

Case report | DOI: https://doi.org/10.31579/2834-796X/097
The Experience of off-the-shelf use of Merit Wrapsody® Covered stent for Arterial Disease
- Guilherme Centofanti 1,2,3
- Nicole Inforsato 1
- Mariana Krutman 1,2
- Kenji Nishinari 1,2
- Guilherme Yasbek 1
- Rafael Noronha Cavalcante 1,2
- Bruno Soriano Pignataro 1
- Thais Dante Correia Rocha 2
- Bruno Giovani Valese 2
- Henrique Elkis 3
- Bruna de Fina 3
- Gian Carlo Vassoler 3
- Elton Wolaniuk 3
- Rafael de Athayde Soares 4
1Hospital AC Camargo Cancer Center.
2Hospital Alemão Osvaldo Cruz.
3Hospital Paulistano.
4Hospital do Servidor Público Estadual de São Paulo, IAMSPE.
*Corresponding Author: Rafael de Athayde Soare, Hospital do Servidor Público Estadual de São Paulo, Iamspe.
Citation: Guilherme Centofanti, Nicole Inforsato, Mariana Krutman, Kenji Nishinari and Rafael de Athayde Soares et.al, (2025), The Experience of off-the-shelf use of Merit Wrapsody® Covered stent for Arterial Disease, International Journal of Cardiovascular Medicine, 4(2); DOI:10.31579/2834-796X/097
Copyright: © 2025, Rafael de Athayde Soare. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 February 2025 | Accepted: 17 March 2025 | Published: 26 March 2025
Keywords: arterial iatrogenic injuries; penetrating aortic ulcers; aneurysms
Abstract
In this paper, we aimed to report the off-the-shelf use of Merit Wrapsody® for arterial disease. We describe a case series of reports of 6 patients submitted to endovascular repair with Merit Wrapsody® for arterial disease. Merit Wrapsody® a flexible self-expanding endoprosthesis indicated for use in hemodialysis patients for the treatment of stenosis or occlusion within the dialysis outflow circuit of an arteriovenous (AV) fistula or AV graft, consisting of Nitinol, ePTFE, PTFE structure. In a case series communication, we aimed to describe the feasibility of a PTFE-lined stent for percutaneous treatment of conditions other than AV fistula obstruction. We report the successful use of Wrapsody to percutaneously treat several arterial vascular conditions, including iatrogenic arterial lesions, abdominal aortic ulcers, abdominal aortic saccular aneurysms, subclavian artery aneurysms, and arterial thrombosis. This case series illustrates the feasibility of the "off-label" use of self-expanded Wrapsody endoprosthesis to percutaneously treat arterial pathology conditions, especially arterial territory with satisfactory and safe results.
1. Introduction
Arterial iatrogenic injuries, such as bleeding, pseudoaneurysm, and dissection or fistula, are potentially life-threatening complications, requiring a prompt diagnosis and management. Despite surgical treatment representing the traditional approach, endovascular treatment proved to be an effective and less invasive alternative, especially in patients with comorbidities or unsuitable for open surgery.[1] The use of covered stent grafts allows the exclusion of the lesion/defect without sacrificing the target vessel, thus avoiding ischemic complications.[2]
Merit Wrapsody is a flexible cell impermeable self-expanding endoprosthesis indicated for use in hemodialysis patients for the treatment of stenosis or occlusion within the dialysis outflow circuit of an arteriovenous (AV) fistula or AV graft, consisting of Nitinol, ePTFE, PTFE structure. Several papers showed encouraging results regarding the target lesion primary patency at 30 days of 100% (45 45 patients had reached 30 days of follow-up). The target lesion primary patency for the patients who had completed 12 months of follow-up was 84.6% (33 of 39).[3,4] Indeed, despite the massive use of Wrapsody in venous obstructions, there is a case report published showing satisfactory results of the use of Wrapsody in popliteal artery aneurysms, with 1-year follow-up.[5] Moreover, a recent publication reported the use of Wrapsody endoprosthesis for an endoconduit for EVAR, demonstrating the safety and efficacy of the shelf use of this device for arterial diseases.[6]
Furthermore, penetrating aortic ulcers (PAUs) are a subset of acute aortic syndrome (AAS), defined as the rupture of atherosclerotic lesions through the internal elastic lamina of the aortic wall with subsequent hematoma formation between the media and adventitia.[7] Although most PAUs will be asymptomatic, the rupture rate for PAUs (as great as 38%) presenting in patients with AAS has been greater than that in patients with PAUs and aortic dissection.[8] endovascular repair is the preferred treatment for this condition. In this study, we aimed to report the use of Merit Wrapsody® for arterial disease in a case series (6 patients).
Case Presentations Case 1
A male patient, 73 years old, with lung cancer, receiving chemotherapy was submitted to a dialysis catheter implant. During the procedure, the catheter was inadvertently implanted at the common carotid artery. Our vascular team was called and decided to perform an endovascular procedure to treat this iatrogenic condition. The patient was then submitted to an endovascular implant of Wrapsody Merit 9x50mm at the carotid artery. The final image showed excellent results with no endoleaks e complete resolution of the carotid lesion. (Figure 1). The patient evolved very well and 2 years follow-up showed endoprosthesis patency with no endoleaks at Carotid Duplex ultrasound. Unfortunately, the patient died 2 years after the surgery due to metastatic complications of lung cancer.
Pre Post
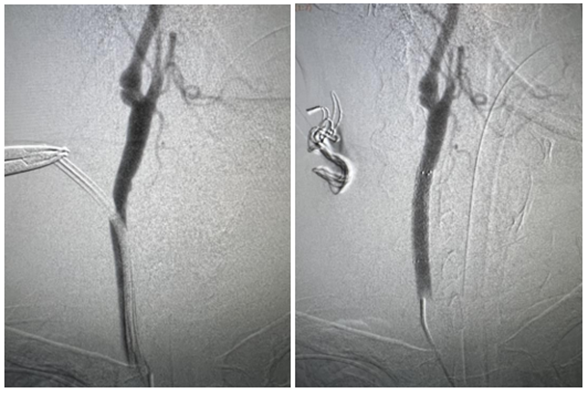
Figure 1: Implant of Wrapsody Merit 9x50mm at the carotid artery.
Case 2
A male patient, 92 years old, with liver cancer was submitted to a pacemaker insertion due to cardiac conditions. The pacemaker catheter was inadvertently inserted at the subclavian artery. The patient evolved with subclavian artery occlusion and bleeding. Our vascular team was called and
immediately decided to perform an endovascular treatment with mechanical thrombectomy with lightning 7 and subsequent implant of Wrapsody Merit 8x75mm (Figure 2). The patient evolved very well post-operative and 1-year follow-up showed endoprosthesis patency and no endoleaks.
Pre Post
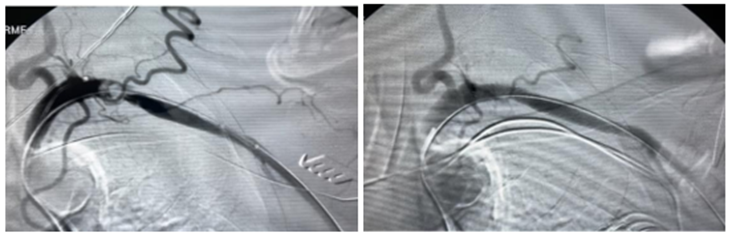
Figure 2: Thrombectomy with lightning 7 and subsequent implant of Wrapsody Merit 8x75mm
Case 3
A female patient, 72 years old, active smoker, with arterial hypertension and a history of previous abdominal saccular aortic aneurysm endovascular correction, was admitted with endoleak type 1a. The patient was submitted
to endovascular surgery with a catheter balloon dilatation of the previous endoprosthesis and an implant of a new endoprosthesis Wrapsody Merit 14x30mm proximally (Figure 3). The patient was discharged from the hospital first day post-operative and CT-SCAN after 2 years of follow-up showed endoprosthesis patency with no endoleaks.

Figure 3: Implant of a new endoprosthesis Wrapsody Merit 14x30mm proximally
Case 4
A male patient, 72 years old, active smoker, with arterial hypertension, diabetes, and chronic kidney disease was admitted with PAU at the infra-renal abdominal aorta.
The patient was submitted to an endovascular surgery with an implant of endoprosthesis Wrapsody Merit 16x40mm followed by post-dilatation with a catheter balloon at the infra-renal abdominal aorta. (Figure 4) The patient was discharged from the hospital first day post-operative and 1-year follow-up CT-SCAN showed endoprosthesis patency with no endoleaks.
CT-Scan previous post-Operative
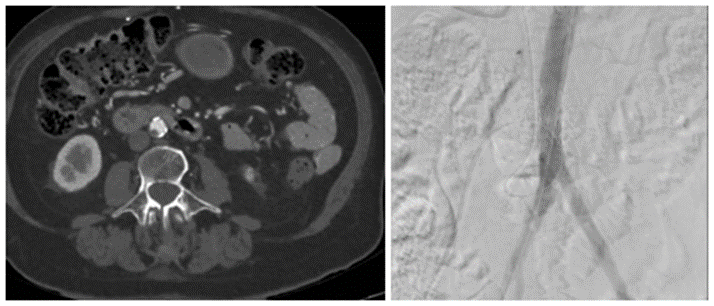
Figure 4. Implant of endoprosthesis Wrapsody Merit 16x40mm:
Case 5
A female patient, 34 years old, with no comorbidities was admitted with a sacular aneurysm of the right subclavian artery. The patient was scheduled to undergo endovascular surgery with a covered endovascular Wrapsody 9x50mm implanted at the right subclavian artery followed by post-dilatation with a catheter balloon (Figure 5). The patient was discharged from the hospital first day post-operative and a 2-year Duplex ultrasound follow-up showed endoprosthesis patency without endoleaks.
Pre Post
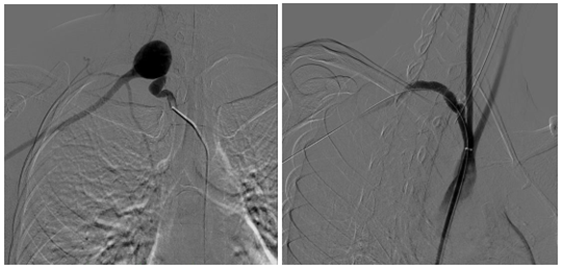
Figure 5: Wrapsody 9x50mm implanted at the right subclavian artery
Case 6
A male patient, 50 years old, with arterial hypertension, diabetes, and chronic kidney disease in hemodialysis was admitted with a previous stent at brachial artery acute thrombosis and previous arteriovenous fistula occlusion. The patient was submitted to thrombectomy and implant of Wrapsody Merit 8x125mm at the brachial artery (Figure 6). The patient was discharged from the hospital second day post-operative and a 2-year follow-up Duplex ultrasound showed endoprosthesis patency with no stenosis.
Pre Post
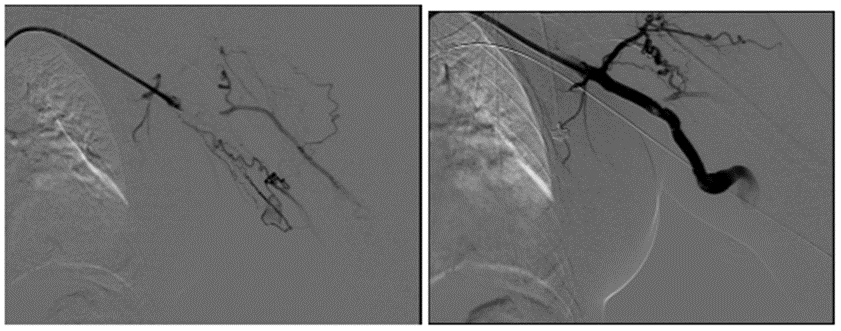
Figure 6. Thrombectomy and implant of Wrapsody Merit 8x125mm at the brachial artery
Discussion
This paper presents a challenging case series report of patients with arterial disease, including arterial iatrogenic lesions, aorta abdominal aneurysm, PAU, and arterial thrombosis treated with a new device covered stent Wrapsody. In this present paper, we reported two cases of arterial iatrogenic lesions that were successfully treated with Wrapsody Merit. Open surgical repair was for a long time the treatment of choice for iatrogenic injuries of peripheral arteries. However, general anesthesia and the patient's underlying comorbidities increase the risk of systemic complications.[9] Therefore, the treatment of these lesions shifted from emergency surgery to an endovascular approach, becoming part of the treatment algorithm.[10] The growing number of percutaneous procedures managing a wide spectrum of cardiovascular diseases is expected to increase the incidence of iatrogenic vascular injuries. Percutaneous transluminal angioplasty with a covered stent has been proposed as an alternative to open surgery in this setting: the possibility to perform stenting under local anesthesia and the wide accessibility to PTA facilities represent arguments supportive of endovascular approach as compared with open surgery. Self-expandable stent-grafts are generally considered more flexible and suitable for tortuous vessels, showing proper results in the treatment of iatrogenic arterial injuries in both peripheral and visceral vessels. Some papers11 reported a 93.5% technical success with 12 months patency rates between 85.7% and 76.4% in 62 patients. Kufner et al12 achieved 100% technical success and a 12-month patency of 100% in 30 patients treated with either self-expandable or balloon expandable stent for iatrogenic arterial injuries. Similarly, in this present paper, the two cases with arterial iatrogenic lesions treated with rhapsody-covered stent presented 100% technical success and 1-year follow-up of 100% primary patency.
Another case reported in this paper was a successful clinical case of a patient with abdominal PAU who was submitted to endovascular treatment with a Wrapsody Merit implant, with 2 2-year follow-up of 100% primary patency and no endoleaks. PAU clinical course is variable, with only 20?ing symptomatic. They have an elusive natural evolution, with rates of progression to intramural hematoma and aortic dissection up to 30% and rupture rates of 40% in selected series.[13]
The most frequent aortic location is the descending thoracic aorta, with over 60% of all PAUs occurring there. Abdominal PAUs make up 30% of the cohort aorta, with the remaining 7% to 10% occurring in the aortic arch.[14] A systematic review of PAU from 2013 reports that around 30% of patients treated up to that point underwent open surgical repair, with 70% receiving endovascular treatment. Endovascular treatment of this condition traditionally includes the use of standard endovascular aortic repair (EVAR) stent grafts or tubular thoracic/iliac extensions.[15] However, there are some papers in the literature reporting good results of the use of covered stents in the treatment of this clinical condition. Stana et al16 evaluated 40 patients undergoing endovascular treatment with the BeGraft aortic stent-graft. The authors reported a technical success of 97.5%, with 30-day mortality of 0%, and no cases of graft migration, thrombosis, or stent-fracture at 13.9 months follow-up. The Merit Wrapsody has a larger diameter, 16mm, which can perfectly outfit at aorta diameter, being a proper and safe solution for treating abdominal PAU and even aortic abdominal saccular aneurysms.
The Merit Wrapsody® is a self-expandable covered stent consisting of Nitinol, ePTFE, and PTFE structure. Self-expanding stents are better suited for tortuous vessels, especially in areas of permanent external forces such as the external iliac artery. These stents guarantee precise placement only on the end that is deployed first, but newer-generation nitinol self-expanding stents exhibit minimal foreshortening at human body temperature and have a more predictable length once deployed in the body. As a rule, the leading end of the device is always maneuvered just past the planned landing zone, allowing for fine adjustments and retraction during its deployment. [3,4] Given the PTFE lining, covered stents may overcome some limitations of standard stent designs by introducing a mechanical barrier between intimal hyperplasia and the arterial lumen. This covering potentially also prevents the migration of macrophages in the vascular wall, which are attracted by proinflammatory mediators secreted by the damaged vessel wall. These macrophages release further cytokines, metalloproteinases, and growth factors that contribute to the initiation of the restenotic process. [3,4]
Another clinical case reported in this paper referred to an arteriovenous fistula and previous brachial artery stent thrombosis, treated with thrombectomy and implant of a new stent Wrapsody Merit successfully. Indeed, the WAVE trial17 evaluated 6-month outcomes of the safety and efficacy of a cell-impermeable endoprosthesis (Wrapsody) versus standard of care with percutaneous transluminal angioplasty (PTA) for treatment of stenosis within the peripheral venous outflow circuit of patients on hemodialysis. Six-month target lesion primary patency and access circuit primary patency were significantly higher for the Wrapsody cohort versus PTA (TLPP: 89.6% vs. 62.3%; ACPP: 72.2% vs. 57.0%). These data are comparable with those found in this study, with 2 2-year follow-ups showing 100% primary patency of the brachial artery and the arteriovenous fistula with the implant of the Wrapsody. This case report series has some limitations since it is a case series report, without a large number of patients. Larger studies should be performed to evaluate the safety and efficacy of endovascular treatment with Merit Wrapsody® for arterial diseases.
Conclusion
Endovascular treatment with Merit Wrapsody® covered stents for arterial disease seems to be a safe and effective alternative for patients with iatrogenic arterial lesions PAU, aortic aneurysm, and arteriovenous fistula occlusion. Further and more robust studies are needed to validate these preliminary results.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The Authors declare that there is no conflict of interest regarding this paper.
Informed consent has been obtained from the patient for publication of the case report and accompanying images.
References
- Tonnessen BH. (2011). Iatrogenic injury from vascular access and endovascular procedures. Perspect Vasc Surg Endovasc Ther 23:128–35.
View at Publisher | View at Google Scholar - Stampfl U, Sommer CM, Bellemann N, et al. (2012). The use of balloon-expandable stent grafts for the management of acute arterial bleeding. J Vasc Interv Radiol 23:331–7.
View at Publisher | View at Google Scholar - Gilbert J. Prospective First-in-Human Study of the Merit WRAPSODY Endovascular Stent Graft for Treatment of Access Circuit Outflow Stenosis in Hemodialysis Patients. Journal of Vascular Surgery Abstracts 7S Volume 75, Number 4S.
View at Publisher | View at Google Scholar - Gilbert J, Rai J, Kingsmore D, Skousen J, Ptohis N. (2021). First Clinical Results of the Merit WRAPSODY™ Cell-Impermeable Endoprosthesis for Treatment of Access Circuit Stenosis in Haemodialysis Patients. Cardiovasc Intervent Radiol. Dec;44(12):1903-1913.
View at Publisher | View at Google Scholar - de Athayde Soares R, Cury MVM, Futigami AY. (2024). Popliteal Artery Aneurysm Treated with Endovascular Technique and New Device: Case Report and Literature Review. JSM Heart Surg Case Images 4(1): 1012.
View at Publisher | View at Google Scholar - Rodolfo M. Mansano, Elias A. Neto, Paulo F. Gasparetto, Rodrigo E. Sahyun, and Igor S. Perozin et.al (2025), The use of a new device for an endoconduit for EVAR: an innovative technique off the shelf, International Journal of Cardiovascular Medicine, 4(1).
View at Publisher | View at Google Scholar - Stanson, A.W. ∙ Kazmier, F.J. ∙ Hollier, L.H. (1986). Penetrating atherosclerotic ulcers of the thoracic aorta: natural history and clinicopathologic correlations Ann Vasc Surg. 1:15-23.
View at Publisher | View at Google Scholar - Javed U, Balwanz CR, Armstrong EJ, et al. (2013). Mid-term outcomes following endovascular re-intervention for iliac artery in-stent restenosis. Catheter Cardiovasc Interv. 82:1176–1184.
View at Publisher | View at Google Scholar - Xiao L, Shen J, Tong JJ. (2013). Emergency stent-graft implantation for iatrogenic peripheral arterial rupture. Radiol Med (Torino) 118:152–7.
View at Publisher | View at Google Scholar - Matsumoto J, Lohman BD, Morimoto K, et al. (2015). Damage control interventional radiology (DCIR) in prompt and rapid endovascular strategies in trauma occasions (PRESTO): a new paradigm. Diagn Interv Imaging 96:687–91.
View at Publisher | View at Google Scholar - White R, Krajcer Z, Johnson M, et al. (2006). Results of a multicenter trial for the treatment of traumatic vascular injury with a covered stent. J Trauma 60:1189– 95.
View at Publisher | View at Google Scholar - Kufner S, Cassese S, Groha P, et al. (2015). Covered stents for endovascular repair of iatrogenic injuries of iliac and femoral arteries. Cardiovasc Revasc Med 16:156– 62.
View at Publisher | View at Google Scholar - Oderich GS, Kärkkäinen JM, Reed NR, et al. (2019). Penetrating aortic ulcer and intramural hematoma. Cardiovasc Intervent Radiol. 42:321–334.
View at Publisher | View at Google Scholar - Nathan DP, Boonn W, Lai E, et al. (2012). Presentation, complications, and natural history of penetrating atherosclerotic ulcer disease. J Vasc Surg. 55:10–15.
View at Publisher | View at Google Scholar - Georgiadis GS, Antoniou GA, Georgakarakos EI, et al. (2013). Surgical or endovascular therapy of abdominal penetrating aortic ulcers and their natural history: a systematic review. J Vasc Interv Radiol. 24:1437–1449.e3.
View at Publisher | View at Google Scholar - Stana J, Fernandez Prendes C, Kruszyna L, Passaloglou IT, Ruffino MA, Reyes Valdivia A, Del Castro Madrazo JA, Oikonomou K, Chan HL, Makaloski V, Tsilimparis N. (2021). Multicenter Experience with Large Diameter Balloon-Expandable Stent-Grafts for the Treatment of Infrarenal Penetrating Aortic Ulcers. J Endovasc Ther. Dec;28(6):871-877.
View at Publisher | View at Google Scholar - Razavi MK, Balamuthusamy S, Makris AN, Hoggard JG, Harduin LO, Roy- Chaudhury P, Jones RG; WAVE Trial Investigators. (2025). Six-month safety and efficacy outcomes from the randomized-controlled arm of the WRAPSODY Arteriovenous Access Efficacy (WAVE) trial. Kidney Int. Jan 23:S0085-2538(25)00063-8.
View at Publisher | View at Google Scholar
