

Research Article | DOI: https://doi.org/10.31579/2835-8325/002
Research Article: Preeclampsia Patients in Owerri Metropolis: Studies of C-Reactive Protein and Uric Acid Status
- Amaobi Rosecollet Ngozi
- Nnodim Johnkennedy *
Department of Medical Laboratory Science, Imo State University, Owerri Nigeria.
*Corresponding Author: Nnodim Johnkennedy. Department of Medical Laboratory Science, Imo State University, Owerri Nigeria.
Citation: Amaobi Rosecollet Ngozia and Nnodim Johnkennedy, (2022). Preeclampsia Patients in Owerri Metropolis: Studies of C-Reactive Protein and Uric Acid Status. Clinical Research and Clinical Reports.1(1); DOI:10.31579/2835-8325/002
Copyright: © 2022 Nnodim Johnkennedy, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 September 2022 | Accepted: 24 September 2022 | Published: 01 October 2022
Keywords: preeclampsia; c-reactive protein; uric acid; studies
Abstract
The goal of the study was to measure and assess the c-reactive protein and uric acid levels in preeclampsia patients. In the study, serum samples from 30 participants—15 preeclampsia patients and 15 healthy pregnant women—were tested for levels of c-reactive protein and uric acid. The level of c-reactive protein was determined using an enzymatic technique. The findings demonstrated that, at p0.05, the c-reactive protein concentration was substantially higher in preeclampsia patients (4.770.9 mg/dl) than in healthy pregnant women (1.30.39 mg/dl). Additionally, at p 0.05, preeclampsia patients had significantly higher uric acid concentrations (8.973.35 mg/dl) than healthy pregnant women (3.60.5 mg/dl). These results suggest that preeclampsia is associated with elevated levels of c-reactive protein and uric acid. Consequently, it likely act as a biochemical marker for preeclampsia.
Introduction
Preeclampsia is a medical disease in which pregnancy-related hypertension (blood pressure more than or equal to 110/90 mmHg) develops in conjunction with the presence of protein in the urine (proteinuria). Preeclampsia is a potentially catastrophic condition that puts both the mother and the fetus' lives in danger (Sibai et al, 2005).
Preeclampsia is a disorder unique to human pregnancy that manifests as substantial proteinuria and hypertension in a previously healthy woman on or after the 20th week of pregnancy. It affects 2-8% of pregnancies (Ghumiyyah and Sibai, 2012)
Early detection, careful monitoring, and treatment of preeclampsia by appropriate prenatal care are essential in preventing mortality related to preeclampsia. Intrauterine fetal growth retardation, low birth weight, fetal death, and neonatal death due to complications of preterm delivery are common parietal outcomes associated with preeclampsia. (Hoque et al. 2008)
Preeclampsia is linked to oedema, proteinuria, decreased renal function, maternal mortality, placental insufficiency, and intrauterine fetal growth retardation, according to Crook (2006). It is unclear how these risk factors and preeclampsia are related. The variations in risk between racial and ethnic groups point to a significant genetic component in the etiology of preeclampsia.
The acute phase protein known as C-reactive protein (CRP) is made by the liver and is present in the blood. Its level increases in response to a variety of inflammatory circumstances in the body since it is an acute phase protein (Pepys and Hirschfield, 2003). Women with preeclampsia have changed levels of inflammatory response mediators, such as C-reactive protein (Teran et al, 2001).
The last byproduct of purine metabolism is uric acid. Purines, such as adenosine guanine, are produced when nucleic acids break down (Ochei and kolhaktar,2008). The body's elevated uric acid concentration is known as hyperuricemia. In preeclampsia-related pregnancies, hyperuricemia is a frequent finding. According to Power et al. (2006), the clinical symptoms used to identify preeclampsia in women frequently come before proteinuria and hypertension. Uric acid in preeclampsia may have numerous causes, including accelerated tissue breakdown, acidosis, and increased activity of the enzyme xanthine oxidase/dehydrogenase (Johnson et al, 2003). Either a reduced or increased uric acid production has been implicated as the cause of hyperuricemia in preeclampsia. While altered tubular function and decreased uric acid clearance have both been observed, Fay (1990) postulated that the overproduction of uric acid may be due to increased purine breakdown in the placenta (Jeyabalan and Conrad,2007; Hill,1987; Fay,1990). Preeclampsia-related hyperuricemia is typically seen as a sign of renal impairment rather than a risk factor for the disease's progression.
Preeclampsia is a serious pregnancy condition that increases the risk of mortality and morbidity for both the mother and the fetus. Preeclampsia requires more study in order to enhance diagnosis, treatment, and prevention. Preeclampsia research has not been extensively conducted in Owerri, so the goal of this study is to assess the levels of C-reactive protein and uric acid in preeclampsia patients in Owerri, with the hope that the pattern of results will aid in preeclampsia clinical decision-making generally.
Materials And Methods
Study Area/Setting
This study was carried out in Imo State University situated in Owerri metropolis; the capital city of Imo State located in the tropical rainforest of South-Eastern part of Nigeria. The major ethnic group is Igbo, with a few people from other tribe resident therein. The inhabitant are predominantly Christians with few muslims and pagans. Owerri is located within the South-East geopolitical zone of Nigeria and is situated on latitude 5o 271-5o 311N and longitude 6o 55-7o 031 E.
Study Population
The study population consisted of 30 subjects attending antenatal clinic at the Federal Medical Centre Owerri, within the age of 25-40years. The 30 subjects were divided into two groups:
Group 1 are 15 pregnant women with preeclampsia
Group 2 (control group) are 15 healthy pregnant women with normal blood pressure.
Selection Criteria
The subjects selected for the study were based on the following criteria: Pregnant women with systolic blood pressure of 140mmHg or (Bp≥140/90mmHg) developed during pregnancy were selected for preeclampsia group (group 1).
Healthy pregnant women with blood pressure were selected for group 2 (control group).
Preeclampsia women and healthy pregnant women whose informed consent were obtained.
Exclusive Criteria
The following subjects were excluded from the sudy:
Preeclampsia patients who had Bp≥140mmHg before being pregnant. Preeclampsia patients with a history of diabetes, renal disease other cardiovascular illness and symptomatic diseases.
Preeclampsia patients with known systemic disease, as mentioned above. Preeclampsia patients whose informed consent could not be obtained because they were sceptical about the research work.
All these were investigated during routine interviews and checked of medical records.
Sample Collection
In all subjects, about 5ml of venous blood were collected by venepunture technique from antecubital vein with 5ml disposable syringe. The whole blood samples were dispensed into centrifuge test tubes without anticoagulants and were immediately labelled for proper identification. The centrifuge test tubes containing the whole blood sample to clot. After that, the centrifuge test tubes were loaded in the centrifuge
and were spun at 10,000rpm for 10 minutes using wisperfuge model 1384 centrifuge (Samson Holland). The supernatant serum was separated from the sedimented clotted blood by using pasture pipette to collect the serum and transferred it into a sterile serum sample tube, which were again labelled for proper identification. The serum samples obtained were used for C-reactive protein estimation, and uric acid estimation.
Laboratory Methods and Procedure
The reagents used in the research work were of analytical grade. All the materials and reagents used were listed in the appendix 1.
(a) Estimation of serum c-reactive protein(crp) by latex agglutination slide test using c-reactive protein reagent kit (agappe disnostics switzerland gmbh)
(b) Estimated of serum uric acid by enzymatic spectrophotometric method using uric acid kit (biosystem reagents).
Statistical Analysis
All the values were expressed as mean ± standard deviation. The statistical analysis was carried out using student’s t-test to determine whether the difference between two groups is statistically significant or not when compared. Values with level of significance (p<0>
Result
Table 1: Results showing the mean ± standard deviation (X±SD) of the age, systolic blood pressure and the diastolic blood pressure of preeclampsia women (the test group) and the healthy women (the control group).
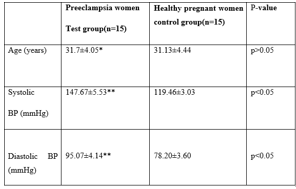
Table 1: Shows that the value of the maternal age of preeclampsia women 31.47 ±4.05years was not significantly different (p>0.05) when compared with the value of the maternal age of healthy pregnant women 31.13 ± 4.44years. This could be suggestive that age has no effect on preeclampsia.
As was expected, the values of the systolic blood pressure and diastolic blood pressure of preeclampsia women 147.67 ± 5.53mmHg and 95.07 ± 4.14mmHg respectively where significantly higher (p<0>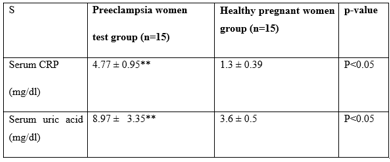
Key:
** Statistically different when compared with the control group (p<0>
Table 2: Shows that the value of serum CRP of preeclampsia women 4.77 ± 0.95mg/dl was significantly different (p<0>
Also, the same table shows that the value of serum uric acid of preeclampsia women 8.97 ±3.35mg/dl was significantly different (p<0>
Discussion
The purpose of this study was to compare the serum levels of c-reactive protein and uric acid in preeclampsia patients with those of healthy controls. It was discovered that preeclampsia patients' serum levels of c-reactive protein were higher than those of age-matched healthy women. Despite much investigation, the physiopathology of preeclampsia remains unclear (Myatt and Miodovink,1990). Preeclampsia's development has been linked to a number of etiologies. Preeclampsia's potential pathogenic pathways have been hypothesized to involve changes in endothelial function and vasoactive substances (Robert and Redman, 1993). It is believed that endothelial dysfunction and inflammation play a significant part in the pathophysiologic mechanism of preeclampsia (Kharb et al, 1998). A sensitive indicator of tissue damage and the inflammatory response that characterizes preeclampsia is C-reactive protein (Redman et al, 1999). Membranes and nuclear antigens are cleared by the scavenger action of C-reactive (Du clos, 1996). Some academics have already looked into the link between preeclampsia and c-reactive protein. In those earlier investigations, preeclampsia was associated with greater C-reactive protein concentrations (Teran et al, 2001; Okerengwo et al, 1990; Ghazavi et al, 2008). The current findings are consistent with the theory that systemic inflammation plays a role in the etiology of preeclampsia. According to this study, preeclampsia patients' serum uric acid levels were considerably greater than those of pregnant women who were healthy. The primary byproduct of purine metabolism is uric acid. The kidneys filter, reabsorb, and secrete it. Either a decrease in uric acid excretion or an increase in uric acid synthesis has been identified as the cause of hyperuricemia in preeclampsia. Preeclampsia may also result in increased uric acid generation from maternal, fetal, or placental tissue due to increased tissue breakdown (increasing substrate availability) and/or increased xanthine oxidase activity. While an increased breakdown of purines in the placenta as a potential explanation for the overproduction of uric acid in preeclampsia was proposed by Fay in 1990, hyperuricemia has historically been attributed to renal clearance as reflected by altered function (Jeyabalon and Conrad, 2007; Hill 1987; Fay). The relationship between hyperuricemia and preeclampsia has been the subject of numerous studies by some researchers (Redman et al, 1976; Ancien et al, 1990). Additionally, in this study (Frank et al., 1991; Sanchezramos et al., 1991), the prevalence of preeclampsia was evidently significantly higher than that of healthy pregnant women.
Conclusion
According to the study's findings, preeclampsia patients have higher levels of serum uric acid and C-reactive protein. Therefore, measuring serum uric and C-reactive will aid in the identification and treatment of preeclampsia patients
References
- Ancient, p., Lioret, G., And Lioret, M., (1990). Perintal Morbidity and Mortality in pregnancy hypertensive disorders: prognostic value of the clinical and laboratory finings. International Journal of Gynecology and Obstetrician; 3(3): 229-235.
View at Publisher | View at Google Scholar - Choi, H.K., (2004). Purine-rich foods, dietary and protein intake and the risk of gout in Men. N. Engl.J.Med.350(11): 1093-1103.
View at Publisher | View at Google Scholar - Crook, M.A., (2006). Clinic Chemistry and metabolic.7th Edition Edward Arnold (unblisher) Ltd. Horder Arnold. 10:158-159.
View at Publisher | View at Google Scholar - Du clos, T.W., (1996). The interaction of C-reactive protein and Serum Amyloid P component with nuclear antigens. Molecular Biology Reproduction, 23(3-4): 253-260.
View at Publisher | View at Google Scholar - Fay, R.A., (1990). Uric acid in pregnancy and preeclampsia: AN Alternative hypothesis Aust. N.Z.J. Obstete, Gyneco. 30:141-142.
View at Publisher | View at Google Scholar - Frankel, Y., Barkai, G., Mashiach, S., Dolev, E., Zimlichman, R., And Weiss M., (1991). Hypocalciria of preeclampsia is independent of parathyroid hormone level. Obstetrics and Gynecology; 77(5): 68-691.
View at Publisher | View at Google Scholar - Ghumiyyah. L and Sibai.B (2012) Maternal mortality from preeclampsia/eclampsia□, seminar in pernatology,56-59.
View at Publisher | View at Google Scholar - Hill, L.M., (1987) Metabolism of uric acid in normal and toxemic pregnancy. Mayo Clin. Proc. 53:743-751.
View at Publisher | View at Google Scholar - Hoque, M.M., Bulbul, T., Mahal M., Islam, N.A., Ferdauss, M., (2008). Serum homocystein in preeclampsia and enclampsia babgaltesh Med. Res. Counc. Bull 34:16-20
View at Publisher | View at Google Scholar - Jeyabalan, A.,And Conrad, K.P., (2007). Renal function during normal pregnancy and preeclamsia. Front Bioscience. 1:2425-2437.
View at Publisher | View at Google Scholar - Jeyabalan, A., Powers, R.W., Durica, A.r., Harger, G.F., Roberts J.M., Wess, R.B, (2008). “Cigarette smoke exposure and angiogenic factors in pregnancy and preeclampsia” Am j. hypertens. 21(8): 94947.
View at Publisher | View at Google Scholar - Kharb, S., Gulati, N., Sing, G.P., (1998). Lipid Preoxidation and Vitamin E. Levels in preeclampsia Gynecel. Obstet. Invest. 46:238-240.
View at Publisher | View at Google Scholar - Myatt and Miodovink, (1990). Prediction of preeclampsia Semin. Perinatol. 23:45-57.
View at Publisher | View at Google Scholar - Ochie, J., And Kolhatkar, A., (2008). Medical Laboratory Science Theory and practice 7th edition. Mc. Graw-Hill. 4118: -119.
View at Publisher | View at Google Scholar - Okerengwo, A.A., Williams, A.I., and Ibeziako P.A., (1990), Immunological studies on preeclampsia in Nigeria Women. International Journal of Gynecology and Obstestrics; 33(2)-121-125.
View at Publisher | View at Google Scholar - Pepys, M.B., And Hirschfield, G.M., (2003). “C-reactive Protein: A Critical update”. Clin Invest 111(12): 1805- 1812.
View at Publisher | View at Google Scholar - Powers, R.W., Bodnar, L.M.,Ness, R.B., Cooper, K.M., Gallaher M.J., Frank, M.P., Daftaly, A.R., Roberts, J.M., (2006). Uric acid Concentrations in early pregnancy among preeclamptic women. With getational hyporuicemia at delivery. Am. J. Obstet. Gynecol. 194:160.
View at Publisher | View at Google Scholar - Redman, C.W., And Sergetn, I.L, (2005). Latest advances in Understanding preeclampsia. Science 308 (5728): 1592-1594.
View at Publisher | View at Google Scholar - Redman, C.W., Beilin, L.G., Bonnar, J., And Wilknson, R.H., (1976). Plasma Urate measurements in predicting fetal death in Hypertensive pregnancy. Lancet, 1(7974): 1370-1373.
View at Publisher | View at Google Scholar - Redman, C.W.,Sacks,G.P.,And Sargent,I.L.,(1999). Preeclampsia an Excessive Maternal Inflammatory response to pregnancy Am. J. Obstet. And Gynecol. 180(2): 499-506.
View at Publisher | View at Google Scholar - Roberts, J.M., And redman, C.w., (1993). Preeclampsia: more than Pregnancy-induced hypertension. Lancet, 341:1447-1451.
View at Publisher | View at Google Scholar - Roberts, J.M., Lain, K.Y., Ness, R.B., (2005). Uric acid is as Important As proteinuaria Kin Identifying fetal risk in women with gestational hypertension. Hypertension. 46:1263-1264.
View at Publisher | View at Google Scholar - Sanchez-Ramos, L., Sandroni, S., Andres F.J., And Kaunitz, A.M., (1991). Calcium excretion in pregnancy. Obstet. And Gyneco., 77(4): 510-513.
View at Publisher | View at Google Scholar - Sibai, B.M., (1999), The HELP syndrome (hemolysis, elevated liver Enzymes, and low platelet). Am. J. Obstet Gynecol. 162(2): 311-316.
View at Publisher | View at Google Scholar - Sibai, B.m., and Gozalez-Ruiz A., (1986). Severe preeclampsia Eclampsia in young primigravid women: subsequent pregnancy Outcome and remove prognosis. Am Journal Obstet. Gynecol. 155:785-794.
View at Publisher | View at Google Scholar - Sibai, B.M., Dekker, G., Kupfeminc, M., (2005). Preeclamsia. Lancet. 365:785-794.
View at Publisher | View at Google Scholar - Teran, E., Escudero, C., Moya, W., Flores, M., Vallance P., And Lopez Javamillo, P., (2001). Elevated C-reactive protein and pro-Inflammatory cytokines in Andean women with preeclampsia. Int. J. Gynecol. Obstet 75(3): 243-249.
View at Publisher | View at Google Scholar
