

Case report | DOI: https://doi.org/10.31579/2834-796X/091
The use of a new device for an endoconduit for EVAR: an innovative technique off the shelf
- Rodolfo Marques Mansano 1
- Elias Arcênio Neto 1
- Paulo Fernando Gasparetto 1
- Rodrigo Eik Sahyun 1
- Igor Shincariol Perozin 1
- Ana Júlia de Souza Alfieri 1
- Diego Castro Musial 1
- Rafael de Athayde Soares 2
1Hospital Evangélico de Londrina
2Hospital do Servidor Público Estadual de São Paulo, IAMSPE
*Corresponding Author: Rafael de Athayde Soares, 2Hospital do Servidor Público Estadual de São Paulo, IAMSPE.
Citation: Rodolfo M. Mansano, Elias A. Neto, Paulo F. Gasparetto, Rodrigo E. Sahyun, and Igor S. Perozin et.al (2025), The use of a new device for an endoconduit for EVAR: an innovative technique off the shelf, International Journal of Cardiovascular Medicine, 4(1); DOI:10.31579/2834-796X/091
Copyright: © 2025, Rafael de Athayde Soares. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 January 2025 | Accepted: 27 January 2025 | Published: 17 February 2025
Keywords: popliteal artery, endovascular surgery, popliteal artery aneurysm.
Abstract
In this paper, we aimed to report using a new device for an endoconduit for EVAR. An 89-year-old male patient, an active smoker with hypertension, and a history of punctiform lesion at the left inferior limb toe associated with rest pain was admitted with an asymptomatic aorta aneurysm measuring 57.3 mm. The patient was submitted to a CT angiogram, that showed the combination of Trans-Atlantic Intersociety Consensus (TASC) D aortoiliac occlusive disease as well as a symptomatic abdominal aortic aneurysm (AAA). Then, the patient was scheduled to undergo endovascular treatment of the aorta aneurysm with two covered self-expandable 12x80 and 10x80 Merit Wrapsodyâ implanted in both right iliac common and external iliac arteries respectively used as an endoconduit to allow the aorta endoprosthesis implant. After that, a Herculesâ monoiliac endograft 30x140x14 was implanted at the aorta below the renal arteries, followed by a right-left femoral-femoral bypass with PTFE 8mm. The patient was discharged from the hospital two days after the surgery with no complications, palpable pedal pulses taking aspirin 100mg and Clopidogrel 75mg daily. At year follow-up the patient was asymptomatic and duplex showed patent stent without evidence of endoleak.
Introduction
Challenging aortoiliac anatomy continues to be one of several limiting factors in the applicability of endovascular aortic repair (EVAR) to all patients with abdominal aortic aneurysm (AAA), especially in patients with the combination of Trans-Atlantic Intersociety Consensus (TASC) D aortoiliac occlusive disease as well as a symptomatic abdominal aortic aneurysm (AAA). Among the factors related to challenging aortoiliac anatomy extensive, calcified atherosclerotic disease, occlusions, and small iliofemoral segmental arteries make transfemoral access difficult for EVAR.[1]
Various techniques have been described in the literature to modify the iliac anatomy to render it suitable for delivering stent-grafts in EVAR. These include simple dilation of the iliofemoral segmental vasculature using over-the-wire dilators, balloon angioplasty, endoluminal balloon endarterectomy, direct retroperitoneal iliac conduits, and the internal endoconduit.[2] All but direct iliac conduits and the endoconduit have the disadvantage of being uncontrolled and carry the devastating complications of iliac dissection or free iliac artery rupture.
In this study, we aimed to report the use of a new device for an endoconduit for EVAR in a patient with chronic limb-threatening ischemia.
Case Report
In this paper, we aimed to report the use of a new device for an endoconduit for EVAR. An 89-year-old male patient, an active smoker with hypertension, and a history of punctiform lesion at the left inferior limb toe associated with rest pain was admitted with an asymptomatic aorta aneurysm measuring 57.3 mm. On physical examination, he had good general health, with no femoral, popliteal, and tibial pulses palpable bilaterally and punctiform gangrene at the left limb 5th toe. The patient was submitted to a computed tomography angiography (CTA) of the thorax, abdomen, and pelvis that showed an aortic aneurysm measuring 57mm, right iliac arteries stenosis, and left iliac artery total occlusion (Figures 1, 2 and 3). Due to TASC D at iliac arteries and an aortic aneurysm, the team decided to revascularize the left limb through an endovascular approach with an endoconduit at right iliac arteries, EVAR to treat the aortic aneurysm and a right femoral-left femoral bypass with prosthesis.
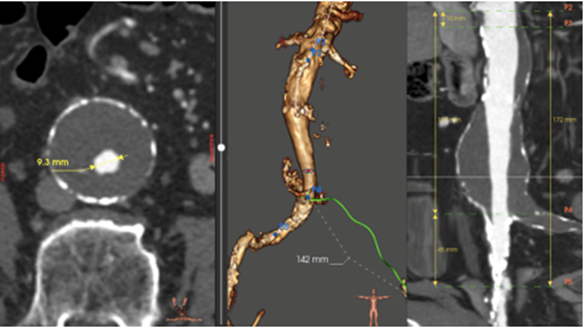
Figure 1: Angio-CT scan demonstrating aortic aneurysm measuring 57mm, right iliac arteries stenosis and left iliac artery total occlusion
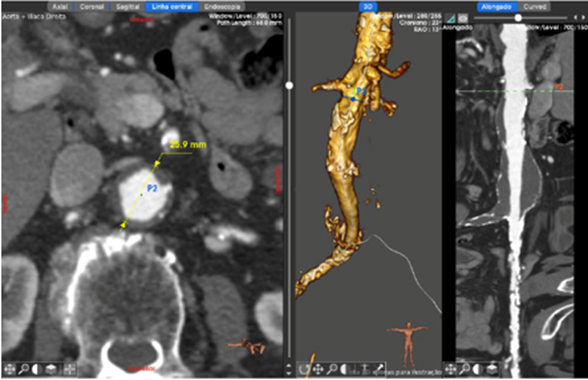
Figure 2: Angio-CT scan demonstrating aortic aneurysm measuring 57mm, right iliac arteries stenosis and left iliac artery total occlusion.
Under general anesthesia, the operation was performed with bilateral femoral artery cutdowns, exposing the right common femoral artery for delivery of the stent graft. The left brachial artery was punctured with a 5F 11cm introducer, and a pigtail 5F through a 0,035”260cm SPLASHâ guidewire placed at the abdominal aorta was used to perform image control (figures 3 and 4).
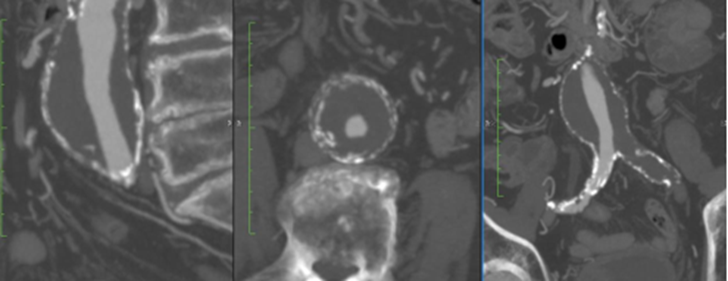
Figure 3: Angio-CT scan demonstrating aortic aneurysm measuring 57mm with narrowing lumen and important stenosis

Figure 3: Preoperative arteriography showing right iliac artery stenosis
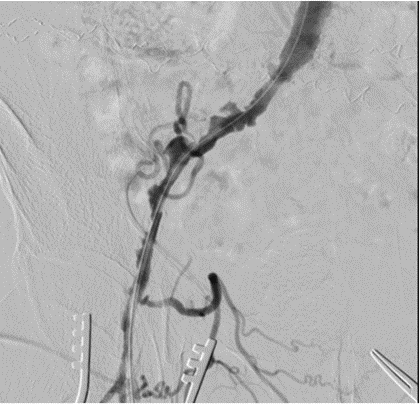
Figure 4: Preoperative arteriography showing right iliac artery stenosis
The patient was heparinized with a 5000UI intravenous bolus. We punctured the right femoral artery with an introducer 12 F and performed a balloon angioplasty at the common and external right iliac arteries with a 10x80 MAGNUSâ catheter balloon. After proper evaluation, two covered self-expandable 12x80 and 10x80 Merit Wrapsodyâ were placed under roadmap into the common iliac artery and external iliac artery respectively, and post-dilatated with a 10x80 and 12x80 catheter balloon MAGNUSâ to create an endoconduit (figure 5).

Figure 5: Post-operative image of endovascular treatment of the aorta aneurysm with two covered self-expandable 12x80 and 10x80 Merit Wrapsody implanted in both right iliac common and external iliac arteries respectively used as an endoconduit to allow the aorta endoprosthesis implant.
After the creation of the endo conduit, we placed a 14F introducer at the right common femoral artery to deploy the infra-renal endoprosthesis 30x140x14 HERCULESâ associated with the accommodation balloon. Control angiography showed the proper position of the endoprosthesis with no endoleaks. After that, we performed a right femoral-left femoral bypass with PTFE 8. The control angiography demonstrated a right external iliac artery dissection and profundal femoral artery stenosis, which were corrected with the deployment of a WRAPSODYâ 8x50 at the iliac external artery and profunda artery angioplasty with catheter balloon 4x100 MAGNUSâ. The final image demonstrated a satisfactory result with no endoleaks and prosthesis patent (figures 6 and 7). The patient was transferred to the nursery room, being discharged from the hospital two days after the surgery with no complications, femoral pulses present bilaterally, taking aspirin 100mg and Clopidogrel 75mg/day. After 1 month the patient was evaluated, presenting no further symptoms with proper ulcer healing and an ankle brachial index of 0,58 (previous was inaudible).
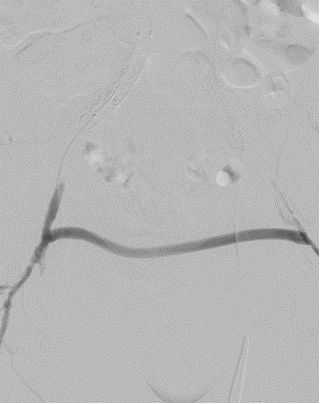
Figure 6: Post-operative image of Herculesâ monoiliac endograft 30x140x14 was implanted at the aorta below the renal arteries, followed by a right-left femoral-femoral bypass with PTFE 8mm.
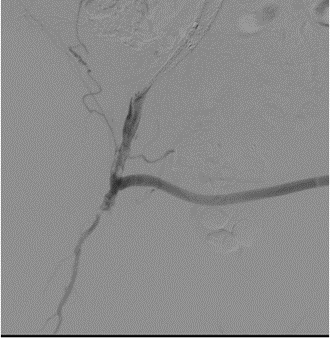
Figure 7: Post-operative image of Herculesâ monoiliac endograft 30x140x14 was implanted at the aorta below the renal arteries, followed by a right-left femoral-femoral bypass with PTFE 8mm.
Discussion
This paper presents a challenging case report of a patient with chronic limb-threatening ischemia associated with an asymptomatic aortic aneurysm. The applicability of endovascular aneurysm repair (EVAR) is often limited by ilio-femoral occlusive disease,[3] which was observed in this case report. The placement of covered stents in the iliac arteries as end conduits (EC) with dilation to large diameters causing controlled rupture of the access vessels is known as the “pave and crack” technique.[4] The advantage of the pre-emptive use of covered stents lies in protecting against extensive dissection and even more importantly in avoiding the hemodynamic instability associated with possible rupture.
The endoconduit was first described by Yano et al2 in 2001 as an alternative approach to difficult iliofemoral anatomy in stent-graft repairs of aortic aneurysms. As originally described, the endo conduit is composed of a PTFE graft sewn onto a self-expanding metallic stent, which was then backloaded onto a delivery system. This covered stent was then deployed into the common iliac artery and, when necessary, extended into the external iliac artery. A non-compliant balloon was then utilized to perform a “controlled rupture” of the iliac artery, allowing passage of the stent-graft delivery system. Endoconduits have the advantage of avoiding the complications of retroperitoneal dissection associated with the direct iliac conduit, offering a greater degree of control than over-the-wire dilator catheters or balloon angioplasty of diseased iliofemoral anatomy. Since the first publication, several case reports about the use of endoconduit in common and external iliac arteries have been published in overall literature [5,6,7] demonstrating the safety and efficacy of this technique.
There are several types of covered stents available for use in endovascular surgery. We chose the Wrapsody-covered stent. Merit Wrapsody are flexible self-expanding endoprosthesis indicated for use in hemodialysis patients for the treatment of stenosis or occlusion within the dialysis outflow circuit of an arteriovenous (AV) fistula or AV graft, consisting of Nitinol, ePTFE, PTFE structure. Several papers showed encouraging results regarding the target lesion primary patency at 30 days of 100% (45 of 45 patients had reached 30 days of follow-up). The target lesion primary patency for the patients who had completed 12 months of follow-up was 84.6% (33 of 39). [8,9] Indeed, despite the massive use of Wrapsody in venous obstructions, there is a case report published showing satisfactory results of the use of Wrapsody in popliteal artery aneurysms, with 1-year follow-up.[10]
In this present paper, we describe a patient with both chronic limb-threatening ischemia that required revascularization and aortic abdominal aneurysm. Concomitant procedures were realized in this patient with EVAR and femorofemoral bypass, obtaining a satisfactory result. Several studies have assessed the influence of various types of concomitant procedures on outcomes. [11,12] Recent reports showed that concomitant endovascular procedures were associated with low additional risks.[13] Takeuchi et al[14] evaluated the use of bifurcated endoprosthesis after iliac artery recanalization for concomitant abdominal aortic aneurysm and chronic total occlusions of access routes. They showed that recanalization of unilateral iliac chronic total occlusion lesions and placement of bifurcated stent-grafts in cases with concomitant aneurysmal disease and unilateral iliac occlusive disease demonstrated a significant primary patency rate with improvements in claudication and ankle-brachial index. According to the authors, freedom from aneurysm-related events was 100%; no patient needed secondary interventions. All patients with claudication pain preoperatively reported improvement in their symptoms during follow-up. In addition, the ankle-brachial index improved significantly from 0.51 ± 0.25 preoperatively to 0.88 ± 0.20 postoperatively (P < .001) in patients who underwent BFG placement. Indeed, this present case report showed the safety and efficacy of performing a concomitant EVAr in combination with femorofemoral bypass to treat the left limb ischemia.
This case report has some limitations since it is a single case report, with no long-term follow-up. Larger studies should be performed in order to evaluate the safety and efficacy of endovascular treatment with Merit Wrapsody for endoconduit in patients with concomitant aortic aneurysm and aortoiliac occlusive disease.
Conclusion
Endovascular conduit with Merit Wrapsodyâ covered stents for concomitant EVAR and limb revascularization seems to be a safe and effective alternative for patients with chronic limb-threatening ischemia and aortic aneurysm. Further and more robust studies are needed to validate these preliminary results.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The Authors declare that there is no conflict of interest regarding this paper.
Informed consent has been obtained from the patient for publication of the case report and accompanying images.
References
- Wu T, Carson JG, Skelly CL. (2010). Use of internal endoconduits as an adjunct to endovascular aneurysm repair in the setting of challenging aortoiliac anatomy. Ann Vasc Surg. Jan;24(1):114.e7-114.e11.
View at Publisher | View at Google Scholar - Yano OJ, Faries PL, Morrissey N, Teodorescu V, Hollier LH, Marin ML. (2001). Ancillary techniques to facilitate endovascular repair of aortic aneurysms. J Vasc Surg. 34:69–75.
View at Publisher | View at Google Scholar - Bischoff, M.S. ∙ Peters, A.S. ∙ Meisenbacher, K. (2014). Challenging access in endovascular repair of infrarenal aortic aneurysms. J Cardiovasc Surg (Torino). 55:75-83.
View at Publisher | View at Google Scholar - Hinchliffe, R.J. ∙ Ivancev, K. ∙ Sonesson, B. (2007). “Paving and cracking”: an endovascular technique to facilitate the introduction of aortic stent-grafts through stenosed iliac arteries. J Endovasc Ther. 14:630-633.
View at Publisher | View at Google Scholar - Hinchliffe RJ, Ivancev K, Sonesson B, Malina M. (2006). “Paving and cracking”: an endovascular technique to facilitate the introduction of aortic stent grafts through stenosed iliac arteries. J Endovasc Ther. 14:630–633.
View at Publisher | View at Google Scholar - Murray D, Ghosh J, Khwaja N, Murphy MO, Baguneid MS, Walker MG. (2006). Access for endovascular aneurysm repair. J Endovasc Ther. 13:754–761.
View at Publisher | View at Google Scholar - Peterson BG, Matsumura JS. (2008). Internal endoconduit: an inno vative technique to address unfavorable iliac artery anatomy encountered during thoracic endovascular repair. J Vasc Surg. 47:441–445.
View at Publisher | View at Google Scholar - Gilbert J. Prospective First-in-Human Study of the Merit WRAPSODY Endovascular Stent Graft for Treatment of Access Circuit Outflow Stenosis in Hemodialysis Patients. Journal of Vascular Surgery Abstracts 7S Volume 75, Number 4S.
View at Publisher | View at Google Scholar - Gilbert J, Rai J, Kingsmore D, Skousen J, Ptohis N. (2021). First Clinical Results of the Merit WRAPSODY™ Cell-Impermeable Endoprosthesis for Treatment of Access Circuit Stenosis in Haemodialysis Patients. Cardiovasc Intervent Radiol. Dec;44(12):1903-1913.
View at Publisher | View at Google Scholar - de Athayde Soares R, Cury MVM, Futigami AY (2024). Popliteal Artery Aneurysm Treated with Endovascular Technique and New Device: Case Report and Literature Review. JSM Heart Surg Case Images 4(1): 1012.
View at Publisher | View at Google Scholar - Kalliafas S, Albertini JN, Macierewicz J, Yusuf SW, Whitaker SC, Macsweeney ST, et al. (2000). Incidence and treatment of intraoperative technical problems during endovascular repair of complex abdominal aortic aneurysms. J Vasc Surg. 31(6):1185–92.
View at Publisher | View at Google Scholar - Fairman RM, Velazquez O, Baum R, Carpenter J, Golden MA, Pyeron A, et al. (2001). Endovascular repair of aortic aneurysms: critical events and adjunctive procedures. J Vasc Surg. 33(6):1226–32.
View at Publisher | View at Google Scholar - Hobo R, Van Marrewijk CJ, Leurs LJ, Laheij RJ, Buth J, Eurostar C. (2005). Adjuvant procedures performed during endovascular repair of abdominal aortic aneurysm. does it influence outcome? Eur J Vasc Endovasc Surg. 30(1):20–8.
View at Publisher | View at Google Scholar - Takeuchi Y, Morikage N, Mizoguchi T, Nagase T, Samura M, Ueda K, Suehiro K, Hamano K. (2019). Using bifurcated endoprosthesis after iliac artery recanalization for concomitant abdominal aortic aneurysm and chronic total occlusions of access routes. J Vasc Surg. Jul;70(1):117-122.
View at Publisher | View at Google Scholar
