

Research Article | DOI: https://doi.org/10.31579/2835-835X/037
The Challenges and Future of Advanced Therapies
*Corresponding Author: Rizwana Shahid, Assistant Professor Community Medicine, Rawalpindi Medical University, Rawalpindi, Pakistan.
Citation: Rehan Haider, (2023), The Challenges and Future of Advanced Therapies, Clinical Trials and Case Studies, 2(5); DOI:10.31579/2835-835X/037
Copyright: © 2023, Rehan Haider. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 August 2023 | Accepted: 10 September 2023 | Published: 22 September 2023
Keywords: advanced therapies; gene therapies; cell-based therapies; tissue engineering; challenges future; personalized treatment
Abstract
Advanced therapies, including gene therapies, cell-based therapies, and tissue engineering, have emerged as revolutionary approaches in medicine. These therapies hold immense promise for treating previously un treatable diseases by targeting underlying causes at the molecular and cellular levels. However, their translation from laboratory breakthroughs to clinical applications is accompanied by significant challenges that must be addressed to realize their full potential.
One major challenge lies in the complexity and variability of patient responses. The personalized nature of advanced therapies demands precise customization of each individual, necessitating the development of robust biomarkers and predictive models. Ensuring the safety of these therapies is paramount. Unforeseen immune reactions, off-target effects, and long-term consequences require stringent preclinical testing and vigilant post-market surveillance.
Manufacturing scalability is another hurdle. Unlike traditional pharmaceuticals, advanced therapies often involve intricate processes specific to each patient. Standardizing and automating these processes, while maintaining product quality and consistency, are critical obstacles. Moreover, the high costs associated with research, development, manufacturing, and delivery hinder accessibility and affordability, raising concerns about equitable patient access.
The regulatory landscape also requires adaptation to accommodate the unique attributes of advanced therapies. Striking a balance between timely access to patients and comprehensive evaluation of safety and efficacy challenges regulatory agencies globally. Intellectual property concerns, data sharing, and ethical considerations compounded these issues.
Collaborative efforts between researchers, clinicians, regulators, and industry stakeholders will be pivotal in overcoming these obstacles. Technological advancements in gene editing, bio materials, and manufacturing techniques have driven innovations. Additionally, adaptive regulatory frameworks and health policies that foster innovation, while upholding safety standards, are instrumental.
Introduction
Globally, we observe that diagnostic and treatment methods are rapidly changing and is evolving because of epidemiologic and demographic transitions. In this context, personalized medicine is increasingly emerging because of recent technological advances in the provision of healthcare services. Several definitions have been proposed for “personalized medicine” (Box 1). A formal definition can be as follows: “Providing the right treatment, to the right patient, at the right time, with the help of new biomarker-based diagnostic tests.” Such tests help identify patients at high risk, or patients for whom conventional therapies are less effective, or ineffective – i.e., “stratification” [1].

Patients with the same diagnosis respond differently to the same therapy owing to their different genetic and biological endowments. Personalized medicine evaluates these differences on a molecular basis and develops advanced therapies that depend on the patient’s specific needs. This new field, which arises from advanced pharmacology and genomics, is known as Pharmacogenomics [2]. Pharmacogenomics focuses on patients in whom pharmaceuticals are ineffective (Box 2). Personalized medicine and advanced therapies are utilized more in genetic and metabolic illnesses, such as cancer or rare genetic diseases. Recent studies have demonstrated the existence of a significant relationship between certain cancer markers and genes. Therefore, especially for cancer patients with a family history of the disease, genetic tests help reveal important information about the prognosis, risk of metastasis, and sometimes even the possible success of the treatment. Thus, genetic tests help to prevent unnecessary treatments and their associated costs. Personalized medicine helps identify key molecules in cell proteins. Advanced therapies can be designed to intervene with these key molecules, rather than others, and therefore, can be more effective. Owing to technological advances, the possibility of identifying, shortly, with genetic testing, the metabolic structure of individuals seems plausible; each patient will therefore be treated at the right time and with the right dosage of the right medicine. Advanced therapies are expected to develop efficient and successful treatments for many severe orphan diseases and chronic illnesses such as cancer. Furthermore, advances in personalized medicine extend beyond individuals who are already ill and can offer early risk identification and preventive measures for the entire population [3-5]. For example, many pharmaceuticals used in neurological and psychiatric treatments are metabolized by an enzyme called cytochrome P450. The cytochrome P450 class includes more than 50 enzymes responsible for metabolizing over 90% of pharmaceuticals. The genetic variability of these enzymes creates differences in patient responses to various pharmaceuticals. Therefore, gaining information on the genetic structure of the P450 enzymatic class is of great importance in the treatment of several severe and chronic illnesses [6].
Recent Developments in Advanced Therapies
In 2014, after a 14-12 months discovery process, the European fee authorized the First gene therapy, Glybera® (alipogene tiparvovec), for the treatment of lipoprotein lipase deficiency (LPLD, type 1 hyperlipidemia). LPLD is a very rare disorder that is found in 1-2 individuals in 10 million individuals [7]. The initial utility manner for gene therapy for such an extremely uncommon ailment began in December 2009, and the EU government rejected its utility twice because of the lack of huge-ranged efficacy exams. After the very last re-exam in 2012, alipogene tiparvovec was permitted and authorized for advertising inside the EU. However, 5 years after approval, Glybera® was withdrawn from the marketplace no longer because of effectiveness or safety issues, but because of its excessive expenses and restricted use. In August 2017, the FDA introduced the approval of Kymriah® (tisagenlecleucel) for children and teenagers suffering from acute lymphoblastic leukemia (ALL), as a result introducing the first gene therapy into our market. superior remedy pills – that have been advanced and are currently being examined – specially goal-specific, intense, and rare sicknesses, including cancer and cardiovascular, musculoskeletal, immunological, neurological, and hematological conditions. those drugs can be particularly classified as Gene remedy Medicinal merchandise (GTMP), somatic mobile therapy
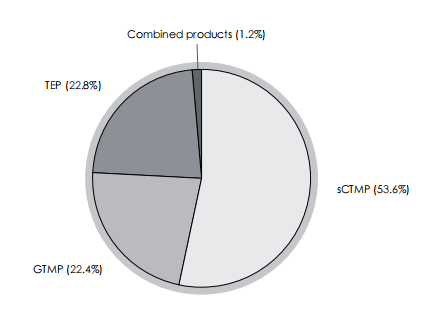
Figure 1: Advanced therapy drugs classification. Modified from [8]
GTMP = Gene Therapy Medicinal Products; sCTMP = somatic Cell Therapy Medicinal Products;
TEP = Tissue Engineered Product
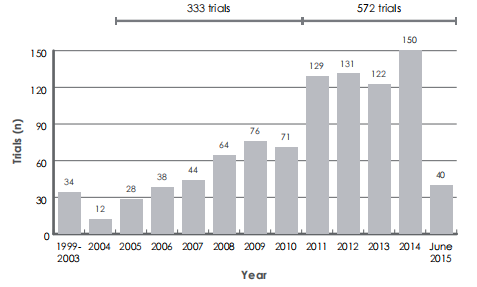
Figure 2: Number of registered trials from 1999 to 2015. Modified from [8]
Medicinal products (sCTMP), tissue-engineered products (TEP), and blended products.
As proven in Part 1, most prescribed drugs are somatic cellular remedies. The development of customized medicinal drugs can be seen in the tremendous increase in the number of trials that have been carried out with superior therapy capsules from 1999 to 2015 (Figure 2).
Even with these high numbers of trials, today (2017), there are the simplest eight superior therapy prescribed drugs available within the EU market and 15 in the US (Table 1). Consequently, it is far more viable to argue that the development of superior remedies for pharmaceuticals and customized medicinal drugs is slower than expected. The reasons for this sluggish progress are three-fold: scientific – the improvement techniques of superior remedy prescribed drugs are complicated and R&D is in-depth; regulatory – there are extensive imperfections within the law of superior therapy pharmaceuticals; and monetary – there are issues regarding value-effectiveness analyses, pricing and reimbursement [1]. similarly, it’s feasible to argue that because of these imperfections, the incentives for personalized remedies and the innovation of superior therapy drugs are not aligned [5]. Even considering the clear fee advantages and social wishes, authorities can be reluctant to pay massive, one-time sums for superior healing procedures for several reasons. First, the effectiveness of the therapy is likely to be in query. Because the approval of advanced treatment options encounters problems with available statistics, the one-time payment has to challenge a “projected” length of efficacy in place of an “actual” period. Second, with current efforts to lower pharmaceutical spending, such amounts can create arguments and criticisms. In particular, sufferers may not use advanced therapies for rare sicknesses. Therefore, even considering their tested effectiveness and price blessings, the reimbursement of superior treatments would possibly result in reluctance on the part of the 1/3-party payers. The authorities’ position ought to also be clarified inside-pricing and repayment choices for superior treatment options. A thoughtful structuring of the repayment gadget will even help pharmaceutical companies to increase the level of investment in superior therapies, which in return will yield better blessings for society [9]. advanced remedies pose a catch-22 situation to health policy government in phrases of significant fitness upgrades and challenges because of imperfections in cost-effectiveness analyses, the market gets an entry, and choices on pricing and reimbursement
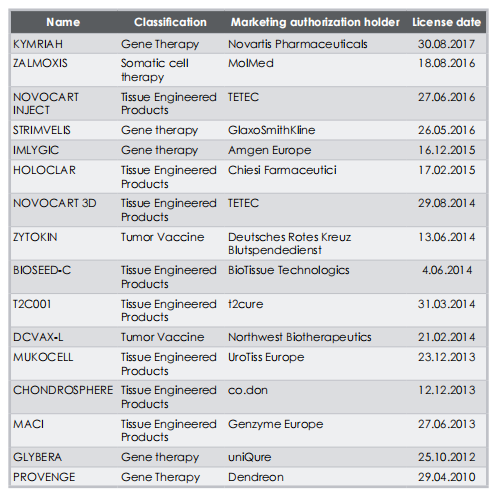
Table 1: Advanced therapy medicinal products currently on the market
Cost-Effectiveness Analysis
Cost-effectiveness analysis (CEA) is widely used in health economics and policy. In short, CEA aims to measure the potential success of any intervention by comparing the relative costs of different actions aimed at achieving the same outcomes or effects [10]. To compare the costs and effectiveness of a course of action, monetary measures for both outcomes and costs must be provided. In terms of health policy, outcomes are usually measured by evaluating changes in life expectancy or improvements in the quality of life. However, measuring these aspects by using money is challenging. The first challenge derives from the basic question of microeconomics: “For whose benefit?”. We can find different values for the same outcome by considering the perspectives of the individual, society, payer, or pharmaceutical company. In addition, as reported by Porter (2010) [11], determining
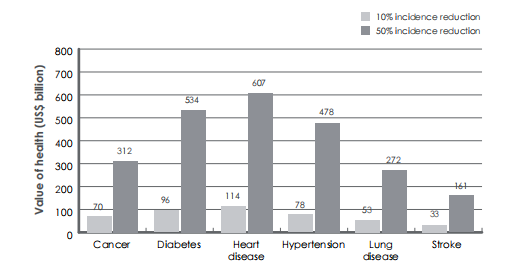
Figure 3: Potential benefits from personalized medicine calculated as cumulative value of additional QALY generated (2012-60, valued at US$ 100,000 each). Modified from [5]
Relative outcomes are a complex process in health economics. Porter [11] proposed a “three-tier hierarchy” for outcome evaluation: the first tier includes “survival”, or “the degree of health recovery; the second tier contains “time to recovery” and “dis utility due to the treatment process; and the third-tier embraces “the sustainability of recovery” and “long-term consequences of the therapy”. Unfortunately, in health economics, only the first tier is typically used, and the other two are ignored in terms of outcome evaluation.
Even with only the first-tier analysis using survival or the degree of health recovery, the individual and social benefits of advanced therapies are undeniable. Dzau et al. [5] use a simulation model to estimate the potential benefits of personalized medicine in early risk detection (Figure 3). With the help of personalized medicine, individual risk levels for diseases such as cancer, diabetes, heart disease, hypertension, lung disease, and stroke can be calculated. With efficient interventions for high-risk individuals, benefits are reported as a 50-year increase in life expectancy, and $ 100,000/QALY has been reported.
Measuring costs can be challenging because of market uncertainties, difficulties in measuring opportunity costs, and external effects [10]. Despite these major challenges, CEA is widely used in both investment and reimbursement decisions in health economics and policy. The nature of advanced therapies makes it even more difficult to perform CEA because it is vital to recognize the risks associated with genetic assessments. moreover, genetic tests are very high-priced, consequently – even though they could provide vital statistics, especially within the early stages of the disorder – because of their excessive prices they may be best adopted at a later degree, after the failure of several treatments.19.4 marketplace gets entry In 1906, the federal US government delivered the Meals and Drug Act. In 1962, amendments to this Act gave the FDA an assignment to test and approve new prescription drugs.
Market Access
In 1906, the federal US government introduced the Food and Drug Act. In 1962, the
amendments to this Act gave the FDA the task to test and approve new pharmaceuticals The FDA evaluation manner – which is lengthy and complicated – has 3 phases. together with the studies and development (R&D) method, a brand-new drug is anticipated to take an average of 14 years to be evolved [10]. other than the entry obstacles, the extreme R&D system, and the guidelines regarding safety and fitness generation tests (HTAs) can restrict or postpone market access to the most recent prescription drugs. restricted and not on time get entry to is more said with advanced treatment options since they are individual-specific and may not assume controlled trials with a large number of patients. After the mid-1970s, the FDA added new guidelines to accelerate the approval process for “crucial” prescription drugs. Consistent with Philip Son et al. [12], the lower approval times following the new FDA regulations caused sizable improvements for patients owing to faster access to prescribed drugs. As noted by Olson et al. [13], this speedy access incorporates the dangers associated with a boom in unfavorable reactions. over the past decade, superior healing procedures originated a big debate, due to the rapid technological enhancements and the media attention on the difficulty: therefore, the FDA and the EMA carefully monitored and addressed this problem. In the Twenty-First Century Treatment Plans Act, the FDA described prescription drugs eligible for regenerative medication superior remedy (RMAT). Consistent with phase 3033 of the 21st Century Cures Act, a drug is considered RMAT if it entails “cell therapy, therapeutic tissue engineering products, human cellular and tissue products, or any aggregate using such treatment plans or merchandise”. Furthermore, the EMA defines superior therapy medicinal products (ATMPs) as “drugs for human use that are based entirely on genes or cells”. A Committee for superior remedies (CAT) monitors the protection and efficacy of such pharmaceuticals.it is crucial to well know the want for advanced treatment options and their capability benefits for the character’s life expectancy and nicely-being. while R&D efforts continue to grow in this area, it’s important to find and advise solutions to deliver superior therapy prescription drugs to the marketplace as soon as possible. in addition, the need for a law of such pharmaceuticals in phrases of protection, effectiveness, and repayment is essential for obtaining a much broader entry into these capsules [14]. Finally, for you to avoid delays in the market and get admission, regulatory approval methods need to be harmonized. Early market admission is essential for each pharmaceutical organization and patient; however, the dangers related to an early get right of entry need not be noted. Due to the shortage of several efficacy facts, including those from randomized managed trials, the dangers associated with advanced therapies are greater than those associated with traditional drugs. Policymakers should be willing to take higher risks for rare life-threatening diseases. Acknowledging such a need in health policy, both the EMA and the FDA offer a “fast track” option in the case of advanced therapies, stating, however, that the increased level of risk acceptability is – and must be – temporary. The main problem is that pharmaceutical companies take advantage of this earlier access, while regulatory agents take risks. This situation can be considered an example of a principal-agent problem: in health economics, it occurs when companies (agents) are acting to maximize their profits, while increasing the risk for patients, especially when regulatory institutions, such as the FDA and the EMA, bear this risk [15,16]
Pricing and Reimbursement Policies
The increasing importance of advanced therapies also brings to our attention the discussion on the pricing and reimbursement of such therapies. To foster investment in advanced therapies, it is estimated that spending over $1 million is necessary. However, the potential economic advantages of advanced therapies should be considered. Brennan and Wilson [9] cite in vivo gene therapy for hemophilia B as an example. The cost of the standard therapy for hemophilia B, which is a rare, severe disease affecting 1 in 20,000 males, is equal to $ 200-300,000 per year, for a total of $ 4-6 million (lifetime treatment), while in vivo gene therapy, which costs just over $ 1 million and requires a one-time treatment, is less expensive. Most countries have experienced a rapid increase in healthcare expenditures over the last 50 years. Moreover, there is concern that most countries will not be able to finance their healthcare expenditures in the future [17]. Pharmaceutical expenditure comprises approximately 10-15% of health spending. In other words, pharmaceutical expenditure is a significant driver of increased healthcare costs in most countries. Table 2 shows the proportion of total health expenditure in gross domestic product (GDP) for the selected OECD countries. It is clear that for all countries, there is an upward trend, which implies a considerable burden on budgets. However, it is also important to mention that pharmaceutical expenditure has been found to have significantly positive effects on patients’ life expectancy [18].
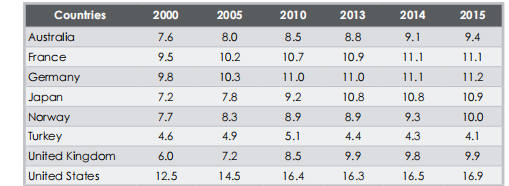
Table 2: Proportion of total health expenditure in GDP for selected OECD countries [OECD Statistics]

Table 3. Proportion of pharmaceutical expenditures compared to total health spending
for selected OECD countries [OECD Statistics]
Table 3 shows the proportion of pharmaceutical expenditure compared to total health spending for selected OECD countries. Despite the introduction of new technological pharmaceuticals in the market, there is a surprisingly decreasing trend in the share of drug expenditure concerning total health spending. This declining trend can be attributed to a series of pricing policy interventions and the penetration of generic drugs in most countries.
Despite the cost-reduction trend which occurred in recent decades, pharmaceutical companies have experienced rapid growth rates in terms of their size and profits. This growth rates attracted the attention of the media, society, policymakers, and insurance companies, and introduced several challenges in terms of expenditure and reimbursement [10]. The delicacy of the issue and the structure of the pharmaceutical market make regulations very important. In a context characterized by monopolistic competition, with a small number of companies, differentiated products, active barriers to entry, and high levels of profit, pharmaceutical companies possess market power; hence, they can increase prices beyond marginal costs and discriminate between prices. As is well-known in microeconomics, these issues lead to a decrease in efficiency [19].
The barriers to entry into the pharmaceutical industry are of great importance. A barrier to entry is defined as any factor that restricts the entry of new companies into the existing markets [20]. Patents, which are highly utilized in the pharmaceutical industry, are the best examples of entry barriers [21]. With active barriers to entry, certain companies can have monopoly power over a specific product and enjoy high levels of profit for a certain period; therefore, the social surplus decreases. In the pharmaceutical industry, companies actively use patents (with many variations of the product) to impede entry [10]. Because of this, it is possible to argue that the pharmaceutical industry is the most heavily regulated worldwide in terms of safety, market access, and reimbursement. Prices in the pharmaceutical industry have long been discussed, due to the high levels of profit for the industry. Pricing strategies depend on the monopoly power of the companies and the monopsony power of the legal Authorities over the pharmaceutical industry, as well as R&D spending, risks involved, price discrimination, regulations, and competition levels. In addition to the similar attributes in terms of safety and efficacy issues, pricing and reimbursement strategies differ among countries and health systems. Price and reimbursement decisions are key concepts for the market access of drugs. When advanced therapies are considered, pricing and reimbursement are even more controversial, due to the high costs associated with such therapies. On the other hand, early market access is important for advanced therapy pharmaceuticals, since they mostly target severe and chronic illnesses.
According to Lu and Comanor [22]. the prices of new pharmaceuticals with significant therapeutic contributions, determined by FDA ratings, are higher at the time of introduction, with premiums ranging from 51 to 79%. The prices of high-ranking pharmaceuticals decline at a slower rate over time, compared to low-ranking pharmaceuticals. A high level of competition from branded rivals negatively affects introductory prices, whereas generic competition has a positive impact. Therefore, Lu and Comanor [22]. conclude that the main strategy when introducing an innovation is the “skimming strategy” – where the highest introductory prices are lowered over time – and if the drug is an imitative (generic) product, the pricing strategy is classified as “penetration strategy” – where a lower price is offered for a new product, to lure customers, proving Dean’s [23]. hypothesis. Prices in the pharmaceutical industry are also closely related to the associated risk levels. Risks can arise from the chemical property of the drug, as well as the regulations. The perception of high prices and profits – whether justified or not – and increased health expenditures in the pharmaceutical industry leads to heavy regulations and price controls.
The main aim of these price controls is to decrease public spending on pharmaceuticals while increasing social benefits. There are different types of price control used by the Authorities, such as; reference pricing, item-by-item negotiation, formula pricing, profit regulation, and budgetary controls (line item and global budget) [24]. In the reference pricing system, pharmaceuticals are grouped and compared within their reference groups, and the lowest price is paid within the group [25]. Reference groups can be based on active ingredients – as in the US – or on disease – as in Germany. However, since advanced therapy pharmaceuticals are heavily personalized, a reference group pricing system is not plausible. Many countries, such as Italy and Canada, also use the prices of similar pharmaceuticals in other countries as references. This drives down the price of drugs of multinational companies, through increasing international competition. Once again, such a strategy is also not possible in the case of advanced therapy pharmaceuticals. Formula pricing is used in Japan, where pharmaceuticals are priced through their formularies. The UK uses the profit regulation system, where companies negotiate with the Authority, are allowed a certain percentage of profit, and set the price accordingly. This leaves big companies with high R&D costs with higher levels of return since the profits are calculated after R&D and other costs are deducted. Such a policy is plausible for advanced therapy pharmaceuticals; however, Authorities will have to face even higher levels of pharmaceutical expenses and increasing levels of company profits. Pricing policies and regulations differ for each country worldwide. Even within the EU, where the drug approval systems are homogeneous, local governments make decisions about pricing and reimbursement
Research Method:
Study design:
An assorted orders approach was secondhand for this study to comprehensively address the challenges and prospects of progressive medicines. Qualitative dossiers were calm through expert interviews, while determinable dossiers were collected through a connected internet survey.
Data Collection:
Expert interviews:
A resolved-to-do-something inspecting arrangement was used to select 15 masters engaged in advanced medicines, containing scientists, clinicians, supervisory masters, and manufacturing representatives.
Semi-organized interviews were administered to investigate the challenges and potential future incidents of state-of-the-art cures. Interviews were written and transcribed for reasoning.
Online survey:
The connection to the Internet survey was created to gain a more extensive view of the challenges of leading therapies. The survey was delivered to healthcare pros, scientists, and things accompanying knowledge in the field.
The survey contained independent-done questions about challenges, costs, supervisory issues, and the function of science. It also contains unlimited questions for the accused to determine approximate visions.
Data study:
Expert interviews:
Thematic analysis was used to label universal ideas and patterns in the interview transcripts. The process complicated systematized the dossier, grouping the codes into ideas, and cleansing the ideas through repetitive study.
Online survey:
Quantitative survey dossiers were analyzed utilizing explanatory enumerations to recognize flows and reaction frequencies.
The qualitative dossier from unlimited survey questions was endangered content reasoning including classification and labeling of recurring plans.
Result:
Challenges finish for dress goods state-of-the-art analyses:
A qualitative study of interviews accompanying experts told various persisting issues:
Personalized situation: The complicatedness of adjusting therapies to individual subjects presents challenges in forecasting reactions and cultivating patterned obligations.
Safety Concerns: Unexpected immune answers, off-course belongings, and general sequelae demand severe preclinical experiments and vigilant Postmarketing following.
Manufacturing scalability: Tailored processes for each patient preclude scalability. Standardizing and automating processes while upholding conditions is a fault-finding hurdle.
Access and affordability: The high costs of research, incident, and result raise concerns about the impartial patient approach to these healing.
Future prospectuses:
The results of the survey designated a consensus with the accused concerning the prospects of new healing:
Technological advances: The duty of gene refining, organic matters, and computerization in healing happening and production has been emphasized.
Regulatory Adaptation: Respondents emphasize the significance of responsive supervisory foundations that balance patient safety accompanying appropriate approaches to creative medicines.
In conclusion, the labeled challenges underscore the complex character of translating progressive cures from the workshop to the hospital, while expected progress and regulatory agreement precede their hopeful future.
Discussion and Perspectives
Given the recent developments in technology in the pharmaceutical industry, advanced therapies will be on our agenda in the coming years. Initiatives regarding the legislation, regulation, and pricing strategies for advanced therapies must be taken early in the process, for increased social benefits. Unfortunately, the current level of regulations regarding pricing and reimbursement is not promising. Several questions need to be answered, such as: Will governments and/or health insurance companies reimburse advanced therapy pharmaceuticals? How will the reimbursement/insurance policy work in advanced therapy pharmaceuticals? Authorities should commit to eliminating the grey areas in terms of advanced therapy pricing and reimbursement. Apart from the reimbursement decisions, a harmonization of the approval processes of advanced therapy pharmaceuticals seems necessary to ensure early market access.
European and US legislation and regulations regarding testing, manufacturing, marketing, and use of advanced therapy products should be harmonized, to produce effective results within personalized medicine. Advanced therapy reimbursement options and strategies are very important in personalized medicine, and should urgently be addressed by all countries. Data collection at an early stage is also of great importance for reimbursement decisions. Ideally, pricing and reimbursement issues should be addressed during the phase of discovery of advanced therapy medicinal products. In addition, the costs associated with advanced therapies should be assessed, and decision-makers should consider the possible effects of increased health expenditures [26]. To create successful policies, all stakeholders – such as scientists, universities, hospitals, pharmaceutical companies, and governments – should be involved in the decision-making process [27].
1. Regulatory and Pricing Challenges:
The countryside of progressive therapies is apparent by rebellious potential, still, the journey from laboratory novelty to dispassionate exercise is not without hurdles. Regulatory foundations, two together in Europe and the United States, present sure inconsistencies that can hinder effective advertising access for leading medicine pharmaceuticals. These disparities power bring about delays in patient approach to life-changing situations. The differences in managing highlight the need for worldwide cooperation to correspond to regulatory guidelines, guaranteeing that novelty is met with rapid and united approvals across domains.
2. Reimbursement Strategies:
The intricate character of state-of-the-art cures necessitates tailor-made compensation methods that accommodate their embodied character. At present, doubts surrounding compensation by administration instrumentalities and health insurance providers relate to an impartial patient approach. Clear and transparent compensation procedures should reside to address these concerns. As governments and insurers endure novel medicines, there's a space to pioneer creative compensation models that align accompanying the different ness of state-of-the-art therapies.
3. Early-Stage Consideration:
The importance of trying to fix, reimbursement, and supervisory concerns all the while the discovery time of state-of-the-art remedy medicinal devices cannot be exaggerated. Early-stage disputes can prevent harmful delays and promote a more modernized transition from growth to retail. Initiatives that strengthen proactive cooperation 'tween researchers, managers, and manufacturing colleagues can lead to up-to-date adaptations in supervisory pathways and ensure that costing and compensation devices are thoughtfully organized into the novelty process.
4. Collaboration and Stakeholder Involvement:
The versatile challenges posed by leading analyses demand a combined approach from various partners. Scientists, academies, clinics, pharmaceutical associations, and governments all play important acts in shaping the course of these remedies. Collaborative accountability can bridge knowledge breaks, help the giving of expertise, and authorize a well-balanced understanding of the complicated interplay middle from two points of controlled breakthroughs, regulatory foundations, and patient needs.
5. Data Collection and Evidence-Based Decision-Making:
Central to forming productive reimbursement blueprints is the group of healthy, evidence-based dossiers. Early-stage dossier accumulation can provide judgments into situation efficiency, long-term consequences, and cost influence. By setting decisions in practical evidence, supervisory instrumentalities and policymakers can navigate the complicatedness of progressive cures with better assurance, happening in more informed and reasonable determinations that had a connection with pricing and compensation.
6. Future Directions:
As science continues to develop and the potential of leading remedies becomes more and more apparent, it is incumbent upon collaborators to adapt to change ful chances. Technological progress in gene refining, mechanization, and production techniques holds promise for defeating a few of the current challenges. The development of regulatory foundations and healthcare tactics will be partly responsible for creating an atmosphere that nurtures novelty while conserving patient welfare.
Conclusion:
The intersection of advanced therapies, regulatory frameworks, and pricing strategies necessitates a proactive and collaborative approach. Addressing these challenges early on, harmonizing regulations, and establishing transparent reimbursement mechanisms are crucial steps toward realizing the potential of advanced therapies in personalized medicine. The road map to success lies in the hands of a united global effort involving scientists, regulators, industry professionals, and governments alike.
Acknowledgment
The completion of this research project would not have been possible without the contributions and support of many individuals and organizations. We are deeply grateful to all those who played a role in the success of this project, We would also like to thank My Mentor [. Naweed Imam Syed Prof. Department of Cell Biology at the University of Calgary and Dr. Sadaf Ahmed Psychophysiology Lab University of Karachi for their invaluable input and support throughout the research. Their insights and expertise were instrumental in shaping the direction of this project
Declaration of Interest
I at this moment declare that:
I have no pecuniary or other personal interest, direct or indirect, in any matter that raises or may raise a conflict with my duties as a manager of my office Management
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Financial support and sponsorship
No Funding was received to assist with the preparation of this manuscript
References
- Garrison LP, (2014).Towse A. Personalized Medicine: Guidelines for Pricing and Reimbursement as a potential barrier to development and adoption, Economics. In: Culyer AJ(ed). Encyclopedia of health economics. San Diego: Elsevier.
View at Publisher | View at Google Scholar - (2013). American foods and drug administration. We prepare the way for a tailor-made remedy:FDA's Role in New Technology Medical Product Improvement.
View at Publisher | View at Google Scholar - Hamburg MA, Collins FS. (2010). Towards a tailored medicine. N Engl J Med;363: 301-304
View at Publisher | View at Google Scholar - Foroutan B. (2015). personalized medication: Evaluation concerning biomarkers. J Bioequiv Availab; 7: 244-256
View at Publisher | View at Google Scholar - Dzau VJ, Ginsburg GS, Van Nuys K, et al. (2015). Aligning incentives to fulfill a promise of personalized medicine. Lancet, 385: 2118-2119
View at Publisher | View at Google Scholar - Lynch T, Speed A. (2007). Influence of cytochrome P450 metabolism on drug response,Interactions and side effects. Am Fam Physician. 76: 391-396
View at Publisher | View at Google Scholar - Burnett JR, Hooper AJ, Hegele RA. Familial lipoprotein lipase deficiency. In: AdamMP, Ardinger HH, Pagon RA, et al. (eds.). Seattle (WA): College of Washington, (1993-2018).
View at Publisher | View at Google Scholar - Hanna E, Rémuzat C, Auquier P, et al. (2016). Medicinal products for modern treatment:the present and a view of destiny. J Mark Get Access to Fitness Coverage.
View at Publisher | View at Google Scholar - Brennan TA, Wilson JM. (2014). A unique case of the price of a gene drug. Nat Biotechnol; 32: 874-876
View at Publisher | View at Google Scholar - Folland S, Goodman AC, Stano M. (2016). The economics of health care and fitness.London: Taylor & Francis Ltd.
View at Publisher | View at Google Scholar - Porter ME. (2010). What is the value of fitness care? N Engl J Med, 363: 2477-2481.
View at Publisher | View at Google Scholar - Philipson T, Berndt ER, Gottschalk AH, et al. (2008). Evaluation of price and convenience FDA: The Case for the Number of Prescription Drug Users. J Public Econ; 92:1306-1325.
View at Publisher | View at Google Scholar - Olson MK. (2008). The chance we take: speed and industrial consumer price evaluation results on safety of new drugs. J fitness Econ, 27: 175-200.
View at Publisher | View at Google Scholar - Dunoyer M. (2011). Accelerating access to the treatment of uncommon diseases. Nat Rev Drug Discov, 10: 475-476.
View at Publisher | View at Google Scholar - Eichler HG1, Pignatti F, Flamion B, et al. (2008). Balancing the early market to gain the right of entry to the new benefit/danger information pills: assembly catch-22 situation. Nat Rev Drug Discov, 7: 818–826.
View at Publisher | View at Google Scholar - Nguyen H. (2011). Important agent issues in fitness care: evidence from prescribing patterns of personal providers in Vietnam. fitness coverage plan; 26:53-62.
View at Publisher | View at Google Scholar - Erixon F, van der Marel E. (2011). What drives health care spending to increase?: An investigation of the nature and causes of the price disease. Brussels: the European Center for the global political financial system,Challenging situations and the fate of advanced treatment plans
View at Publisher | View at Google Scholar - Çalışkan Z. (2009). Relationship between pharmaceutical expenditure and life expectations: evidence from 21 OECD countries. applied economics letters.16:1651-1655
View at Publisher | View at Google Scholar - Carlton DW, Perloff JM. (2015). today's business organization. Boston: Pearson.
View at Publisher | View at Google Scholar - Waldman D, Jensen E. (2016). Commercial organizations: idea and practice. Oxford:Routledge.
View at Publisher | View at Google Scholar - 21.Çalışkan Z. (2 008). Health Economics: A Conceptual Method. Hacettepe University Journal of Economics and Administrative Sciences; 26: 29–50.
View at Publisher | View at Google Scholar - Lu ZJ, Komanor WS. (1998). Strategic valuation of current medicines. Evaluation Economics and Records, 80: 108–118.
View at Publisher | View at Google Scholar - Dean J. (1969). The pricing of pioneering products. Journal of Business Economics, 17:165-179.
View at Publisher | View at Google Scholar - Scherer FM. (2000). Pharmaceutical company. In Culyer AJ, Newhouse JP (eds).Handbook of Health Economics, Vol. 1. Amsterdam: Elsevier.
View at Publisher | View at Google Scholar - Çalışkan Z. (2008). Reference prices and the pharmaceutical market. Hacettepe magazine fitness management, 11: 49–75
View at Publisher | View at Google Scholar - Atilgan E, Kilic D, Ertugrul HM, et al. (2017). Dynamic dating between health spending and the economic boom: is health-led boom speculation legitimate?Turkey? Eur J Fitness Econ,18: 567–574
View at Publisher | View at Google Scholar - Erben RG, Silva-Lima B, Reischl I, et al. (2014). A white paper on the way forward completely advanced cell-based treatment options in Europe. Tissue Eng Part, 20: 2549–2554
View at Publisher | View at Google Scholar
