 21,763 were diagnosed with GW. During the same time period, a total of 213,541 cancer cases were reported to the registry, of which 1002 were recorded among patients who had GW. The age-specific incidence rates of GW and standardized incidence ratios (SIRs) of malignancies in comparison with the general population were calculated. Women were found to have acquired GW earlier than men, with a mean age at diagnosis of 32.63±12.78 years. The highest incidence rate for both genders had peaked at between 20 years and 29 years. Out of the 1002 patients who had GW and malignancies, the SIR was 1.95 (95%CI 1.83-2.07). The most markedly increased risk was found for HPV-related cancers, with a SIR of 9.74 (95%CI 3.70-15.77). Significantly elevated risks were also observed for smoking-related cancers, anogenital cancers, cervix in situ, colon, rectum, lung, kidney, and prostate cancers. Majority of cancers had developed within 10 years pursuant to the diagnosis of GW. Cho et al. [18] made the ensuing conclusions:
- Patients who are afflicted by GW do have an increased risk of HPV-related cancers, especially anogenital malignancies in Taiwan.
- The higher risk of other cancers has highlighted differences in exposure and risk factors among patients with GW compared to the general population.
- Cancer screening and HPV vaccination programs should be emphasized for at-risk individuals.
Thappa and Chiramel. [19] made the ensuing educative iterations:
- Cutaneous and genital warts are common dermatological conditions which are caused by the human papilloma virus (HPV).
- Even though it is a benign condition, it does tend to cause disfigurement, has a tendency to koebnerize, and could be transmitted to other individuals. This makes adequate and timely therapy very important.
- There are many conventional treatment options available with variable response.
- Topical and systemic immunotherapy has now found a significant place in the treatment of warts due to its non-destructive action, ease of utilisation, and promising results.
- Some of the various immunotherapeutic agents used for the treatment of warts include: more established agents such as imiquimod, Mycobacterium w vaccine, bacillus Calmette-Guérin vaccine, measles, mumps, and rubella vaccine, Candida antigen, trichophyton antigen, tuberculin, zinc, cimetidine, levamisole, HPV vaccine, and autoimplantation therapy. Other agents such as contact immunotherapy which is sparsely used now than before and newer agents such as Corynebacterium parvum, sinecatechins, echinacea, propolis, glycyrrizinic acid, and Vitamin D have also been discussed.
Cui et al. [25] made the ensuing iterations:
- The giant condyloma acuminatum (GCA), which is also referred to as Buschke–Löwenstein tumor (BLT), is a type of human papilloma virus‐associated sexually transmitted infection.
- Therapeutic options for condyloma acuminatum do remain controversial; however, surgery does seem to be the best option of treatment.
- The management of GCA during pregnancy tends to be more complicated since one has to assess the condition of both the mother and the fetus.
- They had reported a GCA case in a pregnant woman who had giant masses which had covered her perineal and perianal region.
- Considering her gestational age and the fetal neurological risk from the anticipated lengthy procedure of mass removal surgery for tumor of this size, they had decided to undertake resection of the tumor, 2 weeks pursuant to the delivery of infant via C‐section.
- The giant condyloma acuminatum (GCA), which is also referred to as Buschke–Löwenstein tumour (BLT), a type of sexually transmitted infection, was first described by Abraham Buschke and Ludwig Löwenstein back in 1925. [26]
- GCA is known to be associated with human papilloma virus (HPV) infection, especially types 6 and 11. [27-28]
- Infection risks for GCA are stated to be raised with poor hygiene, local irritation, immunosuppression, HIV infection, multiple sexual partners, and anal intercourse. [29]
- The most frequently afflicted areas are perineum, vulva, vagina, perianal region, and rectum. [30]
- HPV infection during pregnancy had been reported to increase complications during delivery and affect newborns.
- An emerging body of evidence had indicated that vertical transmission of HPV from mother to infant could occur while the infant passes through the infected birth canal or in the case of prematurely ruptured membrane. [31-32]
- It has been iterated that as considerations should be given to the appropriate mode of delivery, more patients might require C‐sections. [33]
- HPV infection should be screened and managed more actively in pregnant women.
- GCA entails the development and slow progression of exophytic, ulcerative, and cauliflower‐shaped tumours of significant dimensions which typically infiltrate and invade local tissue without spontaneous resolution.
- Even though the lesions do not emanate in the development of distant metastases, their locally aggressive behaviour and a relatively high local recurrence do complicate the cure process and require more active management. [34]
- In a study with 51 cases, men were found to more likely get infected in comparison with women (2.7:1), [35] and GCA is an uncommon clinical type of genital wart in the pregnant population, with less than five cases reported at the time of publication of their article.
Cui et al. [25] reported a 17‐year‐old Chinese female, who had manifested with pain within her perineal and perianal area and positional abnormality during the 34th week of her gestation. A cord‐like tumour that measured about 1 cm × 1 cm in size was found within her perianal region in week 14 of her gestation in a private clinic of the remote area where she lived. The patient refused to undergo treatment despite explanation of the prognosis by the local doctors back then and she administered some topical traditional Chinese medicine herself. Nevertheless, the patient recounted that the mass had kept growing rapidly. Unfortunately, the details of that care encounter were not available to Cui et al. [25]. Since she had noticed her genital lesion, her husband had manifested with the same type of neoplasm many times, and he cut the cauliflower‐like growth upon his penis by himself at home without any further physician visits or follow‐up. When she presented to Cui et al. [25] during week 34 of her gestation with perineal pain, she was not able to stand upright as a result of compression from the two large masses. During her clinical examination, large, irregular, ulcerative, and verrucous vegetations were identified, that had covered both her perineal and perianal region with malodorous discharge upon the surface (see figure 1). The anterior vegetation had measured 5 cm × 3.8 cm and the posterior one had measured 13 cm × 6 cm. Cui et al. [25] presented the case to the board of multidisciplinary teamwork to discuss the plans for her delivery and the proper sequence of the two procedures, namely the mass removal and the infant delivery. Given the fact that the giant vegetation had occupied her vaginal birth canal and that prolonged general anaesthesia might increase the neurological risk to the infant, Cui et al. [25] decided to undertake a C‐section before the neoplasm resection. Risks and benefits of infant delivery and resection procedure were discussed with the patient. The infant was delivered successfully by means of C‐section at full term. Two weeks subsequently, her perineal and perianal giant tumours were excised en bloc at the pedicles by electric scalpel until healthy tissue was reached in gynaecological position under general anaesthesia. In view of the fact that the resection did not leave large wound or tissue defect, reconstruction was not indicated for this patient (see figure 2).

Figure 1: The two large, irregular, ulcerative growths found covering the perineal and perianal area with malodorous discharge on the surface. The anterior one measured 5 cm × 3.8 cm and the posterior one 13 cm × 6 cm. Reproduced from: [25] under the Creative Commons Attribution License.
The resected masses were sent to the pathology department for staining and sectioning of paraffin‐embedded tissue. The pathology examination demonstrated squamous mucosa with dysplasia and viral cytopathic effect, consistent with koilocytosis in HPV infection (see figure 3). Cytological study on the cervical specimen demonstrated HPV‐11 positivity, one of the two serotypes associated with GCA from the literature. [27-28]

Figure 2: The surgical wound after lesion resection and skin closure. Reproduced from: [25] under the Creative Commons Attribution License.
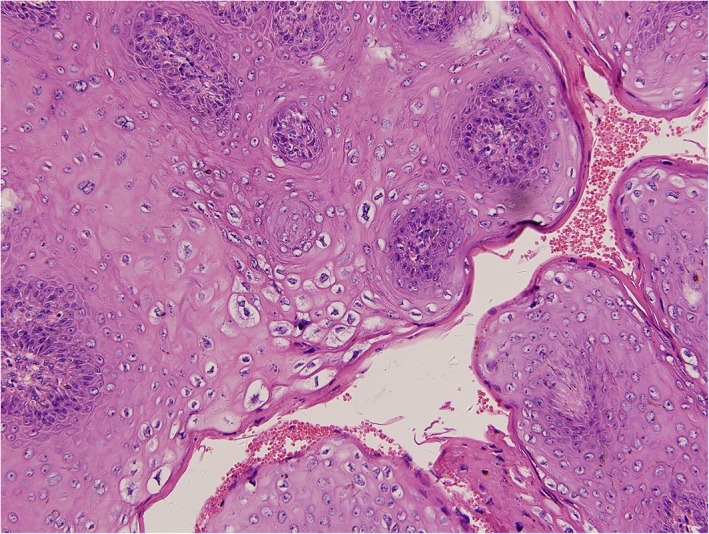
Figure 3: Squamous mucosa with dysplasia and viral cytopathic effect from pathology study of the surgical specimen, consistent with koilocytosis of HPV infection (hematoxylin and eosin staining, ×200). Reproduced from: [25] under the Creative Commons Attribution License.
Pursuant to the procedure, the patient was informed of possible recurrence, which is common and was presumably related to the infection in the encompassing healthy tissue. Her husband received treatment as well and it was decided he should be followed up in the local health organization.
Cui et al. [25] made the ensuing educative discussions:
- The treatment for condyloma acuminata has remained to be controversial; nevertheless, surgery has constituted the best option of treatment.
- Extended surgical excision or radical local excision with reconstruction of skin had represented the primary treatment described. [36] and minimally invasive surgery had been favoured as a first‐line treatment. [34]
- Alternative treatment options reported include CO2 laser, electrocoagulation, radiotherapy, intralesional injection of INF‐alpha, or topical imiquimod. [37-39]
- Cryotherapy (liquid nitrogen, nitric oxide) associated with topic chemotherapy has been proved effective in patients with small‐sized tumours. Carbon dioxide, argon fluoride, and laser therapy have produced satisfactory results in recurrence treatment.
- For their reported case, the giant tumours were excised en bloc by electric scalpel at the pedicles.
- The treatment of GCA during pregnancy is more complicated since clinicians have to assess both the mother and the foetus.
- Vaginal delivery was not an option for their reported case in view of the fact that the mass had filled up the natural birth canal and increased the risk of vertical transmission of human papillomavirus to the infant as it passes through the infected vagina. [33,40]
- As it was 34 weeks into her pregnancy, considerations were given to the appropriate sequence of intervention.
- The excision of the two giant growths under general anaesthesia is a major operation which is associated with a high risk of intraoperative maternal bleeding.
- Non-obstetric surgeries had been demonstrated with risks of spontaneous abortion, intrapartum haemorrhage, premature delivery, low birth weight, etc. [41-43]
- In view of this, it had been generally recommended to postpone elective surgery until pursuant to delivery. [44]
- Also, the lengthy procedure of GCA resection meant an extended period of anaesthesia of the mother, which might delay neurological development and might impair brain function of the foetus.
- According to a recent alert from the US FDA, foetal exposure to anaesthetics within the third trimester of pregnancy amid prolonged surgery might compromise brain development and function, while the association between such exposure within the limited duration, such as epidural anaesthesia during C‐section, and learning disabilities had not been established. [45]
- Based upon the evidence and the fear of development of severe and even life‐threatening complications to the patient and the foetus, they had decided to deliver the child around the due date through C‐section before they would plan and schedule the GCA resection procedure per the patient's condition, such as her coagulability and the lesion size.
- GCA is iterated to feature tendency toward the development of local recurrence and conversion into squamous cell carcinoma. [46-47]
- The risk for the development of recurrence in the anorectal and perianal regions pursuant to excision is between 60 percent and 66 percent, with an overall mortality of 20 percent and 30 percent.
- The development of malignancy had been reported in between 30 percent and 56 percent of cases. [48]
- In their reported case, squamous mucosa with dysplasia and the viral cytopathic effect were noticed, which were signs of expectable spontaneous regression.
- Recurrence ensuing an incomplete excision or reinfection to the encompassing tissue remained could be frequent and follow‐up visits for signs of recurrence would be necessary.
Jha [49] stated the ensuing:
- Anogenital warts (AGWs) are caused by human papilloma virus (HPV) and are transmitted by sexual route.
- The available options for the treatment of AGWs tend to be cumbersome, require multiple sittings and are associated with recurrence.
Jha [49] reported a case of a male with condyloma acuminata who was treated successfully utilising injection vitamin D3. No recurrence was observed in a follow-up period of 6 months.
Achdiat et al. [50] made the ensuing iterations:
- Anogenital Warts (AGWs) are benign proliferations which are caused by Human Papillomavirus (HPV) infection upon the genital or anal areas.
- Various treatment options are available for the therapy of AGWs but there is no best or ideal therapy, and the recurrence of AGWs is significantly high.
- A promising new therapy which was being evaluated at the time of publication of their article is immunotherapy with the intralesional Bacillus Calmette-Guérin (BCG) vaccine.
Achdiat et al. [50] reported two cases of a 23-year-old woman and a 41-year-old man, who had manifested condyloma acuminata type AGWs. The patients were immunocompetent and had received single dose intralesional BCG vaccine on the largest lesion. Clinical improvements of AGWs lesions were identified commencing on the 14th day after receiving therapy by the disappearance of some lesions with no recurrence and side effects. Achdiat et al. [50] made the ensuing discussions:
- Intralesional BCG vaccine does activate the immune system, treats other AGWs lesions which do not receive an intralesional injection, and also prevents recurrence.
- Even though the intralesional BCG vaccine is effective for treating AGWs, further evaluation is still required to assess for its recurrence.
Kirchhof and Wong [51] stated that the prevalence of tattoos is increasing and as such every physician should be aware of the potential adverse events that are associated with tattooing. Kirchhof and Wong [51] reported a 36-year-old man who had a recent history of skin-coloured papules appearing suddenly in a 20-year-old tattoo upon his right forearm. Histopathology examination of biopsy specimen of his lesion confirmed a diagnosis of verrucae planae or flat warts. Kirchhof and Wong [51] stated the following:
- Tattoo-associated human papilloma virus infections do develop clinical presentations following long latency periods and are often difficult to treat.
- The risk of developing tattoo-related human papilloma virus infection should be discussed when considering acquiring a tattoo.
Ural et al. [52] made the ensuing iterations:
- Verruca vulgaris (common warts) is a benign lesion of skin and mucous membranes that is caused by human papillomovirus (HPV).
- The lesions are typically self-limited; however, they may vary with regard to size and number.
- The occurrence upon the tongue is very rare.
- To the best of their knowledge, only one verruca vulgaris existing in the tongue had been reported in the literature by the time of publication of their case in 2014.
Ural et al. [52] reported a rare case of verruca vulgaris of the tongue which had afflicted a 36-year-old Caucasian man.
Mattoo and Bhatia [53] stated the ensuing:
- Oral verruca vulgaris is caused by human papillomavirus (HPV) infection.
- Verruca vulgaris most frequently afflicts the fingers, toes, soles, and dorsal surfaces of hands and is mostly asymptomatic.
- Varieties of verrucous and papillary lesions afflict the skin as well as oral mucosa which could be either benign or reactive.
- Common wart is one of the most commonly encountered skin growths and a lesion of childhood.
- Intra-oral warts could occur at any age with equal incidence in both genders but they are most commonly encountered within the third to fifth decade of life.
- It is found commonly upon the palate followed by lip, tongue, buccal mucosa, and rarely seen on gingiva.
- Surgical excision with adequate margins is the treatment of choice.
Zayko et al. [54] stated the following:
- A condyloma acuminatum is a sexually transmitted, human papillomavirus (HPV) associated, neoplasm.
- In men, it is predominantly found upon the external genitalia and rarely progresses more proximally than the distal penile urethra.
- Condyloma acuminata of the prostatic urethra are uncommon and are usually visualised as an extension of, or in association with external lesions. In view of this, it is not typically considered in the differential diagnosis of isolated papillary lesions limited to the prostatic urethra.
Zayko et al. [54] reported a 62-year-old male with rheumatoid arthritis who was treated with abatacept and who had manifested with a history of intermittent bladder self-catheterization for urinary obstruction. He underwent a transurethral resection of the prostate gland and had incidental findings of papillary lesions which were restricted to his prostatic urethra which were presumed to be urothelial carcinoma. Microscopy pathology examination of the specimen established the diagnosis of condyloma acuminata, and low-risk HPV 6 and 11 were detected by in-situ hybridization. He subsequently underwent cystoscopy which demonstrated marked growth and extension of condyloma acuminata to near his external urethral meatus. After multiple treatments with intraurethral 5-fluorouracil, several small lesions had remained within his bulbous urethra. With follow up for 2 years since diagnosis, the patient had not developed external condylomata. Zayko et al. [54] made the ensuing conclusions:
- A condyloma acuminatum might manifest as an isolated papillary growth in the prostatic urethra without clinical or historical evidence of a visible lesion on external genitalia.
- Immunosuppression and/or urethral instrumentation might be a risk factor for such a manifestation.
- Urologists and pathologists need to be aware of this rare possibility in order to avoid misdiagnosis, and ensure that the patient receives appropriate treatment.
Sen et al. [55] stated the ensuing:
- Condyloma acuminatum (CA) is a human papillomavirus-induced sexually transmitted disease which is typified by epithelial proliferation within the genital region, perianal region, oral cavity and larynx.
- It was first reported by Knapp and Uohara in 1967. [56]
- The disease is more commonly encountered in children and teenagers and does tend to appear as solitary or multiple, pinkish, sessile papules or plaques with pebbled surface or as pedunculated papillary lesions.
- Oral lesions commonly afflict the lips, floor of the mouth, lateral and ventral surfaces of tongue, buccal mucosa, soft palate and rarely gingiva.
Sen et al. [55] reported a case of CA affecting a 75-year-old man patient with emphasis upon its clinical presentation, histological features and importance of PCR for establishment of definitive diagnosis. Sen et al. [55] stated that their reported case was unique because CA is very rare in the geriatric age group.
Shruti et al. [57] made the ensuing iterations:
- Epidermodyplasia verruciformis (EV) is a rare heritable disease which is typified by an increased susceptibility to infection with specific human papillomavirus (HPV) types due to a defect in cell-mediated immune response to HPV infection.
- Widespread infection with HPV is responsible for the development of wart-like lesions and pityriasis versicolor-like spots.
- These individuals do have a lifelong risk for the development of cutaneous malignancies, especially Bowen's disease and squamous cell carcinoma, mainly in sun-exposed parts.
- Being the first disease to correlate cancer and viral infection, EV had served as the cornerstone of the understanding of viral oncogenesis.
Shruti et al. [57] reported three cases of EV, of which one patient had subsequently developed Bowen's disease. The patients had multiple hypopigmented papules and plaques of various sizes which had started erupting in childhood and which were mainly distributed over sun-exposed parts of their body. Histopathology of the skin biopsies was reported to be consistent with EV. One of these patients had started developing an ulcerated plaque upon the left clavicle 2 years earlier. A biopsy from the clavicular region also demonstrated histopathology examination features of Bowen's disease arising in EV.
Ingordo et al. [58] made the ensuing iterations:
- Warty Dyskeratoma (WD) is an uncommon condition consisting in single or multiple papular or nodular lesions of the skin or of the oral mucosamucosa.
- Histologically, a cup-shaped epidermal invagination centred by a plug of epidermal hyperparakeratosis with supra-basal acantholysis and dyskeratosis is typically found on pathology examination of the lesions.
- They had reported a case of post-inflammatory WD, which was also observed by dermoscopy. Dermoscopy had demonstrated an eight-shape whitish collarette encompassed by light brown pigmentation. A central white structureless area with an adjacent rosette were visualized. Some small rust-coloured blood crusts were also seen within the centre of the lesion; no prominent vascular pattern was identified. They also stated the following:
- Aetiopathogenesis of this benign neoplasm could be multifactorial.
- Dermoscopy of WD is not specific but may help to exclude other skin tumors.
Ingordo et al. [58] made the ensuing iterations:
- Following the seminal description by Helwig in 1954 as “isolated Darier’s disease”, [59] Warty Dyskeratoma (WD) had been described as a distinctive clinic-pathological entity by Szymanski in 1957. [60]
- Shortly after, Graham and Helwig [61] had proposed the name “isolated dyskeratosis follicularis”, because their cases had exhibited a pattern of dyskeratosis and acantholysis similar to that described in Darier’s disease.
- Ackerman [62] had suggested that WD should be included within the spectrum of dermatoses with Focal Acantholytic Dyskeratosis (FAD): he postulated that the terminology WD should be restricted to lesions that clinically present as a single nodule, whereas papular lesions should be best labelled as “papular form of FAD”.
- Up to the time of publication of their article; however, the terminology WD had been commonly used for both papular and nodular lesions. [63-64]
Ingordo et al. [58] reported a small erythemato-papular lesion which was superficially eroded and which had afflicted the hairy region of the chest in a 53-year-old Caucasian man. He was on the whole in good health; he was affected by a mild hypertension which was under control with an ACE-inhibitor medication. No other skin lesions were found during his assessment. He did not have any history of Darier’s disease. After undergoing a one-week topical corticosteroid-antibiotic therapy, the lesion appeared as a skin-coloured and umbilicated papule with a central keratotic plug (see figure 4A). Dermoscopy was undertaken with Molemax II, Derma Medical Systems, Vienna, Austria, which demonstrated an eight-shape whitish collarette encompassed by light brown pigmentation. A central white structureless area with an adjacent rosette were identified. Some small rust-coloured blood crusts were also visualised within the centre of the lesion; no prominent vascular pattern was identified (see figure 4B). Histopathology examination of the lesion demonstrated a cup-shaped epidermal invagination (see figure 4C) that was filled with a hyperkeratotic and parakeratotic plug, containing numerous grains and corps ronds (see figure 4D). The base of the invagination consisted of hyperplastic epithelium with digitate projections (villi). Based upon these microscopy pathology examination features of the lesion, a diagnosis of WD was made.
Ingordo et al. [58] made the ensuing educative discussions:
- Cutaneous WD is stated to be an uncommon condition; [63-64]
- It appears in middle-aged individuals as a cutaneous elevated nodule or cyst with a raised border and a somewhat umbilicated or pore-like centre.
- Majority of the lesions tend to be brown, but some had tended to be described as skin-coloured, yellow, red, black, tan, or grey. [61,63-64]
- Usually a single lesion is visualised, [62,63-64] but cases with multiple lesions had been reported [65-67]
- Head and neck are stated to be mainly afflicted. [62-64]
- Trunk and limbs are reported in a minority of patients; [62-64] a few cases of vulvar [68] and oral [69] WD had been described.
- Patients who are afflicted by cutaneous WD are usually middle-aged. [62-64]
- In some case series the male sex was reported to be prevalent, [62,64,70] in another series women were documented to be more affected than men, [64] but according to other authors both sexes were reported in the same proportion. [63]
- Mucosal WD does seem instead to be more prevalent in middle-aged males. [69]
- Kaddu et al. [64] had described three architectural patterns of cutaneous WD, including: cup-shaped, cystic, and nodular. They had postulated that nodular lesions might represent an early stage in the occurrence of WD, whereas cystic and cup-shaped lesions are relatively well-developed lesions.
- Majority of authors are of the opinion that cutaneous WD is derived from the hair follicle in view of its closeness or clear-cut connection to pilosebaceous unit, [61,63] [64,66,70] thereby suggesting that “follicular dyskeratoma” could be a better terminology for this entity. [64]
- A study which was undertaken with human keratin antibodies, specific for cortex and inner root sheet of normal human hair, [65] and a survey undertaken searching the expression of cytokeratins CK1, CK5, Ck10, CK17, CK19 [63] had confirmed this postulate.
- WD which arise in regions that are devoid of follicular structures (oral mucosa [69] and nail bed [71,72] might represent examples of isolated FAD secondary to a local inflammation or a neoplastic proliferation. [63-64,66,69] In view of this, Allon et al. had indicated that for oral lesions the terminology “isolated FAD” rather WD should be used. [69]
- The aetiology of cutaneous WD is not known.
- Ultraviolet light, autoimmunity, viral infections, and chemical carcinogens had been postulated to play a role. [60-61,64,66,70,73]
- Szymanski [60] had demonstrated the presence of viral DNA and RNA within the epithelial cells lining the villi, but Kaddu et al. [64] had failed to find HPV-DNA in wide number of HPV in their case series.
- It has been iterated that in oral WD, smoking did seem to play the main aetiologic role. In this instance, ill-fitting dentures, alcohol use, check biting, sniff use, extraction site, and immunosuppression were also suggested to be aetiologic factors. [69]
- It was postulated that WD represents a sporadic localized error in epithelial maturation and cohesiveness. [74] In this regard it is of interest to emphasize that Ackerman classified solitary FAD in three forms: i) a clinically nonapparent type (histologically incidental lesions); ii) a papular type (focal acantholytic dyskeratoma) and iii) a nodular type (warty dyskeratoma). [62]
- “Incidental FAD” had also been identified within many skin lesions (i.e. epithelial lesions, fibrohistiocytic lesions, inflammatory conditions, melanocytic neoplasms as well as miscellaneous lesions).
- The pathological changes had either occurred within the lesion or in the “clinically normal-appearing” epithelium immediately adjacent to the lesion. [73]
- Accordingly, as was postulated by Griffiths et al., [65] the development of WD at various anatomical sites could be multifactorial. This postulate is in agreement with the post-inflammatory onset of their reported case.
- It had been iterated that the clinical differential diagnoses of cutaneous and mucosal WD includes the ensuing: basal cell carcinoma, epidermal cyst, seborrheic keratosis, actinic keratosis, squamous cell carcinoma, melanocytic nevus, keratoacanthoma, common wart, condyloma acuminatum, bowenoid papulosis, sebaceous hyperplasia, adnexal tumour, oral papilloma or fibroma. [64,68,75]
- Histopathology examination differential diagnoses must be made with Darier’s disease, Grover’s disease, acantholytic squamous cell carcinoma, keratoacanthoma, pemphigus vulgaris, Hailey-Hailey disease, syringocystoadenoma papilliferum. [61] [64] [70] [75] Noteworthy, the presence of histopathology examination clear surgical margins virtually excludes the inflammatory dermatoses listed above. [61,64]
- Dermoscopy of WD had been undertaken in a limited number of cases (Appendix). [74-78]
- Papules of acantholytic dyskeratotic acanthoma, acantholytic dyskeratoses, and Grover’s disease do demonstrate a central yellowish to brown star-like pattern overlying a pinkish homogeneous structure-less area. [74]
- Syringocystoadenoma papilliferum demonstrates a polymorphous vascular pattern on a pinkish-white background. [77]
- Papules of Darier’s disease demonstrate a centrally located yellowish/brownish area surrounded by a thin whitish halo. [75]
- Dermoscopy of keratoacanthoma and squamous cell carcinoma is typified by keratin masses, white structures (white circles, white clods, and white structureless areas), and hairpin vessels. [75,78]
- In viral wart, the most frequent dermoscopy findings are the mosaic pattern and the exophytic keratotic projection pattern (dotted, linear, or hairpin vessels, often encompassed by a whitish halo), often with micro-haemorrhages. [78]
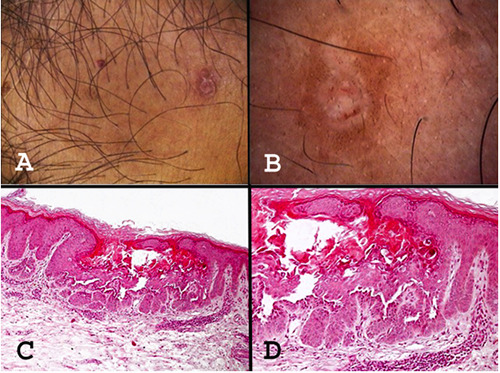
Figure 4: A) Clinical picture featuring a skin-coloured, umbilicated nodule with a central keratotic plug. B) Dermoscopy of WD, typified by an eight-shape whitish collarette surrounded by light brown pigmentation; a central white structureless area with an adjacent rosette; some small rust-coloured blood crusts at the centre of the lesion. C) Histopathologic picture disclosing a cup-shaped epidermal invagination filled with keratinous hyper-parakeratotic plug. D) A closer histologic view with numerous grains and corps ronds. Reproduced from: [58] under the Creative Commons Attribution License.
Ingordo et al. [58] made the ensuing conclusions:
- WD is a rare condition and its development might be multifactorial, including also a post-inflammatory pathogenesis.
- According to patterns that had been reported in Appendix, the dermoscopy features of WD are not specific; [78] nevertheless, dermoscopy might help exclude the above-mentioned conditions, thereby making WD a clinical diagnosis which could be established by exclusion.
Conclusion
- Wart is an uncommon condition which consists of single or multiple papular or nodular lesions upon the skin or on the oral mucosa.
- The development of warts could be multifactorial, including also a post-inflammatory pathogenesis.
- The dermoscopic features of warts are not specific; nevertheless, dermoscopy might exclude the differential diagnosis and warts is generally diagnosed by exclusion.
- Diagnosis of warts can be confirmed based upon pathology examination of biopsy specimens or excised specimens of the lesion.
Conflict of Interest - Nil
Acknowledgements
Acknowledgements to:
- Dermatologic Therapy and Wiley Periodicals Inc. for granting permission for reproduction of contents and figures of their journal article under Copyright: Copyright 2019 The Authors. Dermatologic Therapy published by Wiley Periodicals, Inc. This is an open access article under the terms of the http://creativecommons.org/licenses/by/4.0/ License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
- Dermatology Reports for granting permission for reproduction of contents and figures of their journal article under Copyright: Copyright © the Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
- Cohen PR, Hebert AA, Adler-Storthz K (1993). Focal epithelial hyperplasia: Heck disease. Pediatr Dermatol. 1993 Sep. 10(3):245-51.
View at Publisher | View at Google Scholar - Shenfelt P D, Talavera F, James W D, Zelchner J A (2020). Nongenital Warts. Medscape. 2020 September 25.
View at Publisher | View at Google Scholar - Luria L, Cardoza-Favarato G (2023). Human Papillomavirus. StatPearls [Internet]. Updated 2023 Jan. 16.
View at Publisher | View at Google Scholar - Mallory SB, Baugh LS, Parker RK (1991). Warts in blacks versus whites. Pediatr Dermatol. 1991 Mar. 8(1):91.
View at Publisher | View at Google Scholar - Silverberg NB. Human papillomavirus infections in children (2004). Curr Opin Pediatr. 2004 Aug. 16(4):402-9.
View at Publisher | View at Google Scholar - Guadara J, Sergi A, Labruna V, Welch M, Gazivoda PL (1992). Transformation of plantar verruca into squamous cell carcinoma. J Foot Surg. 1992 Nov-Dec. 31(6):611-4.
View at Publisher | View at Google Scholar - Kolker AR, Wolfort FG, Upton J, Tahan SR, Hein KD, et.al (1998). Plantar verrucous carcinoma following transmetatarsal amputation and renal transplantation. Ann Plast Surg. 1998 May. 40(5):515-9.
View at Publisher | View at Google Scholar - Noel JC, Detremmerie O, Peny MO, et al (1994). Transformation of common warts into squamous cell carcinoma on sun-exposed areas in an immunosuppressed patient. Dermatology. 1994. 189(3):308-11.
View at Publisher | View at Google Scholar - Abdelkader, H, Elbendary A. Warts (verrucae) (2024). PathologyOutlines.com website.
View at Publisher | View at Google Scholar - Manini I, Montomoli E (2018). Epidemiology and prevention of Human Papillomavirus. Ann Ig. 2018 Jul-Aug;30(4 Supple 1):28-32.
View at Publisher | View at Google Scholar - Dunne EF, Park IU (2013). HPV and HPV-associated diseases. Infect Dis Clin North Am. 2013 Dec;27(4):765-78.
View at Publisher | View at Google Scholar - Abeck D, Tetsch L, Lüftl M, Biedermann T (2019). Extragenital cutaneous warts - clinical presentation, diagnosis and treatment. J Dtsch Dermatol Ges. 2019 Jun;17(6):613-634.
View at Publisher | View at Google Scholar - Bruggink SC, Eekhof JA, Egberts PF, van Blijswijk SC, Assendelft WJ, et. al (2013). Natural course of cutaneous warts among primary schoolchildren: a prospective cohort study. Ann Fam Med. 2013 Sep-Oct;11(5):437-41
View at Publisher | View at Google Scholar - Stulberg DL, Hutchinson AG (2003). Molluscum contagiosum and warts. Am Fam Physician. 2003 Mar 15;67(6):1233-40.
View at Publisher | View at Google Scholar - Kaliterna V, Barisic Z (2018). Genital human papillomavirus infections. Front Biosci (Landmark Ed). 2018 Mar 1;23(9):1587-1611.
View at Publisher | View at Google Scholar - de Jong SJ, Imahorn E, Itin P, Uitto J, Orth G, et al (2018). Epidermodysplasia Verruciformis: Inborn Errors of Immunity to Human Beta-Papillomaviruses. Front Microbiol. 2018 Jun 12;9: 1222.
View at Publisher | View at Google Scholar - Heusinkveld LE, Yim E, Yang A, Azani AB, Liu Q, (2017). Pathogenesis, diagnosis and therapeutic strategies in WHIM syndrome immunodeficiency. Expert Opin Orphan Drugs. 2017;5(10):813-825.
View at Publisher | View at Google Scholar - Cho CY, Lo YC, Hung MC, Lai CC, Chen CJ, Wu KG (2017). Risk of cancer in patients with genital warts: A nationwide, population-based cohort study in Taiwan. PLoS One. 2017 Aug 14;12(8) :e0183183.
View at Publisher | View at Google Scholar - Thappa DM, Chiramel MJ (2016). Evolving role of immunotherapy in the treatment of refractory warts. Indian Dermatol Online J. 2016 Sep-Oct;7(5):364-370.
View at Publisher | View at Google Scholar - Bacaj P, Burch D (2018). Human Papillomavirus Infection of the Skin. Arch Pathol Lab Med. 2018 Jun;142(6):700-705.
View at Publisher | View at Google Scholar - Wititsuwannakul J, Ko CJ (2012). Myrmecia wart inclusions as an incidental histopathologic finding. J Cutan Pathol. 2012 Oct;39(10):936-9.
View at Publisher | View at Google Scholar - Betz SJ (2019). HPV-Related Papillary Lesions of the Oral Mucosa: A Review. Head Neck Pathol. 2019 Mar;13(1):80-90.
View at Publisher | View at Google Scholar - Kazlouskaya V, Shustef E, Allam SH, Lal K, Elston D (2013). Expression of p16 protein in lesional and perilesional condyloma acuminata and bowenoid papulosis: clinical significance and diagnostic implications. J Am Acad Dermatol. 2013 Sep;69(3):444-9.
View at Publisher | View at Google Scholar - Rogel-Gaillard C, Pehau-Arnaudet G, Breitburd F, Orth G (1993). Cytopathic effect in human papillomavirus type 1-induced inclusion warts: in vitro analysis of the contribution of two forms of the viral E4 protein. J Invest Dermatol. 1993 Dec;101(6):843-51.
View at Publisher | View at Google Scholar - Cui T, Huang J, Lv B, Yao Q (2019). Giant condyloma acuminatum in pregnancy: A case report. Dermatol Ther. 2019 Jul;32(4):e12972.
View at Publisher | View at Google Scholar - Buschke A, Loewenstein L (1925). Über carcinomähnliche Condylomata acuminata des Penis. Klinische Wochenschrift. 1925 Sep;4(36):1726-8.
View at Publisher | View at Google Scholar - Dianzani C, Bucci M, Pierangeli A, Calvieri S, Degener AM (1998). Association of human papillomavirus type 11 with carcinoma of the penis. Urology. 1998 Jun;51(6):1046-8.
View at Publisher | View at Google Scholar - Gissmann L, deVilliers EM, zur Hausen H (1982). Analysis of human genital warts (condylomata acuminata) and other genital tumors for human papillomavirus type 6 DNA. Int J Cancer. 1982 Feb 15;29(2):143-6.
View at Publisher | View at Google Scholar - Kreuter A, Potthoff A, Brockmeyer NH, Gambichler T, Swoboda J, Stücker M, Schmitt M, Pfister H, Wieland U; German Competence Network HIV/AIDS. Anal carcinoma in human immunodeficiency virus-positive men: results of a prospective study from Germany. Br J Dermatol. 2010 Jun;162(6):1269-77.
View at Publisher | View at Google Scholar - Chu QD, Vezeridis MP, Libbey NP, Wanebo HJ (1994). Giant condyloma acuminatum (Buschke-Lowenstein tumor) of the anorectal and perianal regions. Analysis of 42 cases. Dis Colon Rectum. 1994 Sep;37(9):950-7.
View at Publisher | View at Google Scholar - Hahn HS, Kee MK, Kim HJ, Kim MY, Kang YS,et al (2013). Distribution of maternal and infant human papillomavirus: risk factors associated with vertical transmission. Eur J Obstet Gynecol Reprod Biol. 2013 Jul;169(2):202-6.
View at Publisher | View at Google Scholar - Lee SM, Park JS, Norwitz ER, Koo JN, Oh IH, et.al . Risk of vertical transmission of human papillomavirus throughout pregnancy: a prospective study. PLoS One. 2013 Jun 13;8(6):e66368.
View at Publisher | View at Google Scholar - Park H, Lee SW, Lee IH, Ryu HM, Cho AR,(2012). Rate of vertical transmission of human papillomavirus from mothers to infants: relationship between infection rate and mode of delivery. Virol J. 2012 Apr 12;9:80.
View at Publisher | View at Google Scholar - Spinu D, Rădulescu A, Bratu O, Checheriţă IA, Ranetti AE, Mischianu D; -. Giant condyloma acuminatum - Buschke-Lowenstein disease - a literature review. Chirurgia (Bucur). 2014 Jul-Aug;109(4):445-50.
View at Publisher | View at Google Scholar - Trombetta LJ, Place RJ (2001). Giant condyloma acuminatum of the anorectum: trends in epidemiology and management: report of a case and review of the literature. Dis Colon Rectum. 2001 Dec;44(12):1878-86.
View at Publisher | View at Google Scholar - Ahsaini M, Tahiri Y, Tazi MF, Elammari J, Mellas S, et.al (2013) . Verrucous carcinoma arising in an extended giant condyloma acuminatum (Buschke-Löwenstein tumor): a case report and review of the literature. J Med Case Rep. 2013 Dec 19;7:273.
View at Publisher | View at Google Scholar - Akpadjan F, Adégbidi H, Attinsounon CA, Koudoukpo C, Dégboé B, et. al (2017). A case of reccuring giant condyloma of vulva in infant without sexual abuse successfully treated with electrocoagulation in Benin. Pan Afr Med J. 2017 Jun 30; 27:159.
View at Publisher | View at Google Scholar - Calderón-Castrat X, Blanco S, Santos-Durán JC, Roncero-Riesco M (2017). Giant periurethral condyloma acuminata in a 2-year-old girl: Successful treatment with carbon dioxide laser. Actas Dermosifiliogr. 2017 May;108(4):385-387. English, Spanish.
View at Publisher | View at Google Scholar - Skowron C, Raoulx M, Skowron F (2010). Condylomes acuminés du nourrisson traités par imiquimod local [Topical imiquimod for the treatment of anogenital warts in an infant]. Ann Dermatol Venereol. 2010 Oct;137(10):622-5. French.
View at Publisher | View at Google Scholar - Chatzistamatiou K, Sotiriadis A, Agorastos T. Effect of mode of delivery on vertical human papillomavirus transmission - A meta-analysis. J Obstet Gynaecol. 2016;36(1):10-4.
View at Publisher | View at Google Scholar - Amos JD, Schorr SJ, Norman PF, Poole GV, Thomae KR, et. al(1996). Laparoscopic surgery during pregnancy. Am J Surg. 1996 Apr;171(4):435-7.
View at Publisher | View at Google Scholar - Jenkins TM, Mackey SF, Benzoni EM, Tolosa JE, Sciscione AC (2003). Non-obstetric surgery during gestation: risk factors for lower birthweight. Aust N Z J Obstet Gynaecol. 2003 Feb;43(1):27-31.
View at Publisher | View at Google Scholar - Mazze RI, Källén B (1989). Reproductive outcome after anesthesia and operation during pregnancy: a registry study of 5405 cases. Am J Obstet Gynecol. 1989 Nov;161(5):1178-85.
View at Publisher | View at Google Scholar - O'Shea M. Nonobstetric Surgery During Pregnancy. Obstet Gynecol. 2018 Dec;132(6):1506.
View at Publisher | View at Google Scholar - Olutoye OA, Baker BW, Belfort MA, Olutoye OO (2018). Food and Drug Administration warning on anesthesia and brain development: implications for obstetric and fetal surgery. Am J Obstet Gynecol. 2018 Jan;218(1):98-102.
View at Publisher | View at Google Scholar - Chao MW, Gibbs P (2005). Squamous cell carcinoma arising in a giant condyloma acuminatum (Buschke-Lowenstein tumour). Asian J Surg. 2005 Jul;28(3):238-40.
View at Publisher | View at Google Scholar - Papapanagiotou IK, Migklis K, Ioannidou G, Xesfyngi D, Kalles V, Mariolis-Sapsakos T, Terzakis E (2017). Giant condyloma acuminatum-malignant transformation. Clin Case Rep. 2017 Feb 23;5(4):537-538.
View at Publisher | View at Google Scholar - Akdag O, Yildiran G (2018). Malign Differentiation of a Large Buschke Loewenstein Tumor in Penis. Surg J (N Y). 2018 Mar 28;4(2):e53-e54.
View at Publisher | View at Google Scholar - Jha N (2021). Complete clearance of condyloma acuminata using injection Vitamin D3. Australas J Dermatol. 2021 Aug;62(3):e417-e418.
View at Publisher | View at Google Scholar - Achdiat PA, Suwarsa O, Hidayat YM, Shafiee MN, Dwiyana RF, et,al (2023). Successful treatment of anogenital warts with single dose Bacillus Calmette Guerin vaccine without prior sensitization in tuberculosis endemic country: Two case report. Hum Vaccin Immunother. 2023 Dec 31;19(1):2187591.
View at Publisher | View at Google Scholar - Kirchhof MG, Wong SM (2019). Tattoos and human papilloma virus: A case report of tattoo-associated flat warts (verrucae planae). SAGE Open Med Case Rep. 2019 Jun 19;7:2050313X19857416.
View at Publisher | View at Google Scholar - Ural A, Arslan S, Ersoz Ş, Değer B (2014). Verruca vulgaris of the tongue: a case report with a literature review. Bosn J Basic Med Sci. 2014 Aug 16;14(3):136-8.
View at Publisher | View at Google Scholar - Mattoo A, Bhatia M (2018). Verruca vulgaris of the buccal mucosa: A case report. J Cancer Res Ther. 2018 Jan-Mar;14(2):454-456.
View at Publisher | View at Google Scholar - Zayko MO, Velilla RE, Shurbaji MS (2018). Condyloma Acuminata Presenting as Isolated Papillary Lesions in the Prostatic Urethra. Am J Case Rep. 2018 Dec 22;19: 1522-1525.
View at Publisher | View at Google Scholar - Sen R, Shah N, Sheikh MA, Chatterjee RP (2018). Oral condyloma acuminatum in a 75-year-old geriatric patient. BMJ Case Rep. 2018 Feb 1;2018:bcr2017222905.
View at Publisher | View at Google Scholar - Rimkevičius A, Pūrienė A, Gaigalas M. Condyloma acuminatum: some aspects. Acta Medica Lituanica. 2011 Apr 1;18(2):43-6.
View at Publisher | View at Google Scholar - Shruti S, Siraj F, Singh A, Ramesh V (2017). Epidermodysplasia verruciformis: three case reports and a brief review. Acta Dermatovenerol Alp Pannonica Adriat. 2017 Sep;26(3):59-61.
View at Publisher | View at Google Scholar - Ingordo V, Ferrara G, Ingordo I, Argenziano G (2020). A case of post-inflammatory warty dyskeratoma of the chest: Other dermoscopic features. Dermatol Reports. 2020 Oct 22;12(2):8791.
View at Publisher | View at Google Scholar - Helwig EB (1954). Proceedings of the 20th seminar on skin neoplasms and dermatoses, International Congress of Clinical Pathologists, 1954 Sept, Washington, DC, USA. Am Soc Clin Pathol. 1955:53-6.
View at Publisher | View at Google Scholar - SZYMANSKI FJ (1957). Warty dyskeratoma; a benign cutaneous tumor resembling Darier's disease microscopically. AMA Arch Derm. 1957 Apr;75(4):567-72.
View at Publisher | View at Google Scholar - GRAHAM JH, HELWIG EB (1958). Isolated dyskeratosis follicularis. AMA Arch Derm. 1958 Apr;77(4):377-89.
View at Publisher | View at Google Scholar - Ackerman AB (1972). Focal acantholytic dyskeratosis. Arch Dermatol. 1972 Nov;106(5):702-6. PMID: 4635801.
View at Publisher | View at Google Scholar - Diallo M, Cribier B, Scrivener Y (2007). Dyskératome verruqueux: une tumeur d'origine infundibulaire [Warty dyskeratoma: infundibular histogenesis. Anatomoclinical study of 43 cases]. Ann Dermatol Venereol. 2007 Aug-Sep;134(8-9):633-6.
View at Publisher | View at Google Scholar - Kaddu S, Dong H, Mayer G, Kerl H, Cerroni L (2002). Warty dyskeratoma--
View at Publisher | View at Google Scholar - Griffiths TW, Hashimoto K, Sharata HH, Ellis CN (1997). Multiple warty dyskeratomas of the scalp. Clin Exp Dermatol. 1997 Jul;22(4):189-91. PMID: 9499610.
View at Publisher | View at Google Scholar - Martorell-Calatayud A, Sanmartin-Jimenez O, Traves V, Guillen C (2012). Numerous umbilicated papules on the trunk: multiple warty dyskeratoma. Am J Dermatopathol. 2012 Aug;34(6):674-5.
View at Publisher | View at Google Scholar - Ugras N, Adim SB, Kilicoglu M, Baskan EB (2014). Multiple warty dyskeratomas: case report. Iran J Public Health. 2014 Aug;43(8):1145-7.
View at Publisher | View at Google Scholar - Torres KM, Junkins-Hopkins JM (2016). Cystic acantholytic dyskeratosis of the vulva: An unusual presentation of a follicular adnexal neoplasm. Indian Dermatol Online J. 2016 Jul-Aug;7(4):272-4.
View at Publisher | View at Google Scholar - Allon I, Buchner A (2012). Warty dyskeratoma/focal acantholytic dyskeratosis--an update on a rare oral lesion. J Oral Pathol Med. 2012 Mar;41(3):261-7.
View at Publisher | View at Google Scholar - Tanay A, Mehregan AH (1969). Warty dyskeratoma. Dermatologica. 1969;138(3):155-64.
View at Publisher | View at Google Scholar - Baran R, Perrin C (1997). Focal subungual warty dyskeratoma. Dermatology. 1997;195(3):278-80.
View at Publisher | View at Google Scholar - Vargas-Laguna E, Imbernón-Moya A, Aguilar-Martínez A, Burgos F (2017). An Unusual Location of Subungual Warty Dyskeratoma: A Case Report and Review of the Literature. Case Rep Dermatol Med. 2017;2017:3613109.
View at Publisher | View at Google Scholar - DiMaio DJ, Cohen PR (1998). Incidental focal acantholytic dyskeratosis. J Am Acad Dermatol. 1998 Feb;38(2 Pt 1):243-7.
View at Publisher | View at Google Scholar - Salerni G, Alonso C, Calligaris M, Gorosito M, Fernández-Bussy R (2017). Dermoscopy of multiple warty dyskeratomas. Dermatol Pract Concept. 2017 Oct 31;7(4):47-49.
View at Publisher | View at Google Scholar - Nakagawa T, Umekage K, Komatsu S, Mizumoto T, Hashimoto Y, et. al (2017). Case of warty dyskeratoma with unique dermoscopic features. J Dermatol. 2018 Apr;45(4):e74-e75.
View at Publisher | View at Google Scholar - Lencastre A, Campos S, Cabete J. Warty dyskeratoma. J Am Acad Dermatol. 2016 Sep;75(3):e97-e98.
View at Publisher | View at Google Scholar - Isaka Y, Matsuda H, Ogita A, Saeki H, Tanaka M, Ansai SI (2018). Case of warty dyskeratoma on the anterior chest: The relationship between its dermoscopic and histopathological findings. J Dermatol. 2018 Jun;45(6):e171-e172.
View at Publisher | View at Google Scholar - Di Brizzi EV, Russo T, Piccolo V, Calabrese G, Mascolo M,(2019). Warty dyskeratomas: clinical and dermoscopic features. Int J Dermatol. 2019 Nov;58(11):e229-e231.
View at Publisher | View at Google Scholar
