

Case report | DOI: https://doi.org/10.31579/2834-796X/018
True Isolated Deep femoral artery aneurysm treated with endovascular technique: case report and literature review
- Rafael de Athayde Soares *
- Marcus Vinícius Martins Cury
- Aline Yoshimi Futigami
Hospital do Servidor Público Estadual de São Paulo, IAMSPE
*Corresponding Author: Rafael de Athayde Soares, Hospital do Servidor Público Estadual de São Paulo, IAMSPE
Citation: Athayde Soares RD., Martins Cury MV., Aline Y. Futigami., (2023), True Isolated Deep femoral artery aneurysm treated with endovascular technique: case report and literature review, International Journal of Cardiovascular Medicine, 2(2); DOI:10.31579/2834-796X/018
Copyright: © 2023, Rafael de Athayde Soares. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 March 2023 | Accepted: 21 March 2023 | Published: 27 March 2023
Keywords: deep femoral artery; endovascular surgery; deep femoral artery aneurysm
Abstract
In this paper, we aimed to report an alternative for endovascular treatment in a patient with an isolated deep femoral artery aneurysm. A 49 year-old male patient, with no comorbidities, was admitted with right limb pain, mainly in the thigh, associated with a weakness and difficulty to walking in the past seven days. The patient was submitted to a duplex ultrasound, that suggested a dilatated deep femoral artery aneurysm, with 6 cm diameter, confirmed with CT angiograman angioCT-scan. The patient was scheduled to undergo endovascular treatment of the deep femoral artery aneurysm with a covered self-expandable 9x100 Solarisâ and an embolization of the first branch of the Deep femoral artery with Azur â coils 2 4x5, 6x10, 6x15 and 6x20. The patient was transferred to the room, being discharged from the hospital two days after the surgery with no complications, femoral, popliteal and podalpalpable pedal pulses present bilaterally, takingon Aspirin 100mg / day and Clopidogrel 75mg/day. After At year1 month follow-up the patient was evaluated, presenting nowas asymptomatic and duplex showed patent stent without evidence of endoleak. further symptoms, no palpable mass in the right groin, and was submitted to a Duplex Ultrasound that showed deep femoral artery patency, stent patency and no endoleaks. Furthermore, after one year follow-up, the patient remains assymptomatic, with Duplex Ultrasound showing deep femoral and stent patency and no endoleaks.
Introduction
Isolated deep femoral artery aneurysms is a very rare disease, and due to a deep location profound localization, those aneurysms can grow extensively and most of times often remain undetected as a result of their deep location in the thigh. [1,2] Despite being a rare condition, this disease presents athese aneurysms are associated with a high incidence of rupture and may be associated with high rates of lower extremity major amputation. [2] Their Deep femoral artery aneurysms incidence is accounting account for around approximately 0.5% of all peripheral aneurysms and 1-2.6% of femoral aneurysms. [3] In the vast majority of cases, the etiology of deep femoral artery aneurysm’sit’s etiology is atherosclerosisotic, being more common with a higher prevalence in men (92%) with and a mean age of 70 years. [4,5]
Although Despite the revascularization of the deep femoral artery (DFA) is still controversial in the treatment of aneurysms, since some reports in literature recommend ligation of the DFA, when the superficial femoral artery is patent, the cornerstone of deep femoral artery aneurysm treatment is to prevent rupture and relieve venous compression and it`s symptoms associated, such as leg and thigh swelling, pain and varicose veins. In this era of evolving endovascular treatment, transcatheter embolization and stent graft placement have been reported as an alternative therapy to treat deep femoral artery aneurysms. [6]
In this study, we describe an option for endovascular treatment in a patient with an isolated DFA aneurysm. The Research Ethics Committee approved this study (decision number 32380920.5.0000.5463).
Case Report
A 49 year-old male patient, with no comorbidities, except for occasional smoking and overweight, was admitted with right limb pain, mainly in the thigh, associated with a weakness and difficulty to walk in the past seven days. The patient was submitted to a duplex ultrasound, that suggested a dilatated deep femoral artery, with 6 cm diameter. On physical examination, he had a good general health, with a pulsating bulge with fibroelastic consistency palpable in the right inguinal region. The patient had femoral, popliteal and distal pulses present bilaterally. The patient was submitted to a duplex ultrasound, that suggested a deep femoral artery aneurysm, with 6 cm diameter. and then. The patient was submitted to a computed tomography angiography (CTA) of the abdomen, pelvis and inferior limbs bilaterally. The CTA showed no other abnormalities in the arterial system, except for an isolated right deep femoral artery aneurysm, with 6,6 cm diameter. (Figures 1 and 2). The distance between the origin of the deep femoral artery aneurysm and the femoral common bifurcation was satisfactory (36,685cm), providing an adequate neck length for endovascular treatment (Figures 2-4). The proximal landing zone had 7,8mm diameter and distal landing zone had 7mm diameter. The total length of the DFAA was 6,85cm. Since there is no consensus in the literature regarding the best way to treat those kind of aneurysms, both techniques, open surgery and endovascular treatment, were extensively explained to the patient. The surgical team and the patient had decided to perform endovascular treatment.
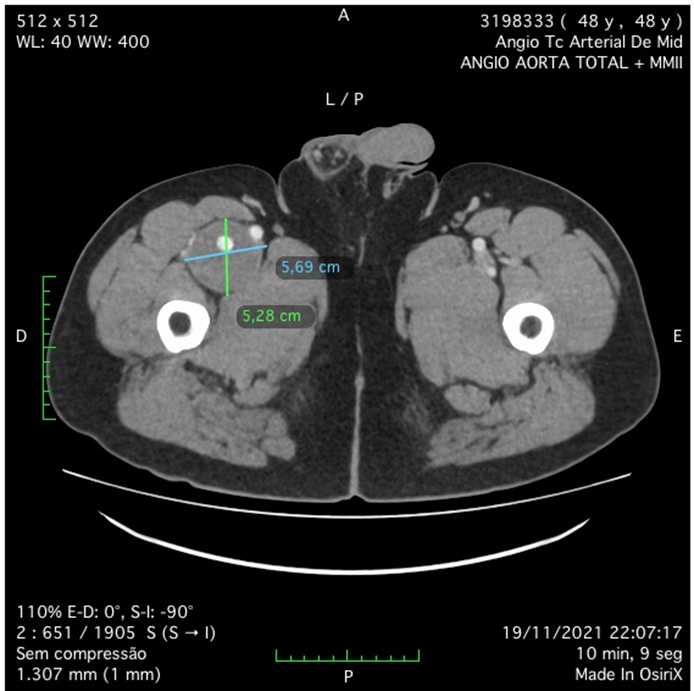
Figure 1: Angio-CT scan in axial incidence showing deep femoral artery aneurysm (DFFA).

Figure 2: Angio-CT scan showing DFFA
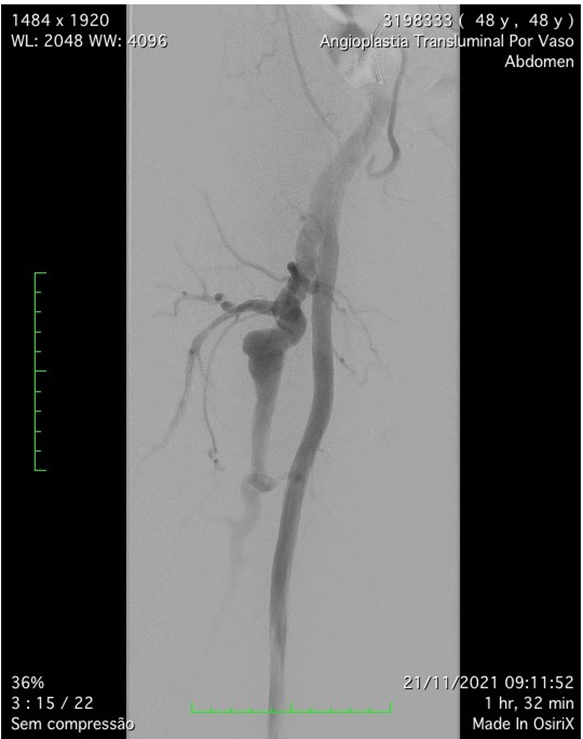
Figure 3: Preoperative arteriography confirming Deep femoral artery aneurysm.

Figure 4: Post-operative arteriography showing covered self-expandable 9x100 Solaris â into the Deep femoral artery.
The patient was scheduled to undergo endovascular treatment of the deep femoral artery aneurysm. Under general anesthesia, a left common femoral artery was punctured guided with a duplex ultrasound., with a 6f 11cm sheath. We decided to use a contralateral access and perform the whole intervention percutaneously. After the puncture, the Perclose Proglide â was inserted, in order to preload and guarantee the sealing of the puncture. Then, a 0,035”260cm Terumo â was passed untiused to perform the crossing overl of the aorta, and a 9F 11cm sheath was placed through the left common femoral artery. The patient was heparinized with 5000UI intravenous in bolus., and the aorta was crossed with an internal mammary 6F catheter alongside the 0,035”260cm Terumo â. We performed a right limb arteriography to confirm the deep femoral artery aneurysm (Figure 3s 5 and 6). The deep femoral artery was properly catheterizedselected with a Headhunter catheter 5F. After this, and we changed the guidewire for an Amplatz 0,035”260cm, in order to place a 55cm 9F delivery system catheter until the origin of the right deep femoral artery. In the arteriography, we have identified a larger branch emerging from the first portion of the deep femoral artery, and we have decided to embolize this branch, to avoid endoleak type II, since it was a larger branch. The microcatheter Progreat â 2,7F alongside the microguidewire Avigo â was used to select the branch. We embolized this branch with Azur â coils 2 4x5, 6x10, 6x15 and 6x20 (figures 7 and 8). After the successful embolization, a covered self-expandable 9x100 Solaris â (Scitech Medical, Brasil) was placed under roadmap into the proximal and distal deep femoral artery aneurysm, and post dilatated with a 9x80 catheter balloon Oceanus â (figure 4 Figures 9 and 10). There were no endoleaks, and the deep femoral artery patency was identified. All the materials were removed, and we completed the final step of the perclose Proglide â puncture closing. The patient was transferred to the room, being discharged from the hospital two days after the surgery with no complications, femoral, popliteal and podal pulses present bilaterally, taking Aspirin 100mg / day and Clopidogrel 75mg/day. After 1 month the patient was evaluated, presenting no further symptoms, no palpable mass in the right groin, and was submitted to a Duplex Ultrasound (Figure 5s 11 and 12), that showed deep femoral artery patency, stent patency, reduction of the aneurysm sac and no endoleaks. Furthermore, after one year follow-up, the patient remained assymptomatic, with Duplex Ultrasound showing deep femoral and stent patency and no endoleaks. (Figure 6).
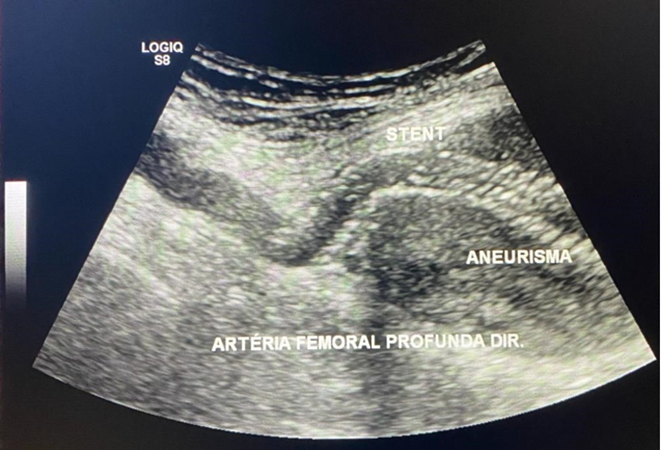
Figure 5: Duplex Ultrasound showing deep femoral artery patency, stent patency and no endoleaks at 1 month.
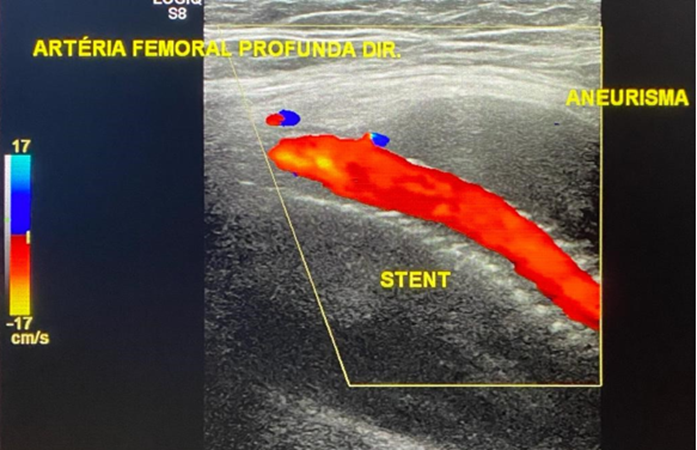
Figure 6: Duplex Ultrasound showing deep femoral artery patency, stent patency and no endoleaks at 1 year;
Discussion
Deep femoral artery aneurysm (DFAA) is a rare vascular disease, accounting for only 0.5% of all peripheral artery aneurysms. [7] It DFAA presents an incidence of only 1–2.6% of femoral artery aneurysms8 and most of cases occur in older men, caused by age-related atherosclerosis of the arterial wall. [9] Particularly in this present case report, the patient was under 50 years, had no associated comorbidities, except for occasional smoking and overweight, and the CTA showed no associatedconcomitant aneurysms in the arterial system, being even more rare this case in overall literature. One thing that we have observed in this present case was that the images in the arteriogram appeared to be consistent with an arteriomegaly presentation, since the common femoral and superficial femoral artery were unusually large. The arteriomegaly presentation could be an etiology. Another possible etiology should be atherosclerotic, since the patient was an occasional smoker and presented with overweight,
Deep femoral arteries aneurysms are difficult to diagnose, specially when the aneurysm is still small, reflecting in the incidence of asymptomatic cases and cases with nonspecific lower limb symptoms, such as pain, limb swelling and neurological symptoms.10 The most common finding of deep femoral artery aneurysm is a pulsatingve mass with or without pain, moreover these aneurysms can also be diagnosed as incidental findings in radiological exams. Likewise, in this present case, the patient was asymptomatic for years, and the deep femoral artery aneurysm was diagnosed when it had a 6cm diameter with 6cm and the main symptoms were right limb pain, mainly in the thigh, associated with a weakness and difficulty to walk in the past days.
Due to the difficulty for diagnosis, deep femoral artery aneurysms have higher risk of complication, such as thrombosis, distal embolization, and rupture.11 Different from femoropopliteal arterial aneurysms, rupture is the most common complication and presentation of DFAA with a risk ranging from 15 to 55%, presenting a direct relationship with aneurysm size. Moreover, DFA aneurysms generally have a larger diameter than those of the superficial femoral artery. [12] Furthermore, if the DFAA is associated with femoropopliteal occlusive disease, there is a high risk of major amputation, since the DFA is one of the most important artery related to lower limb vascularization and tissue nutrition. [13] The patient in this present case had no lower limb occlusive disease associated, and had the complete patency of the lower limb arteries, having no risk of amputation with the DFAA.
There has been described several forms of treating a DFAA, however there is a lack of data in literature regarding the best results and approach for this vascular disease. DFA can be revascularized with a bypass using a great
saphenous vein graft or vascular graft. However, surgical treatment can be more invasive. Ligature and resection of the aneurysm in isolation or combined with revascularization using synthetic or autologous grafts had also been described in overall literature. [7,8,9,10] Ligature is considered feasible, specially when distal pulses are present and there is no disease in femoroal-popliteal segment, however every effort should be made to achieve revascularization when the distal pulse is absent, since the DFA is an important artery providing collateral circulation to the legs. Endovascular treatment with covered stents had also been related, with good and safe results. [12] One of the limitations for endovascular treatment may be related to involvement of the aneurysm with the common femoral artery or absence of a large enough proximal landing zone to enable proper flow sealing. Fortunately, in this present case report, the patient had favorable anatomy for endovascular treatment, with satisfactory proximal neck length, diameter and proper proximal and distal landing zone for the covered stent. The choice for embolization of one of the larger branch of the DFA was to avoid immediate endoleak type II, which could interfere in adequate sealing zone of the covered stent, since it was a larger DFAA, with 6cm of diameter.
Covered stents can be either produced with Dacron or polytetrafluoroethylene (PTFE), and are used for the treatment of traumatic arterial lesions, arteriovenous fistulas, aneurysms, pseudoaneurysms, also for the treatment of obstructive vascular disease of the aortoiliac and femoropopliteal sectors. [13] The Solaris System is a covered stent with high flexibility designed for higher conformability. There are few cases in literature regarding the long-term outcomes of this covered system, since it is a new platform, however it`s electrospinning PTFE ultrathin membrane encapsulating a nitinol stent structure, which allows minimal shortening and instantaneous sealing during deployment associated with an accurate delivery system. [14] In a study of 1014 patients with isolated common femoral artery with or without deep femoral artery interventions, Siracuse et al15 reported that endovascular interventions have low periprocedural morbidity and mortality, are increasingly common, and should be studied for further application. Orchard et al 16 have also shown that endovascular embolization is effective and safe in the treatment of DFAA caused by physical injury.
This case report has some limitations, since it is a single case report, with no long-term follow-up. Larger studies should be performed in order to evaluate the safety and efficacy of endovascular treatment for DFFA.
Conclusion
DFFA are very rare among overall literature with very few and controversial options for proper therapy. DFA is crucial and important artery in thigh and leg tissues nutrition. Endovascular treatment with covered stents for this vascular disease is a safety and effective alternative for treating minimally invasive this condition, leading to and adequate flow sealing and proper aneurysm exclusion.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
The Authors declare that there is no conflict of interest regarding this paper.
Informed consent has been obtained from the patient for publication of the case report and accompanying images.
References
- femLevi N., Schroeder T.V (1997). Arteriosclerotic femoral artery aneurysms: a short review. J Cardiovasc Surg (Torino) 38:335–338.oral artery aneurysms: a short review. J Cardiovasc Surg (Torino) 38:335–338.
View at Publisher | View at Google Scholar - Dawson J., Fitridge R (2013). Update on aneurysm disease: current insights and controversies: peripheral aneurysms: when to intervene is rupture really a danger? Prog Cardiovasc Dis. 56:26–35.
View at Publisher | View at Google Scholar - Okugi S, Watanabe K, Kunii Y, Koide M (2020). Surgical and endovascular treatment of a bilateral deep femoral artery aneurysm. Interact Cardiovasc Thorac Surg. 30(6):945-946.
View at Publisher | View at Google Scholar - Posner SR, Wilensky J, Dimick J, Henke PK (2004). A true aneurysm of the profunda femoris artery: A case report and review of the English language literature. Ann Vasc Surg. 18(6):740-746.
View at Publisher | View at Google Scholar - Grillo VTRS, Jaldin RG, Sertório ND, et al (2021). True isolated deep femoral artery aneurysm associated with peripheral artery disease: case report. J Vasc Bras. 20: e20200220.
View at Publisher | View at Google Scholar - Fakhoury E., Oh K., Koudoumas D., Harris L.M., Dosluoglu H.H., Curl R (2019). Successful treatment of a ruptured profunda femoris artery aneurysm in association with fibromuscular dysplasia. J Vasc Surg Cases Innov Tech. 5:485–487.
View at Publisher | View at Google Scholar - Valiulis AP, Johnston KW (1980). Isolated arteriosclerotic aneurysm of the profunda femoris artery. J Cardiovasc Surg (Torino) 21: 498–500.
View at Publisher | View at Google Scholar - Dent TL, Lindenauer SM, Ernst CB, et al. (1972). Multiple arteriosclerotic arterial aneurysms. Arch Surg 105: 338–344.
View at Publisher | View at Google Scholar - Posner SR, Wilensky J, Dimick J, et al. (2004). A true aneurysm of the profunda femoris artery: a case report and review of the English language literature. Ann Vasc Surg 18: 740–746.
View at Publisher | View at Google Scholar - Jang LC, Park SS (2017). The true deep femoral artery aneurysm: a case report. Vasc Specialist Int. 33(1):40–42.
View at Publisher | View at Google Scholar - Ikeda H, Takeo M, Murakami T, Yamamoto M (2015). A case of deep femoral artery aneurysm. J Surg Case Rep. 2015(8): rjv111.
View at Publisher | View at Google Scholar - Lewszuk A, Madycki G (2019). Endovascular management of a giant true aneurysm of the deep femoral artery in a patient with a history of internal diseases. World J Surg Surg Res. 2:1–2.
View at Publisher | View at Google Scholar - Norbert EMS, Fidalgo-Domingos LA, Cenizo N, Revilla A, Taylor JH, Vaquero C (2020). Endovascular Treatment of Venous Bypass Graft Pseudoaneurysm with the New Solaris Self-Expanding Covered Stent. Case Rep Vasc Med. 2020: 4871814.
View at Publisher | View at Google Scholar - Ishii R. M., Guillaux C. H., Spósito R., Silveira A. C., Martinez Franco H. L., Folino F (2018). Solaris stent angioplasty: an alternative to endovascular treatment in the femoropopliteal territory. Vascular and Endovascular Surgery. 52: p. S12.
View at Publisher | View at Google Scholar - Siracuse J.J. Orden K.V. Kalish J.A. Eslami M.H. Schermerhorn M.L. Patel V.I.et al (2017). Endovascular treatment of the common femoral artery in the Vascular Quality Initiative. J Vasc Surg. 65: 1039-1046
View at Publisher | View at Google Scholar - Orchard P. Tan B.H. Abayasekara K (2013). Rupture of the profunda femoris artery in a patient with alcoholic liver disease: a case report. J Med Case Rep.7: 95-97.
View at Publisher | View at Google Scholar
