

Case Report | DOI: https://doi.org/10.31579/2835-835X/062
Unilateral Spinal Cord Infarction Presenting as Stroke: A Rare Interventional Case Report
- Karthick Murugesan 1
- Thiruvengadarajan Vasanthi Srinivass 2
- Shalini Sivadasan 2
- Suresh Kumar Krishnan 2
- Rajasekaran Aiyalu 2
- Senthil Kumar Elumalai 3
1Pharm.D Intern, KMCH College of Pharmacy, Coimbatore 641 048, Tamil Nadu, India.
2Professor, KMCH College of Pharmacy, Coimbatore 641 048, Tamil Nadu, India.
3Consultant Neurologist, Kovai Medical Center and Hospital, Avinashi road, Coimbatore 641 014, Tamil Nadu, India
*Corresponding Author: Thiruvengadarajan Vasanthi Srinivass, Professor, KMCH College of Pharmacy, Coimbatore 641 048, Tamil Nadu, India.
Citation: Karthick Murugesan, Thiruvengadarajan V. Srinivass, Shalini Sivadasan, Suresh K. Krishnan, R. Aiyalu, et.al, (2024), Unilateral Spinal Cord Infarction Presenting as Stroke: A Rare Interventional Case Report, Clinical Trials and Case Studies, 3(3); DOI:10.31579/2835-835X/062
Copyright: © 2024, Thiruvengadarajan Vasanthi Srinivass. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 March 2024 | Accepted: 18 March 2024 | Published: 03 June 2024
Keywords: spinal cord infarction; left hemiparesis; magnetic resonance imaging; thrombolytics
Abstract
Spinal Cord Infarction is an uncommon destructive neurovascular disorder that occurs more infrequently than cerebral infarction that accounts for 0.3-2% only of all neurological vascular disease conditions. It mostly presents as cerebrovascular accident or Central nervous system Demyelination. This case aims to describe the atypical presentation of idiopathic SCI and its possible aetiologies. A 54-year-old man with no relevant past medical history admitted to the emergency department, presented with left hemiparesis and right facial palsy. The initial Magnetic Resonance Imaging of the brain was non-diagnostic, and the patient was admitted to intensive care unit for surveillance. With the strong clinical suspicion of infarction, the patient was treated with thrombolytics and steroids. On the second day extensive imaging of cervical spine study revealed left anterolateral cervical cord C5-C7 vertebral infarcts and hence antiplatelets and anticoagulants were initiated. The patient improved significantly with physical rehabilitation and was discharged with dual antiplatelet therapy.
Introduction
Spinal cord infarction (SCI) is an uncommon severe destructive neurovascular disorder predominantly due to abruptly reduced blood supply to the spinal cord, following ischemia, infarction and spinal cord weakness [1,2]. It constitutes only 0.003% of all events and 0.3-2% of all stroke cases [3]. The clinical presentation is defined by the involvement of vascular territory and its severity may vary from disability to minor impairment [4]. The common cause of spinal stroke is not identified. Causes can be categorized into iatrogenic and non-iatrogenic where, iatrogenic may be due to aortic surgeries or injuries to the spinal cord and non-iatrogenic can be due to trauma, polycythaemia vera, myelitis, arteriovenous malformations, infections or neoplasm [3,5]. Magnetic Resonance Imaging (MRI) is the significant tool for imaging and diagnosing SCI [6,7]. Imaging presentations of hyperintense T2 signal changes and restricted diffusion in the spinal cord are the diagnostic parameters for SCI [8,9]. The treatment for SCI is still not clear and the use of thrombolytics and steroids has a lack of evidence [3]. In most of the situations, SCI was misdiagnosed as cerebrovascular accident or central nervous system demyelination because of negative MRI reports. This case aims to describe the atypical presentation of idiopathic SCI and its diagnosis, particularly for the treatment and its possible aetiologies.
Case Report
A 54-year-old man with no relevant past medical history presented to the Emergency Department (ED) complaining of sudden onset of left upper and lower limb weakness, deviation of mouth to right side, dysarthria and aphasia. There was no record of injury, infection, surgery, smoking or alcohol. No allergies were reported. On arrival, his vitals were: blood pressure 140/60 mm/Hg, heart rate 68 beats/min, respiratory rate 20 breaths/min, body temperature 97.6℉, and oxygen saturation 99% on ambient air. On neurological checkup, he was completely conscious and alert, with no neck rigidity and no cranial nerves or right limb disabilities. Left-side hemiparesis was presented with severe upper limb weakness (proximal > distal), and left Lower Motor Neuron (LMN) facial palsy. A MMT showed left upper and lower limbs had flaccid tone with 3/5 power (Table 1). Deep tendon reflexes were brisk in the right patellar and hypoactive in the left patellar and left achilles.
| On arrival | |
Right | Left | |
Hip flexion | 5/5 | 3/5 |
Hip extension | 5/5 | 3/5 |
Wrist flexion | 5/5 | 1/5 |
Grip strength | 5/5 | 0/5 |
Ankle dorsiflexion | 5/5 | 3/5 |
Knee extension | 5/5 | 3/5 |
Elbow extension | 5/5 | 3/5 |
Wrist extension | 5/5 | 3/5 |
Table 1: Manual Muscle Testing score on admission
Plantar responses were flexor and sensory tests exhibited reduced pinprick sensation on left feet with normal temperature and position was also normal. He had urinary incontinence and a catheter was inserted to prevent urinary retention. Based on the clinical presentations of stroke, MRI brain was performed within 2.5 h from the onset of symptoms which showed no abnormal diffused weighted imaging (DWI), diffusion restriction suggestive of acute infarction and no evidence of large vessel occlusion (LVO) or significant stenosis. Haematological and biochemical findings were mostly within normal ranges VLDL-11.0 mg/dl; triglycerides-55mg/dl; HDL-39.8 mg/dl; total cholesterol-212 mg/dl; haemoglobin-14.2 g/dl; WBC-5900 cells; RBC-5.19 million cells; Platelet-238000 cells; urea-25 mg/dl; Creatinine, 0.8mg/dl; prothrombin time, 12seconds; INR, 1.00; homocysteine, 18.74 mol/L; except slight elevation in LDL, 169 mg/dl. liver function tests were also within normal limits (SGOT-27U/L; SGPT-28U/L; ALP-95U/L; Total Bilirubin-0.37 mg/dl; Direct bilirubin-0.05 mg/dl; Indirect bilirubin-0.32 mg/dl; Albumin-4.5 g/dl; Globulin-2.3 g/dl; Total protein-6.8 g/dl). Serum electrolytes were also found to be within limits. Macroscopic and microscopic urine analysis was normal. Based in the investigations the provisional diagnosis made was spinal cord demyelination or SCI. ECG showed sinus rhythm. A computed tomography aortogram was done from neck to thigh which showed no definite evidence of dissection or stenosis and normal angiography of the aorta. With the clinical presentation and strong clinical suspicion of infarction patient underwent thrombolysis with tenecteplase 15 mg; citicoline 500 mg; edaravone 30 mg; atorvastatin 80 mg was administered in ED, then the patient was shifted to ICU for continuous surveillance. After 12 h of thrombolysis, MRI brain with spine screening was performed, which showed no abnormal parenchymal DWI changes suggestive of no acute infarction in the brain, but spine screening showed long segment signal changes involving the left anterolateral cervical cord from C5-C7 vertebral levels with altered diffusivity represents ischemia. Hence, methylprednisolone (IVMP) 500 mg; enoxaparin (LMWH), 40 mg and aspirin 75 mg were administered. On the next day, MRI of the cervical spine was performed which revealed long segment non-enhancing T2 hyperintense signal changes showing diffusion restriction in the anterior and left anterolateral cervical cord at C5-C7 vertebral levels acute infarct, less likely other causes including demyelination. Finally, the patient was diagnosed with acute unilateral spinal cord infarction where the etiology cannot be identified. ECHO was done to rule out cardiac-related aetiologies, which showed normal left ventricle ejection fraction LVEF. The patient was found to be non-diabetic with HbA1c, 5.9%. antibody panel testing includes Anti-HIV 1&2, HCV AB & HBS AG, antiphospholipid antibody (APLA) IGM & IGG, anti-nuclear antibody (ANA) was negative were negative; VDRL syphilis testing was nonreactive; anti neutrophil cytoplasmic Antibodies (ANCA), P-ANCA and C-ANCA includes Anti PR3, negative (0.0390) and Anti-MPO, negative (0.4161). No relevant investigations were found in this case to identify the aetiology of SCI. The patient received five doses of pulse steroid therapy of intravenous methylprednisolone 500 mg, to prevent the risk of demyelination or myelitis. However, this did not improve neurological deficits. The patient was treated with enoxaparin (LMWH) 40 mg, aspirin 75 mg, atorvastatin 40 mg, and citicoline 500 mg. From day two patient started responding to treatment. On day 3, improvement in left-hand weakness was identified and finger weakness persisted. Physiotherapy and occupational therapy rehabilitation facilities were given. On day 6, the patient walked with minimal support and mild imbalance. On day 8, the patient was able to get up from the chair and walk without assistance, where no facial palsy was found and cranial nerves were normal. After day 8, the patient was stable and discharged with dual antiplatelets and hypolipidemic.
Discussion
SCI is an unusual and often calamitous neurovascular disorder [2]. It is incessantly misdiagnosed as cervical spondylitis, CNS demyelination or cerebrovascular accident. Often it presents as atypical with no classical presentation of SCI. In this case, unilateral SCI presents as left hemiparesis with facial palsy as a typical presentation of stroke. Detection of tiny infarctions in the upper cervical cord using thin-section, coronal DWI of brain MRI, unilateral and small-sized SCI is not often. MRI is sometimes unsuccessful or fails to find small ischemic lesions of the spinal cord. Earlier reports stated that in patients with SCI, spine MRI was persuasive in only a portion of patients with unilateral SCI [10]. The stage of illness or the size of the infarct may interfere in detection of SCI by spinal cord MRI [2]. Aetiology of SCI is still uncertain. Though SCI shares similar aetiologies with cerebral infarction, its characteristics without vessel dissection remain unidentified. The causes can be enumerated into iatrogenic and non-iatrogenic; where iatrogenic SCI is mostly due to aortic surgery, injuries or surgical procedures, whereas non-iatrogenic SCI is because of trauma, atherosclerosis, arteriovenous malformations, polycythaemia vera, myelitis, infections and neoplasms [3,5]. But, in this case, the patient had no past relevant vascular aetiology and comorbidities. Blood and biochemical examinations were normal within limits and the MRI brain showed no acute infract or LVO. MRI cervical spine disclosed infarcts in the left anterolateral spinal cord on C5-C7 with hyperintense T2 signal changes and diffusion restriction changes. Autoantibody panels were negative and there was no evidence to pinpoint the aetiology of SCI.
There are no recommendations for the treatment of SCI. No evidence or clear data is suggesting for use of fibrinolytics as an initial treatment for SCI. The use of antiplatelets, anticoagulants and hypolipidemic is justified to control and prevent cardiovascular risk. Corticosteroids should be considered independently to diminish medullary oedema and myelitis. The use of pulse steroids in SCI is still controversial and not definite [5,11]. In this case, the patient was admitted to ED within 1 hour of the onset of symptoms with clinical presentations of stroke, even though the MRI brain showed no acute infarcts patient underwent thrombolysis with Tenecteplase. MRI Cervical spine showed infarct in C5-C7 segment in spinal cord. Pulse steroid therapy and LMWH were given for 5days. Then patient managed with dual antiplatelet therapy (Aspirin and clopidogrel), neuroprotective (Citicoline, piracetam) and hypolipidemic (atorvastatin). However, there were no standardized guidelines, thrombolysis can be a better treatment option if there are no absolute and relative contraindications in administering fibrinolytics. Otherwise, antiplatelets and LMWH can be a wiser treatment option. Recovery and outcome are variable for every individual and determined by the size and region of the infarct, and aetiology of the infarct [12]. Rehabilitation is necessary and recommended for the improvement of neurological deficits. In SCI, maximal neurological weakness occurs within 12 h in most of the patients. Generally, SCI requires a shorter term than cerebral infarction. In this case, the patient recovered within 7 days of treatment and was able to walk without assistance.
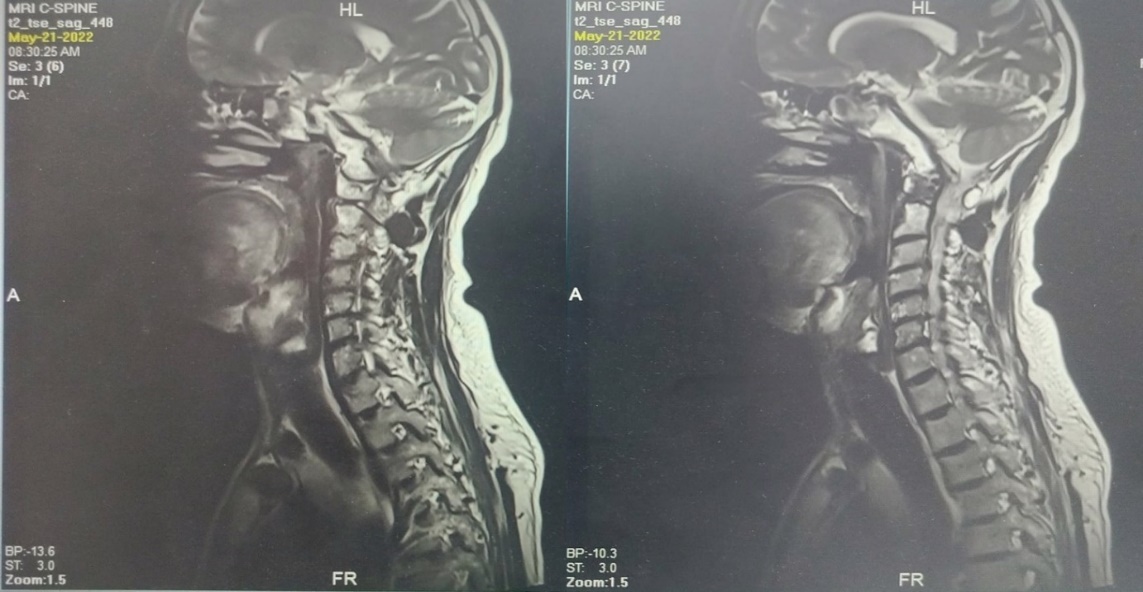
Figure 1. MRI spine findings of T2 hyperintense signal changes showing diffuse restriction in cervical cords at C5-C7 levels.
Conclusion
SCI is a destructive neurovascular disease with a lower incidence rate and atypical presentation including variety of symptoms and aetiologies. The diagnosis of SCI is hard and challenging for clinicians because of its variable presentations and sudden onset of weakness. In this study, we diagnosed a case of unilateral SCI presenting as stroke and treated with thrombolytics, pulse steroids and dual antiplatelet therapy and the patient improved significantly. Hence, we conclude that early presentation and diagnosis with DWI changes in the MRI spine need to be done to reduce the severity and progression of SCI. Thrombolysis can be beneficial in patients with no absolute or relative contraindications or otherwise can be managed with antiplatelets and LMWH. Recovery is based on the size of the infarct and the individual. In general, if SCI is diagnosed and treated rapidly in the acute phase, recovery is better compared to cerebral infarction.
Acknowledgement
The authors are thankful to the management of Kovai Medical Center and Hospital to carry out this case study.
Funding
The authors have no proprietary or commercial interest in any material discussed in this article.
Conflict of intertest
The authors hereby declare that, there is no conflict of interest.
Funding
None.
References
- Romi F, Naess H (2016). Spinal cord infarction in clinical neurology: a review of characteristics and long-term prognosis in comparison to cerebral infarction. European Neurology 76(3-4):95-98.
View at Publisher | View at Google Scholar - Vargas MI, Gariani J, Sztajzel R, et al (2015). Spinal cord ischemia: practical imaging tips, pearls and pitfalls. American Journal of Neuroradiology 36(5):825-830.
View at Publisher | View at Google Scholar - Correio MP, Ferreira A, Ermida V, et al (2017). Spinal cord infarction: case report and literature review]. Rev Soc Portuguesa Med Física Reabil 29: 40-44.
View at Publisher | View at Google Scholar - Cheshire WP, Santos CC, Massey EW, Howard JF Jr (1996). Spinal cord infarction: etiology and outcome. Neurology 47(2): 321-330.
View at Publisher | View at Google Scholar - Naik A, Houser SL, Moawad CM, Iyer RK, Arnold PM (2022). Non iatrogenic spinal cord ischemia: a patient level meta-analysis of 125 case reports and series. Surgical Neurology International 13:228.
View at Publisher | View at Google Scholar - Kister I, Johnson E, Raz E, et al (2016). Specific MRI findings help distinguish acute transverse myelitis of neuromyelitis optica from spinal cord infarction. Multiple Sclerosis and Related Disorder 9:62-67.
View at Publisher | View at Google Scholar - Weidauer S, Nichtweiß M, Hattingen E, et al (2015). Spinal cord ischemia: aetiology, clinical syndromes and imaging features. Neuroradiology 57:241-257.
View at Publisher | View at Google Scholar - Thurnher MM, Bammer R. (2006) Diffusion-weighted MR imaging (DWI) in spinal cord ischemia. Neuroradiology 48(11):795-801.
View at Publisher | View at Google Scholar - LoherTJ, Bassetti CL, Lovblad KO, Stepper FP, Sturzenegger M, et al. (2003) Diffusion-weighted MRI in acute spinal cord ischaemia. Neuroradiology 45(8):557–561.
View at Publisher | View at Google Scholar - Kumral E, Polat F, Gulluoglu H, Uzunkopru c, Tuncel, et.al. (2011). “Spinal ischaemic stroke: clinical and radiological findings and short-term outcome”. European Journal of Neurology 18(2):332-339.
View at Publisher | View at Google Scholar - Ros Castello V, Sánchez Sanchez A, Natera Villalba E, et al (2023). Spinal cord infarction: aetiology, imaging findings, and prognostic factors in a series of 41 patients. Neurologia (English Ed) 38(6):391-398
View at Publisher | View at Google Scholar - Hanson SR, Romi F, Rekand T, et al. (2015). Long-term outcome after spinal cord infarctions. Acta Neurologica Scandinavica 131(4):253-257
View at Publisher | View at Google Scholar
