

case report | DOI: https://doi.org/10.31579/2835-7957/098
Vaccine Marketing: Strategies for Promoting Public Health and Enhancing Vaccine Acceptance
1Department of Pharmacy, University of Karachi-Pakistan
2Fazaia Ruth Pfau Medical College Air University Karachi, Pakistan
3GD Pharmaceutical Inc OPJS University Rajasthan India
4Dow University of Health Sciences Karachi Pakistan
5Dow University of Health Sciences Karachi Pakistan
*Corresponding Author: Rehan Haider, Department of Pharmacy, University of Karachi-Pakistan.
Citation: Rehan Haider, Asghar Mehdi, Geetha K. Das, Zameer Ahmed, Ambreen Zameer, (2025), Vaccine Marketing: Strategies for Promoting Public Health and Enhancing Vaccine Acceptance, Clinical Reviews and Case Reports, 4(3); DOI:10.31579/2835-7957/098
Copyright: © 2025, Rehan Haider. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 09 May 2025 | Accepted: 22 May 2025 | Published: 02 June 2025
Keywords: vaccine marketing; community health; communication campaigns; target to foreshadow; collaborator engagement; trust; transparency; believeableness; cure acceptance; additional dose of vaccine programs
Abstract
Vaccine marketing serves as an essential tool in advancing community health by brightening the acceptance and rudeness of vaccines. In essence, it includes the calculated dissemination of facts, tailor-made to foreshadow, and engaging with colleagues to address concerns and impressions. The overarching aim is to efficiently communicate the benefits of immunization while supporting trust and confidence in additional doses of vaccine programs. Communication campaigns are a pillar of marketing efforts. These campaigns employ miscellaneous platforms in the way that established radio, social news, and society exceed programs to reach diverse audiences. By engaging in target messaging, marketers can address particular mathematical, educational, and socioeconomic factors that can influence curing rude answers. For instance, campaigns may stress the significance of immunization for vulnerable populations or climax the security and efficacy of vaccines through tributes and experimental evidence. Stakeholder date is another crucial facet of cure marketing. This involves colluding and accompanying healthcare providers, community rulers, policymakers, and advancement groups to spread accurate news and address concerns in a convenient class. By partnering with trustworthy beginnings, vaccine marketers can intensify their ideas and build believability within societies. Transparency and believeableness are fundamental standards that underpin favorable cure marketing initiatives. Providing clear and correct facts about the growth, safety, and productiveness of vaccines helps to lighten misstatements and build trust among all. Additionally, continuous listening and evaluation of marketing campaigns allow marketers to perfect their strategies and adapt them to evolving needs and challenges. In summary, cure marketing plays an important role in advancing public health by supporting the agreement and uptake of vaccines. Through focus ideas, partner engagement, and an obligation to transparency, marketers can help guarantee that vaccines reach those who need them most.
Introduction
An impacted tooth cannot erupt into its normal functional position.1 Most impactions are asymptomatic and usually do not cause any abnormalities. However, some impacted teeth can lead to pathological complications such as resorption of adjacent tooth roots, cyst formation, loss of arch length, and referred pain.[2] Impaction of the maxillary canine is a common clinical issue. The canine is vital for facial appearance, dental aesthetics, arch development, and occlusion.[3] They also provide significant support for the cheeks, and their absence can result in a flattened appearance of the upper lip.
Failure of a tooth to erupt due to impaction can disrupt occlusion, increase the risk of infection and cyst formation, root resorption of adjacent lateral incisors, and may even impact the psychological well-being of the affected individuals (4). The exact etiology of maxillary-impacted canines is unknown. There are several reasons: (1) physical obstruction by adjacent teeth, (2) loss of space in the arch, (3) over-retained deciduous teeth, and (4) differences in the direction of tooth movement. (5) genetic predisposition. After the third molars, maxillary canines are the most commonly impacted teeth (5). Their impaction occurs more than twice as often as mandibular canines.[6] Additionally, the incidence is twice as high in females than in males, with palatal canine impaction being more frequent than labial impaction. The impaction of all four permanent canines is very rare.[7] Given the patient's age, an intraoral clinical assessment is the initial step in formulating a diagnostic hypothesis. Early diagnosis and timely intervention during the mixed dentition period are crucial for successfully managing cases of impacted canines. Certain clinical signs may indicate the presence of an impacted canine, such as the persistence of a deciduous canine beyond the age of 14 to 15 years, the absence of a canine bulge or its palatal appearance, and a deviation in the tip of the lateral incisors.[8] Palpation of the alveolar bone is advised on the palatal and buccal sides of the alveolar process in the canine region. The absence of a palpable bulge is considered abnormal, and a slightly concave contour of the alveolar bone mesial to the deciduous canine may indicate an eruption anomaly.[9] In addition to clinical examination, radiographs are crucial for accurate diagnosis.[10] Radiographic techniques include lateral, occlusal, panoramic, and periapical radiographs. The precise position of the impacted canine relative to adjacent teeth can be assessed using the same lingual and opposite buccal technique and cone-beam computed tomography (CBCT). Panoramic radiographs are recommended for early prediction of maxillary impacted canines from the age of 8 and are also suggested for older children (>11 years) without erupted canines if the canine bulge is impalpable. [11] In clinical practice treating patients with impacted maxillary canines is often perceived as more challenging and time-consuming than typical orthodontic cases. The treatment duration was influenced by the distance of the impacted canine from the occlusal plane, its angulation, and its medial displacement. The dilemma arises whether to attempt and bring the impacted tooth into the arch, knowing this will extend treatment time and increase costs, or to extract the tooth, which might save time and money but compromise aesthetics and long-term function. The most common approach to repositioning impacted canines involves surgically exposing the tooth, placing an attachment to the exposed area, and then using orthodontic traction to move the tooth into the desired position. Extraction is typically considered when the canine is in an unfavorable position, potentially leading to complications (12). A multidisciplinary approach is necessary for treating impacted canines. The literature presents various treatment options for maxillary canine impaction,[13][14] though there is no absolute consensus on the best treatment protocol for these cases.
Case Report
Diagnosis
An African female, aged 12 years and 11 months, had a presenting complaint of “missing upper canine and crooked teeth” with an insignificant medical history. She has a habit of occasional nail biting and a family history of impacted maxillary canines in her mother and brother. She has a bilaterally symmetrical face, a mesio-cephalic skull shape, a straight soft tissue profile, a small size of nose and prominent chin appearance, a normal nasolabial angle, and competent lips (►Fig. 1).

Figure: 1
Adequate gingival exposure was noted on her smile. Intraoral and cast examinations (►Figs. 1 and 2) demonstrated Class I incisors, impacted canines, and Class I bilateral molar relationship.
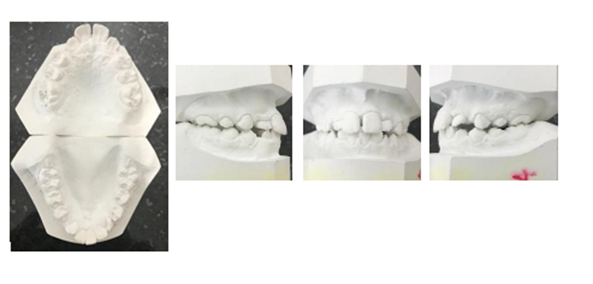
Figure: 2
The midline was coincident with the face and lower teeth. Overjet of 2 mm, an overbite of 3 mm, and crowding of -5 mm in the upper and -7 mm in the lower jaws were observed. The patient is in the permanent dentition stage, 13,23,43 teeth are clinically missing and impacted. The upper and lower arches are V in shape. Gingival recession was observed on all anterior teeth in both the upper and lower jaws. During the opening or closing of her jaws, no mandibular deviations or clicking noises were detected. The panoramic radiograph (►Figure. 3A) showed all permanent teeth were present, 13,43,23,37 teeth were impacted. According to the Nolla stage of root formation grading system, tooth no. 18 was in stage 4, and tooth no. 28,38,48 teeth were in stage 5, tooth no. 27 was in stage 7, whereas tooth no. 17,37,47 were in stage 8, tooth no. 13,23,43,33,15,25,35,45,14,24,34,44 were in Nolla stage 9 and the remaining teeth including 1st molars and upper and lower incisors were in Nolla stage 10. No other associated anomaly was noticed in the OPG assessment. The Pretreatment cephalometric analysis (►Figure. 3B, ►Table 1) showed a Class I skeletal relationship with a high-angle vertical growth pattern. Normal upper incisors and proclined upper incisors with a hold away ratio of 6:1 showing little or no chin support and procumbent lower lips with a small nose size were observed.
Diagnostic And Evaluation of The Maxillary Canines
| Measurement | Norms | Pre-Treatment | Post-Treatment |
| SNA | 82±2 | 80 | 82 |
| SNB | 78±2 | 76 | 80 |
| ANB | 2±2 | 4 | 2 |
| Facial Angle | 87±3 | 85 | 86 |
| Mac-A (mm) | 1±2 | -1 | -2 |
| Mac-Pog (mm) | -3±4 | -8 | -6 |
| Wits | 0±2 | -1 | 0 |
| SNMP | 32±2 | 40 | 40 |
| FMA | 25±2 | 36 | 35 |
| Y-AXIS | 60±2 | 61 | 62 |
| UI-SN | 102±4 | 108 | 125 |
| IMPA | 87±3 | 90 | 93 |
| II | 125-135 | 117 | 116 |
| UI-NA | 22 | 27 | 40 |
| UI-NA (mm) | 4±2 | 5 | 6 |
| LI-NB | 25 | 29 | 24 |
| LI-NB (mm) | 4±2 | 6 | 5 |
| Holdaway Ratio | 1:1 | 6:0 | 2.5:1 |
| S-Plane | 0±2 | +6 | +4 |
| Z- Angle | 76±5 | 56 | 65 |
| Nasiolabil Angle | 90-110 | 99 | 99 |
Table I: Cephalometric Analysis
Clinical Assessment
Intra oral examination revealed the presence of a canine bulge on top of the lateral incisor on the right side. However, the canine bulge was neither visible nor palpable on the left side ►Figure. 1 and 2)
Prognostic Evaluation
Different aspects of canine position were assessed using radiographs, with prognostic factors referenced from McSherry (15), Pitt, Hamdan, and Rock (16), and Counihan, Al-Awadhi, and Butler (17).
1. The extent of the canine crown's horizontal overlap with the adjacent incisor: In our patient, the canines were closer to the midline and overlapping the adjacent lateral incisors, but not the central incisor (Figure 3A). This suggested a poor prognosis and a risk of lateral incisor root resorption during canine traction.
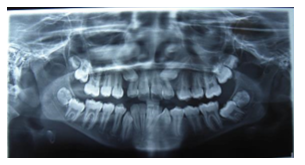
Figure: 3A
2. The vertical height of the canine crown: In this case, the canine tips were located more than halfway up the root of the central incisor but less than the complete length of the root (Figure 3B), indicating an average prognosis.

Figure: 3B
3. Canine angulation to the midline: The canines in this patient were mesioangular at 35 and 40 degrees to the midline on the left and right sides, respectively (Figure 3C). This made the case more challenging in terms of biomechanics and the application of orthodontic forces.
Ericson and Kurol (1988) defined the number of sectors to denote different types of impactions (18). The canines' cusp tips were located in sector 3 with an angulation of 35 and 40 degrees, suggesting a poor prognosis.
The case was diagnosed as Angle’s Class I malocclusion on a class I skeletal base with an orthognathic maxilla associated with an orthognathic mandible, upper and lower anterior crowding, with impaction of right maxillary canine and left canine with challenging prognostics.





Treatment Objectives
The goals were to bring the upper canine back in the arch and achieve canine-guided occlusion, expand the upper arch to give support to upper lips while correcting crowding and maintaining transverse dimension and bilateral Class I molar relationship.
Treatment Alternatives:
To achieve the above treatment goals, two plans were discussed with the patient and her mother during consultation. Plan A was surgical exposure of impacted 13 and 23 and tracking them to the arch, combined with fixed orthodontic treatment including extraction of all first premolars that give us the desired result in lip support and canine guided occlusion type A anchorage is planned for maxilla, advised to band upper 7’s and place trans palatal Arch to maintain Class I molars while tracking upper canines. Plan B was to extract upper maxillary canines as they were very high in position and simulate 14 as 13, 24, and 23. As a patient still in the growing phase, Plan A was recommended and accepted by the patient and parents. Also fixed retention was advised on completion of treatment.
Treatment Progress
At the onset of treatment, the patient was referred to a periodontist for consultation to address the issue of a gingival recession on tooth no. 11, 21, 41 and 42 anterior. The patient was classified with class I in Miller's Classification of gingival recession in 11 and 21. It was decided to use minimal orthodontic forces during treatment to prevent further damage to the periodontium. In addition, the patient was advised to keep up with good oral hygiene protocol throughout the orthodontic treatment.
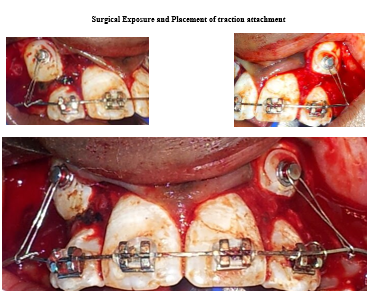
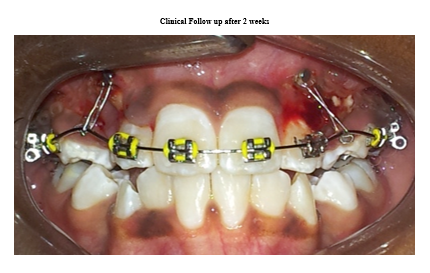
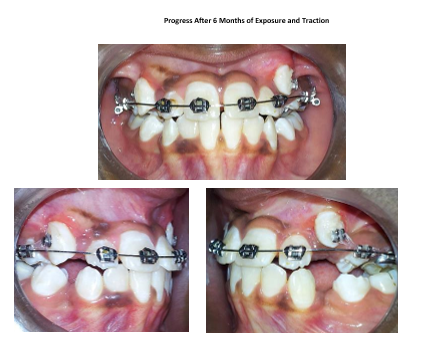
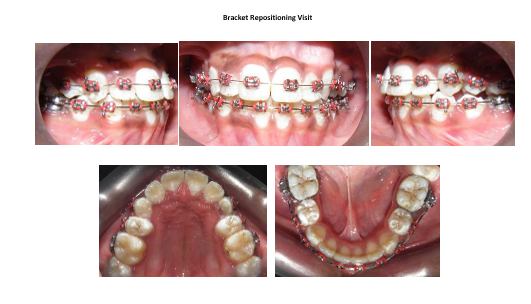
The patient was also sent to the Maxillofacial surgeon for evaluation of 13 and 23 exposure and traction. After using SLOB radiographic technique it was found that canines are positioned very high on the buccal side. Bands were placed on the maxillary first molars and an impression was made for a transpalatal arch fabrication in a laboratory. Pre-adjusted 0.022 0.028” slot straight wire MBT prescription brackets were bonded in the upper arch and 0.014 MNiTi archwires were used for the initial leveling followed by use of 16*25 MNiTi, upper first premolars were extracted after 6 months of bonding, after 9 months of basic alignment, the patient went under general anesthesia for surgical exposure of impacted upper canines. Orthodontic attachments and traction wire were placed in the operating room and follow-up appointments in the clinic were made after one month. During follow-up visits, the canine was first pulled distally and then pulled occlusal to protect the root of lateral incisors from resorption. Once the canine came back in occlusion, lower braces were placed followed by extraction of lower first premolars. After 4 months OPG was done (►Fig. 5), alignment of roots and crowns were assessed and the patient was booked for a bracket repositioning visit, any repositioning errors were corrected in that visit and the wire dropped to 0.016 MNiTi, alignment was continued, spaces were consolidated and midlines were corrected, wires were progressed from 0.016 MNiTi to 16*25 MNiTi to 18*25 MNiTi in both arches. The interproximal reduction was performed on the upper incisors to correct residual midline shifts in the upper jaw. A final archwire of size 0.017 x 0.025 SS was inserted, and the case was completed with a prescription for settling elastics (1/4 inch, 6 oz.). After debonding upper and lower fixed retainers were placed from canines to canines in both upper and lower arches. The total active orthodontic treatment duration was 4 years.

Figure: 5
Treatment Results
Post-treatment treatment records showed that the treatment objectives were successfully achieved (►Figure. 6). A positive smile arc with well aligned teeth, and canine guided occlusion was noticed. In addition, marked improvement in the patient’s self-esteem and confidence was
observed. The patient’s lip support was improved in functionality, offering overall great satisfaction to the patient. Extraoral photographs showed marked improvement in facial esthetics (►Figure. 6). Class I incisors, canine and molar relationships were maintained (►Figure. 6 and 6), and midline deviation was corrected with the achievement of ideal overbite and overjet.
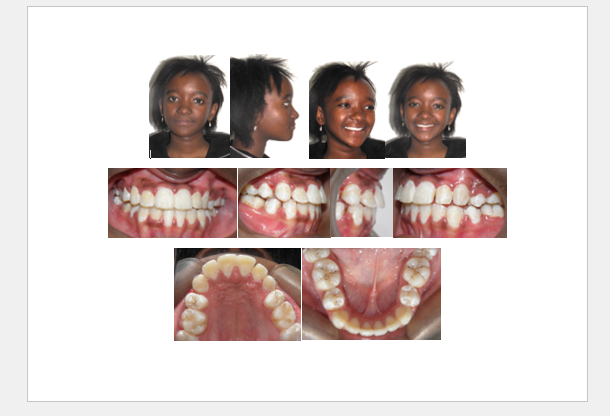
Figure: 6
The upper arch was expanded to parabolic in shape and canines were tracked into the occlusion. The panoramic radiograph showed satisfactory
root parallelism (suggest tooth # left upper second premolar, left lower canine, and right lower 2nd premolar roots should go distal) with proper space in between teeth (►Figure. 7).

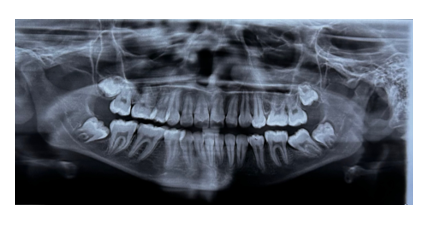
Figure: 7
Post treatment lateral cephalometric analysis (►Table 1) showed forward mandibular growth improving ANB angle from 4 to 2 degrees, facial angle
from 85 to 86 degrees and Mcnamara-pog reading improved from -8 to -6 mm. Vertical dimension was maintained. Significant proclination of the
maxillary (U1-SN, 108–125) and mandibular incisors (IMPA 90–93) was observed compared with the pretreatment angles. Improvement in soft tissue profile was noted (Z angle, 56-65) (►Figure. 1, 6, and 7). These achieved results are stable and retained as shown in 5 years retention pictures (►Figure. 8).

Figure: 8
Case Discussion:
Treatment success in this case results from the combined efforts of the orthodontist, oral surgeon, and the patient. Canines are the cornerstone of the dental arches. Several treatment options are available for correcting impacted maxillary canines including observation, intervention, relocation, and extraction. The option with the most favorable long-term prognosis is to bring these teeth into alignment, the choice depending on factors such as the position of the impacted canine and anchorage requirements. In this case, the position of both maxillary canines was not very favorable but an attempt was made based on the age of the patient as she was still in the growing phase and in her early permanent dentition. In the literature, two basic approaches are described for the surgical exposure of impacted teeth: open (apically positioned flap) and closed-eruption techniques. The closed-eruption technique is often considered the best method for uncovering labially impacted teeth, especially if the tooth is located high above the mucogingival junction or deep in the alveolus, where using technique to place apically positioned flap may be hard to be successful [19,20]. Some clinicians believe that the closed-eruption method replicates natural tooth eruption, producing the best aesthetic and periodontal results. Vermette et al. compared these two surgical techniques and found that the apically positioned flap technique had more negative aesthetic effects, such as increased crown length and gingival scars, than the closed-eruption technique [21]. Despite the benefits of the closed eruption technique for canine traction, the clinical decision in the operating room was to remove surrounding bone during the exposure of impacted canines and to use an apically positioned flap. This decision was made by the surgeon in agreement with the treating Orthodontist, to prevent the patient from needing readmission under general anesthesia in case of detachment during canine traction. To bring the canine into occlusion with supporting periodontium, as an orthodontist we must aim for low forces and plan appropriate biomechanics to protect the roots of the lateral incisors during traction of maxillary canines, in addition to ensuring sound bone and gingival support for canines. Deficiency in the amount of attached gingiva poses a potential risk for gum recession and plaque accumulation. The maintenance of oral hygiene was crucial for achieving the final clinical height of the crown after orthodontic treatment. The periodontal status of the exposed canines after orthodontic treatment showed an acceptable gingival contour and attached gingiva as illustrated in post-treatment and 5-year retention intraoral pictures and side effects of apical positioning flap technique were limited using controlled mechanics. Anchorage was prepared with the placement of molars bands and transpalatal arch to control reactionary intrusive forces and mesial migration of maxillary 1st molars. Traction of both maxillary canines was done with ligature wires distally initially followed by occlusally in direction. The piggyback technique was used in managing this case. This technique employs rigid stainless-steel base archwires to increase stabilizing force on abutment teeth and auxiliary super-elastic NiTi wire to provide inherent flexibility for correcting malposed teeth by providing continuous eruptive force. Subsequent alignment using the piggyback technique is achieved by ligating the auxiliary archwire to the canine attachment and inserting the ends into the auxiliary tube of the molar band. All the above-mentioned intra-arch mechanics may tip or intrude adjacent teeth. We have encountered such effects during treatment and corrected them by repositioning the brackets and by using vertical eruptive forces that can be applied using intermaxillary elastics. However, the use of intermaxillary elastics requires patient compliance, we got lucky in this regard, the patient was highly self-motivated and cooperative. Appointments were scheduled at 3-week intervals for regular monitoring and adjustments and treatment finished in four years.
We achieved our goal in this case by not only tracking the impacted maxillary canine into normal alignment but also achieving functional occlusion, a healthy zone of attached gingiva, and ideal alveolar bone height on completion of treatment.
Conclusion:
Managing impacted maxillary canines is always a challenge for orthodontists. Successful management is crucial for both aesthetic and functional reasons. Ongoing assessment and early intervention can help prevent adverse situations. Proper treatment planning, effective space management, and the application of light, continuous traction forces are the key factors determining the success of each impacted case. The treatment outcome in this case is quite satisfactory.
Patient Consent:
The patient has provided written informed consent
References
- Becker A. (2007). 2nd ed. London: Informa Healthcare; The Orthodontic Treatment of Impacted Teeth. [Google Scholar]
View at Publisher | View at Google Scholar - Bishara SE. (1992). Impacted maxillary canines: A review. Am J Orthod Dentofacial Orthop. 101:159–171. [PubMed] [Google Scholar]
View at Publisher | View at Google Scholar - Bedoya MM, Park JH. (2009). A review of the diagnosis and management of impacted maxillary canines. J Am Dent Assoc. 140:1485–1493. [PubMed] [Google Scholar]
View at Publisher | View at Google Scholar - Seehra J, Yaqoob O, Patel S, et al. National clinical guidelines for the management of unerupted maxillary incisors
View at Publisher | View at Google Scholar - in children. Br Dent J. (2018). 224(10):779-85. https://doi.org/10.1038/sj.bdj.2018.361 PMid:29795486
View at Publisher | View at Google Scholar - Bishara SE. (1998). Clinical management of impacted maxillary canines. Semin Orthod.4(2):87–98.
View at Publisher | View at Google Scholar - Yavuz MS, Aras MH, Büyükkurt MC, Tozoglu S. (2007). Impacted mandibular canines. J Contemp Dent Pract. 8:78–85. [PubMed] [Google Scholar]
View at Publisher | View at Google Scholar - Crawford LB. (2000). Four impacted permanent canines: An unusual case. Angle Orthod. 70:484–499. [PubMed] [Google Scholar]
View at Publisher | View at Google Scholar - Hirschhaut M, Leon N, Gross H, Flores-Mir C. (2021). Guidance for the clinical management of impacted maxillary canines. Compend Contin Educ Dent .42(5): 220-226.
View at Publisher | View at Google Scholar - Sajnani AK, King NM. (2012). Early prediction of maxillary canine impaction from panoramic radiographs. Am J Orthod Dentofacial Orthop. 142(1): 45-51.
View at Publisher | View at Google Scholar - Shin JH, Oh S, Kim H, et al. (2022). Prediction of maxillary canine impaction using eruption pathway and angular measurement on panoramic radiographs. Angle Orthod; 92(1): 18-26.
View at Publisher | View at Google Scholar - Eslami E, Barkhordar H, Abramovitch K, Kim J, Masoud MI. (2017). Cone-beam computed tomography vs. conventional radiography in visualization of maxillary impacted-canine localization: A systematic review of comparative studies. Am J Orthod Dentofacial Orthop 151(2): 248-258.
View at Publisher | View at Google Scholar - Sajnani AK, King NM. Complications associated with the occurrence and treatment of impacted maxillary canines.
View at Publisher | View at Google Scholar - Migliorati M, Cevidanes L, Sinfonico G, et al. (2021). Three dimensional movement analysis of maxillary impacted canine using TADs: A pilot study. Head Face Med ,17(1):
View at Publisher | View at Google Scholar - Chaushu S, Becker A, Chaushu G. (2008). Lingual orthodontic treatment and absolute anchorage to correct an impacted maxillary canine in an adult. Am J Orthod Dentofacial Orthop; 134(6): 811-819.
View at Publisher | View at Google Scholar - McSherry PF. (1996). The assessment of and treatment options for the buried maxillary canine. Dent Update. 23(1):7-10
View at Publisher | View at Google Scholar - Pitt S, Hamdan A, Rock P. (2006). A treatment difficulty index for unerupted maxillary canines. Eur J Orthod. 28(2):141-144.
View at Publisher | View at Google Scholar - Counihan K, Al-Awadhi EA, Butler J. (2013). Guidelines for the assessment of the impacted maxillary canine. Dent Update. 40(9):770-2, 775-777.
View at Publisher | View at Google Scholar - Ericson S, Kurol J. (1998). Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur J Orthod. 10(4):283-295.
View at Publisher | View at Google Scholar - Crescini A, Clauser C, Giorgetti R, Cortellini P, Pini Prato GP. Tunnel traction of infraosseous impacted maxillary canines. A three-year periodontal follow-up. Am J Orthod Dentofacial Orthop199410561-72
View at Publisher | View at Google Scholar - Wong-Lee T, Wong F. (1985). Maintaining an ideal tooth-gingiva relationship when exposing and aligning an impacted tooth. Br J Orthod,12:189-192.
View at Publisher | View at Google Scholar - Vermette ME, Kokich VG, Kennedy DB. (1995). Uncovering labially impacted teeth: apically positioned flap and closed-eruption techniques. Angle Orthod, 65:23-34
View at Publisher | View at Google Scholar
