

Research Article | DOI: https://doi.org/10.31579/2835-8325/071
The potential roles of IL-6 and NKG2C in the pathogenesis of Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis
- El-Khateeb Hanin 1*
- Shekar Malika 1*
- Iqbal O 2,4
- Dharan A 3
- Campbell E 3
- Bu P 4
- Mudaliar K 2
- Speiser J 2
- Bouchard C 4
1Opthalmology/Pathology, Loyola University Chicago Stritch School of Medicine, Maywood, Illinois, United States
2Opthalmology/Pathology, Loyola University Chicago Stritch School of Medicine, Maywood, Illinois, United States
3Microbiology, Loyola University Chicago Stritch School of Medicine, Maywood, Illinois, United States
4Ophthalmology, Loyola University Health System, Maywood, Illinois, United States
*Corresponding Author: El-Khateeb Hanin, Shekar Malika, Opthalmology/Pathology, Loyola University Chicago Stritch School of Medicine, Maywood, Illinois, United States
Citation: El-Khateeb Hanin, Shekar Malika, Iqbal O, Dharan A, Campbell E, Bu P, Mudaliar K, Speiser J and Bouchard C, (2024), The potential roles of IL-6 and NKG2C in the pathogenesis of Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis”, Clinical Research and Clinical Reports, 4(3); DOI: 10.31579/2835-8325/071
Copyright: © 2024, El-Khateeb Hanin. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 March 2024 | Accepted: 15 April 2024 | Published: 07 May 2024
Keywords: stevens-johnson syndrome; pathogenesis; nkg2c; il-6; immunofluorescence; microscopy
Abstract
Stevens Johnson Syndrome/Toxic Epidermal Necrolysis (SJS/TEN) are most often drug-induced severe cutaneous adverse reactions with increased morbidity and mortality. Eyes are often involved causing ocular surface disease leading to visual impairment and blindness. The pathogenesis is not completely understood. HLA-E-specific activating receptor CD94/NKG2C are reported to trigger T-cell receptor-independent cytotoxicity in cytotoxic T cells. Several cytokines are known to play a role in the pathogenesis of this condition. The role of IL-6 and NKG2C in causing ocular surface disease and keratinocyte apoptosis is not fully explored. Determination of the expression of IL-6 and NKG2C studied by immunofluorescence microscopy will enable better understanding of their potential roles in the pathogenesis of SJS/TEN. It is hypothesized that IL-6 and NKG2C play a crucial role in the pathogenesis of SJS/TEN and may correlate with the degree of severity of skin detachment and ocular surface disease. To validate this hypothesis, the specific aim is to determine the expression of IL-6 and NKG2C in the skin of patients with biopsy confirmed SJS/TEN compared to the lichen planus controls by immunohistochemistry and correlation with severity of skin detachment. Under a current, Loyola IRB approved protocol, 12 collected and archived unstained slides of skin and blood plasma samples from patients with biopsy confirmed SJS/TEN were used for this study. Deconvolution Immunofluorescence (IF) was performed using IL-6 and NKG2C antibodies using a Delta Vision microscope equipped with a digital camera. Human Corneal Epithelial cell cultures was challenged by TNF-α or plasma from patients with SJS/TEN and the induced expression of IL-6 and NKG2C was determined using immunofluorescence microscopy. Deconvolution immunofluorescence performed on skin biopsy-confirmed SJS/TEN patient slides showed expression of IL-6 and NKG2C using a Delta Vision microscope.IL-6 and NKG2C may be involved in the pathogenesis of SJS/TEN. Further studies are warranted to establish their roles in the severity of disease.
Introduction
Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) are classified under the distinct category of Severe Cutaneous Adverse Reactions (SCARs). These lesions are uncommon life-threatening severe mucocutaneous lesions characterized by necrosis and sloughing of the skin, and often associated with multiorgan system involvement leading to dermatologic, hematological, ophthalmologic, and genitourinary complications. Eyes and skin are most often involved. Eyes may be linked to causing severe purulent conjunctivitis and corneal blindness requiring amniotic membrane transplantation or corneal transplantation. Regarding the skin, toxic epidermal necrolysis is a type IV immune reaction that presents with mucocutaneous blistering alongside epidermal detachment [32]. This severe skin reaction is classified based on the degree of skin detachment. SJS is characterized by skin involvement of less than 10%, TEN is defined as skin involvement exceeding 30%, and SJS/TEN overlap is identified as skin involvement of 10-30% [17]. The lesions related to this syndrome typically manifest as blisters accompanied by mucosal epidermal detachment caused by epidermal necrosis with limited dermal inflammation [32]. To distinguish these skin lesions from erythema multiforme (EM), herpes simplex virus, or mycoplasma infection in children, the distribution of the other phenomena has a less widespread distribution compared to SJS and TEN [32]. The lesions that first emerge as dusky or purpuric plaques form vesicles that appear as targetoid lesions. These lesions start to grow and become increasingly confluent. This is followed by painful ulcerations with pseudomembranous and necrosis. Following the resolution of SJS, the skin may experience hypo- or hyper-pigmentation, abnormal nail growth, and paronychia [31-32].
The pathogenesis of this condition has yet to be fully understood. Numerous associations related to the prevalence of SJS/TEN in Southeast Asia have been recorded, including associations with HLA- A*0206, HLA-B*44:03, HLA-B*1502 (carbamazepine), and HLA-B*5801 (allopurinol) genotypes [1-4]. SJS/TEN are considered under the umbrella of immune-mediated specific hypersensitivity reactions that can become triggered by cytotoxic T-lymphocytes [23-25]. In patients with SJS/TEN, it was discovered that Cytotoxic T cells and NK cells infiltrated the skin lesions [22]. Granule-mediated exocytosis mainly of perforin, granzyme B, and Fas/FasL interactions was reported to explain keratinocyte apoptosis [7]. Elevated expression of the death cell receptor TNF-α or TNF receptor 1 has been reported in numerous studies [4]. The granulysin (15 kDa) form that was secreted by the NK cells and cytotoxic T cells was denoted to have infiltrated the blister fluid- This in turn demonstrated its role in the widespread keratinocyte apoptosis [6]. Interleukin-15 was reported to be associated with severity and mortality in SJS/TEN [30]. It was recently reported that there may be a potential role for IL-13, IL-15, and granulysin in the pathogenesis of T-cell receptors confined by the HLA-1b molecule HLA-E [19-20]. In addition, it has also been noted that the HLA-E-specific activating receptor CD94/NKG2C can induce T-cell receptor-independent cytotoxicity in cytotoxic T cells [19-20]. While the expression of cytokines and chemokine receptors present in cutaneous lesions of SJS have been previously documented [6-7], their exact roles in the development of skin necrosis and skin detachment have not been entirely studied. It has been noted that a myriad of cytokines causes apoptosis in both SJS and TEN, including but not limited to perforin, granzyme B, and TNF. The cytotoxic T cells have the capability of secreting granules that carry granulysin perforin, and granzyme B which in turn perforate the membrane resulting in mitochondrial damage, and ultimately death. When analyzing bodily fluid, such as blister fluid in patients with SJS/TEN in comparison to burn patients: The former patients were found to have twenty times more granulysin and eight times more granzyme b. As aforementioned, the precise mechanism and function that T cells and NK cells play in generating these mediators have not been demonstrated [5, 19-20].
Diagnosis of SJS/TEN has been focused on the overall morphology and extent of lesions based on prior drug exposures or illnesses. Currently, it remains challenging to identify early SJS/TEN cases due to the initial signs and symptoms of drug eruptions mimicking non-severe ones. Histological examination has demonstrated efficacy in identifying epidermal necrosis, or separation at the dermo-epidermal junction [5]. The myriad of drugs involved in the pathogenies, and toxicokinetic that precipitate SJS/TEN typically have extended half-lives and are taken systemically. Symptoms develop within just a few days to a few months after starting a new drug [23].
This study assessed the expression of IL-6 and NKG2C in both the skin and blood of patients with SJS/TEN utilizing immunohistochemistry techniques. The levels of IL-6 and NKG2C was correlated with the extent of skin detachment in these patients by referencing the information available in their patient charts. Furthermore, induced expression of IL-6 and NKG2C by TNF-alpha or plasma from confirmed SJS/TEN patients, in corneal epithelial cells and keratinocyte cell cultures were studied. The precise role of IL-6 and NKG2C in the pathogenesis is not fully known. This study is designed to study the roles of IL-6 and NKG2C in the pathogenesis of Stevens-Johnson Syndrome. The hypothesis postulates that IL-6 and NKG2C are vital factors in the pathogenesis of SJS/TEN. This further suggests that the interplay of IL-6 and NKG2C may serve as notable indicators influencing the severity spectrum of both skin and ocular manifestations observed in SJS/TEN cases. Further investigation into the intricate relationship between the cytokine immune factors and the clinical outcomes of SJS/TEN could provide valuable insights into the underlying mechanisms and potential biomarkers for disease progression.
Materials and Methods
Immunofluorescence Microscopy- Utilization of Skin Biopsy Slides
Under a current, Loyola institutional review board (IRB) protocol, 12 collected and archived unstained slides of skin and blood plasma samples from patients with biopsy-confirmed SJS/TEN were utilized. In addition, 4 collected and archived Lichen Planus slides were used for controls in the study. All tissue samples underwent de-identified prior to the initiation of the experiment.
All the slides used for the experiment were stored and processed similarly. The segments of the skin biopsies on the slides underwent deparaffinization by utilizing three washes with xylene for 5 minutes each. Following this, the slides underwent rehydration through the utilization of a progressive ethanol gradient. This gradient followed the respective order: They were subjected to two washes utilizing 100% ethanol (EtOH) for 2 minutes each, followed by a single wash in 95% EtOH for 5 minutes, and ultimately, they were washed in 70% ethanol for 5 minutes. Subsequently, the biopsy slides were rinsed utilizing distilled water for 1 minute and washed for 5 minutes in the phosphate buffer solution (PBS). Next, the slides were blocked with normal goat serum for precisely 1 hour, and then were treated with either IL-6 or NKG2C- the primary antibody and incubated overnight within a humidified container at 4oC. Following the one-hour incubation period, the biopsy slides underwent 3 washes with PBS and then treated with the secondary anti-rabbit IgG, fluorescein isothiocyanate (FITC), and diamino-2 phenylindole (DAPI) antibodies for 30 minutes. After washing with PBS, slide covers were mounted with fluorogel. For each slide stained with primary antibody, an additional control slide was prepared. The slides were then incubated with 10% NDS instead of IL-6 or NKG2C primary antibody and stained with secondary rabbit anti-rabbit IgG, FITC, and DAPI antibodies. The primary objective of the control slides was further to enhance the understanding of SJS/TEN pathology and compare the levels of background auto-fluorescence across all tissue samples.
Images were captured using a DeltaVision microscope equipped with a digital camera, utilizing deconvolution and immunofluorescence. The settings and exposure times were maintained consistently across the entirety of the sample pool.
Results
IL-6 and NKG2C are two crucially recognized cytokines that play a significant role in inflammatory diseases associated with dermatology, and ophthalmology-related inflammatory diseases. In our endeavor to delve deeper into the expression of IL-6 and NKG2C in patients with SJS/TEN and LP, we took the initiative to complete the aforementioned experiment, the findings of which are depicted below.
IL-6 and NKG2C intensities in SJS/TEN, Lichen Planus, and Normal Control Tissue Samples
Figure 1: Representative images obtained through immunofluorescent microscopy and deconvolution. A total of 12 SJS/TEN and 4 Lichen planus skin biopsy samples were analyzed utilizing immunofluorescence microscopy. The above images display a total of 4 samples from SJS. Among them, 2 contained IL-6 cytokines, while the other 2 contained NKG2C samples. Comparative analysis was performed between them and the control, where Lichen Planus lacked the anti-IL-6 or anti-NKG2C primary antibody. All scale bars were standardized to 10 µm.
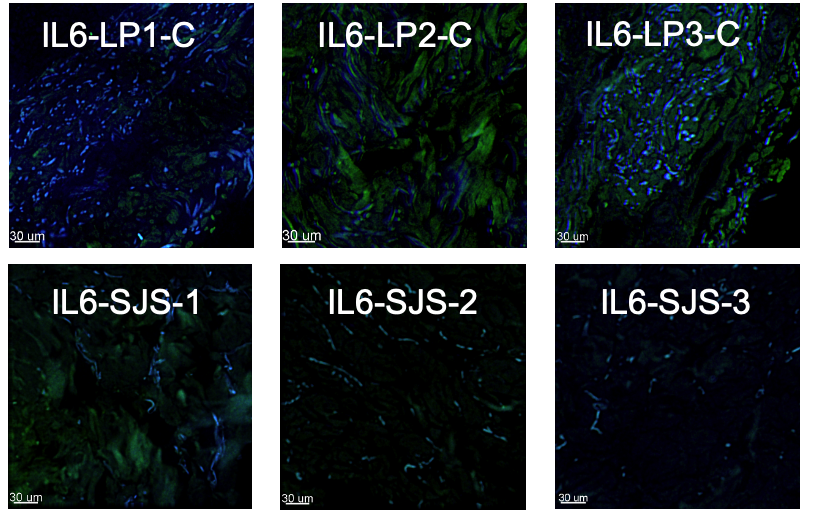
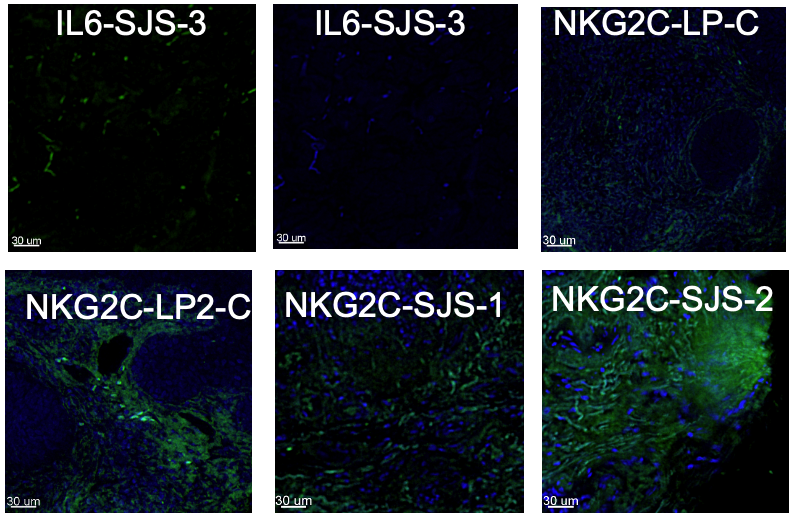
Figure 2: Representative images taken utilizing an immunofluorescent (IF) microscopy equipped with a DeltaVision microscope and a digital camera. Exposure times were kept constant across all samples.
Discussion
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis are life-threatening conditions, associated with a myriad of severe clinical implications. The diagnosis of SJS/TEN is notably challenging, and there is a lack of well-established biomarkers needed for accurate diagnosis or prediction of severity. A potential therapeutic approach to mitigate the overall occurrence of SJS involves HLA screening before administering certain medications [10]. A myriad of studies have concentrated their efforts on identifying the specific cytokines and inflammatory mediators that contribute to the pathogenesis of SJS [21]. The methodology employed in this study and the subsequent outcomes demonstrated that both IL-6 and NKG2C were cytokines that played a crucial role in the pathophysiology of SJS/TEN, evident by the increased level of expression on skin biopsy slides of patients with confirmed SJS/TEN. To date, there has been a limited number of studies demonstrating the expression of IL-6 and NKG2C in patients with confirmed SJS/TEN. Some studies postulated the potential cause involving a hapten-induced immune response where the implicated drugs can stimulate cells by directly binding to immune receptors reversibly. Conversely, other studies have postulated that a myriad of cell death mediators including FasL and regulatory T-cells may also play a role in the occurrence of SJS/TEN [1-2].
NKG2C was identified as a cytotoxic T lymphocyte (CTL) with Natural killer (NK))-like activity that responds to HLA-E found in the skin of patients with SJS/TEN. This in turn leads to the sensitization of keratinocytes to cellular killing [19]. Furthermore, it was found that the frequencies of CD94/NKG2C (+) were increased to a great degree in patients with SJS/TEN, further confirming its inflammatory role in the pathogenesis of this deadly disease [22].
IL-6 cytokine has shown numerous implications about its upregulation in patients with SJS/TEN, in addition to other cytokines in a publication by Stern et alIt was observed that not only was there an elevation in this cytokine, but it also correlated with the extent of cutaneous involvement and the overall clinical course [29]. Elevated levels of the IL-6 cytokine suggest that it plays a role in the inflammatory pathogenesis of SJS, and to a greater severity than of TEN. Furthermore, the study of cytokines not only provides an enhancing contribution to the diagnosis of the disease but
also aids in providing insight into various therapeutic management treatments [14]. A study assessing the diverse expression of tear cytokine levels in patients with chronic SJS, to further comprehend the role of cytokine alteration in disease development [14]. It was noted that there was a significant upregulation of the pro-inflammatory cytokine IL-6 with a p-value < 0>
Gaining insights into the contributions of IL-6 and NKG2C to the pathogenesis and persistent inflammatory state in patients with SJS/TEN will be instrumental in improving both diagnosis and clinical management. Our clinical findings, and extensive research initiative, led us to confidently believe IL-6 and NKG2C hold promise as biomarkers used to assess disease severity. While these cytokines may not be unique to SJS/TEN solely, they have promising indications in the inflammatory pathogenesis associated with the disease process, and their clinical significance in skin biopsy samples plays a prominent role. These findings warrant a further understanding of the currently available treatment types for SJS/TEN. Recent work by Narita et al. focused on whether the overexpression of cytokines plays a role in therapeutic efficacy. Her study further delved into a specific type of plasmapheresis known as double-filtration plasmapheresis which uses a double-filtration system to remove more specific components of the plasma [21]. It has been further confirmed that plasma filtration is a more effective treatment approach for refractory cases of SJS/TEN in comparison to glucocorticoids. However, in non-refractory SJS/TEN methylprednisolone pulse therapy has shown promising results. A study was conducted with 8 patients with confirmed SJS/TEN using the Bastuji-Garin criteria, who experienced high fevers, and mucosal lesions [11]. Methylprednisolone was provided at a dosage of 1000 mg per day for three consecutive days. If no new mucocutaneous lesions were observed on the day following the last dose of methylprednisolone, oral prednisolone at a dose ranging from 0.8 to 1 mg per kilogram per day was started. The results after four days showcased that the mean levels of IFN-α, TNF-α, IL-6, and IL-10 had decreased compared to their levels before administration. However, only the reductions in IFN-α and IL-6 were statistically significant [11]. In addition, IVIG was another therapeutic regimen that utilized antagonistic monoclonal antibodies to target the FAS in the FAS-Fas ligand relationship [8]. Given the involvement of ocular, oral, dermatological, and more, complications tend to vary greatly, and the timing of therapeutic interference is critical. Per Kumar et. al. early referral to an ophthalmologist is critical to assess ocular involvement such as corneal scarring, or corneal xerosis [15]. If disease spread is mild, lubricants and topical steroids can do the job. However, severe involvement requires gas-permeable scleral contact lens therapy and amniotic membrane transplantation [15]. Furthermore, a multicenter retrospective study further stated that the use of systemic glucocorticoids was linked to a reduced likelihood of extensive disease in individuals with body surface area (BSA) involvement of greater than 30% [16]. The myriad of implications regarding treatment courses, whether supportive or intensive, may prove beneficial in the long term; However, further research on the matter is imperative.
Immunological responses to SJS/TEN from an ophthalmologic or dermatological perspective are vast. Numerous studies have demonstrated the next critical step to ensure the patient's skin, eye, and organ manifestations don’t worsen is by understanding the predictive probability based on past studies, as well as unique symptomatology to the disease such as the Nikolsky sign [31]. Furthermore, it has been noted most if not all drug eruptions are linked to T-cell mediated delayed hypersensitive, with the varying sequelae resulting from the activation of varying cytokines such as IL-6 and NKG2C- the two cytokines implicated in our study [24-25, 27]. Overall, Pharmacogenetic studies have established a clear link between human leukocyte antigen allotype and TEN. Human leukocyte antigen testing should be performed on patients before the administration of a drug known to be implicated in the pathogenesis of SJS/TEN [27]. In a study published in 2020, a systemic review was conducted by numerous ophthalmologists, dermatologists, ob/gyn, and infectious disease doctors who were experts in the matter of SJS/TEN pathophysiology, and long-term treatment outcomes. They became participants in developing statements for supportive care in patients with this condition utilizing the 9-point Likert scale questionnaires regarding 135 statements and statements that received greater than 6.5/9 on the scale were included in the guideline. This initiative aimed to gather experts in the field of SJS/TEN to develop guidelines that prioritize meeting the long-term needs of patients and improving their outcomes [28]. This study can be linked to our own study by acquiring specific symptoms that will not only aid in the diagnoses of patients with biopsy-confirmed SJS/TEN, but also aid in their future treatment process.
Overall, to date, various cytokines have been implicated in the pathogenesis of SJS/TEN, and more often then not usually correlating to a specific clinical finding such as retinal detachment, skin necrosis, pancreatic injury, or renal failure seen in the pediatric population with SJS/TEN [13]. In a study conducted by Gao et al. it was discovered that IL-18 overexpression was implicated in acute pancreatic injury [9]. Furthermore, some studies went to the extent of categorizing lesions related to SJS/TEN according to the pattern of erythema multiforme, assessing whether this aids in identifying cases using this nosological framework [3].
Conclusion
Overall, our results showcased an increase in the expression of IL-6 and NKG2C expression in the skin biopsy slides of patients with confirmed SJS/TEN in comparison to the Lichen planus (LP) controls. We can conclude that both IL-6 and NKG2C are key components and regulators involved in the detrimental outcomes of SJS/TEN. The pathogenesis remains complex and incompletely understood. Various genetic associations have been identified, highlighting the importance of individual susceptibility to certain drugs or infections. While cytokines such as IL-6 and NKG2C have been implicated in the pathogenesis, their precise roles and interactions remain to be fully understood. Early recognition is crucial due to the rapid progression of symptoms leading to significant morbidity and mortality. The ongoing study into the expression and function of IL-6 and NKG2C in SJS/TEN pathogenesis represents a significant step in truly understanding these conditions. The correlation between cytokine levels and clinical outcomes helps serve as potential biomarkers for disease progression and aids in the development of targeted therapies. Further exploration of the intricate immune mechanisms involved in SJS/TEN promises to enhance our ability to predict, diagnose, and clinically manage these conditions in an effective manner.
Conflicts of Interest Statement
The authors have no conflicts of interest to declare.
Acknowledgments
We would like to thank the Richard A. Perritt Foundation for their financial support.
References
- Abe, R. (2015). Immunological response in Stevens–Johnson syndrome and toxic epidermal necrolysis. The Journal of Dermatology, 42(1):42-48.
View at Publisher | View at Google Scholar - Abe, R. (2016). Cutaneous Adverse Drug Reactions: Stevens–Johnson Syndrome and Toxic Epidermal Necrolysis. In: Kabashima, K. (eds) Immunology of the Skin. Springer, Tokyo.
View at Publisher | View at Google Scholar - Bastuji-Garin S, Rzany B, Stern RS, Shear NH, Naldi L, Roujeau J. (1993). Clinical Classification of Cases of Toxic Epidermal Necrolysis, Stevens-Johnson Syndrome, and Erythema Multiforme. Arch Dermatol, ;129(1):92-96.
View at Publisher | View at Google Scholar - Chave TA, Mortimer NJ, Sladden MJ, et al. (2005). Toxic epidermal necrolysis: current evidence, practical management and future directions. Br J Dermatol, 153(2):241-253.
View at Publisher | View at Google Scholar - Chuenwipasakul, D., Washrawirul, C, Panpruk, R. et al. (2023). Correlations between histopathologic findings, serum biomarker levels, and clinical outcomes in Stevens–Johnson syndrome/toxic epidermal necrolysis (SJS/TEN), 13:13620.
View at Publisher | View at Google Scholar - Chung WH, Hung SI, Hong GS, et al. (2004). medical genetics: a marker for Stevens Johnson syndrome. Nature, 428(6982):486.
View at Publisher | View at Google Scholar - Chung WH, Hung SI, Yung GY et al. (2008). Granulysin is a key mediator for disseminated keratinocyte death in Stevens Johnson syndrome and toxic epidermal necrolysis. Nat Med, 14(12):1343-1350.
View at Publisher | View at Google Scholar - French, L. E. (2006). Toxic Epidermal Necrolysis and Stevens Johnson Syndrome: Our Current Understanding. Allergology International, 55(1):9-16.
View at Publisher | View at Google Scholar - Gao, X, Tang, X, Ai, L, Gao, Q, Liao, Q, Chen, M, Chen, X, Zhou, H, Ye, Y, Li, M, Han, J, & Wang, F. (2021). Acute pancreatic injuries: A complication of Stevens-Johnson syndrome/toxic epidermal necrolysis associated with cytotoxic immunocell activation. Journal of the American Academy of Dermatology, 84(3):644-653.
View at Publisher | View at Google Scholar - Hasegawa, A, & Abe, R. (2020). Recent advances in managing and understanding Stevens-Johnson syndrome and toxic epidermal necrolysis. F1000Research, 9.
View at Publisher | View at Google Scholar - Hirahara, K, Kano, Y, Sato, Y, Horie, C, Okazaki, A, Ishida, T, Aoyama, Y, & Shiohara, T. (2013). Methylprednisolone pulse therapy for Stevens-Johnson syndrome/toxic epidermal necrolysis: clinical evaluation and analysis of biomarkers. Journal of the American Academy of Dermatology, 69(3):496-498.
View at Publisher | View at Google Scholar - Hsieh, M, Watanabe, T, & Aihara, M. (2021). Recent Dermatological Treatments for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis in Japan. Frontiers in Medicine, 8:636924.
View at Publisher | View at Google Scholar - Hsu, D. Y, Brieva, J, Silverberg, N. B, Paller, A. S, & Silverberg, J. I. (2017). Pediatric Stevens-Johnson syndrome and toxic epidermal necrolysis in the United States. Journal of the American Academy of Dermatology, 76(5):811-817:4.
View at Publisher | View at Google Scholar - Koduri, M. A, Prasad, D, Upadhyaya, S, Jaffet, J, Shanbhag, S. S., Basu, S, & Singh, V. (2021). Differential expression of tear film cytokines in Stevens–Johnson syndrome patients and comparative review of literature. Scientific Reports, 11(1):1-11.
View at Publisher | View at Google Scholar - Kumar, R, Das, A, & Das, S. (2018). Management of Stevens-Johnson Syndrome-Toxic Epidermal Necrolysis: Looking Beyond Guidelines! Indian Journal of Dermatology, 63(2):117-124.
View at Publisher | View at Google Scholar - Kridin K, Brüggen M, Chua S, et al. (2021). Assessment of Treatment Approaches and Outcomes in Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Insights from a Pan-European Multicenter Study. JAMA Dermatol, 157(10):1182–1190.
View at Publisher | View at Google Scholar - Lerch M, Mainetti C, Terziroli Beretta-Piccoli B, Harr T. (2018). Current Perspectives on Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. Clin Rev Allergy Immunol, 54(1):147-176.
View at Publisher | View at Google Scholar - Mockenhaupt M. (2014). Stevens-Johnson syndrome and toxic epidermal necrolysis: clinical patterns, diagnostic considerations, etiology, and therapeutic management. Seminars in cutaneous medicine and surgery, 33(1):10-16.
View at Publisher | View at Google Scholar - Morel E, Escamochero S, Cabanas R, et al. (2010). CD94/NKG2C is a killer effector molecule in patients with Stevens Johnson syndrome and toxic epidermal necrolysis. J Allergy Clin Immunol, 125(3):703-710, 710:8.
View at Publisher | View at Google Scholar - Morel, E, Escamochero, S, Cabañas, R, Díaz, R, Fiandor, A, & Bellón, T. (2010). CD94/NKG2C is a killer effector molecule in patients with Stevens-Johnson syndrome and toxic epidermal necrolysis. The Journal of allergy and clinical immunology, 125(3):703-710:8.
View at Publisher | View at Google Scholar - NARITA, Y.M., HIRAHARA, K., MIZUKAWA, Y., KANO, Y. and SHIOHARA, T. (2011), Efficacy of plasmapheresis for the treatment of severe toxic epidermal necrolysis: Is cytokine expression analysis useful in predicting its therapeutic efficacy? The Journal of Dermatology, 38:236-245.
View at Publisher | View at Google Scholar - Nassif A, Bensussan A, Boumsell L et al. (2004). Toxic epidermal necrolysis: effector cells are drug-specific cytotoxic T cells. J Allergy Clin Immunol, 114(5):1209-1215.
View at Publisher | View at Google Scholar - Oakley AM, Krishnamurthy K. (2023). Stevens-Johnson Syndrome. [Updated 2023 Apr 10]. In: StatPearls [Internet]. Treasure Island (FL).
View at Publisher | View at Google Scholar - Roujeau JC. (2006). Immune mechanisms in drug allergy. Allergol Int, 55(1):27-33.
View at Publisher | View at Google Scholar - Roujeau JC, Stern RS. (1994). Severe adverse cutaneous reactions to drugs. N Engl J med, 331(19):1272-1285.
View at Publisher | View at Google Scholar - Sadek M, Iqbal O, Siddiqui F, et al. (2021). The roles of IL-13, IL-15, and granulysin in the pathogenesis of Stevens Johnson syndrome and toxic epidermal necrolysis. Clin Applied Hemostasis/Thrombosis, 27:1-8.
View at Publisher | View at Google Scholar - Schwartz RA, McDonough PH, Lee BW. (2013). Toxic epidermal necrolysis: Part II. Prognosis, sequelae, diagnosis, differential diagnosis, prevention, and treatment. J Am Acad Dermatol, :69(2):187.1-16:203-204.
View at Publisher | View at Google Scholar - Seminario-Vidal, L, Kroshinsky, D, Malachowski, S. J, Sun, J, Markova, A, Beachkofsky, T. M, Kaffenberger, B. H, Ergen, E. N, Mauskar, M, Bridges, A, Calhoun, C, Cardones, A. R, Chen, S. T, Chodosh, J, Cotliar, J, Davis, M. D, DeNiro, K. L, Dominguez, A. R, Eljure-Téllez, J, Micheletti, R. G. (2020). Society of Dermatology Hospitalists supportive care guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults. Journal of the American Academy of Dermatology, 82(6):1553-1567.
View at Publisher | View at Google Scholar - Stern, R. S, & Divito, S. J. (2017). Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Associations, Outcomes, and Pathobiology-Thirty Years of Progress but Still Much to Be Done. The Journal of Investigative Dermatology, 137(5):1004.
View at Publisher | View at Google Scholar - Su SC, Mockenhaupt M, Wolkerstein P, et al. (2017). Interleukin-15 is associated with severity and mortality in Stevens Johnson Syndrome/toxic epidermal necrolysis. J Invest Dermatol, 137(5):1065-1073
View at Publisher | View at Google Scholar - Weinkle, A, Pettit, C, Jani, A, Keller, J, Lu, Y, Malachowski, S, Trinidad, J. C, Kaffenberger, B. H, Ergen, E. N, Hughey, L. C, Smith, D, & Seminario-Vidal, L. (2019). Distinguishing Stevens-Johnson syndrome/toxic epidermal necrolysis from clinical mimickers during inpatient dermatologic consultation—A retrospective chart review. Journal of the American Academy of Dermatology, 81(3):749-757.
View at Publisher | View at Google Scholar - Zimmerman D, Dang NH. (2019). Stevens–Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN): Immunologic Reactions. Oncologic Critical Care, 9:267-280.
View at Publisher | View at Google Scholar - Zimmermann S, Sekula P, Venhoff M, et al. (2017). Systemic Immunomodulating Therapies for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Systematic Review and Meta-analysis. JAMA Dermatol, 153(6):514-522.
View at Publisher | View at Google Scholar
