

Case report | DOI: https://doi.org/10.31579/2834-796X/094
The use of Merit Wrapsody® Covered stent for Aortoiliac Disease: An Innovative Device off the shelf
- Cristiano Torres Bortoluzzi 1
- Pierre Galvagni Silveira 1
- Rafael Narciso Franklin 1
- Rafael de Athayde Soares 2*
1Hospital Baía Sul, Florianópolis, Santa Catarina.
2Hospital do Servidor Público Estadual de São Paulo, Iamspe.
*Corresponding Author: Rafael de Athayde Soare, Hospital do Servidor Público Estadual de São Paulo, Iamspe.
Citation: Cristiano T. Bortoluzzi, Pierre G. Silveira, Rafael N. Franklin, Rafael de Athayde Soares, (2025), The use of Merit Wrapsody® Covered stent for Aortoiliac Disease: An Innovative Device off the shelf, International Journal of Cardiovascular Medicine, 4(2); DOI:10.31579/2834-796X/094
Copyright: © 2025, Rafael de Athayde Soare. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 February 2025 | Accepted: 24 February 2025 | Published: 07 March 2025
Keywords: aortoiliac disease;iliac artery; wrapsody endoprosthesis
Abstract
In this paper, we aimed to report the use of Merit Wrapsody® for aortoiliac disease. We describe a case series of reports of 8 patients submitted to endovascular repair with Merit Wrapsody® for aortoiliac disease. Merit Wrapsody® are flexible self-expanding endoprosthesis indicated for use in hemodialysis patients for the treatment of stenosis or occlusion within the dialysis outflow circuit of an arteriovenous (AV) fistula or AV graft, consisting of Nitinol, ePTFE, PTFE structure. In a case series communication, we aimed to describe the feasibility of a PTFE-lined stent for percutaneous treatment of conditions other than AV fistula obstruction. We report the successful use of Wrapsody to percutaneously treat several arterial vascular conditions, including post-endovascular procedure common iliac artery rupture, Covered Endovascular Reconstruction of the Aortic Bifurcation or CERAB technique and kissing iliac stenting, This case series illustrates the feasibility of the "off-label" use of self-expanded Wrapsody endoprosthesis to percutaneously treat arterial pathology conditions, specially aortoiliac territory with satisfactory and excellent results.
Introduction
Covered stents formerly have been reserved for arteriovenous fistulas, iliac aneurysms, or iatrogenic perforations and ruptures. However, recent studies have provided encouraging results of covered stents compared with bare metal stents for aortoiliac occlusive disease. Several covered stents have been used with technical success for aortoiliac occlusive disease. Most of these stents are made of stainless steel (Atrium Advanta V12, Gore Viabahn VBX, Bard LifeStream) whereas others are made of cobalt chromium (Bentley BeGraft Aortic, Hechingen, Germany). The design of these stents differs significantly and the way the covering material is applied differs from polytetrafluoroethylene on both sides of the stent (Advanta, VBX, LifeStream) or an external layer only (BeGraft).[1]
Merit Wrapsody is a flexible self-expanding endoprosthesis indicated for use in hemodialysis patients for the treatment of stenosis or occlusion within the dialysis outflow circuit of an arteriovenous (AV) fistula or AV graft, consisting of Nitinol, ePTFE, PTFE structure. Several papers showed encouraging results regarding the target lesion primary patency at 30 days of 100% (45 45 patients had reached 30 days of follow-up). The target lesion primary patency for the patients who had completed 12 months of follow-up was 84.6% (33 of 39).[2,3] Indeed, despite the massive use of Wrapsody in venous obstructions, there is a case report published showing satisfactory results of the use of Wrapsody in popliteal artery aneurysms, with 1-year follow-up.[4]
In this study, we aimed to report the use of Merit Wrapsody® for aortoiliac disease in a case series (8 patients).
Case Presentations
Case 1
A male patient, 70 years, with hypertension and dyslipidemia, was admitted with an asymptomatic infrarenal abdominal aortic saccular aneurysm, measuring 3,6cm. The patient was submitted to endovascular treatment with the aortic implant of endoprosthesis Jotec E-Tegra® 22x22x80mm, followed by implant of Wrapsody 60x12x120mm at left common iliac artery and Wrapsody 60x12x120mm right common iliac artery, communicating with the aortic endoprosthesis. After that, it was performed a kissing balloon at both common iliac arteries with a catheter balloon 10x60mm. The final image showed excellent results with no endoleaks. (Figure 1). The patient was discharged from the hospital on the first day post-operative and 1-month follow-up showed endoprosthesis patency with no endoleaks.

Figure 1: Aortic implant of endoprosthesis Jotec E-Tegra® 22x22x80mm, followed by implant of Wrapsody 60x12x120mm at left common iliac artery and Wrapsody 60x12x120mm right common iliac artery, communicating with the aortic endoprosthesis.
Case 2
Male patient, 76 years, with a history of endovascular repair of aortic abdominal aneurysm (EVAR) evolved with endoprosthesis right limb occlusion, associated with disabling claudication. Due to this important symptom, the patient was scheduled to undergo an endovascular procedure with right limb recanalization and implant of Wrapsody 14x80mm at the infra-renal aorta and right common iliac artery, followed by the implant of Wrapsody 14x80mm at the right common iliac artery and another Wrapsody 16x80mm at iliac bifurcation (Snorkel Technique). The left limb was also treated to perform a Kissing Stent with the implant of Viabahn 13x100mm. (Figure 2). The patient was discharged from the hospital first day post-operative and 1 one-month follow-up showed endoprosthesis patency and no endoleaks with complete resolution of the previous disabling claudication.
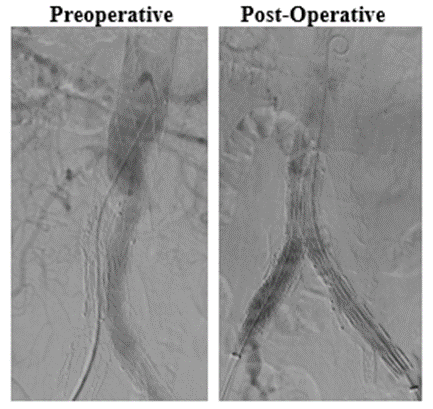
Figure 2: Right limb recanalization and implant of Wrapsody 14x80mm at the infra-renal aorta and right common iliac artery, followed by the implant of Wrapsody 14x80mm at the right common iliac artery and another Wrapsody 16x80mm at iliac bifurcation (Snorkel Technique).
Case 3
A female patient, 71 years old, active smoker, with arterial hypertension and diabetes, was admitted with right inferior limb rest pain. The patient was submitted to Angioct-Scan which demonstrated common iliac arteries bilateral occlusion. The patient was submitted to endovascular surgery with
an iliac kissing stent and implant of Wrapsody 8x50mm at the right common iliac artery and Wrapsody 7x75mm at the left common iliac artery, followed by post-dilatation with a catheter balloon. (Figure 3). The patient was discharged from the hospital first day post-operative and 1-month follow-up showed endoprosthesis patency with complete resolution of the previous symptoms.

Figure 3: Iliac kissing stent and implant of Wrapsody 8x50mm at the right common iliac artery and Wrapsody 7x75mm.
Case 4
Male patient, 72 years, active smoker, with arterial hypertension, diabetes, and disabling bilateral inferior limbs claudication. The patient was submitted to endovascular surgery with an iliac kissing stent and implant of Wrapsody 9x50mm at the right iliac common artery and Wrapsody 9x75mm at the left common iliac artery, followed by post-dilatation with a catheter balloon. (Figure 4) The patient was discharged from the hospital first day post-operative and 1-month follow-up showed endoprosthesis patency with complete resolution of the previous symptoms.
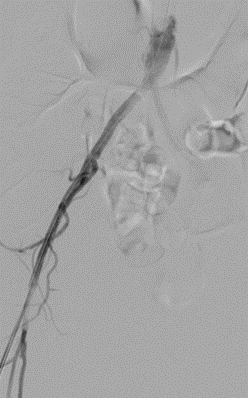
Figure 4: Iliac kissing stent and implant of Wrapsody 9x50mm at the right iliac common artery and Wrapsody 9x75mm at the left common iliac artery.
Case 5
A male patient, 61 years old, obese, active smoker, with arterial hypertension and diabetes, was admitted with right inferior disabling claudication. AngioCT-Scan showed distal aorta and right iliac common artery stenosis (Figure 5). The patient was scheduled to undergo endovascular surgery with covered endovascular reconstruction of aortic bifurcation (CERAB) technique, using Wrapsody 16x40mm implanted at distal aorta, Wrapsody 10x50mm implanted at distal aorta and left common iliac artery associated to Wrapsody 9x50mm at distal aorta and right common iliac artery, followed by post-dilatation with catheter balloon. The patient was discharged from the hospital first day post-operative and 1-month follow-up showed endoprosthesis patency with complete resolution of the previous symptoms.

Figure 5: AngioCT-Scan showed distal aorta and right iliac common artery stenosis.
Case 6
A male patient, 59 years old, with arterial hypertension, ischemic heart disease, active smoker was admitted with left inferior limb disabling claudication. AngioCT-Scan showed distal aorta and complete left iliac common and external artery occlusion. The patient was submitted to left femoral common artery endarterectomy and profundoplasty followed by complete recanalization of the left iliac common and external artery occlusion with Wrapsody 8x125mm and 7x75mm respectively. (Figure 6). The patient was discharged from the hospital second day post-operative and 1-month follow-up showed endoprosthesis patency with complete resolution of the previous symptoms.
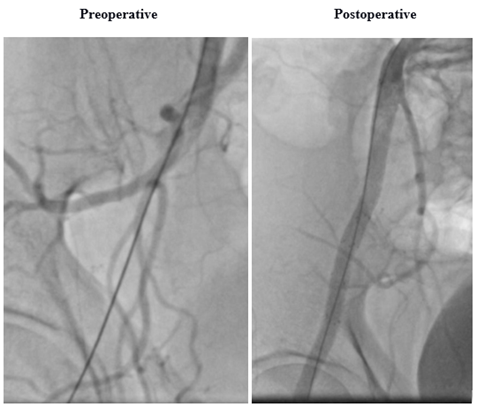
Figure 6: Left Femoral common artery endarterectomy and profundoplasty followed by complete recanalization of the left iliac common and external artery occlusion with Wrapsody 8x125mm and 7x75mm respectively.
Case 7
A male patient, 72 years, obese, active smoker, with arterial hypertension and dyslipidemia was admitted with bilateral inferior limbs rest pain. The patient was submitted to an iliac kissing stent with the implant of Wrapsody 10x75mm at the right iliac common artery and Wrapsody and Wrapsody 10x75 at the left iliac common artery. Furthermore, both external iliac arteries were also treated with the implant of Wrapsdoy 9x100mm and 9x50mm at the right and left external iliac arteries respectively. The patient was discharged from the hospital first day post-operative and 1-month follow-up showed endoprosthesis patency with complete resolution of the previous symptoms.

Figure 7: Iliac kissing stent with the implant of Wrapsody 10x75mm at the right iliac common artery and Wrapsody and Wrapsody 10x75 at the left iliac common artery.
Case 8
A male patient, 84 years old, was submitted to a Transfemoral Transcatheter Aortic Valve Replacement (TAVI) due to cardiac valvulopathy. During the procedure, the patient had an iatrogenic right external and common iliac artery dissection and rupture, associated with hemorrhagic shock. Promptly our vascular team was called and intervened to solve the vascular complication with an implant of Wrapsody 8x75mm and 8x50mm at common and external iliac arteries respectively followed by post-dilatation catheter-balloon (Figure 8). The patient evolved very well, with complete resolution of the complication and stabilization, being discharged from the hospital three days after the procedure.

Figure 8: Implant of Wrapsody 8x75mm and 8x50mm at common and external iliac arteries respectively
Discussion
This paper presents a challenging case series report of patients with aortoiliac disease, including iliac rupture, aorta abdominal aneurysm, and aortoiliac occlusive disease treated with a new device covered stent Wrapsody. The past two decades have witnessed a paradigm shift to endovascular strategies as the preferred treatment for mild-to-moderate aortoiliac occlusive disease (AIOD).5 Covered stents may be optimal for complex lesions, particularly those involving aortic bifurcation, due to the high risk of rupture related especially to heavily calcified arteries. A covered stent or stent graft is a metal stent lined with polytetrafluoroethylene (PTFE) or Dacron.
Currently, available covered stents for the iliac arteries include both self-expanding and balloon-expandable platforms. Recently, a prospective evaluation of the Viabahn stent in 61 iliac arteries provided primary patency rates for the iliac arteries of 98% at 6 months and 91% at 12 months. The mean lesion length was 6.9 cm. Primary technical success, with correct placement and antegrade flow through the prosthesis, was achieved in all patients. Embolization to distal arteries was observed after stent graft placement in two out of five cases where an iliac artery occlusion was treated. No device- or procedure-related deaths were reported.[6]
The Covered Versus Balloon-Expandable Stent Trial (COBEST) was a prospective, multicenter, randomized controlled trial that included 125 patients (168 iliac arteries) with severe iliac occlusive disease who were randomized to receive either the V12-covered balloon-expandable stent (which is similar to the current iCAST stent) or a bare-metal stent (BMS). Lesions treated with a covered stent were significantly more likely to remain free from binary restenosis compared to those treated with a BMS (hazard ratio [HR]: 0.35; 95% confidence interval [CI]: 0.15–0.82). Freedom from occlusion was not statistically different (HR: 0.28; 95% CI: 0.07–1.09). Subgroup analyses demonstrated a significant improvement in freedom from binary restenosis for covered stents in TASC C and D lesions (HR: 0.14; 95% CI: 0.04–0.44). There was also a lower rate of repeat revascularization in the covered stent group compared with the BMS group (odds ratio [OR]: 0.21; 95% CI: 0.07–0.64). Most of the reinterventions were performed between 12 months and 18 months. The amputation rate was similar and low between the two groups.[7]
The Merit Wrapsody® is a self-expandable covered stent consisting of Nitinol, ePTFE, and PTFE structure. Self-expanding stents are better suited for tortuous vessels, especially in areas of permanent external forces such as the external iliac artery. These stents guarantee precise placement only on the end that is deployed first, but newer-generation nitinol self-expanding stents exhibit minimal foreshortening at human body temperature and have a more predictable length once deployed in the body. As a rule, the leading end of the device is always maneuvered just past the planned landing zone, allowing for fine adjustments and retraction during its deployment.9 Given the PTFE lining, covered stents may overcome some limitations of standard stent designs by introducing a mechanical barrier between intimal hyperplasia and the arterial lumen. This covering potentially also prevents the migration of macrophages in the vascular wall, which are attracted by proinflammatory mediators secreted by the damaged vessel wall. These
macrophages release further cytokines, metalloproteinases, and growth factors that contribute to the initiation of the restenotic process.[9]
There was 1 case in this present paper where we used the CERAB technique to perform an endovascular treatment of the aortoiliac occlusive disease. Indeed, this technique involves the placement of a PTFE-covered stent expanded in the distal aorta with two additional kissing-covered balloon-expandable stents extending from the distal aorta into the common iliac arteries, endovascularly reconstructing the aortoiliac bifurcation.10 Grimme et al10 described a 95.1% technical success rate with primary patency rates of 87 and 82% at 1 and 2 years, respectively, and secondary patency rates of 95% through 2 years of follow-up. In a later retrospective multicenter analysis by Saratzis et al11 in 2021 which included 116 TASC D lesions treated with CERAB, the authors found primary patency, assisted primary patency, and secondary patency rates of 88, 94, and 98%, respectively. These studies demonstrate the effectiveness of CERAB as a potential initial intervention for aortoiliac disease, especially in patients with high associated surgical risk.
There was one case reported in this present cohort that had an iliac artery rupture during the TAVI procedure. The patient was submitted to a successfully covered stent implant. In cases that evolved with rupture, endovascular treatment has advantages over open surgery because it does not require the clamping of blood vessels and sutures of calcified vessels.12 Several endovascular techniques can be utilized for iliac artery rupture, such as balloon tamponade, a coagulated thrombus injection, and stent graft placement.13,14 If the rupture was confirmed during the procedure, temporary hemostasis should be performed through a balloon tamponade while preparing the covered stent or endograft, which has been mentioned in previous studies as well.
This case report has some limitations since it is a case series report, with no long-term follow-up. Larger studies should be performed in order to evaluate the safety and efficacy of endovascular treatment with Merit Wrapsody® for aortoiliac occlusive disease.
Conclusion
Endovascular treatment with Merit Wrapsody® covered stents for aortoiliac disease seems to be a safe and effective alternative for patients with chronic limb-threatening ischemia, aortic aneurysm, and iliac rupture. Further and more robust studies are needed to validate these preliminary results.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The Authors declare that there is no conflict of interest regarding this paper.
Informed consent has been obtained from the patient for publication of the case report and accompanying images.
References
- Reijnen M.M.P.J. (2020). Update on covered endovascular reconstruction of the aortic bifurcation. Vascular. 28:225–232.
View at Publisher | View at Google Scholar - Gilbert J. Prospective First-in-Human Study of the Merit WRAPSODY Endovascular Stent Graft for Treatment of Access Circuit Outflow Stenosis in Hemodialysis Patients. Journal of Vascular Surgery Abstracts 7S Volume 75, Number 4S.
View at Publisher | View at Google Scholar - Gilbert J, Rai J, Kingsmore D, Skousen J, Ptohis N. (2021). First Clinical Results of the Merit WRAPSODY™ Cell-Impermeable Endoprosthesis for Treatment of Access Circuit Stenosis in Haemodialysis Patients. Cardiovasc Intervent Radiol. Dec;44(12):1903-1913.
View at Publisher | View at Google Scholar - de Athayde Soares R, Cury MVM, Futigami AY (2024). Popliteal Artery Aneurysm Treated with Endovascular Technique and New Device: Case Report and Literature Review. JSM Heart Surg Case Images 4(1): 1012.
View at Publisher | View at Google Scholar - Norgren, L. ∙ Hiatt, W.R. ∙ Dormandy, J.A. TASC II Working Group Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) J Vasc Surg. 2007; 45:S5-S67
View at Publisher | View at Google Scholar - GORE® VIABAHN® Endoprosthesis [webpage on the Internet] GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface. [Accessed July 25, 2015].
View at Publisher | View at Google Scholar - Mwipatayi BP, Thomas S, Wong J, et al. (2011). Covered Versus Balloon Expandable Stent Trial (COBEST) Co-investigators A comparison of covered vs bare expandable stents for the treatment of aortoiliac occlusive disease. J Vasc Surg. 54:1561–1570.
View at Publisher | View at Google Scholar - Javed U, Balwanz CR, Armstrong EJ, et al. (2013). Mid-term outcomes following endovascular re-intervention for iliac artery in-stent restenosis. Catheter Cardiovasc Interv. 82:1176–1184.
View at Publisher | View at Google Scholar - Jongkind V, Akkersdijk GJ, Yeung KK, Wisselink W. (2010). A systematic review of endovascular treatment of extensive aortoiliac occlusive disease. J Vasc Surg. 52:1376–1383.
View at Publisher | View at Google Scholar - Grimme F AB, Goverde P CJM, Verbruggen P JEM, Zeebregts C J, Reijnen M M. (2015). Editor's choice – first results of the covered endovascular reconstruction of the aortic bifurcation (CERAB) technique for aortoiliac occlusive disease. Eur J Vasc Endovasc Surg. 50(05):638–647.
View at Publisher | View at Google Scholar - Saratzis A, Salem M, Sabbagh C. (2021). Treatment of aortoiliac occlusive disease with the covered endovascular reconstruction of the aortic bifurcation (CERAB) technique: results of a UK multicenter study. J Endovasc Ther. 28(05):737–745.
View at Publisher | View at Google Scholar - Duran C, Naoum JJ, Smolock CJ, Bavare CS, Patel MS, Anaya-Ayala JE, et al. (2013). A longitudinal view of improved management strategies and outcomes after iatrogenic iliac artery rupture during endovascular aneurysm repair. Ann Vasc Surg. 27:1–7.
View at Publisher | View at Google Scholar - Nyman U, Uher P, Lindh M, Lindblad B, Brunkwall J, Ivancev K. (1999). Stent-graft treatment of iatrogenic iliac artery perforations: report of three cases. Eur J Vasc Endovasc Surg. 17:259–263.
View at Publisher | View at Google Scholar - Scheinert D, Ludwig J, Steinkamp HJ, Schröder M, Balzer JO, Biamino G. (2000). Treatment of catheter-induced iliac artery injuries with self-expanding endografts. J Endovasc Ther. 7:213–220.
View at Publisher | View at Google Scholar
