

Case Report | DOI: https://doi.org/10.31579/2835-8147/044
Right-Sided Hand Assisted Laparoscopic Living DONOR Nephrectomy in 48- Year-Old Female with Multiple Scars: Successful First Experience
- Khin Phyu Pyar 1*
- Saw Yan Naing 2
- Yan Naung 3
- Aung Kyaw Tun 4
- Aung Thaw Hein 4
- Yan Naung Win 4
- Aung Khant 4
- Kyaw Thura 5
- Yu Aye Latt 6
- Chann Myei 7
- Myo Min Thant 8
- San Lin 9
- Hlawn Moe 3
- Soe Min Aung 10
- Nyan Lin Maung 10
- Tin Mar Yee 11
1 Professor and Head/Senior Consultant Physician and Nephrologist, Department of Medicine/Nephrology, Defence Services Medical Academy/ No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
2 Professor and Head/Senior Consultant Uro-surgeon, Department of Urology, Defence Services Medical Academy/ No. (2) Base Military Hospital (700-Bedded), Aung Ban, Myanmar.
3 Senior Consultant Vascular surgeon, Department of Cardiovascular surgery, Defence Services Medical Academy, Yangon, Myanmar.
4 Senior Consultant Uro-surgeon, Department of Urology, No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
5 Senior Consultant Vascular surgeon, Department of Cardiovascular surgery, No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
6 Professor and Head/ Senior Consultant Anesthetist, Department of Anesthesiology/Intensive care, Defence Services Medical Academy/ No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
7 Senior Consultant Anesthetist, Department of Anesthesiology/Intensive care, No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
8 Consultant Physician/Nephrology Fellow, No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
9 Senior Consultant Nephrologist, Department of Nephrology, No. (2) Base Military Hospital (700-Bedded), Aung Ban, Myanmar.
10 Senior Consultant Physician, Department of Medicine, No. (2) Base Military Hospital (700-Bedded), Aung Ban, Myanmar.
11 Senior Consultant Surgeon, Department of Surgery, No. (2) Base Military Hospital (700-Bedded), Aung Ban, Myanmar.
*Corresponding Author: Khin Phyu Pyar, Professor and Head/Senior Consultant Physician and Nephrologist, Department of Medicine/Nephrology, Defence Services Medical Academy/ No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
Citation: Khin Phyu Pyar, Saw Yan Naing, Yan Naung, Aung Kyaw Tun, Aung Thaw Hein, et al., (2024), Right-Sided Hand Assisted Laparoscopic Living DONOR Nephrectomy in 48- Year-Old Female with Multiple Scars: Successful First Experience. J. Clinics in Nursing 3(1); DOI:10.31579/2835-8147/044
Copyright: © 2024, Khin Phyu Pyar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 December 2023 | Accepted: 20 December 2023 | Published: 03 January 2024
Keywords: laparoscopic donor nephrectomy; right kidney; short left renal artery
Abstract
Laparoscopic living donor nephrectomy (LLDN) has been practicing as a surgical standard for living kidney donation. LLDN to left kidney has been done in Myanmar for one decade. This is first experience of LLDN to right kidney. The donor was a 48-year-old female with multiple surgical procedure over 10 years; two previous elective cesarean sections, an appendectomy, a total abdominal hysterectomy, and bilateral salpingo-oophorectomy. Because the length of left renal artery was shorter, less than one-third of right renal artery, right LLDN was performed. Postoperative pain was minimal. Grafted kidney was functioning well. We reported our experience of LLDN to right kidney.
Introduction
Among the various options for patients with end stage renal disease, kidney transplantation is the treatment of choice for a suitable patient. The kidney for transplantation is retrieved from either a cadaver or a live donor.
In Myanmar, kidney transplantation has been done since 1995. Living kidney transplant has been done over 30 years in four military transplant centers. They are situated in Mingaladon (Yangon), Nay Pyi Taw, Pyin Oo Lwin and Aung Ban. Living donor nephrectomy (LDN) has been done 456 transplant pairs; and, diseased/cadaveric kidney donor transplant program has not developed yet. Laparoscopic living donor nephrectomy (LLDN) has many advantages over traditional open donor nephrectomy (TODN): less postoperative pain, shorter convalescence, and better cosmetic outcome of the donor nephrectomy. However, the technique of LLDN has undergone evolution at different transplant centers. Being low resource setting, the evolution has been growing slowly to get better skills on LLDN. Many modifications like hand assisted LLDN (HALLDN) have been tried to improve donor safety and recipient outcome. In Myanmar, among 456 successful kidney transplant, 54 pairs had LLDN on left; only two pairs underwent right LLDN. Of 4 transplant centers in Myanmar, right LLDN has been successfully done in Aung Ban.
Case presentation
A 48-year-old woman presented for evaluation to donate her kidney to husband, who had end-stage renal disease secondary to hypertension. The woman had no significant renal or urologic issues. However, she had multiple scars in abdomen; two previous cesarean sections; an appendectomy in 2013; a total abdominal hysterectomy, and bilateral salpingo-oophorectomy in 2016 for dysfunctional uterine hemorrhage. She had no allergies and was not taking any medications. She works as a full-time homemaker. Physical examination was unremarkable including psychological screening. Laboratory studies were normal; complete blood count, liver function study, serum electrolytes, connective tissue disease screening, and tumor markers. Her blood urea was 23.8 mg/dL; serum creatinine, 0.8 mg/dL; and creatinine clearance, 89 mL/min. A hepatitis profile and viral antibody screening were negative. She was ABO compatible with her husband, blood group was B Rh (+). The CDC cross-match result was negative. Furthermore, Class 2 DSA was detected (DRB401:03 and DRB401:01, MFI 3674 and 2938, respectively). Preoperative three-dimensional computerized tomography (CT) reconstruction revealed a single right renal artery measuring 4.8 cm in length, originating from the aorta to the first segment. Similarly, a single left renal artery, measuring 1.3 cm, originated from the aorta to the first segment. Notably, early branching of the left renal artery was observed, and a hemangioma at the L3 lumbar vertebra was also identified. Both kidneys were observed to be of equal size. DTPA renal scan for split renal function was unavailable. Therefore, she underwent a right laparoscopic living donor nephrectomy (LLDN) on October 27, 2023. The procedure involved the use of four tiny incisions (ranging from 0.5 to 1.2 cm) to allow the insertion of the laparoscope. The kidney was extracted through a right flank incision. Warm ischemic time was 7 minutes and 4 seconds; estimated blood loss was 200 cc. The kidney weight was 100 grams. There were no intraoperative complications, and the combined procedure took 3 hours, 1 minute. The donor was discharged on the third postoperative day. Pain management during hospitalization required only 10 mg of morphine sulfate combined with only two days of acetaminophen infusion (500 mg three times per day) and nine plain acetaminophen tablets. The donor was able to resume her daily activities just seven days postoperatively. She has had no long-term complications after one month follow-up; normal serum creatinine; no abdominal wound problem. The transplanted kidney began functioning immediately after grafting. The recipient received treatment consisting of IV thymogam as an induction immunosuppressive agent and tacrolimus, mycophenolate mofetil, and prednisolone as a maintenance immunosuppressive regimen. Notably, by the fourth day post-transplant, the recipient's serum creatinine had decreased from 9.5 mg/dL to 1.4 mg/dL. Subsequently, he has not experienced any episodes of rejection till one month.
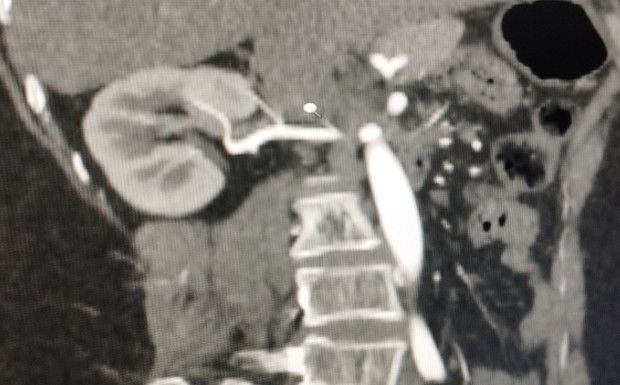
Figure 2: CT renal angiogram showing right kidney and renal artery

Figure 3: CT renal angiogram showing left kidney and short renal artery

Figure (4&5): CT renal angiogram anterior and posterior view

Figure 7: Operative view
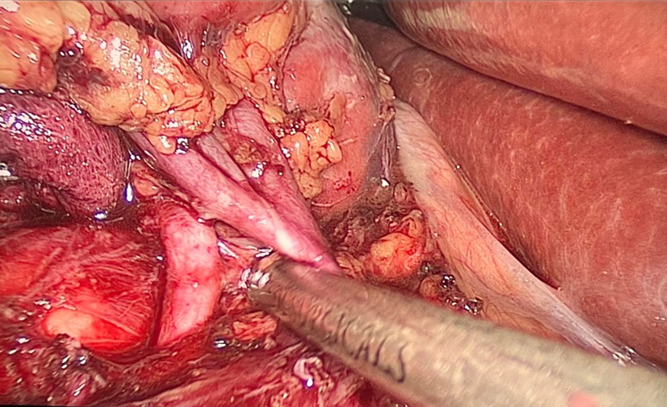
Figure 8: Right renal artery and renal vein
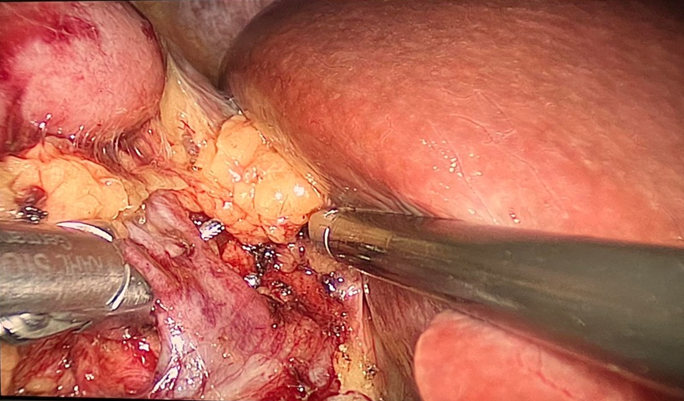
Figure 9: Right renal vein
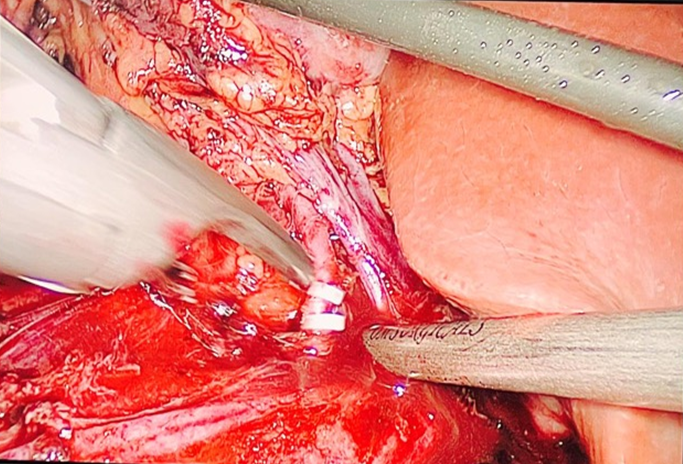
Figure 10: Right renal artery clump
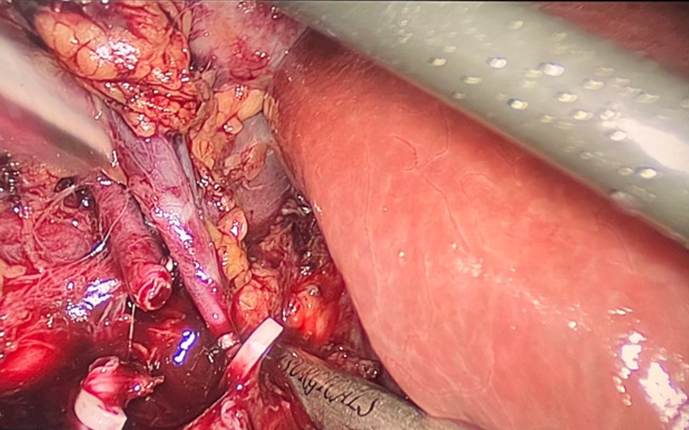
Figure 11: Right renal vein clump
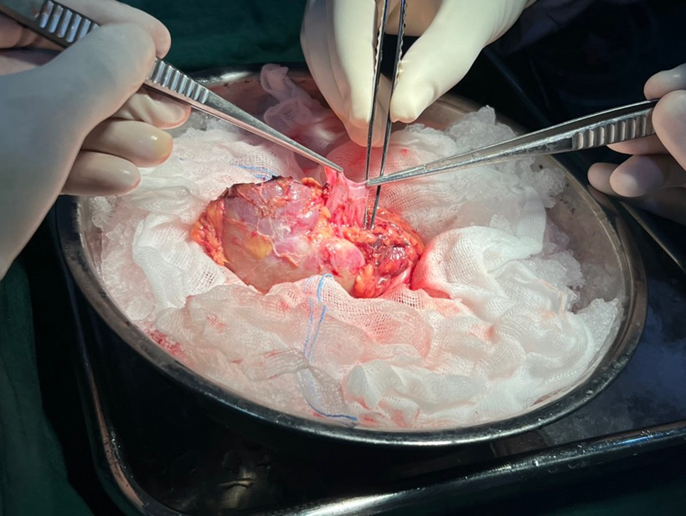
Figure 12: Kidney graft showing renal vein length
Discussion
Of 456 renal transplant pairs done in Myanmar, traditional open donor nephrectomy TODN) was carried out in 400 pairs; laparoscopic living donor nephrectomy LLDN) was performed in 56 pairs. Among 56 pairs with LLDN, left LLDN was made in 54 pairs; and right LLDN was done in 2 pairs. First right LLDN done in 2022 was converted to TODN. This case report had hand assisted right LLDN. This is one reason for doing case report to congratulate surgical transplant team for their success on right LLDN in Myanmar. LLDN has acquired an important role in the era of minimally invasive surgery; it has shown less morbidity than the open approach TODN). It has less pain; therefore, analgesia requirements are less. Moreover, it allows a quicker recovery; hence, the donor has an earlier return to normal activity. The advantages of LLDN was reported as successful surgery in all cases with a short surgical time, low morbidity, and 0% mortality [4,7,10]. However, the technique of LLDN has undergone evolution at different transplant centers. Here, being a low resource setting, it took time to get skills on LLDN. In fact, doing renal transplant has several challenges particularly in low-income country: man, materials and money. Donor factors like anomalies of vasculature, ureter and nearby structure, significant difference in split renal function, are also important in success of LLDN. To improve the skills on LLDN, practice and experience are the main determinants. Highly qualified and well-trained surgeons are allowed to perform LLDN within a very well-equipped environment and with experienced surgical staff. A living donor program should undertake at least 30 cases per year to maintain adequate experienced surgical staff. A living donor program should undertake at least 30 cases per year to maintain adequate experience and offer less complication rate Maroun Moukarzel et al., 2018). To improve donor safety and recipient outcome, the surgical team including anesthetic team have to try their best during surgery. Many modifications like hand assisted LLDN are tried to improve donor safety and recipient outcome. Of 456 pairs, TODN was done in 400 pairs; right LLDN was performed successfully in this case. The warm ischemic time was 7 minutes and 4 seconds in this case; it was longer than other reports. The average warm ischemia time was reported as 4.73 min in LLDN [7]. The skills will improve with experience in future. Regarding the choice of kidney, the right kidney is not commonly selected for donor nephrectomy compared with the left kidney. Generally, most left donor nephrectomies are performed by laparoscopic approach, whereas open donor nephrectomies are preferred on the right side; though each center has varying experiences. According to initial experience from Poland, they recommended using the left kidney in clinical practice because the longer renal vein of the left kidney could decrease operative difficulty [14]. They also pointed out that right and left LLDN were similar in the effect of surgery and postoperative graft function. When there were no differences in bilateral renal function, surgeons could transplant either the right or left kidney. Although left kidney is usually chosen for donor nephrectomy, right kidney is considered if left kidney has some problems: multiple vessels, anomalous vasculature and obesity, short renal artery, multiple renal arteries, short renal vein, etc. The main reason is that shorter length of the right renal vein poses technical challenges for the transplant surgeon in implanting the kidney into the recipient. Therefore, doing left LLDN is relatively easier and less stressful than right LLDN. Moreover, Right-sided operation is technically more difficult and much more challenging because retraction of the liver is usually required and because the shorter right renal vein increases the risk of allograft thrombosis. However, one advantage of right LLDN is that it may shorten the time of surgery because of lack of draining venous tributaries. And, the ratio of left LLDN to right LLDN was reported as 10:1 in several countries. Successful right LLDN was mentioned as safe as left LLDN in experienced hands. Right LLDN could be effectively deal with various vascular and ureteral anomalies without compromising early graft function [15].
In Myanmar, kidney transplant has made 30 years history in military transplant centers. There are 4 transplant centers in Myanmar under the Ministry of Defense; Mingaladon Yangon, Nay Pyi Taw, Pyin Oo Lwin and Aung Ban. Only two pairs underwent right LLDN. First right LLDN was converted to laparotomy in 2022. Right LLDN has been successfully done in Aung Ban; the center has been functioning for 2 years. Here, the success on this case enhances the confidence of our surgical team in doing right LLDN. And, our transplant team congratulates surgical colleagues and we are proud of them. This is another reason for writing case report.
Therefore, this first successful right LLDN supported the findings that ‘right sided kidneys can be harvested safely laparoscopically with excellent donor outcome as well as comparable graft function with left sided LLDN and open group TODN’ [2,9].
Hand-assisted laparoscopic nephrectomy HALLDN) encompasses the benefits of the minimally invasive approach reducing the operative time and learning curve in comparison with the totally laparoscopic procedure. This case also confirmed the fact that right-sided HALLDN is safe and technically feasible in a donor, showing favorable graft outcomes [1,3,11].
Conclusion
Hand-assisted laparoscopic living donor nephrectomy HALLDN) is safe as traditional open donor nephrectomy TODN). If indicated, right-sided LLDN should be done. Right-sided HALLDN is safe and it has favorable graft outcomes like left-sided LLDN.
Acknowledgements
The authors would like to thank the family for giving consent to this article. Also, to all doctors and nursing team for making great efforts in caring him. The authors acknowledged the following team: Dr Tin Tin San for laboratory support, Dr Thet Tin Win for radiological support, Professor Kyaw Zay Ya and Professor Ko Ko Lwin for administrative support.
Declaration of conflict of interest
The authors declared no potential conflicts of interests with respect to authorship and publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting cases.
Funding
The authors received no financial support for publication of this article.
Informed consent
The informed consent for publication in this article was obtained from wife of patient.
References
- Broudeur, L., Karam, G., Chelghaf, I., De Vergie, S., Rigaud, J., et.al., (2020). Feasibility and safety of laparoscopic living donor nephrectomy in case of right kidney and multiple-renal artery kidney: A systematic review of the literature. World Journal of Urology, 38(4), 919–927.
View at Publisher | View at Google Scholar - Broudeur L., Karam G., Rana Magar R., Glemain P., Loubersac T., et. al., (2020). Right Kidney Mini-Invasive Living Donor Nephrectomy: A Safe and Efficient Alternative. Urologia Internationalis, 104(11–12), 859–864.
View at Publisher | View at Google Scholar - Chung M.-S., Kim S. J., Cho H. J., Ha U.-S., Hong S.-H., et. al., (2010). Hand-Assisted Laparoscopic Right Donor Nephrectomy: Safety and Feasibility. Korean J Urol, 51(1), 34–39.
View at Publisher | View at Google Scholar - Gupta N., Raina P., & Kumar, A. (2005). Laparoscopic donor nephrectomy. Journal of Minimal Access Surgery, 1(4), 155–164.
View at Publisher | View at Google Scholar - Kumar A., Chaturvedi S., Gulia A., Maheshwari R., Dassi, V., et. al., (2018). Laparoscopic Live Donor Nephrectomy: Comparison of Outcomes Right Versus Left. Transplantation Proceedings, 50(8), 2327–2332.
View at Publisher | View at Google Scholar - Laparoscopic living-donor nephrectomy: Shorter operating time for right kidney. (2008). Nature Clinical Practice Nephrology, 4(5), 242–243.
View at Publisher | View at Google Scholar - Małkiewicz, B., Kamińska, D., Kobylański, M., Łątkowska, M., Handzlik, W., et. al., (2022). Laparoscopic Living Donor Nephrectomy-Single-Center Initial Experience. Uro, 2(3), 191–198.
View at Publisher | View at Google Scholar - Maroun Moukarzel, Charbel Chalouhy, Nabil Harake, & Freda Richa. (2018). Laparoscopic Live Donor Nephrectomy: Techniques and Results. In Miana Gabriela Pop (Ed.), Basic Principles and Practice in Surgery (p. Ch. 3). IntechOpen.
View at Publisher | View at Google Scholar - Mohsin, R., Shahzad, A., Sultan, G., Aziz, T., & Hashmi, A. (2018). Right Sided Laparoscopic Donor Nephrectomy—Dream Comes True. Transplantation, 102.
View at Publisher | View at Google Scholar - Musquera Felip M., Peri Cusí L., & Alcaraz Asensio, A. (2010). Surgical aspects of living-donor kidney transplantation. Nefrología (English Edition), 30, 71–79.
View at Publisher | View at Google Scholar - Romero, J. A., Meza, J., Marmolejo, A., Bathory, R., Ruiz-Funes, A. P., et. al., (2022). Hand-assisted laparoscopic nephrectomy for a kidney transplant: Surgical technique—Tips and tricks—How we do it? 2022, 7.
View at Publisher | View at Google Scholar - Saad, S., Paul, A., Treckmann, J., Nagelschmidt, M., Heiss, M., et. al., (2008). Laparoscopic live donor nephrectomy for right kidneys: Experience in a German community hospital. Surgical Endoscopy, 22(3), 674–678.
View at Publisher | View at Google Scholar - Serni, S., Pecoraro, A., Sessa, F., Gemma, L., Greco, I., et. al., (2006). Laparoscopic Right Donor Nephrectomy: Is There a Right Way? Journal of Endourology / Endourological Society, 20, 309–311.
View at Publisher | View at Google Scholar - Wang K., Zhang P., Xu X., & Fan M. (2015). Right Versus Left Laparoscopic Living-Donor Nephrectomy: A Meta-Analysis. Exp Clin Transplant, 13(3), 214–226. PubMed.
View at Publisher | View at Google Scholar - Zaytoun O., Elsawy M., Ateba K., Khalifa A., Hamdy A., et. al., (2021). Laparoscopic donor nephrectomy: Technique and outcome, a single-center experience. African Journal of Urology, 27(1), 151.
View at Publisher | View at Google Scholar
