

Case report | DOI: https://doi.org/10.31579/2835-8325/076
Tinea faciei as the main mimicker of cutaneous lupus erythematosus
1 Sr. Professor & Head, Daswani Dental College, Kota, Rajasthan, India.
2 Associate Professor, Daswani Dental College, Kota, Rajasthan, India.
*Corresponding Author: Cesar Bimbi, Private clinic/ Brazilian Society of Dermatology, Brazil.
Citation: Cesar Bimbi, Piotr Brzezinski, Bastos Gomes AC, (2024), Tinea faciei as the main mimicker of cutaneous lupus erythematosus, Clinical Research and Clinical Reports, 4(3); DOI:10.31579/2835-8325/076
Copyright: © 2024, Cesar Bimbi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 May 2024 | Accepted: 27 May 2024 | Published: 14 June 2024
Keywords: fungal infection; skin lesions; dermatophytic infection
Abstract
Tinea faciei (TF) may be clinically deceptive and as many as 70% of patients with this relatively uncommon dermatophytic infection are initially misdiagnosed as having other dermatoses.
Introduction
Tinea faciei (TF) may be clinically deceptive and as many as 70% of patients with this relatively uncommon dermatophytic infection are initially misdiagnosed as having other dermatoses. TF can masquerade convincingly as lupus, especially when incognito, a clinical presentation modified by erroneous treatment with corticosteroids (systemic or topical), which presents as multiple polycyclic annular lesions. Occasionally, the fungal infection itself produces discoid lupus erythematosus-like lesions resembling a malar butterfly rash from the start. Uncertainty raises as tinea and lupus may also share the same histological patterns.
As a result, this fungal infection should be considered as part of the so-called lupus mimickers. These consist of a group of diseases exhibiting clinical and laboratory characteristics resembling those present in patients with LE.
Case 1
A 58-year-old male, visited our department with multiple polycyclic lesions over the face, neck and upper chest present for six months Figure 1. An initial laboratory evaluation revealed a positive ANA (1/80) which (along with the skin manifestations) had been taken for lupus. He had been using prednisone 40 mg/day for this diagnosis. After initial improvement, the rash worsened and rapidly progressed. Considering that he was not improving treatment-wise, the general practitioner sent the patient to our office for the assessment of the skin lesions. Scrapings were collected and Trichophyton rubrum grew out in fungal culture displaying typical white cottony colonies. The patient was treated with 250 mg of terbinafine daily for 1 month and topical miconazole resulting in progressive and complete regression of the lesions.

Figure 1: Butterfly-like polycyclic lesions over the face, neck and upper chest simulating lupus erythematosus
Case 2
A 11-year-old girl presented to our institution with skin lesions on periocular skin (Fig 2). that have appeared for three months. Prior failed therapies were hydrocortisone and acyclovir, both topical. At presentation, there was an erythematous desquamative patch on right lower eyelid. Contact dermatitis and LE were suspected suspected clinically. Scrapings were collected and multiple fungal hyphae were seen. These were grown in culture where Trichophyton rubrum grew. The infection was resolved in 12 days with topical miconazole.

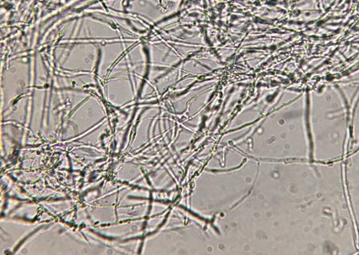
Figure 2a: LE-like mycosis on right lower eyelid and nose. Lupus erythematosus of the periorbita occurs in 6% of lupus patients.
Figure 2b Fungal hyphae and conidia were detected in skin scrapings diluted in potassa.
Keywords: Tinea faciei; dermatophyte; lupus erythematosus
Case 3
A 73-year-old man presented a facial rash on non-bearded regions of the face and was treated firstly as lupus eruption with prednisone (20 mg daily) but for no improvement. Then, antibiotics for presumed rosacea was tried, also unsuccessfully. Physical examination revealed extensive erythematous lesions on the face with some pustules. Figure3 Blood, urine, hepatorenal function and immunity tests were all normal. Scrapings of the lesions border showed hyphae and itraconazole 200mg cleared the face lesions.
Discussion
Our case series show that superficial fungal infections can masquerade convincingly as lupus. Superficial fungal infections are trivial diagnosis in dermatology. In the case of facial dermatophytosis, the peculiar physiology of the face, washing and asepsis, and a myriad of beauty cosmetics currently been placed on the face often produce atypical clinical features and profound dilemmas. The patient's false beliefs that corticosteroid creams are useful (as a relief may happen on the first applications) usually produce deceptive “incognito” clinical patterns.
As many as 70% of patients with tinea faciei are initially misdiagnosed as having other dermatoses. In a 20-year survey of tinea faciei, Nicola et al [2] examined 107 cases of tinea faciei demonstrating that typical forms were 57.1% whereas 42.9% were variants mainly mimicking discoid lupus erythematosus (9 cases), polymorphous light eruption (8 cases) and rosacea-like presentations. Uncertainty raises as tinea and lupus may sometimes share the same histological patterns and the presence of antinuclear antibodies (ANA) is a common finding in healthy people, especially the elderly. Although the search for auto-antibodies towards nuclear antigens is a key step in the diagnosis strategy, it sometimes adds a confounding factor keeping in mind that ANAs are not specific for SLE.
Herein, we present cases of patients who came to department complaining of chronic and difficult to diagnose facial rash and a plain direct mycologic microscope examination was all that was necessary to reach correct diagnosis. A microscope had his role a few decades ago as an indispensable tool to any dermatological office and it is now certainly the time for this valuable, cheap and easy device to return to everyday clinical practice.
The authors recommend that clinicians should be vigilant in patients presenting erythematous lesions of the face for this common differential diagnosis of lupus and consider early direct mycologic exam when suspicion deserves.
References
- Sharifzadeh A, Erfanmanesh A, Chalangari R, Safaei-Naraghi Z, Safar F. (2012). Severe tinea corporis due to Trichophyton verrucosum mimicking discoid lupus erythematosus. J Mycol Med, 22(1):92-95.
View at Publisher | View at Google Scholar - Nicola A, Laura A, Natalia A, Monica P. (2010). A 20-year survey of tinea faciei Mycoses [serial online], 53: 504-508.
View at Publisher | View at Google Scholar - Gupta T, Beaconsfield M, Rose GE, Verity DH. (2012). Discoid lupus erythematosus of the periorbita: clinical dilemmas, diagnostic delays. Eye (Lond). 2012 Apr;26(4):609-612.
View at Publisher | View at Google Scholar
