

Case report | DOI: https://doi.org/10.31579/2834-796X/086
Treadmill Testing- “Episodic Ischemia” in a middle aged woman aged 46 years
President of all Nations, MBBS, MD (General Medicine), D.M(Cardiology), FNB (interventional cardiology), ACCF (belongs to all Nations) Morning star hospital, Marthandam-629165, Kanyakumari District, Indias.
*Corresponding Author: Ramachandran Muthiah, President of all Nations, MBBS, MD (General Medicine), D.M(Cardiology),FNB (interventional cardiology), ACCF (belongs to all Nations) Morning star hospital, Marthandam-629165, Kanyakumari District, Indias.
Citation: Ramachandran Muthiah (2025), Treadmill Testing- “Episodic Ischemia” in a middle aged woman aged 46 years, International Journal of Cardiovascular Medicine, 4(1); DOI:10.31579/2834-796X/086
Copyright: © 2025, Ramachandran Muthiah. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 November 2024 | Accepted: 18 December 2024 | Published: 13 January 2025
Keywords: congenital coronary anomaly; treadmill testing; episodic ischemia; angiographic imaging
Abstract
The treadmill ECG stress test is commonly used as a screening test to identify myocardial ischaemia. During exercise, the physiological increase in heart rate is due to a decrease in vagal tone followed by an increase in sympathetic tone and the sufficient effort during treadmill ECG stress testing is defined as achieving 85% of the age-predicted maximal heart rate. The increase in sympathetic tone and vasodilation during exercise generally causes a rise in blood pressure. An exaggerated blood pressure response, defined as a peak systolic blood pressure of > 210 mmHg in men and > 190 mmHg in women was shown to predict the risk of hypertension in normotensive individuals, A drop in systolic blood pressure > 10 mmHg is an indication to terminate the treadmill ECG stress tests, as it could be due to myocardial ischaemia leading to left ventricular dysfunction. In addition to the evaluation of CAD, the treadmill ECG stress test is also often used to evaluate for chronotropic incompetency, in which the patient is unable to mount an adequate heart rate response to exercise, leading to symptoms such as effort-related dyspnoea and lethargy.The Bruce protocol is the most commonly used and it consists of a total of seven stages, with a gradual increment in the speed and gradient of the treadmill. Each stage lasts three minutes to allow the patient to acclimatise to the specific speed and gradient before advancing to the next stage. The MET value increases as the patient advances to higher stages of the Bruce protocol. Exercise intensity during the treadmill ECG stress test is calculated in METs, which reflect the amount of oxygen consumed per minute. 1 MET is equal to 3.5 mL/min/kg of oxygen used. Continuous ECG monitoring is carried out throughout the test and into the recovery period to assess for any changes in the ST segments due to limitation of coronary blood flow may lead to myocardial ischaemia, as well as for arrhythmia. The test is often stopped before completing Stage 7, when the patient achieves the target heart rate or is symptomatic, or when the test is positive.The duration of ST-segment depression is also important, as prolonged recovery after peak stress is consistent with a positive treadmill ECG stress test. Another finding that is highly indicative of significant CAD is the occurrence of ST-segment elevation > 1 mm (often suggesting transmural ischemia) and these patients are frequently referred urgently for coronary angiography.
A 46-year-old female developed anginal episodes during treadmill testing and further evaluation revealed a congenutal coronary anomaly.
Introduction
In normal condition, maintaining the normal coronary artery diameter is critical for myocardial perfusion and it changes continuously to maintain adequate oxygen delivery to the myocardial tissue. Coronary flow reserve defined as the ratio between blood flow at the maximum coronary vasodilation and is higher than 4 at normal condition. In patients with classic angina pectoris, diameter narrowing due to atherosclerosis results in significant reduction of coronary flow reserve. Thus, at resting status, sufficient myocardial perfusion may be possible; however, during exercise or emotional stress requiring adequate increase of cardiac output and myocardial oxygen demand, progressive coronary vasodilatation is limited due to fixed stenosis, resulting in development of myocardial ischemia or chest pain. Myocardial oxygen demand usually parallels with heart rate and the chest pain development due to classic angina pectoris usually aggregates in the daytime coinciding with the changes of the heart rate [1].
Coronary artery vasospasm (CVS) is a transient and reversible vasoconstriction of the major epicardial coronary artery evoking myocardial ischemia and the development of chest pain, is not associated or parallel with increase of myocardial oxygen demand. Accordingly, variant angina is characterized by its circadian variation of development of chest pain or myocardial ischemia and there is no association with the heart rate. But the angina threshold in variant angina shows a typical diurnal variant with significantly lower level during nocturnal time or sleep when the heart rate usually shows lower level. Although resting chest pain is the usual clinical presentation of variant angina, in some cases, development of chest pain is associated with minimal effort such as walking in the morning; do not develop chest pain with more demanding exercise such as running in the daytime. This discrepancy between work loading and angina development represents typical diurnal or circadian variation of angina threshold in variant angina.
Episodes of myocardial ischemia during ambulatory activity in patients with stable coronary artery disease exhibits a marked circadian pattern, with the peak number of events occurring in the first few hours after awakening [2-4] and the majority of ischemic episodes are preceded by a heart rate increase [5] Up to 20–30% of patients with angina-like chest pain have no flow-limiting epicardial coronary stenosis or spasm [6],[7], often defined as cardiac syndrome X [8] or microvascular angina [9], in which coronary microvascular dysfunction occurs due to an inadequate coronary vasodilator capacity and/or enhanced coronary vasoconstrictor responses [10]. and can be detected by pacing-induced myocardial lactate production [11] or regional myocardial perfusion defects on single photon emission computed tomography or PET imaging [12],[13].The underlying mechanism of microvascular angina, suggests the involvement of blunted NO-dependent microvascular dilatation[14]. impaired EDHF(endothelium-derived hyperpolarizing factor) response, increased plasma levels of endothelin-1 (ET-1) and enhanced Rho-kinase activity as Rho-kinase has been identified as one of the effectors of the small GTP-binding protein Rho. Activated Rho-kinase down-regulates endothelial NO synthase, causing endothelial dysfunction [15]. and VSMC (vascular smooth muscle cells) hypercontractions.
Primary congenital coronary anomalies varies from 0.3% in necropsy series reported by Alexander and Griffith to 1.6% of patients undergoing cardiac catheterisation [16]. Clinical suspicion of coronary anomalies remains an important challenge and often discovered as an incidental finding during cardiac assessment and their clinical significance varies greatly across different variants [17]. Most of these anomalies are of little clinical significance during childhood and may become important in adolescence and young adult life when extremes of physical exertion may cause significant intolerance of the previously well tolerated malfunction [18] and so this case has been reported.
2. Case Report
A 46 years old female medical practitioner was rushed to the emergency department with sudden onset of chest discomfort while she was climbing the staircases in a shopping complex. She is diabetic (sugar status under control), not hypertensive and previously asymptomatic. Clinically, she is anxious and her heart rate is initially 110 bpm and later became normal. Blood pressure was in the normal range and ECG, X-Ray chest were normal. Echocardiography revealed no associated cardiac defects. She was symptom free shortly without any medications. She was admitted in the intensive care unit for observation and thereafter no further episodes of chest discomfort. Holter monitoring was normal. Blood chemistry including Thyroid function tests revealed no abnormalities. After 48 hrs observation, she was subjected to Treadmill exercise test which is as follows
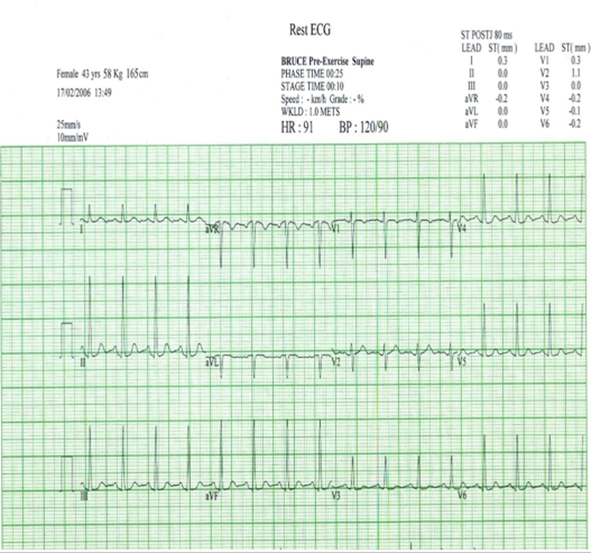
(Rest ECG showing no ST-T changes)
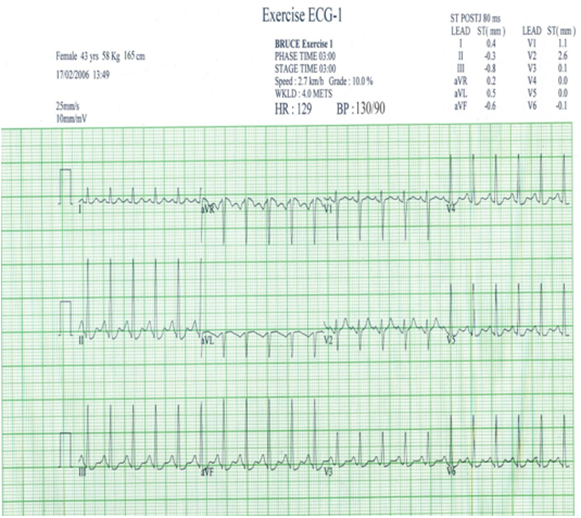
(Exercise ECG- Stage 1 showing 1 mm junctional ST depression in inferior leads (L II, III, aVF) and precordial leads - V4 to V6 according to increase in heart rate)
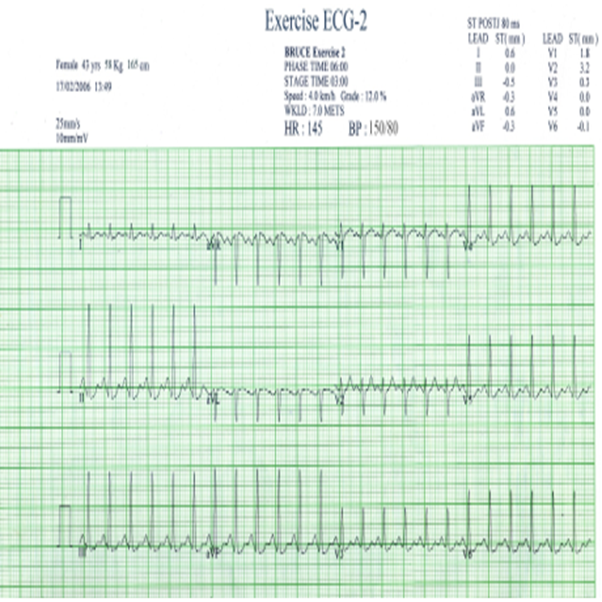
(Exercise ECG stage 2 showing the junctional ST depression becoming “upsloping” in inferior and precordial leads according to progressive increase in heart rate)
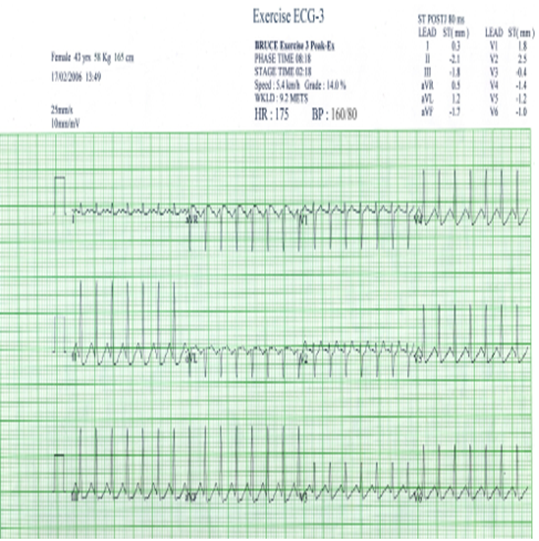
(Exercise ECG- Stage 3 at peak exercise showing the junctional (J point) ST depression becoming “rapid upsloping” in inferior and precordial leads) [19] suggesting “episodic ischemia” due to increase in heart rate.)
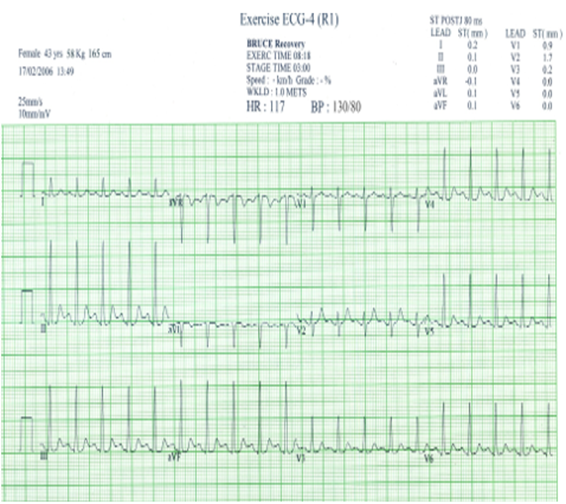
(Exercise ECG in Recovery stage 1 showing the rapid normalisation of ST segment in inferior and precordial leads)

(Exercise ECG in Recovery stage 2 is becoming similar to Rest ECG)
She has achieved 9.2 METS in Bruce protocol stage 3 at peak exercise and developed chest discomfort with sweating and the test was stopped. The ECG in stage 3 at peak exercise revealed junctional ST depression with rapid up
sloping of ST segment which immediately returns to normal as shown in ECG 4 R1, R2 in the recovery period suggesting the exercise induced “episodic ischemia”. she was advised cardiac CT angiography as a screening test which is shown in Figure 1
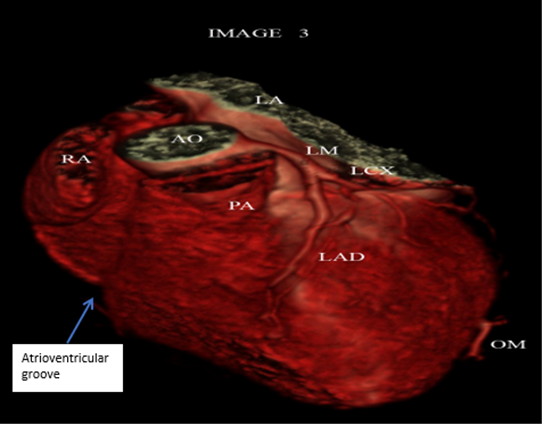
(Figure 1 showing no anomalous vessel between aorta and pulmonary artery). Blue arrow shows no vessel in the right atrioventricular groove.
The CT images , Figure 1 shows “ Right coronary artery is not visualized in the Right AV groove” and no anomalous vessel is passing either anterior to the pulmonary artery or in between pulmonary artery and aorta.
Cardiac MR angiography which is shown in figures 2 revealed non visualization of the clear cut origin of Right coronary artery from the aortic root and trifurcation of left coronary artery (Figure 3).
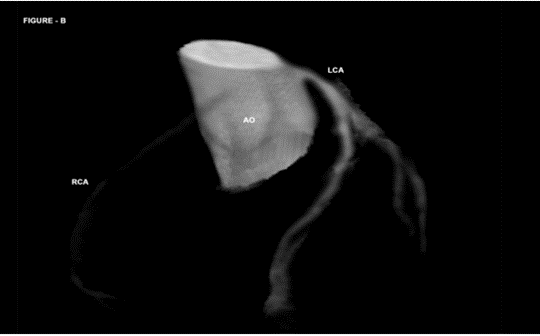
(Figure 2 shows the impression of Right coronary artery with no clear cut lumen and origin from the aortic root)
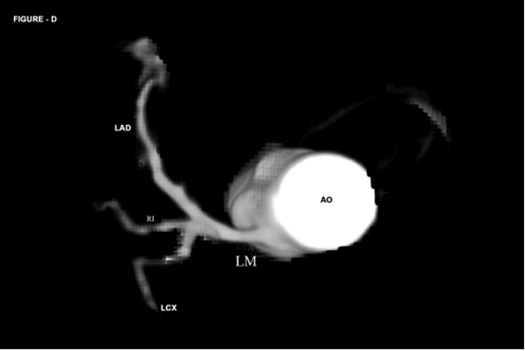
(Figure 3 shows the Left main trifurcates into LAD (left anterior descending artery), RI (ramus intermedius) and LCX (left circumflex coronary artery)
Then, she was advised to invasive coronary angiography as shown in Figures 4 to 8.
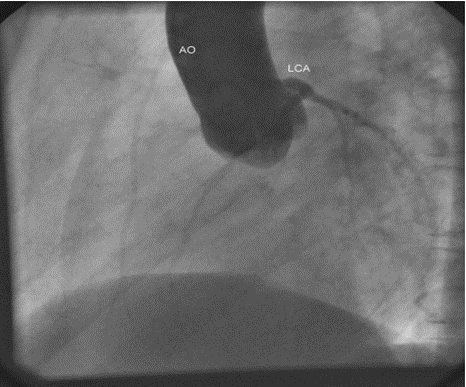
Figure 4 shows aortic root angiogram which revealed non visualization of the origin of Right coronary artery from the aortic root.in LAO cranial view.
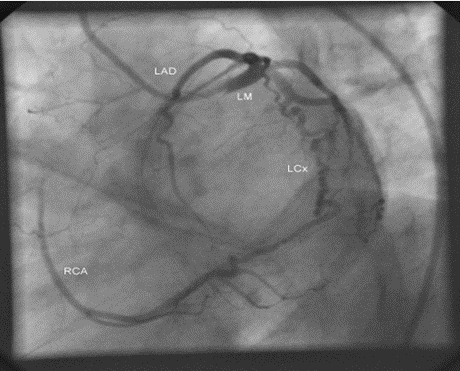
(Figure 5 shows LCx (left circumflex coronary artery) is continuing to form the Right coronary artery (RCA) in “spider view” (LAO caudal)).
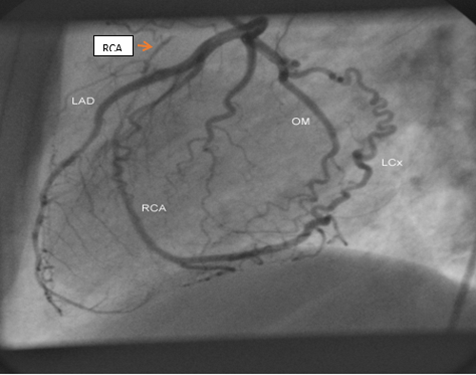
Figure 6 showing the Type III LAD (left anterior descending artery wraps around the cardiac apex into the posterior interventricular groove and LCx (left circumflex coronary artery (tortuous vessel) is continuing to form the RCA (right coronary artery). Red arrow shows the “Proximal RCA” in left lateral view.
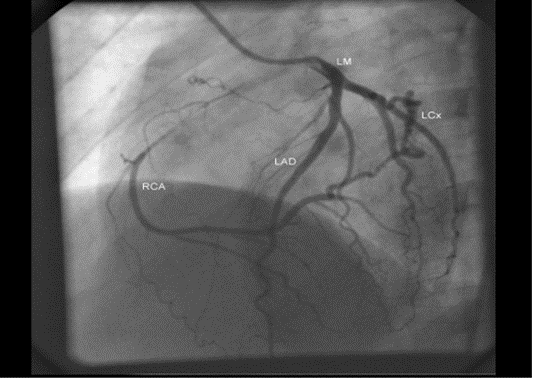
Figure 7 shows the LCx (left circumflex coronary artery is continuing as Right coronary artery) in LAO cranial view.
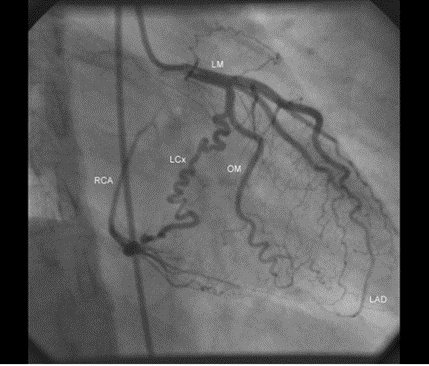
Figure 8 showing the tortuous left circumflex coronary artery (LCx) in RAO caudal view.
The Figures 4 to 8 revealed “Left circumflex coronary artery is continuing to form the Right coronary artery”, a rarest coronary anomaly [20], [21]. The Runs of the coronary angiogram revealed retrograde filling of Right coronary artery as a continuous flow from Left circumflex and there is a delayed filling in the proximal portion of the Right coronary artery.
3. Discussion
1. Review of literature
Angelini et al. described a wide range of anatomical variants [22],[23] and the first classification of CAAs (coronary artery anomalies) is\ was proposed by Ogden in 1969 as three categories: as minor , major and secondary anomalies [24]..According to Angelini, the following characteristics are considered as normal [25-28] as shown in Table 1:
| S.No. | Normal variants |
1. 2. 3. 4. 5. |
two to four ostia, in the right and left coronary sinuses proximal orientation of 45° to 90° from the aortic wall a common trunk, located on the left, giving rise to the left anterior descending artery and circumflex artery a middle subepicardial segment, with branches appropriate for the dependent myocardium termination of the entire system in a capillary network |
Table 1: Normal anatomical variants of coronaries
In 2000, Dodge-Khatami et al. introduced a new system of nomenclature used to record anomalous aortic origin of a coronary artery in order to develop guidelines for its treatment and monitoring [29]. In 2003, a new classification emerged, proposed by Rigatelli et al., groups into seven categories [30] as shown in Table 2.
| S,No | Categories |
1. 2. 3. 4. 5. 6. 7 | Hypoplasia / atresia a single coronary artery (hyperdominance) fistula originating from other arteries originating from the wrong coronary sinus splitting (separate origins from the left anterior descending artery and circumflex artery) tunneling |
Table 2. Rigatelli classification of anomalous coronaries
In 1962, an anomalous left coronary artery originating from right coronary sinus was described in a healthy boy found dead after a cross-country race. Later, in 1974, Cheitlin et al. demonstrated that several autopsied patients with anomalous origin of coronary arteries from the opposite sinus had experienced sudden death [31]. Brothers et al. presented the first case series of families with an interarterial course in the pediatric population [32]
2. Etiopathogenesis
During fetal development, vascular sinusoids develop within the embryonic myocardium and when it becomes more compact, the sinusoids disappear and a network of veins, arteries and capillaries develops. These vessels connect with other mediastinal vessels at approximately 32 days of gestation. The primitive coronary vessels appear around the seventh week of gestation, after the formation of the aorta from the division of truncus arteriosus.. As the coronary artery network develops, endothelial buds appear at the base of the truncus arteriosus and later join with the coronary artery network, which develops from the sinusoids and establishing the definitive coronary artery circulation [33],[34]..
Embryologically, the subepicardial vessels derive from extracardiac epicardial cells, which form a plexus like vasculature, invading the myocardium and growing towards the aortic root to the facing aortic sinuses. At the time of spongy myocardium, intramural blood supply directly from the ventricular cavities through the intertrabecular spaces lined by the endocardium, whereas later, at the time of myocardial compaction, vascularization originates from the subepicardial network. The connection of the subepicardial plexus with the aorta occurs with prongs of the peritruncal ring which penetrate the facing aortic sinuses and the septation of truncus arteriosus is not responsible for the final position of the coronary orifices. “Peritruncal ring” is a subepicardial network of cells (“bioepicardial organ”) surrounds the orifices of the great arteries and eventually connects with the facing aortic sinuses.
In “outgrowth hypothesis”, the development of sprouts or buds from the aortic wall of facing sinuses, capturing the peritruncal ring of coronary subepicardial arterial vasculature [35],[36]. The “ingrowth hypothesis” is supported by the observation that the prongs of the peritruncal ring penetrate the aortic wall and make contact with the endothelial lining of the aorta [37].[38]. Recent investigations confirmed that the proximal coronary arteries do not grow from the aorta and they grow into the aorta from the peritruncal ring of the subepicardial vascular plexus [39]. Formation of the left coronary artery precedes the right coronary artery and different from the tunica media of the ascending aorta as the tunica media of the coronary arteries does not derive from the neural crest.
Cellular cross talks and signaling pathways such as notch and hippo signals, transcription factors, angiogenic molecules, and apoptosis take place [40-44] and VEGF plays a crucial role in the development of coronary ostia and main stem formation [45] . Absence of VEGF was shown to inhibit ostia formation. Epicardial inhibition, reducing apoptotic remodeling at the ventricular–arterial junction, alters vascular connection with the aorta and may produce coronary artery anomalies observed in humans [46]
Molecular hypothesis
Analysis of signalling molecules and transcription factors pivotal to CA (coronary artery) embryogenesis have been recently proposed. Wt1 (Wilms tumour suppressor gene)-dependent disruption of retinoic acid synthesis in the epicardium directly or indirectly down-regulates the expression of Pdgf receptors α,β in EPDCs (epicardial-derived cells) [47], interfering with coronary smooth muscle progenitor cell differentiation.The Notch/Delta cell-to-cell signalling pathway promote arterial endothelium during coronary blood vessel development[48],[49]. Down-regulation of the nuclear transcription factor Coup-tf II (COUP transcription factor 2), a Notch repressor [50] and up-regulation of Ephrinb2 expression in CA progenitor cells also correlate with CA endothelial specification. Myocardium-secreted Fgfs and Vegf participate in the regulation of coronary endothelial cell and vascular assembly [51] and Vegf (Vascular endothelial growth factor) has been reported to be dependent on myocardial Fgf (fibroblast growth dactor) -induced Hedgehog activity [52]. Coronary morphogenesis is linked to the growth and compaction of the ventricular walls since hypoxic gradients in the ventricular walls activate myocardial Vegf and promote endocardial sprouting in CA development[53]. Cell membrane-bound Ephrins [54] and Semaphorins [55] provide attractive cues to the developing coronary endothelium, thus patterning its growth over the myocardium.
The aortic root is important in defining the connections of the LCA and RCA stems to the proper coronary Valsalva sinuses of the aorta. Interestingly, the CXCL12/CXCR4 signalling axis has been recently implicated in proximal CA connection with the aortic endothelium[56]. Developmentally, the ‘proximal’ aorta and the ‘distal’ cardiac chamber coronary vascular plexus are two distinct elements and any genetic factor preventing the correct assembly of these two elements is likely to result in CA anomalous connection. The specific location of the aortic root in the cardiac base, ultimately determines the path followed by coronary stems with respect to the aortic and pulmonary roots, the proximity of the coronary sinuses to the anterior interventricular and atrioventricular grooves probably contributing to the specific location of the two main coronary stems [57]. The formation of the main CA tracts correlates with the areas where the epicardium and associated subepicardial matrix first form [58] which is consistent with the subepicardial association of cardiac fat and CAs (coronary anomalies), that partially, originate from the embryonic epicardium [59].
Episodic myocardial ischemia
Intramural course of the coronary arteries [60],[61] is considered a variant of normal when covered by a myocardial bridge. and may be the cause of myocardial ischemia if completely surrounded by a sleeve of the myocardium with disarray and an intramyocardial course at least 2.5 cm long and 0.5 cm deep has been documented [62]. In young people, under 35 years of age, the major objective is sudden death and in those over 35 years of age is myocardial ischemia. Exercise-induced ischaemia has been attributed to tachycardia (episodic) due to increase in myocardial oxygen requirement and a reduction in the diastolic coronary flow [63] and the mechanisms that produce ischemia in CAAs are shown in Table 3.
| 1. | Angulation of the anomalous artery | In contrast to a normal coronary artery, which is perpendicular to the aorta at its origin, the anomalous coronary artery may bend over itself to reach. Because of this, the ostium of the anomalous coronary artery would be smaller, with valve-like ridges, as compared to the normal circular ostium, and could become compressed in the case of a marked expansion of the aorta, such as that observed during strenuous exercise[64] |
| 2. | Initial course of the CAA. | (a)interarterial, between the aorta and pulmonary artery, the increase in the pressure in the 2 vessels, occurring during exertion, would produce a compression of the anomalous coronary artery [65]. (b) intramural, the obstruction may be enhanced since the coronary artery can become deformed within the aortic wall during periods of hypertension[66] |
| 3. | Spasm in the anomalous coronary artery | as a result of endothelial damage produced by the anomalous pathway [67] |
| 4. | Intussusception | the proximal portion of the CAA in the aortic wall [68]. |
Table 3. Mechanisms that produce ischemia in CAAs
Microvascular Angina
The endothelial monolayer can administer the exchange of fluids and metabolites and, furthermore, can manage vascular hemostasis. In case of a raised myocardial metabolic request, the coronary microvasculature
modulates the peripheral vascular resistance and administrates the blood flow distribution that can reach a fivefold increase in healthy subjects.
The coronary microcirculation is an adaptive system that regulates myocardial perfusion [69], the epicardial coronaries (diameter > 400 μm) act as transport vessels, and the pre-arterioles and arterioles mainly determine the resistance. The autoregulation of this resistance makes it possible to maintain a constant blood flow over a wide range of coronary perfusion pressures, delivering oxygen and nutrients to the tissues and removing waste products. Several mechanisms play a role in this autoregulation, namely: myogenic regulation by the vascular smooth muscle cells, metabolic control by metabolites from adjacent myocardial cells, endothelial function responsive to changes in vascular wall tension, autonomic innervation, and circulating hormones including endothelium dependent relaxation factors such as nitric oxide (NO) and prostaglandins [70] and vasoconstrictor agents such as histamine, norepinephrine, and serotonin [71].
Coronary vascular dysfunction can be caused by functional (endothelial & non-endothelial)[72] and structural abnormalities. Endothelial function can be evaluated by the response of the coronary arteries to acetylcholine. If coronary vasodilation occurs after administration of acetylcholine, reflects a well-functioning endothelium and if vasoconstriction occurs, it indicates endothelial dysfunction, which is often found in the early phase of atherosclerosis [73]. Non-endothelial mediated functional abnormalities are related to decreased diastolic time, increased intramyocardial and intracavitary pressures, and/or tissue edema. Structural abnormalities include microvascular remodeling in arterioles (intimal thickening, smooth muscle cell proliferation and perivascular fibrosis) and decreased capillary density resulting in increased microvascular resistance, seen in left ventricular hypertrophy, calcium surplus and amyloidosis. The non-endothelial mediated functional and/or structural abnormalities of the coronary microcirculation can be assessed by CFR and microvascular resistance measurements.
Camici and Crea defined CMD (coronary microvascular dysfunction) as four types [74],[75] as shown in Table 4
| Type (CMD) | Definition |
1.
2.
3.
4. | in the absence of obstructive CAD and myocardial diseases
associates with cardiomyopathy
occurs in the presence of obstructive CAD
iatrogenic.
|
(Table 4- Types of CMD)
The two primary NPs (Natriuretic peptides) are the atrial natriuretic peptide (ANP), released when atrial wall stretching occurs, and the brain natriuretic peptide (BNP), secreted by ventricular myocytes in case of volume overload. Furthermore, the N-terminal prohormone of BNP (NT-proBNP) has an established role and clinical use as a biomarker. Both NPs control fluid homeostasis, natriuresis and express dose-dependent vasoactive effects. ANP is essential for endothelial homeostasis through autocrine and paracrine secretion. Patients presenting both CMD and left ventricle (LV) diastolic dysfunction showed increased levels of plasma NT-proBNP compared to healthy subjects.The association of low CFR and high Tn (Troponin) levels was related to an increased incidence of major adverse cardiovascular events (MACEs)
Microvascular angina (MVA) due to CMD is difficult to distinguish from classic angina due to obstructive CAD because both are often exercise-related. MVA is more likely if the angina continues after exercise cessation, starts after exercise and/or has limited response to nitroglycerin administration and more often triggered by palpitations or mental stress [76]. The intensity of symptoms can vary over time and can be so severe that patients are limited in daily life activities. Angina at rest often occur in addition to exercise-related complaints [77] due to a vasospastic component of coronary vascular dysfunction [78]. Pure vasospastic (Prinzmetal) angina usually occurs at rest, mainly at night and/or early morning, however, exercise-related symptoms can also be due to vasospasm[79],[80].
The gold standard to diagnose coronary vascular dysfunction is an invasive coronary vasomotor test that can comprehensively test all 4 endotypes of coronary vascular function: epicardial and microvascular coronary vasospasms, vasodilatory capacity and microvascular resistance. Coronary vascular dysfunction (Coronary Vasomotor Disorders (COVADIS)) causes a heterogeneous pattern of non-transmural ischemia, which is not visible as a regional perfusion defect [81]. During a CAG (coronary angiography), obstructive CAD is ruled out, after which vasomotor tests are performed. To evaluate coronary vasospasm, ascending doses (usually 2, 20, 100, and 200 μg) of acetylcholine are given in the left coronary artery with continuous monitoring of symptoms and 12-channel ECG. An alternative to acetylcholine is ergonovine, but it is less effective, especially in women [82].The acetylcholine test is positive for epicardial spasms if recognizable symptoms occur, accompanied by ischemic ECG changes and a ≥ 90% reduction of the coronary lumen. The acetylcholine test ends with the administration of nitroglycerin to ensure that there is complete vasorelaxation of the coronaries and that the patient is free of complaints.
Using systemic infusion of adenosine, the coronary flow reserve (CFR) is determined, This can be done by means of thermodilution or Doppler [83]. An invasively measured CFR < 2> 2.5 is considered normal. CFR values between 2 and 2.5 form a gray area.
If thermodilution is used, the index of microvascular resistance (IMR) is determined and the evaluation is done with Doppler to determine the hyperemic microvascular resistance (HMR)[86]. IMR of 25 U is generally used as cut-off, with values above 25 being diagnostic for CMD. For HMR, 2.5 mmHg/cm/s is often used as a cut-off value for the diagnosis of microvascular disease[87]..
In patients with acute myocardial infarction, coronary microvascular dysfunction is responsible for the so-called ‘no-reflow’’ phenomenon, which is associated with a worse outcome. Therefore, it is recommended that all patients undergoing an invasive test, a complete coronary vasomotor test with administration of both acetylcholine and adenosine should be performed.
PET, CMR and TTDE have been considered) for the detection of coronary vascular dysfunction [88]. With TransThoracic Doppler Echocardiography (TTDE), the Coronary Flow Velocity Reserve (CFVR) can be determined in the Left Anterior Descending coronary (LAD). The CFVR is the ratio of the peak velocity in hyperemia (using systemic adenosine) vs the peak velocity in rest in the LAD and a surrogate for CFR. In CMR (Cardiac magnetic resonance), a technique has been developed to determine the Myocardial Perfusion Reserve Index (MPRI) by using a contrast medium (gadolinium), diffusing from the microvasculature into the interstitial space, perfusion signal intensity upslopes are evaluated in stress (induced with adenosine) vs. rest, the ratio being the MPRI, which is considered a surrogate for the CFR[89]. CMR is more widely available than PET, less expensive and involves no radiation Cardiac Positron Emission Tomography (PET), a radionuclide imaging technique, is considered the most reliable method using 15O-water, 13N-ammonia, or 82rubidium tracers [90] for accurate and reproducible quantification of regional myocardial blood flow (MBF) and CFR in the myocardium[91].[92] and correlates well with invasive assessment of CFR[93]. Despite, PET is not widely used due to some major limitations, namely, high expense, the necessity of an on-site cyclotron when using 15O-water and 13N-ammonia, and the involvement of radiation [94-96]. However, the described methods only assess CFR and the cold-pressor PET which cannot distinguish between epicardial and microvascular vasospasm. Vasospasm is the most prevalent endotype in patients with coronary vascular dysfunction, occurring in 81–97% of patients, while an abnormal CFR or microvascular resistance without vasospasms occurred in only 3–19% [97],[98].
Recently, a novel method has been validated that allows this direct quantification of absolute coronary blood flow (Q) and resistance (R) using continuous thermodilution [99-101].
Sudden cardiac death (SCD)
The anomalous coronary artery arising from the opposite sinus is related to 14–17% of all cardiac deaths among young athletes during or immediately after physical exercise [102], mostly between the ages of 10 and 30 [103].Sudden cardiac death in older individuals is less common due to lower rate of participation in high-intensity sports [104] and is normally associated with atherosclerotic events. Sudden death has major social impact as the result of high number of years of life potentially lost [105]. The anomalous origin of left coronary artery seems to be responsible for up to 85% of cases of sudden cardiac death, which makes it more fatal. Occlusion of the left coronary artery results in a massive anterolateral and septal ischemia, followed by tachycardia/ventricular fibrillation or extensive myocardial infarction and cardiogenic shock. If the occlusion is in the proximal region of the right coronary artery, the resulting infarction occurs in the inferior region of the myocardium and is usually not fatal [106]. Transient ischemia with anomalous coronary arteries, leads to malignant arrhythmias causing SCD. The proposed mechanisms of ischemia induced SCD [107] are shown in Table 5
| S.No | Mechanisms |
1. 2. 3. 4. | acute angulation at the ostium of coronary artery and kinking an abnormal slit-like opening; mechanical compression of the anomalous artery during exertion vasospasm of the anomalous artery |
Table 5. The mechanisms of sudden cardiac death in coronary anomalies.
Single Coronary Artery (SCA)
This is a very rare condition, occuring in approximately 0.024% of the population in which only one CA (coronary artery) arises from the aorta and may originate either from the left or the right Valsalva sinus and can coexist with other congenital anomalies. Endothelial hyperfusion can result in the reduction of coronary blood vessels and failure of one of the two CAs (coronary arteries) to muscularize, can be a factor explaining the absence of a major coronary vessel. It may take the course of either an RCA (right coronary artery) or an LCA (left coronary artery) as in Figure 4 and divide shortly from its origin into two or three of the main coronary branches as in Figure 3. Lipton et al.[108] proposed an anatomical classification of single CA, shown in Table 6 based on the location of the ostium, anatomical distribution, and course.
| Originating from right cusp | Description | Originating from left cusp |
| RI | Solitary vessel arising from either the left or right coronary cusp, following the course of either a normal right or left coronary artery | LI |
| RIIA | Divided into 3 types depending on the relationship of the aberrant vessel to the great vessels. Type A courses anterior to the pulmonary trunk. Type B travels between the aorta and pulmonary trunk. Type P travels posterior to the aorta | LIIA |
| RIIIB | LIIB | |
| RIIP | LIIP | |
| RIII | Absent left coronary artery with the left anterior descending and circumflex arteries arising from the common trunk originating from right coronary cusp |
Table 6. Lipton's classification of single coronary artery
(Alphabets R or L are used to identify the ostial origin of the vessel, roman numerals I, II, or III are used to represent the anatomical distribution of the vessel, and letters A, B, P, S, and C are used to delineate the course of the vessel with respect to the pulmonary artery and the aorta)
Although single CA may be compatible with a normal life expectancy due to the development of collateral branches, patients are at increased risk of myocardial ischemia and SCD when a major CA branch courses between the pulmonary artery and the aorta [109], especially when the single CA originates from the right sinus. A rare case of isolated SCA with absent RCA, with LCX (left circumflex coronary artery), a large vessel which supplied also the territory of the right coronary artery (RCA) through its terminal extension, presented with unstable angina in a 56-year-old female was reported [110]. Taylor et al. Analysed 242 deceased patients with isolated congenital coronary anomalies and found that one-third of the patients suffered sudden cardiac death, and half of these were exercise-related deaths [111]. The features like acute take-off angle of the anomalous vessel, slit-like orifice, and proximal intramural course, are characteristics that can predispose to anginal symptoms and sudden death during exertion [112].
Myocardial bridges
A myocardial bridge is defined as an atypical course of a coronary artery intramyocardially, which may result in compression of the vessel during systole (milking effect) and usually seen in the proximal and mid-segment of the LAD (left anterior descending artery). It may lead to ischemia, when characterized by a deeper (5 mm) and longer (2–3 cm) intramyocardial course, with the myocardium encircling the intramural segment acting like a sphincter [113],[114]. Myocardial bridging occurs frequently in patients with hypertrophic cardiomyopathy, with a prevalence as high as 30% [115],[116]. The major challenge is the functional assessment as it is the incidental finding of angiography or CT imaging [117] since it constitutes an anomaly or a normal variant, according to its frequency in the general population in imaging or autopsy studies [118]. Stress single-photon emission CT can detect reversible myocardial perfusion defects in those patients, with a correlation between the amount of ischemia and degree of systolic luminal narrowing. 256-slice CT contrast-enhanced coronary angiography, a Curve multiplanar reconstruction imaging may show an intramyocardial course and shifting into myocardium of middle LAD with a typical “step down-step up” phenomenon[119]. Coronary physiological measurements during pharmacological infusion are also helpful. A Characteristic flow pattern in the bridged segment can be demonstrated by intracoronary Doppler imaging as a steep rise in the flow velocity at early diastole is followed by a sharp deceleration and subsequent plateau (“fingertip’ phenomenon”) [120]. Imaging by IVUS (intravascular ultrasound) can reveal the characteristic “half-moon” sign, an echolucent area between the bridged coronary segment and epicardial tissue that persists throughout the cardiac cycle [121].
Hypoplastic coronary artery
Hypoplastic coronary artery was first reported in 1970 and refers to congenital underdevelopment of one or more major branches with greatly decreased luminal diameter or length.[122],[123]. Ogden et al found an incidence of 0.022% of hypoplastic proximal coronary artery as in Figure 2 in a study of 224 necropsy cases of congenital coronary artery anomalies.[124]. In living patients, the diagnosis is made by coronary angiography and in a recent analysis of 58,023 coronary angiographies performed in adult patients, coronary artery anomalies were diagnosed in 257 patients (0.44%) with congenital atresia in only 16 patients (atretic RCA in two patients; atretic left circumflex in 14) [125].
A right rudimentary coronary artery has been first described by Walter B.Whiting in 1937 [126]. The term hypoplastic right coronary artery is used in case of a short course that does not reach the crux cordis, a further feature is a narrow vessel lumen [127] and can be an incidental finding on invasive coronary angiography, cardiac CT or cardiac MRI and there have been reports of arrhythmias, myocardial ischemia, syncope or sudden cardiac death as an initial presentation [128].
Therapeutic Aspects
1.Medical therapy
Administration of Nitrates accentuate the degree of systolic narrowing in myocardial bridges and should be avoided because they may worsen the symptoms.
Logically, β blockers are advisable to control tachycardia related ischemia due to myocardial bridges on exertion, recommended in patients with predominantly exercise-related complaints and may be given on close follow up if there is any further episodes of chest discomfort occurs in this patient [129].[130] Nearly all ischemic episodes occurring in the morning and early afternoon are associated with increases in heart rate [131] and, presumably, are related to increases in myocardial oxygen demand [132]. Consequently, β-adrenergic receptor blockade with nadolol was extremely effective in preventing the morning increase in ambulatory ischemia. By contrast, nadolol therapy was actually associated with an increase in the number of ischemic episodes not associated with an increase in heart rate [133]. This increase in presumably supply-mediated episodes, which may be due in part to episodic coronary vasoconstriction, occurred primarily in the late afternoon and nighttime, suggesting that nadolol therapy may have had deleterious effects on myocardial oxygen supply during that period [134].
First-line therapy consists of a non- dihydropyridine calcium channel blocker and a short-acting nitrate to stop vasospasm episodes [135] and if insufficient, a long-acting nitrate can be added [136]. Nicorandil is an effective agent for epicardial spasms and can be added if symptoms are insufficiently controlled [137]. Nicorandil often works better than other long-acting nitrates because, in addition to its effect on nitric oxide production, it has a beneficial effect on the smooth muscle cells around the vessel wall [138]. Non-selective β-blockers, such as propranolol, should be avoided if there is suspected coronary artery spasm, as they can trigger spasm [139],[140], however, nebivolol (a selective β-1 receptor blocker, but also has vasodilatory effects through NO production) was shown to reduce coronary vasospasm [141], [142] although not as effective as diltiazem[143]. Atenolol improves exercise capacity and anginal symptoms [144]. Carvedilol and labetalol (β-blockers with both alpha-1 and β-adrenergic receptor antagonist properties) are also recommended for CMD due to their vasodilatory effect [145]. Calcium channel blockers are recommended because they have been shown to be effective in both epicardial spasms and CMD[146],[147]. Both non-dihydropiridines (e.g., diltiazem) and dihydropiridines (e.g., nifedipine retard) calcium antagonists can be given
Ranolazine is a sodium channel blocker that reduces intracellular calcium in cardiomyocytes leading to improved intraventricular relaxation and microcirculation. A recent randomized trial in 81 patients showed that ranolazine improves symptoms and myocardial perfusion in patients with a CFR < 2>
Novel drugs are promising, the ‘Rho kinase inhibitor’ Fasudil, is effective in preventing acetylcholine-induced vasospasm [150] and other potentially effective agents include type 3 and type 5 phosphodiesterase inhibitors (cilostazol and sildenafil, respectively). In a multicenter randomized trial of vasospastic angina patients refractory to amlodipine, type 3 phosphodiesterase inhibitor (PDEI) , cilostazol, reduced the anginal frequency and intensity without serious adverse effects [151]. In women with ANOCA (Angina with No Obstructive Coronary Arteries), sildenafil (a type 5 PDEI) acutely improved the CFR when it is < 2>
Endothelin 1 (ET-1) contributes to coronary endothelial dysfunction and its tonic inhibitory effect on myocardial perfusion is related to atherosclerosis risk factor burden [153]. Two small randomized trials of an endothelin-1 (ET-1) receptor antagonist in MVA suggested a beneficial effect [154],[155]. Currently, the Precision Medicine With Zibotentan in Microvascular Angina (PRIZE) trial [156] is investigating the effect of zibotentan, an oral endothelin A receptor-selective antagonist, on symptoms, exercise duration and myocardial blood flow in patients with microvascular angina. Dysregulation of the endothelin system is implicated in the development of CMD, and therefore zibotentan has potential as a disease-modifying therapy for CMD.
The endothelium-derived relaxing factor NO (nitric oxide) is synthesized from the amino acid L-arginine by a family of enzymes, the NO synthases, through a metabolic route, namely the L-arginine–NO pathway [157]. NO mediates vascular smooth muscle cell relaxation and inhibits platelet aggregation and adhesion and smooth muscle cell proliferation [158]. Coronary endothelial dysfunction may be a mechanism of exercise-induced myocardial ischemia in patients with effort angina and normal coronary arteriogram[159] It has been recently suggested that an increased synthesis of asymmetric dimethylarginine, which is known to reduce the bioavailability of L-arginine for NO synthase, contributes to the impaired NO activity in these patients [160] and long term oral supplementation with L-arginine for 4 weeks preserved endothelial function in CAD(coronary artery disease) and markedly reducing LDL oxidation [161] and improve exercise tolerence [162]
In epicardial coronary spasm, high-dose aspirin (as given for pericarditis) is not recommended because the blockade of prostacyclin production, can aggravate the spasm [163]. Therefore, aspirin is not routinely given in patients with coronary spasm without obstructive CAD[164]. However, in patients with non-obstructive atherosclerosis with focal epicardial spasm at the location of coronary plaques, the use of low-dose aspirin (80–100 mg per day) is beneficial.
Since most patients (approximately 70%) with microvascular angina are women during or after menopuase, it has been suggested that estrogen deficiency plays a pathogenic role in this disorder. Estrogen receptors are widely expressed in the cardiovascular system[165] and the estrogen inhibits and nicotine enhances the expression of Rho-kinase in human coronary VSMC (vascular smooth muscle cell) in vitro and that Rho-kinase is up-regulated in coronary VSMC in a porcine model of mental stress in vivo. These results may explain, at least in part, why microvascular angina is frequent in women who are post-menopausal and/or under mental stress condition. Short-term supplementation with 17-estradiol reduced the frequency of angina episodes in post-menopausal women with the disorder [166]. However, to date, there is no direct evidence that estrogen supplementation causes sustained improvement in coronary microvascular responses in those patients. Women with menopause have higher levels of anxiety or stress than those with coronary artery disease [167]. Postmenopausal women also have many vascular risk factors (e.g., diabetes mellitus, obesity, hypertension, mental stress), which cluster more frequently in women than in men.
Serotonin plasma levels were significantly higher in patients with CMD [168], the selective serotonin reuptake inhibitors (SSRIs) exhibit endothelium protective properties, reducing inflflammation and improving calcium-/nitric oxide-mediated vasodilatation and sertraline therapy signifificantly reduced CRP and IL- 6 levels[169].
Non-medical anti-anginal therapy such as a Transcutaneous Electrical Nerve Stimulation) (TENS) can be considered for severe refractory symptoms [170], however, studies report varying the results of this therapy on angina pectoris in CMD patients [171].
2 . Surgical interventions
Coronary artery bypass grafting, preferably using the internal mammary artery is the surgical treatment of choice for coronary artery atresia[172]. Coronary angioplasty with placement of stent is the treatment of choice for myocardial bridges if convincing evidence of myocardial ischemia exists either in rest ECG, exercise stress testing or myocardial perfusion imaging in selected patients [173],[174] but the results have been mixed. Unroofing the myocardial bridges [175] has been reported to reduce the incidence of ischemia, sudden death and arrhythmia especially in those with hypertrophic cardiomyopathy with documented ischemia [176].
4. Close follow up
Close follow up is necessary since there is a high propensity of the coronary anomalies[177].[178]. especially those with the anomalous vessel that passes between the two great arteries, to develop myocardial ischemia and sudden cardiac death, particularly in young and otherwise healthy individuals. Documentation of precise ischemic risk for some of these anomalies using conventional exercise stress testing or intravascular Doppler flow studies is poorly predictive and may fail to detect significant anatomic abnormalities. A normal exercise stress testing has been reported in patients who subsequently died suddenly [179],[180] and had an anomalous coronary artery and so it is not a reliable screening test to exclude congenital coronary anomalies in large athletic population [181].Similarly,intracoronary ultrasound (IVUS) may not be indicated since the anomalous vessel is highly tortuous in this patient as in Figure 8.
Thus it is possible that certain myocardial bridges, especially those of long length that courses deeply within the myocardium may also be responsible for sudden unexpected cardiac death following tachycardia related ischemia..Patients with myocardial bridging of coronaries should avoid strenuous physical activity since delayed diastolic relaxation in the bridged segment in humans has been reported.
Case analysis
A 46 year old, previously asymptomatic diabetic woman having the coronary artery anomaly , “Isolated left single coronary artery with left circumflex continuing to form the Right coronary artery with myocardial looping" based on coronary arteriography as in Figures 4 to 8 and CT Angiography as in Figure 1 [182], .presented with sudden onset of exertional chest discomfort. Her symptoms relieved spontaneously and asymptomatic on further follow up of 15 years with routine normal activities and living up to 61 years at present. Coronary Magnetic Resonance Angiography shown in Figures 2 and 3 revealed Isolated left main coronary artery trifurcates into left anterior descending, ramus intermedius and left circumflex arteries.
Angina pectoris [183] and myocardial lactate production have been documented in patients with single coronary arteries where coronary atherosclerosis [184],[185] or an anomalous coronary artery passage was absent. The sudden onset of exertional chest discomfort may be due to tachycardia related episodic ischemia as shown in Exercise ECG 3 , caused by myocardial looping of proximal portion of right coronary artery as in Figure 1[186].. The ischemia is not obligatory since there is no documented evidence as per the established criteria for myocardial ischemia (horizontal or down-sloping ST-segment depression ≥ 1 mm at 60–80 ms after the J point.) either in rest or exercise ECGs 1 to 3 and exercise ECG-4R1 and R2 [187]. Exercise ECGs with up-sloping ST-segment depressions are typically reported as an 'equivocal' test. Usually, the maximum percent reduction in diameter during systole is 56 % in myocardial bridging and the range is 30 to 100 % [188]. Systolic myocardial contraction does not limit coronary flow at heart rates less than 160 bpm or unless coronary compression extends to early diastole [189] and in this patient, the coronary flow get reduced when the heart rate increases > 160 bpm at peak exercise in stage 3 Bruce protocol and produced anginal episodes.
Outcome
Several anatomical studies have reported a protective effect of myocardial bridging that may involve protection from systolic wall stress. Myocardial bridges may slightly increase the chances of proximal coronary atherosclerosis while protecting the bridged segment and the distal artery and the overall frequency of myocardial infarction is same in patients with and without myocardial bridges [190]. Even though the mechanism of myocardial ischemia is speculative, most adverse outcomes appear to result from decreased myocardial perfusion [191],[192]. This patient is remaining healthy and still living as aged 61 years without any medications and interventions.
Exercise programme
Ischemia is unlikely to occur every time when the patient exercises [193] and the presence of additional factors such as volume status and type of physical activity (isotonic, e.g., cycling or running vs. isometric, e.g., weight-lifting [194],[195] may also contribute. SCDs commonly occur in patients participating the dynamic sports and the hemodynamic relevance depends directly on the supplied viable myocardial mass in the downstream of the stenosis. A two-tier concept for the pathomechanisms of ischemia is proposed [196] and in this concept, the occurrence of ischemia is based on the extent of a fixed (anatomic high-risk features of slit-like ostium and proximal narrowing (also referred to as hypoplasia) and a dynamic (acute take-off angle, intramural course with the elliptic vessel shape) component.
Acute take-off angle (below 45°), defined as an axial course of the proximal segment tangential to the great vessel circumference [197] and kinking of the anomalous coronary artery during exercise, i.e., decrease of the acute take-off angle and consequently increased narrowing at the ostium, was proposed as a contributing ischemia-inducing mechanisms [198],[199]. Intramural course is a threatening feature of hemodynamic relevance [200],[201] as shown by several studies and the length of the intramural segment is associated with an increased risk for ischemia [202],[203] . In addition, an elliptic proximal vessel shape (defined as height/width ratio of >1.3) [204] is frequent within the intramural segment, and the deformation (also called lateral compression), dependent from the cardiac phase, i.e., more pronounced during systole than diastole [205] has been shown to increase during physical activity with augmented great vessel wall stress [206]. The reduction of the cross-sectional area creates flow restrictions and the Fractional flow reserve (FFR, defined as the hyperemic mean distal coronary artery pressure divided by the simultaneous recorded mean aortic pressure) [207] was used to assess the hemodynamic relevance of anomalous coronaries in multiple studies and the dynamic component cannot be sufficiently reproduced using pharmacological stress with vasodilators.
The ideal stress test should be able to assess both dynamic and fixed components and has to be strenuous enough to provoke ischemic symptoms. Maximal exercise load is crucial and should aim for maximal or supramaximal stress (100% of predicted maximal heart rate or above, estimated with the formula of 220–age). Unfortunately, most performed stress tests were satisfied with 85% of the maximal heart rate [208] and it has a low reliability for correlation with clinical symptoms and prognosis [209].
“SAD”-test [210] is an invasive pharmacologic stress testing, introduced by Angelini et al with rapid infusion of 500 ml saline, dobutamine stepwise infusion up to 40 μg/kg/min and in addition 0.5 mg atropine if the heart rate is below 140 bpm at the end of the dobutamine infusion and this stress protocol is the closest equivalent to vigorous exercise. A more aggressive approach with steady infusion of saline during the whole invasive procedure (usually more than 1500 ml of saline to prevent a preload decrease) and attempts to reach 100% of the maximal heart rate, i.e., using atropine in addition to the ongoing dobutamine infusion to simulate vigorous physical exercise at the upper limit. The dobutamine and volume challenge is, of course, not practicable for every patient but should be aimed for in order to simulate maximal physical exercise and obtain conclusive results even in absence of ischemia (i.e., true-negative results).
The patients also stressed the importance of a minimum of stimuli (for example audio: the acoustics as well as the volume, preferably no music or loud voices) and pressure (for example setting goals with time limits) since it can trigger symptoms. Furthermore, they expressed the need for a slow start-up. Research has confirmed the importance to do a thorough warming-up (minimal 10 min on 50–60% of maximum intensity) to avoid “warm-up angina” [211],[212].
Conclusion
The point of importance from this case study is junctional (J point) ST depression with rapid up sloping of ST segment at peak exercise as shown in Exercise ECG 3 with rapid normalization in the recovery phase as shown in Exercise ECG 4 R1, R2 in Treadmill Testing may be due to episodic ischemia related to tachycardia with the heart rate of more than 160 bpm is significant and warrants further cardiac evaluation [213].
References
- Song, J.,K (2018) Coronary Artery Vasospasm.Korean Circulation Jourmal, Sep;48(9), 767-777.
View at Publisher | View at Google Scholar - Rocco. M.,B., Barry, J., Campbell. S., Nabel. E., Cook. E.,F., Goldman. L., Selwyn AI (1987) Circadian variation of transient myocardial ischemia in patients with coronary artery disease. Circulation,75. 395-400.
View at Publisher | View at Google Scholar - Mulcahy. D., Cunningham. D., Crean. P., Wright. C., Keegan. J., Quyyumi. A., Park. A., Fox. K (1988) Circadian variation of total ischemic burden and its alteration with anti-anginal agents. Lancet,1. 775-778.
View at Publisher | View at Google Scholar - Nademanee. K., Intarachot, V., Josephson, M.,A., Singh, B.,N.(1987) Circadian variation in occurrence of transient overt and silent myocardial ischemia in chronic stable angina and comparison with Prinzmetal's angina in men. American Journal of Cardiology,60,494-498.
View at Publisher | View at Google Scholar - Parker et al (1994) Morning Increase in Ambulatory Ischemia in Patients With Stable Coronary Artery Disease, Circulation, 89, 604-614.
View at Publisher | View at Google Scholar - Proudfit, W.,L., Shirey, E.,K., Sones, F.,M.(1966)Selective cine coronary arteriography. Correlation with clinical findings in 1,000 patients, Circulation, 33, 901-910
View at Publisher | View at Google Scholar - H.G. Kemp, H.,G.,R.A. Kronmal, R.,A.,R.E. Vlietstra, R.,E.,R.L. Frye, R.,L.(1986) Seven year survival of patients with normal or near normal coronary arteriograms: a CASS registry study, Journal of American College of Cardiology, 7 , 479-483
View at Publisher | View at Google Scholar - H.G. Kemp, H.,G.(1991)Syndrome X revisited Journal of American College of Cardiology, 17 , 507- 508
View at Publisher | View at Google Scholar - Kaski, J.,C.(1998) Chest pain and normal coronary arteriograms: role of “microvascular spasm”, Lancet, 351, 1144-1145
View at Publisher | View at Google Scholar - Crea, F., Lanza, G.,A.(2004) Angina pectoris and normal coronary arteries: cardiac syndrome X, Heart, 90 , 457-463
View at Publisher | View at Google Scholar - Camici, P.,G., Marraccini, P., Lorenzoni, R., Buzzigoli G., Pecori,N., Perissinotto, A. et al (1991).Coronary hemodynamics and myocardial metabolism in patients with syndrome X: response to pacing stress, Journal of American College of Cardiology, 17, 1461-1470
View at Publisher | View at Google Scholar - Galassi,A.,R., Crea,F., Araujo,L.,I., Lammertsma, A.,A., Pupita, G.,Yamamoto, Y. et al (1993)Comparison of regional myocardial blood flow in syndrome X and one-vessel coronary artery disease, American Joutnal of Cardiology, 72, 134-139
View at Publisher | View at Google Scholar - Hasdai,D., Gibbons,R.,J., Holmes, D.,R., Jr., Higano, S.,T., Lerman, A.(1997)Coronary endothelial dysfunction in humans is associated with myocardial perfusion defects, Circulation, 96, 3390-3395
View at Publisher | View at Google Scholar - Motz,W., Vogt, M., Rabenau,O., Scheler,S,, Lückhoff,A., Strauer, B.,E. (1991)Evidence of endothelial dysfunction in coronary resistance vessels in patients with angina pectoris and normal coronary angiograms, American Journal of Cardiology, 68, 996-1003
View at Publisher | View at Google Scholar - Takemoto,M., Sun,J., Hiroki, J., Shimokawa, H., Liao,J.,K.(2002)Rho-kinase mediates hypoxia-induced downregulation of endothelial nitric oxide synthase, Circulation, 106, 57-62
View at Publisher | View at Google Scholar - Alexander, R.,W., Griffith, G.,C (1956) Anomalies of the coronary arteries and their clinical significance. Circulation,14,800–805
View at Publisher | View at Google Scholar - Angelini, P., Villason, S., Chan, A.,V., Diez, J.,G..(1999) Normal and anomalous coronary arteries in humans. In: Angelini P, ed. Coronary Artery Anomalies: A Comprehensive Approach. Philadelphia: Lippincott Williams & Wilkins, 27–150.
View at Publisher | View at Google Scholar - Gräni, C,, Benz, D.,C., Steffen, D.,A., Clerc, O.,F., Schmied, C., Possner, M., et al.(2017) Outcome in middle-aged individuals with anomalous origin of the coronary artery from the opposite sinus: a matched cohort study. European Heart Journal. 38, 2009– 2016.
View at Publisher | View at Google Scholar - Ramachandran Muthiah (2022) Episodic Ischemia on Treadmill Testing, Webinar on 12th World Congress on Healthcare, Morning star hospital, Marthandam, Kanyakumari District, India, Walsh Medical Media, Health Care: Current Reviews, February 17.
View at Publisher | View at Google Scholar - Ramachandran Muthiah (2022) Congenital coronary anomaly, Global Summit on Cardiology and Cardiac Surgery, May 09 | Webinar, Journal of clinical & Experimental Cardiology
View at Publisher | View at Google Scholar - Muthiah R (2011) Left circumflex coronary artery is continuing to form the right coronary artery - Angiographic imaging. Journal of Saudi Heart Association, Jul. 23(3), 161-162
View at Publisher | View at Google Scholar - Roberts, W.,C., Shirani, J. (1992)The four subtypes of anomalous origin of the left main coronary artery from the right aortic sinus (or from the right coronary artery).American Journal of Cardiology, 70, 119-122.
View at Publisher | View at Google Scholar - Steffensen, T.,S., Spicer,D.,E.,(2014) Congenital coronary artery anomalies for the pathologist, Fetal and Pediatric Pathology, 33, 268-288
View at Publisher | View at Google Scholar - Villa, A.,D.,M., Sammut, E., Nair,A., et al (2016) Coronary artery anomalies overview: the normal and the abnormal, World Journal of Radiology, 8, 537-555.
View at Publisher | View at Google Scholar - Ogden, J.,A.(1969) Congenital anomalies of the coronary arteries, American Journal of Cardiology, 70, 474-479.
View at Publisher | View at Google Scholar - Angelini, P.(2007) Coronary artery anomalies. An entity in search of an identity, Circulation, 115, 1296-1305
View at Publisher | View at Google Scholar - Angelini, P.(1989) Normal and anomalous coronary arteries: definitions and classification. American Heart Journal. 117, 418–34.
View at Publisher | View at Google Scholar - Erol, C., Koplay, M., Paksoy,Y.(2013)Evaluation of anatomy, variation and anomalies of the coronary arteries with coronary computed tomography angiography, Anatolian Journal of Cardiology, 13, 154-164
View at Publisher | View at Google Scholar - Pérez-Pomares, J.,M., Pompa,J.,L., Franco,D., et al. (2016), and pathology ESC Working Group Congenital coronary artery anomalies: a bridge from embryology to anatomy and pathophysiology – a position statement of the development, anatomy,Cardiovascular Research, 109, 204-216.
View at Publisher | View at Google Scholar - Rigatelli, G., Docali,G., Rossi, P., et al (2003).Congenital coronary artery anomalies angiographic classification revisited. International Journal of Cardiovascular Imaging, 19, 361-366
View at Publisher | View at Google Scholar - Mirchandani,S., Phoon, C.,K.,L.(2005)Management of anomalous coronary arteries from the contralateral sinus, International Journal of Cardiology, 102, 383-389
View at Publisher | View at Google Scholar - Brothers, J.,A., Stephens, P., Gaynor,J.,W. et al.(2008) Anomalous aortic origin of a coronary artery with an interarterial course. Should family screening be routine? Journal of American College of Cardiology, 51, 2062-2064
View at Publisher | View at Google Scholar - Spicer, D.,E., Henderson, D.,J., Chaudhry,B., et al (2015).The anatomy and development of normal and abnormal coronary arteries,Cardiology in The Young, 25, 1493-1503
View at Publisher | View at Google Scholar - Malagò, R., Pezzato, A., Barbiani, C.,et al (2011).Coronary artery anatomy and variants,Pediatric Radiology, 41, 1505-1515
View at Publisher | View at Google Scholar - De la Cruz, M.,V., Moreno-Rodriguez, R., Angelini, P..(1999) Chapter 2: Ontogeny of the coronary vessels. In: Angelini P, Fairchild VD, editors. Coronary Artery Anomalies: A Comprehensive Approach. Philadelphia, PA: Lippincott Williams & Wilkins). p. 11–16.
View at Publisher | View at Google Scholar - Thiene, G., Frescura, C., Padalino, M., Basso, C., and Rizzo, S., (2021) Coronary Arteries: Normal Anatomy With Historical Notes and Embryology of Main Stems. Frontiers in Cardiovascular. Medicine. 8, 649855.
View at Publisher | View at Google Scholar - Bogers, A.,J., Gittenberger-de Groot, A.,C., Dubbeldam, J.,A., Huysmans, H.,A.,(1988) The inadequacy of existing theories on development of the proximal coronary arteries and their connexions with the arterial trunks. International Journal of Cardiology, 20, 117–123.
View at Publisher | View at Google Scholar - Bogers, A.,J., Gittenberger-de Groot, A.,C., Poelmann, R.,E., Péault, B.,M., Huysmans, H.,A.,(1989) Development of the origin of the coronary arteries, a matter of ingrowth or outgrowth? Anatomy and Embryology (Berl), 180,437–441.
View at Publisher | View at Google Scholar - Tomanek, R., Angelini, P.,(2019) Embryology of coronary arteries and anatomy/pathophysiology of coronary anomalies. A comprehensive update. International Journal of Cardiology,. 281, 28–34.
View at Publisher | View at Google Scholar - Eralp. I., Lie-Venema, H., DeRuiter, M.,C., van den Akker, N.,M.,S., Bogers, A.,J.,J.,C., Mentink, M.,M.,T., et al (2005). Coronary artery and orifice development is associated with proper timing of epicardial outgrowth and correlated Fas-ligand-associated apoptosis patterns. Circulation Research. 96, 526–534
View at Publisher | View at Google Scholar - Mu, H., Ohashi, R., Lin, P., Yao, Q., Chen, C..(2005) Cellular and molecular mechanisms of coronary vessel development. Vascular Medicine , 10, 37–44.
View at Publisher | View at Google Scholar - Lie-Venema, H., Gittenberger-de Groot, A.,C., Van Empel, L.,J., Boot, M.,J., Kerkdijk, H., De Kant, E., et al (2003). Ets-1 and Ets-2 transcription factors are essential for normal coronary and myocardial development in chicken embryos. Circulation Research, 92, 749–756.
View at Publisher | View at Google Scholar - Van den Akker, N.,M., Caolo, V., Wisse. L.,J., Peters, P.,P., Poelmann, R.,E., Carmeliet, P., et al (2008). Developmental coronary maturation is disturbed by aberrant cardiac vascular endothelial growth factor expression and Notch signalling. Cardiovascular Research, 78, 366–375.
View at Publisher | View at Google Scholar - Lavine, K.,J., Ornitz, D.,M., (2009) Shared circuitry: developmental signaling cascades regulate both embryonic and adult coronary vasculature. Circulation Research, 104, 159–169.
View at Publisher | View at Google Scholar - Räsänen, M, Sultan, I, Paech J, Hemanthakumar, K.,A., Yu, W., He, L., Tang, J., et al (2021). VEGF-B Promotes Endocardium-Derived Coronary Vessel Development and Cardiac Regeneration,. Circulation, 5,143,1,65-77.
View at Publisher | View at Google Scholar - Gittenberger-de Groot. A.,C., Vrancken Peeters, M.,P., Bergwerff, M., Mentink, M.,M., Poelmann. R.,E.. (2000) Epicardial outgrowth inhibition leads to compensatory mesothelial outflow tract collar and abnormal cardiac septation and coronary formation. Circulation Research, 87, 969–971.
View at Publisher | View at Google Scholar - Guadix,J,A.,Ruiz-Villalba, A.,Lettice, L., Velecela, V.,Muñoz-Chápuli, R., Hastie, N.,D., Pérez-Pomares, J.,M. Martínez-Estrada,O.,M., (2011).Wt1 controls retinoic acid signalling in embryonic epicardium through transcriptional activation of Raldh 2, Development, 138, 1093 –1097
View at Publisher | View at Google Scholar - DelMonte,G..Casanova,J.,C.,Guadix,J.,A.,MacGrogan,D.,Burch,J.,B.,E.Pérez-Pomares,J.,M.,de la Pompa, J.,L.,(2011) Differential Notch signaling in the epicardium is required for cardiac inflow development and coronary vessel morphogenesis, Circulation Research, 108, 824 –836
View at Publisher | View at Google Scholar - Grieskamp, T., Rudat, C., Lüdtke, T.,H.,W. ,Norden ,J., Kispert, A.,(2011).Notch signaling regulates smooth muscle differentiation of epicardium-derived cells, Circulation Research, 108, 813 – 823.
View at Publisher | View at Google Scholar - You, L., Lin. F. Lee, C.,T. Demayo, F.,J.(2005) Suppression of Notch signalling by the COUP-TFII transcription factor regulates vein identity, Nature, 435, 98,–104
View at Publisher | View at Google Scholar - Tomanek, R.,J. Ishii, Y. Holifield, J.,S. Sjogren, C.,L., Hansen, H.,K., Mikawa, T.,(2006)VEGF family members regulate myocardial tubulogenesis and coronary artery formation in the embryo, Circulation Research , 98, 947–953.
View at Publisher | View at Google Scholar - Lavine, K.,J., White, A.,C.,Park, C., Smith, C.,S. Choi, K., Long, F., Hui,C.,Ornitz, D.,M., (2006) Fibroblast growth factor signals regulate a wave of Hedgehog activation that is essential for coronary vascular development, Genes & Development, 20, 1651–1666.
View at Publisher | View at Google Scholar - Wu,B., Zhang, Z., Lui, W., Chen, X., Wang, Y., Chamberlain, A., Moreno-Rodriguez,R.,A., Markwald, R.,R., O'Rourke, B.,P., Sharp,D.,J., Zheng, D., Lenz, J., Baldwin, H.,S.,Chang,C.,P., Zhou,B., (2012) Endocardial cells form the coronary arteries by angiogenesis through myocardial-endocardial VEGF signaling, Cell, 151, 1083-1096
View at Publisher | View at Google Scholar - Red-Horse, K., Ueno, H., Weissman, I.,L., Krasnow, M.,(2010) Coronary arteries form by developmental reprogramming of venous cells, Nature, 464, 549- 553.
View at Publisher | View at Google Scholar - Katz,T.,C., Singh,M.,K., Degenhardt,K., Rivera-Feliciano, J.,Johnson,R., Epstein,J., Tabin, C.(2012) Distinct compartments of the proepicardial organ give rise to coronary vascular endothelial cells, Developmental Cell, 22, 639 –650.
View at Publisher | View at Google Scholar - Ivins,S., Chappell, J., Vernay,B., Suntharalingham,J., Martineau, A., Mohun,T.,J.,Scambler, P.,J.(2015) The CXCL12/CXCR4 axis plays a critical role in coronary artery development, Developmental Cell, 33, 455 – 468
View at Publisher | View at Google Scholar - Chiu,I.,S., Anderson,R.,H.,(2012) Can we better understand the known variations in coronary arterial anatomy? Annals of Thoracic Surgery, 94, 1751 –1760
View at Publisher | View at Google Scholar - Wessels,A., Pérez-Pomares,J.,M.(2004) The epicardium and epicardially derived cells (EPDCs) as cardiac stem cells,The anatomical record. Discoveries in molecular, cellular, and evolutionary biology. 276, 43 -57.
View at Publisher | View at Google Scholar - Yamaguchi,Y., Cavallero, S., Patterson,M., Shen, H., Xu,J., Kumar, S.,R., Sucov, H.,M.(2015) Adipogenesis and epicardial adipose tissue: a novel fate of the epicardium induced by mesenchymal transformation and PPARγ (Peroxisome proliferator- activated receptor gamma) activation, Proceedings of the Natlonal Academy of Sciences, 112, 2070 –2075
View at Publisher | View at Google Scholar - Frescura. C., Basso, C., Thiene. G., Corrado. D., Pennelli, T., Angelini, A., et al (1998). Anomalous origin of coronary arteries and risk of sudden death: a study based on an autopsy population of congenital heart disease. Human Pathology. 29, 689–695.
View at Publisher | View at Google Scholar - Thiene, G., Rizzo, S., Frescura, C., Basso, C.. (2020) Chapter 21: Specific cardiovascular diseases and competitive sports participation: coronary anomalies and myocardial bridging at risk of sudden death. In: Pressler A, Niebauer J, editors. Textbook of Sports and Exercise Cardiology. Cham: Switzerland Springer p. 403–421.
View at Publisher | View at Google Scholar - Angelini, P., Trivellato, M., Donis, J., Leachman. R.,D..(1983) Myocardial bridge: a review. Progress in Cardiovascukar Diseases, 26, 75–88.
View at Publisher | View at Google Scholar - Mohlenkamp,S.,Hort, W, Ge, J.,Erbel, R., (2002) Update on myocardial bridging, Circulation, 106, 2616- 2622.
View at Publisher | View at Google Scholar - Virmani, R., Chun, P.,K.,.C., Goldstein, R.,E., Robinowitz, M., McAllister, H.,A.(1986)Acute takeoffs of the coronary arteries along the aortic wall and congenital coronary ostial valve-like ridges: association with sudden death..Journal of American College of Cardiology, 3, 766-771
View at Publisher | View at Google Scholar - Bloomfield, P., Erhlichm C,, Folland, A.,D., Bianco, J., Tow, D.,E., Parisi, A.,F.(1983) A surgically correctable cause of angina pectoris..American Journal of Cardiology, 51, 1235-1237
View at Publisher | View at Google Scholar - Frommelt, P.,C., Frommelt, M.,A., Tweddell, J.,S., Jaquiss, R.,D .(2003) Prospective echocardiographic diagnosis and surgical repair of anomalous origin of a coronary artery from the opposite sinus with an interarterial course..,Journal of American College of Cardiology, 42, 148-154.
View at Publisher | View at Google Scholar - Basso, C., Corrado, D., Thiene, G.,(2001) Congenital coronary anomalies as an important cause of sudden death in the young..Cardiology in Review, 9, 312-317
View at Publisher | View at Google Scholar - Angelini, P., Velasco, J.,A., Ott, D., Khoshnevis, G.,R. (2003)..Anomalous coronary artery arising from the opposite sinus: descriptive features and pathophysiologic mechanisms, as documented by intravascular ultrasonography. Journal of Invasive Cardiology, 15, 507-514.
View at Publisher | View at Google Scholar - Duncker, D.,J., et al (2015) Regulation of coronary blood flow in health and ischemic heart disease. Progress in Cardiovascular Diseases, 57, 409–422.
View at Publisher | View at Google Scholar - Furchgott, R.,F., Zawadzki, J.,V (1980)The obligatory role of endothelial cells in the relaxation of arterial smooth muscle by acetylcholine. Nature, 288, 373–376.
View at Publisher | View at Google Scholar - Pries, A.,R., et al (2015) Coronary vascular regulation, remodelling, and collateralization: mechanisms and clinical implications on behalf of the working group on coronary pathophysiology and microcirculation. European Heart Journal,. 36, 3134–3146.
View at Publisher | View at Google Scholar - Kaski, J.,C., et al (2018) Reappraisal of ischemic heart disease. Circulation, 138, 1463–1480.
View at Publisher | View at Google Scholar - Ong P, et al. (2012) High prevalence of a pathological response to acetylcholine testing in patients with stable angina pectoris and unobstructed coronary arteries: the ACOVA study. Journal of American College of Cardiology, 59, 655–662.
View at Publisher | View at Google Scholar - Camici, P.,G., Crea, F. (2007) Coronary microvascular dysfunction, New England Journal of Medicine, 356, 830‐840.
View at Publisher | View at Google Scholar - Bradley, C., Berry, C. (2022) Definition and epidemiology of coronary microvascular disease. Journal of Nuclear Cardiology. 29, 1763–1775.
View at Publisher | View at Google Scholar - Gulati, M., Shaw, L.,J., Bairey Merz, C.,N (2012) Myocardial ischemia in women: lessons from the NHLBI WISE study. Clinical Cardiology,.35, 141–148.
View at Publisher | View at Google Scholar - Cosin-Sales, J., et al (2003) C-reactive protein, clinical presentation, and ischemic activity in patients with chest pain and normal coronary angiograms. Journal of American College of Cardiology, 41, 1468–1474.
View at Publisher | View at Google Scholar - Ong, P., et al (2012) Increased coronary vasoconstrictor response to acetylcholine in women with chest pain and normal coronary arteriograms (cardiac syndrome X). Clinical Research in Cardiology. 101, 673–681.
View at Publisher | View at Google Scholar - Matsuda, Y., et al (1983) Coronary arteriography and left ventriculography during spontaneous and exercise-induced ST segment elevation in patients with variant angina, American Heart Journal., 106, 509–515.
View at Publisher | View at Google Scholar - Minoda, K., et al (1994) Comparison of the distribution of myocardial blood flow between exercise-induced and hyperventilation-induced attacks of coronary spasm: a study with thallium-201 myocardial scintigraphy. American Heart Journal, 127, 1474–1480.
View at Publisher | View at Google Scholar - Sara, J.,D., et al (2015) Prevalence of coronary microvascular dysfunction among patients with chest pain and nonobstructive coronary artery disease. JACC Cardiovascular Interventions, 8, 1445–1453.
View at Publisher | View at Google Scholar - Sueda, S, et al (2016). Gender differences in sensitivity of acetylcholine and ergonovine to coronary spasm provocation test. Heart Vessels, 31, 322–329.
View at Publisher | View at Google Scholar - Everaars, H., et a (2018)l Doppler flow velocity thermodilution to assess coronary flow reserve: a head-to-head comparison with [(15)O]H2O PET. JACC Cardiovascular Interventions, 11, 2044–2054.
View at Publisher | View at Google Scholar - Taqueti, V.,R., Di Carli M.,F. (2016) Clinical significance of noninvasive coronary flow reserve assessment in patients with ischemic heart disease. Current Opinion in Cardiology. 31, 662–669.
View at Publisher | View at Google Scholar - Ford, T.,J., Berry, C, (2019) How to diagnose and manage angina without obstructive coronary artery disease: lessons from the british heart foundation CorMicA trial. Interventional Cardiology., 14, 76–82.
View at Publisher | View at Google Scholar - Williams, R.,P., et al (2018)Doppler versus thermodilution-derived coronary microvascular resistance to predict coronary microvascular dysfunction in patients with acute myocardial infarction or stable angina pectoris. American Journal of Cardiology, 121, 1–8.
View at Publisher | View at Google Scholar - Rahman, H., et al (2020) Physiological stratification of patients with angina due to coronary microvascular dysfunction. Journal of American College of Cardiology, 75, 2538–2549.
View at Publisher | View at Google Scholar - Knuuti, J., et al (2020). ESC Guidelines for the diagnosis and management of chronic coronary syndromes. European Heart Journal, 41, 407–477.
View at Publisher | View at Google Scholar - Thomson, L.,E., et al (2015). Cardiac magnetic resonance myocardial perfusion reserve index is reduced in women with coronary microvascular dysfunction. A national heart, lung, and blood institute-sponsored study from the women's ischemia syndrome evaluation. Circulation: Cardiovascular Imaging. 8, 2481.
View at Publisher | View at Google Scholar - Taqueti ,V.,R., Di Carli, M.,F.(2016) Clinical significance of noninvasive coronary flow reserve assessment in patients with ischemic heart disease. Current Opinion in Cardiology, 31, 662–669.
View at Publisher | View at Google Scholar - Kaufmann, P.,A., et al (1999) Assessment of the reproducibility of baseline hyperemic myocardial blood flow measurements with 15O-labeled water PET. Journal of Nuclear Medicine., 40, 1848–1856.
View at Publisher | View at Google Scholar - Nagamachi, S., et al (1996) Reproducibility of measurements of regional resting hyperemic myocardial blood flow assessed with PET. Journal of Nuclear Medicine., 37, 1626–1631.
View at Publisher | View at Google Scholar - Everaars, H., et al (2018) Doppler flow velocity thermodilution to assess coronary flow reserve: a head-to-head comparison with [(15)O]H2O PET. JACC Cardiovascular Interventions, 11, 2044–2054.
View at Publisher | View at Google Scholar - Bravo, P.,E., Di Carli, M.,F., Dorbala, A (2017) Role of PET to evaluate coronary microvascular dysfunction in non-ischemic cardiomyopathies. Heart failure reviews, 22,455–464.
View at Publisher | View at Google Scholar - Kuruvilla, S., Kramer, C.,M (2013) Coronary microvascular dysfunction in women: an overview of diagnostic strategies. Expert Review of Cardiovascular Therapy. 11, 1515–1525.
View at Publisher | View at Google Scholar - Maddahi, J., Packard, R.,R.,S. (2014) Cardiac PET perfusion tracers: current status and future directions. Seminars in Nuclear Medicine., 44, 333–343.
View at Publisher | View at Google Scholar - Konst, R.,E, et al (2021)Vasomotor dysfunction in patients with angina and non-obstructive coronary artery disease is dominated by vasospasm. International Journal of Cardiology. 2, 79.
View at Publisher | View at Google Scholar - Suda, A., et al (2019) Coronary functional abnormalities in patients with angina and nonobstructive coronary artery disease. Journal of American College of Cardiology, 74, 2350–2360.
View at Publisher | View at Google Scholar - Everaars, H, et al (2019) Continuous thermodilution to assess absolute flow and microvascular resistance: validation in humans using [15O]H2O positron emission tomography. European Heart Journal,. 40, 2350–2359.
View at Publisher | View at Google Scholar - Xaplanteris, P., et al (2018). Catheter-based measurements of absolute coronary blood flow and microvascular resistance: feasibility, safety, and reproducibility in humans. Circulation: Cardiovascular Interventions,.11, e006194.
View at Publisher | View at Google Scholar - Van 't Veer, M., et al (2016) Novel monorail infusion catheter for volumetric coronary blood flow measurement in humans: in vitro validation. EuroIntervention, 12, 701–707.
View at Publisher | View at Google Scholar - Mery, C.,M., Lopez, K.,N., Molossi, S., et al (2016). Decision analysis to define the optimal management of athletes with anomalous aortic origin of a coronary artery, Journal of Thoracic and Cardiovascular Surgery, 152, 1366-1375
View at Publisher | View at Google Scholar - Mery, C.,M., Lawrence, S,M., Krishnamurthy, R., et al (2014).Anomalous aortic origin of a coronary artery: towards a standardized approach, Seminars in Thoracic and Cardiovascular Surgery, 26,110-122.
View at Publisher | View at Google Scholar - Frommelt, P.,C. (2009) Congenital coronary artery abnormalities predisposing to sudden cardiac death, Pacing and Clinical Electrophysiology, 32, 63-66
View at Publisher | View at Google Scholar - Stecker, E.,C., Reinier, K., Marijon,E., et al (2014).Public heath burden of sudden cardiac death in the United States, Circulation: Arrhythmias and Electrophysiology, 7, 121-217
View at Publisher | View at Google Scholar - Cheitlin, M.,D., MacGregor, J.,(2009) Congenital anomalies of the coronary arteries, Herz Cardiovascular diseases, 34. 268-279.
View at Publisher | View at Google Scholar - Basso, C., Maron, B.,J., Corrado, D., Thiene, G.(2000) Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes.Journal of American College of Cardiology, 35, 14931501.
View at Publisher | View at Google Scholar - Lipton, M.,J., Barry, W.,H., Obrez, I., Silverman, J.,F., Wexler, L.(1979) Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 130, 39-47
View at Publisher | View at Google Scholar - Yurtdaş, M., Gülen, O.(2012) Anomalous origin of the right coronary artery from the left anterior descending artery: review of the literature. Cardiology Journal. 19, 122–129.
View at Publisher | View at Google Scholar - Elbadawi, Ayman, et al.(2018)
View at Publisher | View at Google Scholar - Taylor, A.,J., Rogan, K.,M., Virmani, R (1992) Sudden cardiac death associated with isolated congenital coronary artery anomalies. Journal American College of Cardiology, 20, 640-647.
View at Publisher | View at Google Scholar - Akcay, A., Tuncer, C., Batyraliev, T., Gokce, M., Eryonucu, B., Koroglu, S., Yilmaz, R (2008) Isolated single coronary artery, Circulation Journal, 72, 1254-1258.
View at Publisher | View at Google Scholar - Morales, A.,R., Romanelli, R., Tate, L.,G., Boucek, R.,J., de Marchena, E (1993). Intramural left anterior descending coronary artery: significance of the depth of the muscular tunnel, Human Pathology, 24, 693–701.
View at Publisher | View at Google Scholar - Ferreira ,A.,G., Jr, Trotter, S.,E., König, B., Jr, Décourt, L.,V., Fox, K., Olsen, E.,G (1991) Myocardial bridges: morphological and functional aspects. British Heart Journal. 66, 364–367.
View at Publisher | View at Google Scholar - Kitazume, H., Kramer, J.,R., Krauthamer, D., El Tobgi, S., Proudfit, W.,L., Sones, F.,M (1983).Myocardial bridges in obstructiv hypertrophic cardiomyopathy.American Heart Journal, 106, 131–135.
View at Publisher | View at Google Scholar - Navarro-Lopez, F., Soler, J., Magrina, J., Esplugues, E., Pare, J.,C., Sanz, G. et al. (1986) Systolic compression of coronary artery in hypertrophic cardiomyopathy. International Journal of Cardiology, 12, 309–320.
View at Publisher | View at Google Scholar - Corban, M.,T., Hung, O.,Y., Eshtehardi, P., Rasoul-Arzrumly, E., McDaniel, M., Mekonnen, G.,et al.(2014) Myocardial bridging: contemporary understanding of pathophysiology with implications for diagnostic and therapeutic strategies. Journal of American College of Cardiology, 63, 2346–2355.
View at Publisher | View at Google Scholar - Angelini, P., Trivellato, M., Donis, J., Leachman, R.,D..(1983) Myocardial bridges: a review. Progress in Cardiovascular Diseases. 26, 75–88.
View at Publisher | View at Google Scholar - En-sen Ma, Guo-lin Ma, Hong-wei Yu, Wang Wu, and Kefeng Li (2013) Assessment of Myocardial Bridge and Mural Coronary Artery Using ECG-Gated 256-Slice CT Angiography:A Retrospective Study, The Scientific World Journal, Fig2
View at Publisher | View at Google Scholar - Ge,J., Jeremias, A., Rupp, A., Abels, M., Baumgart, D., Liu, F., et al (1999). New signs characteristic of myocardial bridging demonstrated by intracoronary ultrasound and Doppler. European Heart Journal, 20, 1707–1716.
View at Publisher | View at Google Scholar - Jorge, R., Alegria, Joerg Herrmann, David, R., Holmes, Jr, Amir Lerman, Charanjit, S., Rihal (2005), Myocardial bridging, European Heart Journal, 26, 12, 1159–1168.
View at Publisher | View at Google Scholar - Roberts, W.,C, Glick, B.,N. (1992). Congenital hypoplasia of both right and left circumflex coronary arteries. American Journal of Cardiology, 70, 121–123.
View at Publisher | View at Google Scholar - Zugibe, F.,T., Zugibe, F.,T. Jr, Costello, J.,T., et al (1993). Hypoplastic coronary artery disease in the spectrum of sudden unexpected death in young and middle age adults.,American Journal of Forensic Medicine and Pathology, 14: 276–283.
View at Publisher | View at Google Scholar - Ogden, J.,A.(1970) Congenital anomalies of the coronary arteries. American Journal of Cardiology, 25, 474–479.
View at Publisher | View at Google Scholar - Go¨lMK,O.Zatik, M.,A., Kunt, A., et al (2002). Coronary anomalies in adult patients. Medical Science Monitor, 8, CR636–641.
View at Publisher | View at Google Scholar - Whiting, W.(1937).Angina Pectoris at the Age of Fourteen Associated with Congenital Rudimentary Right Coronary Artery and Rudimentary Posterior Cusp of Mitral Valve. American Heart Journal; 14, 1, 104-106.
View at Publisher | View at Google Scholar - Aydar, Y., Yazici, H., Birdane, A. et al (2013). Relationship Between Hypoplastic Right Coronary Artery and Coronary Artery Anomalies. European Review for Medical and Pharmacological Sciences., 17, 5, 694-700.
View at Publisher | View at Google Scholar - McFarland, C., Swamy, R., Shah, A. (2011) Hypoplastic Coronary Artery Disease: A Rare Cause of Sudden Cardiac Death and Its Treatment with an Implantable Defibrillator. Journal of Cardiology Cases, 4, 3, :e148-151.
View at Publisher | View at Google Scholar - Imperi,G.,A., Lambert, C.,R.,, Coy, K., Lopez, L., Pepine, C.,J. (1987) Effects of titrated beta-blockade (metoprolol) on silent myocardial ischemia in ambulatory patients with coronary artery disease, American Journal of Cardiology, 60, 519-524
View at Publisher | View at Google Scholar - Nair, C.,K., Dang, B., Heintz, M.,H, et al (1986). Myocardial bridges: effect of propranolol on systolic compression. Canadian Journal of Cardiology. 1986, 2, 218–221.
View at Publisher | View at Google Scholar - Muller, J.,E., Stone, P.,H., Turi, Z.,G., Rutherford, J.,D., Czeisler, C.,A., Parker, C., Poole, W.,K., Passamani, E., Roberts, R., Robertson, T., Sobel. B.,E., Willerson, J.,T., Braunwald, E. (1985) The MILIS Study Group. Circadian variation in the frequency of onset of acute myocardial infarction. New England Journal of Meducine,313,1315-1322.
View at Publisher | View at Google Scholar - Hjalmarson, A., Gilpin, E.,A., Nicod, P., Dittuch, H., Engler, H., Blacky, A.,R., Smith, S.,C., Rocco, F., Ross, J., Jr (1989)Differing circadian patterns of symptom onset in subgroups of patients with myocardial infarction. Circulation, 80, 267-275.
View at Publisher | View at Google Scholar - Peters, R.,W., Muller, J.,E., Goldstein, S., Byington, R., Freidman, L.,M.(1989),The BHAT Study Group. Propranolol and the morning increase in the frequency of sudden cardiac death (BHAT Study). American Journal of Cardiology, 63, 1518-1520.
View at Publisher | View at Google Scholar - McClenachan, J.,M., Weidinger, F.,F., Barry, J., Yeung, A.,C., Nabel, E.,G., Rocco, M.,B., Selwyn, A.,P.(1991) Relations between heart rate, ischemia, and drug therapy during daily life in patients with coronary artery disease. Circulation,83, 1263-1270.
View at Publisher | View at Google Scholar - Knuuti, J., et al (2019) ESC Guidelines for the diagnosis and management of chronic coronary syndromes. European Heart Journal, 23, 357.
View at Publisher | View at Google Scholar - Task Force, M., et al. (2013). ESC guidelines on the management of stable coronary artery disease: the task force on the management of stable coronary artery disease of the European Society of Cardiology. European Heart Journal., 34, 2949–3003
View at Publisher | View at Google Scholar - Kusama Y, et al (2011) Variant angina and coronary artery spasm: the clinical spectrum, pathophysiology, and management. Journal of Nippon Medical School, 78, 4–12.
View at Publisher | View at Google Scholar - Tarkin, J.,M., Kaski, J.,C (2016) Vasodilator Therapy: Nitrates and Nicorandil. Cardiovascular Drugs And Therapy., 30, 367–378.
View at Publisher | View at Google Scholar - Robertson, R.,M., et al (1982) Exacerbation of vasotonic angina pectoris by propranolol. Circulation, 65, 281–285.
View at Publisher | View at Google Scholar - Rosamond, W (2004) Are migraine and coronary heart disease associated? an epidemiologic review. Headache, 44, S5–12.
View at Publisher | View at Google Scholar - Sen, N., et al (2009) Nebivolol therapy improves endothelial function increases exercise tolerance in patients with cardiac syndrome X. Anadolu Kardiyol Derg, 9, 371–379.
View at Publisher | View at Google Scholar - Erdamar, H, et al (2009) The effect of nebivolol treatment on oxidative stress antioxidant status in patients with cardiac syndrome-X. Coronary Artery Disease, 20, 238–244.
View at Publisher | View at Google Scholar - Kook, H., et al (2020). Comparison of nebivolol versus diltiazem in improving coronary artery spasm and quality of life in patients with hypertension and vasospastic angina: a prospective, randomized, double-blind pilot study. PLoS (Public Library of Science) ONE., 15, e0239039.
View at Publisher | View at Google Scholar - Rousseau, M.,F., et al (2005) Comparative efficacy of ranolazine versus atenolol for chronic angina pectoris. American Journal of Cardiology, 95, 311–316.
View at Publisher | View at Google Scholar - Dean, J., et al (2015) Coronary microvascular dysfunction: sex-specific risk, diagnosis, and therapy. Nature Reviews Cardiology., 12, 406–414.
View at Publisher | View at Google Scholar - Ong, P., Athanasiadis, A., Sechtem, U (2015) Pharmacotherapy for coronary microvascular dysfunction. European Heart Journal - Cardiovascular Pharmacotherapy, 1, 65–71.
View at Publisher | View at Google Scholar - Marinescu, M.,A., et al (2015) Coronary microvascular dysfunction, microvascular angina, and treatment strategies. JACC Cardiovasc Imaging, 8, 210–220.
View at Publisher | View at Google Scholar - Rambarat, C.,A., et al (2019) Late sodium channel blockade improves angina and myocardial perfusion in patients with severe coronary microvascular dysfunction: women's ischemia syndrome evaluation-coronary vascular dysfunction ancillary study. International Journal of Cardiology, 276, 8–13.
View at Publisher | View at Google Scholar - Bairey Merz, C.,N., et al (2020) Treatment of coronary microvascular dysfunction. Cardiovascular Research. 11, 856–870.
View at Publisher | View at Google Scholar - Masumoto, A., et al (2002) Suppression of coronary artery spasm by the Rho-kinase inhibitor fasudil in patients with vasospastic angina. Circulation, 105, 1545–1547.
View at Publisher | View at Google Scholar - Shin. E.,S., et al (2014) A randomised, multicentre, double blind, placebo controlled trial to evaluate the efficacy and safety of cilostazol in patients with vasospastic angina. Heart, 100, 1531–1536.
View at Publisher | View at Google Scholar - Denardo, S.,J., et al (2011) Effect of phosphodiesterase type 5 inhibition on microvascular coronary dysfunction in women: a Women's Ischemia Syndrome Evaluation (WISE) ancillary study. Clinical Cardiology, 34, 483–487.
View at Publisher | View at Google Scholar - Mather, K.,J., et al (2010) Role of endogenous ET-1 in the regulation of myocardial blood flow in lean and obese humans. Obesity, 18, 63–70.
View at Publisher | View at Google Scholar - Johnson, N.,P., Gould, K.,L.(2013) Physiology of endothelin in producing myocardial perfusion heterogeneity: a mechanistic study using darusentan and positron emission tomography. Journal of Nuclear Cardiology, 20, 835–844
View at Publisher | View at Google Scholar - Reriani, M., et al (2010) Long-term administration of endothelin receptor antagonist improves coronary endothelial function in patients with early atherosclerosis. Circulation, 122, 958–966.
View at Publisher | View at Google Scholar - Morrow, A.,J., Ford, T.,J., Mangion, K., Kotecha, T., Rakhit, R., Galasko, G., et al (2020) Rationale and design of the Medical Research Council’s Precision Medicine with Zibotentan in Microvascular Angina (PRIZE) trial. American Heart Journal 229, 70‐80.
View at Publisher | View at Google Scholar - Moncada, S., Higgs, A (1993).The L-arginine-nitric oxide pathway. New England Journal of Medicine., 329, 2002–2012.
View at Publisher | View at Google Scholar - Drexler, H., Zeiher, A.,M., Meinzer, K., Just, H. (1991) Correction of endothelial dysfunction in coronary microcirculation of hypercholesterolemic patients by L-arginine, Lancet; 338, 1546–1550.
View at Publisher | View at Google Scholar - Zeiher, A.,M., Krause, T., Schächinger, V., Minners, J., Moser, E. (1995). Impaired endothelium-dependent vasodilation of coronary resistance vessels is associated with exercise-induced myocardial ischemia. Circulation, 91, 2345–2352.
View at Publisher | View at Google Scholar - Okyay,K., Cengel, A.,. Sahinarslan, A,, Tavil, Y., Turkoglu, S., Biberoglu,G., et al.(2007) Plasma asymmetric dimethylarginine and L-arginine levels in patients with cardiac syndrome X, Coronary Artery Disease, 18, , 539-544.
View at Publisher | View at Google Scholar - Yin, W.,.H.., Chen, J.,.W., Tsai, C.., Chiang, M.,.C.., Young, M.,.S.., Lin, S.,.J (2005).L-arginine improves endothelial function and reduces LDL oxidation in patients with stable coronary artery disease. Clinical. Nutrition, 24, 988–997.
View at Publisher | View at Google Scholar - Bellamy,M.,F., Goodfellow,J.,Tweddel, A,C., Dunstan, F.,D.,.Lewis, M.,J., Henderson, A.,H.(1998)Syndrome X and endothelial dysfunction, Cardiovascular Research, 40, 410-417.
View at Publisher | View at Google Scholar - Miwa, K., Kambara, H., Kawai, C (1983) Effect of aspirin in large doses on attacks of variant angina. American Heart Journal,. 105, 351–355.
View at Publisher | View at Google Scholar - Picard, F., et al (2019). Vasospastic angina: A literature review of current evidence. Archives of Cardiovascular Diseases., 112, 44–55.
View at Publisher | View at Google Scholar - Orshal, J.,M., Khalil, R.,A (2004) Gender, sex hormones, and vascular tone. American Journal of Physiology- Regulatory, Integrative and Comparative Physiology, 286, R233—249.
View at Publisher | View at Google Scholar - Rosano, G.,M., Peters, N.,S., Lefroy, D., Lindsay, D.,C., Sarrel, P.,M., Collins, P., et al (1996)17-Beta-estradiol therapy lessens angina in postmenopausal women with syndrome X. Journal of American College of Cardiology, 28, 1500—1505
View at Publisher | View at Google Scholar - Asbury, E.,A., Creed, F., Collins, P.(2004) Distinct psychosocial differences between women with coronary heart disease and cardiac syndrome X. European Heart Journal,25, 1695—1701
View at Publisher | View at Google Scholar - Rocco, E.; Grimaldi, M.C.; Maino, A.; Cappannoli, L.; Pedicino, D.; Liuzzo, G.; Biasucci, L.M.(2022) Advances and Challenges in Biomarkers Use for Coronary Microvascular Dysfunction: From Bench to Clinical Practice. Journal of Clinical. Medicine, 11, 2055.
View at Publisher | View at Google Scholar - Pizzi, C.; Mancini, S.; Angeloni, L.; Fontana, F.; Manzoli, L.; Costa, G.M. (2009) Effects of Selective Serotonin Reuptake Inhibitor Therapy on Endothelial Function and Inflflammatory Markers in Patients with Coronary Heart Disease. Clinical. Pharmacology &. Therapeitics., 86, 527–532.
View at Publisher | View at Google Scholar - Crea, F., Camici, P.,G., Bairey Merz, C.,N.(2014).Coronary microvascular dysfunction: an update. European Heart Journal, 35, 1101–1111
View at Publisher | View at Google Scholar - Kaski, J.,C., Valenzuela Garcia, L.,F.(2001)Therapeutic options for the management of patients with cardiac syndrome X. European Heart Journal,. 22, 283–293.
View at Publisher | View at Google Scholar - Iversen, S., Hake, U., Meyer, E., et al (1992). Surgical treatment of myocardial bridging causing coronary artery obstruction. Scandinavian Journal of Thoracic and Cardiovascular Surgery. 26, 107–111.
View at Publisher | View at Google Scholar - Hariharan, R., Kacere, R.,D., Angelini, P.(2002). Can stent-angioplasty be a valid alternative to surgery when revascularization is indicated for anomalous origination of a coronary artery from the opposite sinus? Texas Heart Institute Journal. 29, 308–313
View at Publisher | View at Google Scholar - Chen, M., Hong, T., Huo, Y. (2005).Stenting for left main stenosis in a child with anomalous origin of left coronary artery: case report. Chinese Medical Journal. 118: 80–82.
View at Publisher | View at Google Scholar - Betriu, A., Tabau, J., Sanz, G., et al.(1980) Relief of angina by periarterial muscle resection of myocardial bridges. American Heart Journal,100, 223–226
View at Publisher | View at Google Scholar - Ochsner, J.,L., Mills, N.,L. (1984). Surgical management of diseased intracavitary coronary arteries, Annals of Thoracic Surgery, 38, 356–362
View at Publisher | View at Google Scholar - Roberts.W.,C.(1986)Major anomalies of coronary arterial origin seen in adulthood, American Heart Journal, 111, 941–963
View at Publisher | View at Google Scholar - Davis, J.,A., Cecchin, F., Jones, T.,K., Portman. M.,A. (2001) Major coronary artery anomalies in a pediatric population: incidence and clinical importance. Journal of American College of Cardiology. 37, 593–597.
View at Publisher | View at Google Scholar - Shang, S.,J., Jr, Pepine , C.,J. (1977) Transient asymptomatic ST segment depression during daily activity, American Journal of Cardiology, 39, 396-402
View at Publisher | View at Google Scholar - Kwok ,Y., Kim, C., Grady, D, et al (1999) Meta-analysis of exercise testing to detect coronary artery disease in women. American Journal of Cardiology. 83, 660
View at Publisher | View at Google Scholar - Hejmadi,A., Sahn, D.,J. (2003). What is the most effective method of detecting anomalous coronary origin in symptomatic patients? Journal of American College of Cardiology. 42, 155–157.
View at Publisher | View at Google Scholar - Kulkarni, M., Sodani, A., Rosita, Puranik, C., Sullere, S., Saha, B..(2004) Right myocardial bridge on CT coronary angiography. Journal of the Association of Physicians of India, 52, 661–662.
View at Publisher | View at Google Scholar - Mulcahy, D, Keegan, J., Sparrow, J., et al.(1989) Ischemia in the ambulatory setting—the totally ischemic burden relation to exercise testing and investigative and therapeutic implications, Journal of American College of Cardiology, 14, 1166-1172
View at Publisher | View at Google Scholar - Liberthson, R.,R. (1989) Nonatherosclerotic coronary artery disease. In: Eagle K.,A., ed. The Practice of Cardiology. Boston: Little, Brown and Company, 614–651
View at Publisher | View at Google Scholar - Corrado, D., Thiene, G., Cocco, P., Frescura,C.(1992) Non-atherosclerotic coronary artery disease and sudden death in the young. British Heart Journal, 68: 601–607.
View at Publisher | View at Google Scholar - Woldow, A.,B., Goldstein, S., Yazdanfar, S. (1994) Angiographic evidence of right coronary bridging. Catheterization and Cardiovascular Diagnosis, 32, 351–353.
View at Publisher | View at Google Scholar - Deanfield,E., Maseri,A., Selwyn,A.P., et al (1983).Myocardial ischaemia during daily life in patients with stable angina: its relation to symptoms and heart rate changes, Lancet, 2, 753-758
View at Publisher | View at Google Scholar - Malek. A.,M., Alper, S.,L., Izumo. S..(1999) Hemodynamic shear stress and its role in atherosclerosis. Journal of American Medical Association, 282, 2035–2042.
View at Publisher | View at Google Scholar - Ge, J., Erbel, R., Görge, G, et al(1995). High wall shear stress proximal to myocardial bridging and atherosclerosis: intracoronary ultrasound and pressure measurements. British Heart Journal. 73, 462–465.
View at Publisher | View at Google Scholar - Agirbasli, M,, Martin, G.,S., Stout, J.,B., et al (1997).Myocardial bridge as a cause for thrombus formation and myocardial infarction in a young athlete. Clinical Cardiology. 20, 1032–1036.
View at Publisher | View at Google Scholar - Taylor, A.,J., .Rogan, K.,M., Virmani. R. (1992) Sudden cardiac death associated with isolated congenital coronary artery anomalies, Journal of American College of Cardiology, 20. 640–647.
View at Publisher | View at Google Scholar - Taylor, A.,J., Farb, A., Ferguson, M., Virmani, R..(1997) Myocardial infarction associated with physical exertion in a young man. Circulation, 96, 3201–3204.
View at Publisher | View at Google Scholar - Brothers, J., Carter. C., McBride, M., Spray, T., Paridon, S (2010) Anomalous left coronary artery origin from the opposite sinus of Valsalva: evidence of intermittent ischemia. Journal of Thoracic and Cardiovascular Surgery, 140, e27–29.
View at Publisher | View at Google Scholar - Mitchell, J/.H., Haskell, W., Snell, P., Van Camp, S.,P. (2005) Task force 8: classification of sports. Journal of American College of Cardiology, 45, 1364–1367.
View at Publisher | View at Google Scholar - Grani, C., Chappex, N., Fracasso, T., Vital, C., Kellerhals, C., Schmied, C., et al (2016) Sports-related sudden cardiac death in Switzerland classified by static and dynamic components of exercise. European Journal of Preventive Cardiology, 23, 1228–1236.
View at Publisher | View at Google Scholar - Angelini, P., Uribe, C (2018) Anatomic spectrum of left coronary artery anomalies and associated mechanisms of coronary insufficiency. Catheterization and Cardiovascular Interventions, 92, 313–321.
View at Publisher | View at Google Scholar - Nasis, A,, Machado, C,, Cameron, J.,D., Troupis, J.,M., Meredith, I.,T,, Seneviratne, S.,K (2015).Anatomic characteristics and outcome of adults with coronary arteries arising from an anomalous location detected with coronary computed tomography angiography. International Journal of Cardiovascular Imaging, 31, 181–191.
View at Publisher | View at Google Scholar - Taylor, A.,J., Byers, J.,P., Cheitlin, M.,D., Virmani, R. (1997) Anomalous right or left coronary artery from the contralateral coronary sinus: “high-risk” abnormalities in the initial coronary artery course and heterogeneous clinical outcomes. American Heart Journal, 133, 428–350
View at Publisher | View at Google Scholar - Grollman, J.,H. Jr, Mao, S.,S., Weinstein, S.,R (1992) Arteriographic demonstration of both kinking at the origin and compression between the great vessels of an anomalous right coronary artery arising in common with a left coronary artery from above the left sinus of Valsalva. Catheterization and Cardiovascular Diagnosis, 25, 46–51.
View at Publisher | View at Google Scholar - Lim, J.,C., Beale, A.., Ramcharitar, S (2011) Anomalous origination of a coronary artery from the opposite sinus. Nature Reviews Cardioliogy. 8, 706–719.
View at Publisher | View at Google Scholar - Angelini, P., Walmsley, R., Cheong, B.,Y., Ott, D.,A (2010) Left main coronary artery originating from the proper sinus but with acute angulation and an intramural course, leading to critical stenosis. Texas Heart Institute Journal, 37, 221–225.
View at Publisher | View at Google Scholar - Jegatheeswaran, A., Devlin, P.,J., McCrindle, B.,W., Williams, W.,G., Jacobs, M.,L., Blackstone, E.,H., et al (2019).Features associated with myocardial ischemia in anomalous aortic origin of a coronary artery: a congenital heart surgeons' society study. Journal of Thoracic and Cardiovascular Surgery, 158, 822–834.e3.
View at Publisher | View at Google Scholar - Kaushal, S., Backer, C.,L., Popescu, A.,R., Walker, B.,L., Russell, H.,M., Koenig, P.,R., et al (2011)Intramural coronary length correlates with symptoms in patients with anomalous aortic origin of the coronary artery. Annals of Thoracic Surgery, 92, 986–991.
View at Publisher | View at Google Scholar - Harris, M.,A., Whitehead, K.,K., Shin, D.,C., Keller, M.,S., Weinberg, P.,M., Fogel, M., A (2015) Identifying abnormal ostial morphology in anomalous aortic origin of a coronary artery. Annals of Thoracic Surgery, 100, 174–179.
View at Publisher | View at Google Scholar - Angelini, P., Flamm, S.,D. (2007) Newer concepts for imaging anomalous aortic origin of the coronary arteries in adults. Catheterization and Cardiovascular Interventions, 69, 942–954.
View at Publisher | View at Google Scholar - Boler, A.,N., Hilliard, A.,A., Gordon, B.,M (2017) Functional assessment of anomalous right coronary artery using fractional flow reserve: an innovative modality to guide patient management. Catheterization and Cardiovascular Interventions, 89:316–320.
View at Publisher | View at Google Scholar - Pijls, N.,H., Van Gelder, B., Van der Voort, P., Peels, K., Bracke, F.,A., Bonnier, H.,J., et al (1995).Fractional flow reserve. A useful index to evaluate the influence of an epicardial coronary stenosis on myocardial blood flow. Circulation, 92, 3183–3193.
View at Publisher | View at Google Scholar - Uebleis, C., Groebner, M., Von Ziegler, F., Becker, A., Rischpler, C., Tegtmeyer, R., et al(2012) Combined anatomical and functional imaging using coronary CT angiography and myocardial perfusion SPECT in symptomatic adults with abnormal origin of a coronary artery. International Journal of Cardiovascular Imaging, 28,1763–1774.
View at Publisher | View at Google Scholar - Angelini, P., Uribe, C., Monge, J., Tobis, J.,M., Elayda, M/.A, Willerson, J.,T (2015). Origin of the right coronary artery from the opposite sinus of Valsalva in adults: characterization by intravascular ultrasonography at baseline and after stent angioplasty. Catheterization and Cardiovascular Interventions, 86, 199–208.
View at Publisher | View at Google Scholar - Bigler, M.,R., Ashraf, A., Seiler, C., Praz, F., Ueki, Y., Windecker, S., Kadner, A., Räber, L.., Gräni, C (2021) Hemodynamic Relevance of Anomalous Coronary Arteries Originating From the Opposite Sinus of Valsalva-In Search of the Evidence. Frontiers in Cardiovascular Medicine. 7, 591326.
View at Publisher | View at Google Scholar - Bogaty, P., et al (2003) What induces the warm-up ischemia/angina phenomenon: exercise or myocardial ischemia? Circulation, 107, 1858–1863.
View at Publisher | View at Google Scholar - Williams, R.,P., et al (2014)'Warm-up Angina': harnessing the benefits of exercise and myocardial ischaemia, Heart, 100, 106-114.
View at Publisher | View at Google Scholar - Angelini, P., Velasco, J.,A., Flamm, S..(2002) Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation, 105, 2449–2454
View at Publisher | View at Google Scholar
