

Review Article | DOI: https://doi.org/10.31579/2835-8325/135
Temporomandibular disorders treatment, symptoms
1 Dental-College HITEC Institute of Medical Sciences, Taxila, Pakistan
2 Department of Microbiology, MNSUAM, Pakistan.
*Corresponding Author: Fatima Mazhar, Department of Microbiology, MNSUAM, Pakistan.
Citation: Maryam Shafqat, Arshia Shaukat, Amina Ejaz, Fatima Mazhar. (2024). Temporomandibular disorders treatment, symptoms, J. Clinical Research and Clinical Reports, 6(1) DOI: 10.31579/2835-8325/135.
Copyright: © 2024 Fatima Mazhar. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 October 2024 | Accepted: 15 November 2024 | Published: 12 December 2024
Keywords: TMDs; symptoms; treatment; causes
Abstract
One typical sign of TMJ illness is joint and muscle pain related to temporomandibular joint disorders. Vertigo, ringing in the ears, hearing loss, jaw stiffness, limited mobility, or locking of the jaw joint are some of the symptoms that might appear at the same time. The jaw joint may also hurt while opening or closing the mouth. Scientists study their mechanisms and genetic makeup.
Introduction
Together, these illnesses are referred to as "temporomandibular disorders" (TMDs), because they affect the jaw joint and muscles, causing pain and dysfunction. [1] said that "TMJ" only refers to the temporomandibular joint, whereas "TMDs" refers to the illnesses. There is one TMJ on each side of the jaw. Put your fingers in front of your ears and open your lips to listento them [2].
Although injuriesto the jaw or temporomandibular joint are possiblecauses of TMDs, theprecise etiology of TMDs is frequently unknown. Many people report being unable to pinpoint the exact cause of their symptoms. Recent research suggests that a person's pain threshold, genetics, and psychological and life stressors may all influence the occurrence and prognosis of TMD [3]. Researchers are attempting to ascertain if the differences in the anatomyand mechanics of the TMJ between the sexes contribute to the higher prevalence of TMDs in women than in men. The idea that TMDs are brought on by orthodontic braces or a misaligned bite is not supported by research. [4].
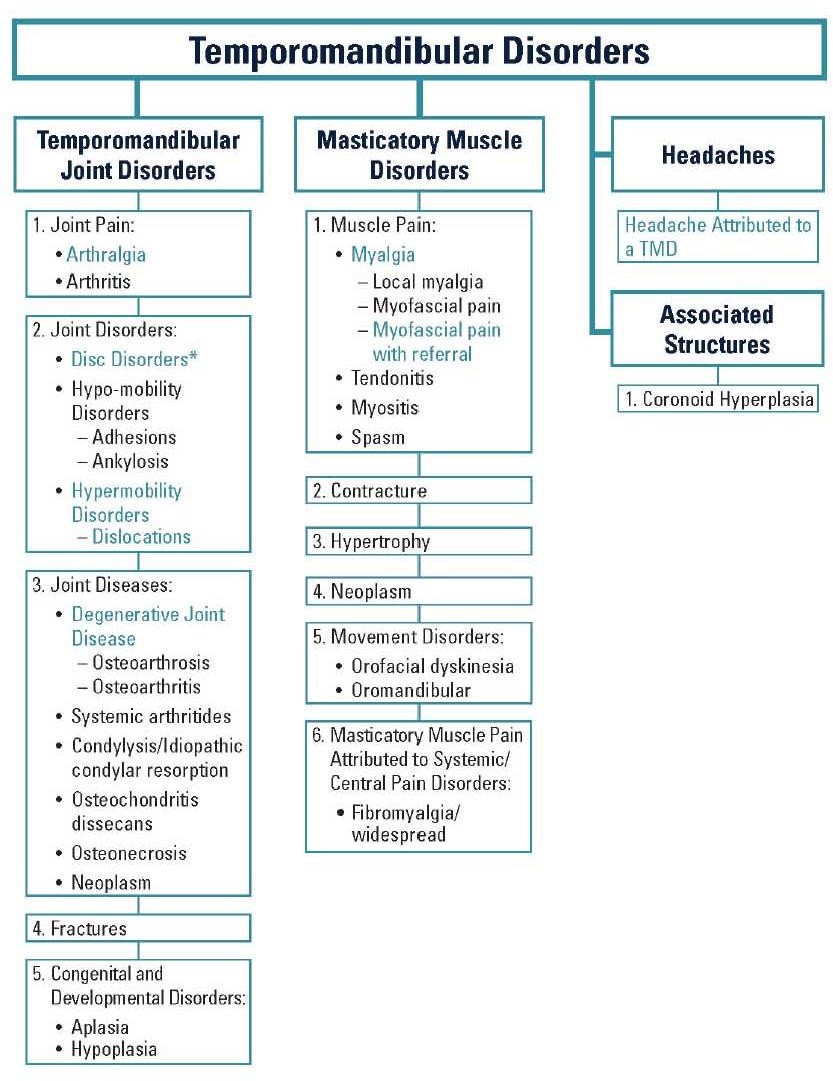
Figure1: Temporomandibular disorder overview
These indicate the situation. Remember that popping or clicking sounds in the TMJs that are not painful are normal, natural,and don't need to be treated. However,these symptoms could point to a TMD: soreness in the jaw and chewing muscles (the most common symptom), swelling that ascends the body, jaw discomfort, jaw lock, limited movement of the jaw, discomfort in the jaw joint caused by popping, clicking, or grinding when chewing hearing loss, ringing in the ears, vertigo, and A change in the way the two sets ofteeth are related [5].
Diagnosis
The patient looks for jaw pain, jaw cracking or clicking, or difficulty moving their head, neck, or jaw. Imaging examinations such as CT scans, x-rays, or magnetic resonance imaging (MRI) may also be recommended by dental and medical specialists. It is questionable if TMDs are the cause of discomfort in the mouth, jaw, or face. Before diagnosing TMD, a physician or dentist might need to rule out other potential reasons [6].
Treatment
The following are things to be aware of before beginning TMD therapy:
- If you hear normal, common, and painless noises coming from your temporomandibular joints, you don't need to go to the doctor. Many TMD patients report considerable relief in their symptoms even in the absence of treatment.
- Since there is little evidenceto support the majority of TMD therapies, specialists advise avoiding operations or other treatments that permanently change the bite, jaw joints, or teeth [7]. Nonsurgical Treatments Many of the joint and muscle problemsof the jaw are transientand do not get worse over time, so a simple therapy plan could be enough. as soon as you notice any jaw or impacted muscle ache.
Stick to soft foods
Exercises for strengthening and extending the jaw muscles may be beneficial in addition to applying heat or ice to the face.
- Take nonsteroidal anti-inflammatory drugs (NSAIDs), which are availableover-the-counter and includeibuprofen [8]. At this point, your dentist or physician may diagnose a particular type of TMD, or if those treatments don't work, they may recommend one or more of the following.
Physical Therapy
The purpose of physical therapy is to assist patients in regaining, maintaining, or improving their function and mobility. There are various types of physical therapy. One way to do this is by manual therapy, in which a therapist stretchesthe muscles and connective tissues surrounding a joint by hand. There is ample evidence on the impact of manual therapy on pain and function.[9]. Research has shown that specificbehavioral health techniques, frequently offered by psychologists, can help with TMD treatment. Cognitive behavioral therapy and biofeedback are a couple of these. Cognitive behavioral therapy seeks to help patients identify and change harmful thought patterns in addition to teaching coping skills. Biofeedback uses sensors that measure body temperature, heart rate, breathing rate, and muscle contractions. Your jaw's sensor may be able to tell when you clench your muscles. With a therapist's assistance, you can identifythe bad behavior and learn how to relax [10].
Medications
Your dentist or doctor may recommendmedicine to treat your symptoms.These include:
- Prescription drugs, such as non-steroidal anti-inflammatory drugs (NSAIDs),which are usedas pain relievers.
- Prescription medications, such as:o Anxiety medications.
- medications for the treatment of depression. medication intended to stop seizures.
- chemicals that are classified as opiates [11].
Intraoral Appliances
appliances that fit over teeth are known as intraoral ones. They do not affect the bite or teeth in any way. Other names for these devices include night guards, bruxism splints, stabilization appliances, splints, and inter occlusal splints. Few studies have demonstrated that they reduce TMD-related pain. If a dentist or other health care provider suggests using them:
- It's not meant to permanently change the way you bite. Stop using it and see your doctor or dentist if it hurts.
Complementary Treatments
Treatments that are used in conjunction with traditional medicine but do not form part of it are known as complementary therapies. Two complementary therapies that have been researched for TMDs include acupuncture and transcutaneous electrical nerve stimulation (TENS) [12]. The phrase "acupuncture" refers to a technique whereby skilled practitioners apply pressure to specific anatomical locations, often by using tiny needles that are put beneath the skin. There is little proof that ithelps with TMDs.
TENS is an electrode-based, battery-powered skin application device. The electrical impulses produced by the apparatus have the potential to alter how pain is perceived. Transcutaneous electrical nerve stimulation (TENS) has shown promise in reducing pain associated with TMJs and enhancing the ability to open the jaw, despite the limited data from trials employing short TENS treatments [13].
Surgery and Other Medical & Dental Procedures
The treatments listed here are more extensive and intrusive than others; they entail changing your bite and teeth alignmentor introducing devices into your temporomandibular joints or jaw muscles. Certain techniques, like the occlusal therapies that are covered below, are ineffective and could even make your issue worse. Prior to having any of these operations done, you ought to: • Look into and test out less invasive choices. • Request a thorough and easily understood description of the treatment from your dentist or doctor. • Find out how the treatment will benefit the specific TMD you have. • Find out what dangers are present. • Consult with knowledgeable dentistsor medical professionals.
Occlusal Treatments
The fit of a person's teeth is known as their occlusion. Research has refuted the long-held theory that misaligned teeth, or malocclusion, is the primary cause of TMDs. The jaw and dental alignmentare altered by orthodontic therapy(Balaji and Senkumar). Here are few instances:
- Applying dental crowns to seal teeth.
- Bruxism, or teeth grinding.
- Repositioning one or more teeth by use of orthodontic therapy or procedures These occlusal interventions have little evidenceof benefit and may worsenthe condition.
A Botulinum toxin It functions by relaxing muscles using a particular kind of botulinum toxin. It is FDA-approved for various conditions (including migraines), but TMDs are not one of its approved uses. In an effort to lessen excruciating chewing muscle spasms, researchers have [14].
Prolo therapy
As part of Prolo therapy, an irritating solution is injected into the TMJ area to promote the body's healing reaction and restore joint function. Prolo therapy has demonstrated promising outcomes in the treatment of TMDs, especially when the joint is dislocated or hypermobilized—that is, moves beyond its normal range of motion. There haven't been many studies conducted on this type of TMD treatment [15].
Arthrocentesis
During this operation, fluids are injectedinto the TMJ using a needle. The fluid pressureremoves adhesions, or scar tissue. Once the liquid is emptied out, the joint is also free of chemicals that cause inflammation. For individuals with a misplaced temporomandibular disc, arthrocentesis may reduce pain and improve mouth opening, but these advantages soon wear off [16].
Arthroscopy
The doctor puts a gadget with a tiny video camera into the jaw joint during an arthroscopy. When the physician can view the joint, diagnosis is made easy. He or she could also realign the joint disc or eliminate adhesions. With this approach, functional ability and pain thresholds are only slightlyraised.[17].
Surgery
During open surgery, an incision made near to the ear may provideaccess to the temporomandibular joint. Remember that following surgery, there will be permanent changes to your joint. There haven't been any long-term studies looking at the safety or effectiveness of open surgeryfor TMD symptom relief.
Getting an is something you should only consider if:
The joint has irreversible damage that cannot be fixed by conventional procedures.
- The severe symptoms (pain and/or difficulties opening the mouth) are not significantly improved by other therapies.
Replacement of the TMJ
Implants are prosthetic devices that are used to restore mobilityin the tyre joint or jaw. The FDA has authorized three TMJ implantsthus far. When should implantsbe taken into account?
The joint has been injured.
People who had dental implants, which were formerlycommon but are now unavailable, experienced severe issues, including permanent damage to their jaw joint(s). As a result, in order to assess the effectiveness and safety of TMJ implants, experts have advocated for long-term follow-up studies.Before having any operation, especially one involving implants,patients should carefully weigh the risks involved and speak with many doctors. It is best to visit TMD- focusedsurgeons whenever feasible.
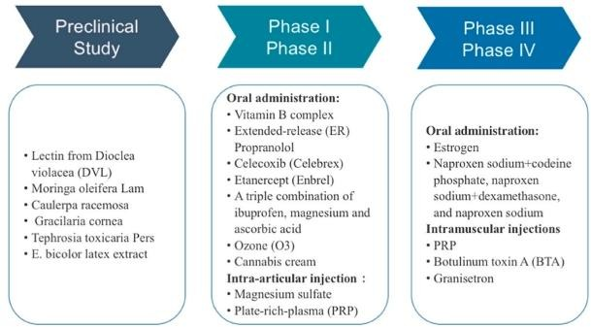
Figure 2: Summary of Treatments for Temporomandibular Disorders (TMDs)
Remember that starting with simple solutions is the best course of action for treating TMD symptoms, which typically go away withouttreatment. Speak with a dentistor physician.
- Learn everything you can about your traumatic brain injury.
- If at all possible, avoid treatments that involve accessingor permanently altering the jaw joints,such as TMJ implants or surgery.
- Before having surgeryor any other dental or medical procedurethat permanently changesyour look, see an orofacial pain clinic if at all feasible.
Conflict of interest: The authors have no conflict-of-Interest Contribution Statement: All authors contribute Equally Funding: No funding for this research.
References
- Ohrbach, R., et al., (2021). Temporomandibular disorders. Burket's Oral Medicine: p. 349- 417.
View at Publisher | View at Google Scholar - Clukey, J.L., (2022). A Voice Teacher's Guide to Temporomandibular Disorders. Shenandoah University.
View at Publisher | View at Google Scholar - Szarejko, K.D., et al., (2023). Stress Experience, Depression and Neck Disability in Patients with Temporomandibular Disorder—Myofascial Pain with Referral. Journal of Clinical Medicine. 12(5): p. 1988.
View at Publisher | View at Google Scholar - Karkazi, F. and F. Özdemir, (2020). Temporomandibular disorders: fundamental questions and answers. Turkish journal of orthodontics. 33(4): p. 246.
View at Publisher | View at Google Scholar - Freyne, B., et al., (2024). Pain Patterns of the Temporomandibular Joint Dysfunction and Implications of Stress-Related Behaviors: A Pilot Study. International Journal of Morphology. 42(1).
View at Publisher | View at Google Scholar - Yost, O., et al., (2020). Caring for Individuals with a TMD, in Temporomandibular Disorders: Priorities for Research and Care, National Academies Press (US).
View at Publisher | View at Google Scholar - Busse, J.W., et al., (2023). Management of chronic pain associated with temporomandibular disorders: a clinical practice guideline. BMJ. 383.
View at Publisher | View at Google Scholar - Saboowala, H., (2020). “Bruxism” (Teeth Grinding or Clenching): Causes, Symptoms, Diagnosis & Management. An Overview.
View at Publisher | View at Google Scholar - Romanowski, M.W., et al., (2020). Manual therapy (postisometric relaxation and joint mobilization) in knee pain and function experienced by patients with rheumatoid arthritis: a randomized clinical pilot study. Evidence‐Based Complementary and Alternative Medicine. 2020(1): p. 1452579.
View at Publisher | View at Google Scholar - Ohrbach, R. and S. Sharma, (2021). Behavioral therapy for temporomandibular disorders. Frontiers of Oral and Maxillofacial Medicine. 3: p. 37-37.
View at Publisher | View at Google Scholar - Ifeadi, C.N. and F. Agodi, (2024). MISUSE AND ABUSE OF PRESCRIPTION DRUGS: AN OVERVIEW. Disseminating Scholarly Research Across the Globe: p. 27.
View at Publisher | View at Google Scholar - Serritella, E., et al., (2021). Comparison of the Effectiveness of Three Different Acupuncture Methods for TMD‐Related Pain: A Randomized Clinical Study. Evidence‐Based Complementary and Alternative Medicine. 2021(1): p. 1286570.
View at Publisher | View at Google Scholar - Mauro, G., et al., (2024). Temporomandibular Disorders Management—What’s New? A Scoping Review. Dentistry Journal. 12(6): p. 157.
View at Publisher | View at Google Scholar - Mena, M., et al., (2020). Efficacy of topical interventions for temporomandibular disorders compared to placebo or control therapy: a systematic review with meta-analysis. Journal of dental anesthesia and pain medicine. 20(6): p. 337.
View at Publisher | View at Google Scholar - Fernández-de-Las-Peñas, C. and H. von Piekartz, (2020). Clinical reasoning for the examination and physical therapy treatment of temporomandibular disorders (TMD): a narrative literature review. Journal of Clinical Medicine. 9(11): p. 3686.
View at Publisher | View at Google Scholar - Massé, L., (2022). Comparison of the effectiveness between peri/intra-articular injections and conventional treatments in patients with temporomandibular disorders’ symptoms: A systematic review.
View at Publisher | View at Google Scholar - Cohen, S.P., et al., (2020). Consensus practice guidelines on interventions for lumbar facet joint pain from a multispecialty, international working group. Regional Anesthesia & Pain Medicine. 45(6): p. 424-467.
View at Publisher | View at Google Scholar
