

Research Article | DOI: https://doi.org/10.31579/2835-8147/052
Related of the age, body mass index and Anti-Müllerian hormone with the other hormones in polycystic ovarian syndrome patients
*Corresponding Author: Musafer H. Al-Ardi, General directorate for education in Al-Qadisiyah- Ministry of education- Iraq.
Citation: Musafer H. Al-Ardi (2023), Related of the age, body mass index and Anti-Müllerian hormone with the other hormones in polycystic ovarian syndrome patients, Clinics in Nursing, 3(2) DOI:10.31579/2835-8147/052
Copyright: © 2024, Musafer H. Al-Ardi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 January 2024 | Accepted: 20 February 2024 | Published: 02 March 2024
Keywords: polycystic ovarian syndrome; amh; bmi; reproduction hormones; women health
Abstract
Hormonal disorders that come with ageing and affect hormone levels have a significant impact on polycystic ovary syndrome (PCOS), which is linked to infertility. However, it is clear that PCOS and obesity have a two-way overlap and are mutually affecting. Here, we're looking for a correlation between various hormone concentrations with weight and age in PCOS-affected women. The concentration of hormones (AMH, E2, HCG E, Inhibin B, Prolactin, LH, FSH, TSH) was measured by the enzyme-linked fluorescence assay technique in the blood serum of 62 POCS patients (31.42 ± 5.93) years and BMI (27.03± 5.03). Here we notice Significantly BMI-related variables was Negative (decreasing due to BMI increase) with E2, insignificant negative association with HCG E2, Inhibin B, TSH, and FSH, insignificant positive association with prolactin LH, and age. Age related in negative with AMH, HCG_E2, and prolactin or positive with BMI, Inhibin, FSH, LH and TSH, but there were insignificant. AMH changed positively with HCG E2, inhibin B, prolactin, and LH, and negatively with rest hormones. BMI is positively affected by a woman's age and PCOS, this increase in weight affects the production of hormones and the ratio between them. Age affects the increase in the production of inhibin, FSH, LH and TSH, therefore the relationship between AMH and age is negative. |
Introduction
Sex hormones play a crucial role in the continuity of life since they are necessary for reproduction and its continuation. The development and maturity of the ovaries, which generate the ova and cause ovulation, are governed by the hypothalamus-pituitary-ovarian axis [1].
A crucial element in the control of the menstrual cycle is the release of the gonadotropin-releasing hormone (GnRH) by the hypothalamus gland, which in turn stimulates the pituitary gland to release other hormones like prolactin, follicle-stimulating hormone (FSH), and LH from B-cells in the anterior pituitary [2]. While luteinizing hormone (LH) is in charge of the ovulation process in the ovaries once the follicles have reached maturity, FSH works on the evolution and development of ovarian follicles. As a result, a process frequently referred to as luteinizing also aids in the development and function of the corpus luteum. In the embryonic stage, AMH (anti-Müllerian hormone) controls the determination of sex; in males, it promotes the production of male tracts and inhibits the formation of female ducts, and vice versa. It also influences decreasing follicular sensitivity to FSH [3].
More often than FSH, the AMH hormone is used as a biomarker for significant indicators such as ovarian cancer, ovarian ageing, and ova quality [4]. Another name for this hormone is Müllerian Inhibiting Substance (MIS). It is a glycoprotein belonging to the transforming growth factor beta 1 (TGF-β1) family, which controls the growth and differentiation of tissues [5]. The gene responsible for encoding the AMH receptor (AMH-RII) is found on chromosome 12, while the AMH gene is on the short arm of the chromosome (19p13.3) [6].
As an indicator of ovarian reserve in conditions like premature ovarian failure and PCOS, AMH testing can be used to evaluate ovarian function and women's fertility [5]. An ultrasound of the ovaries should be performed after the AMH measurement to evaluate the number and calibre of follicles. When comparing the concentration in healthy women at various age stages, there is a significant decline in AMH concentration with ageing [4].
AMH hormone can be at its highest levels with multiple polycystic ovary syndrome, which gives unclear results on women's fertility. PCOS is the most common hormonal disorder caused by genetic and environmental factors. Signs such as anovulation, obesity, hirsutism, and the appearance of acne, as well as the presence of ovaries containing multiple cysts, affecting approximately 4–12% of women of childbearing age [7].
The causes of polycystic ovary syndrome are not known precisely, and there are many opinions on how to explain its occurrence, including disorders in the hormones that stimulate gonadotropin or a defect in the pituitary gland that increases the ratio of LH to FSH [8]. FSH and increased secretion of male hormones, especially testosterone and prolactin hormone (PRL) affect in some way on insulin's function. Insulin resistance causes Insulin hormone to build up in the blood and its concentration to rise. This increases androgen production, which causes early follicle damage and anovulation. The level of sex hormone binding globulin (SHBG) decreases in response to an increase in insulin, which in turn causes an increase in hormones, particularly the hormone testicular lipids, which in turn causes the development of vascular diseases, cardiovascular disorders, central obesity, and abnormal glucose metabolism [9].
PCOS is one of the most prevalent endocrine diseases in women and one of the primary reasons for infertility [10]. This syndrome is related with numerous indications and symptoms, like weight gain, lipid metabolism issues, insulin resistance, and diabetes [11]. Approximately 30–40% of women with this syndrome have insulin resistance, and they are more likely to develop type 2 diabetes than healthy women [12].
Body mass index (BMI) and polycystic ovarian syndrome are linked. Infertile women had high rates of obesity and central obesity since these conditions affect 10 to 40% of patients. It has been established that 40–90% of women are overweight [13].
Aim of the study:
1. estimation of AMH concentration in women with POCS.
2. figuring out the association between PCOS, BMI, age and AMH.
3. figuring out how age, BMI, and AMH relate to various hormone concentrations in POCS patients.
Materials and Methods:
2.1 Patients and methods:
The study included 62 women with POCS (31.42 ±5.93 years) who attended private women's clinics in Al-Qadisiyah and Al-Muthanna provinces (central-southern Iraq). Their infection was confirmed after an ultrasound examination (sonar).This study performed from December 2022 to May 2023.
2.1.1 Study groups:
After the patients filled out a special questionnaire that included information about the participant’s age, the number of children, and abortion history, and after determining the weight length, the participants were divided into four subgroups according to age and BMI (≥35 years and <35>25 and ≤25) respectively.
2.2 Ethical approvals:
The study was completed by the ethical recommendations of Imam Al-Sadiq University No. 6290- B in 9/23/2022.
2.3 Blood and Serum Samples
10 cc of blood was drawn from the participants on days 2-4 of their menstrual cycle. The serum was separated by centrifugation (242 rpm) for 20 minutes. The serum was stored at -20°C.
2.4 Estimation of hormone concentrations
The concentration of hormones (AMH, E2, HCG E, Inhibin B, Prolactin, LH, FSH, TSH) was measured by the enzyme-linked fluorescence assay technique (ELFA) following the steps indicated in the assay kit for the hormone system (mini VIDAS) from Koma Biotech Inc. Korea [13].
2.5 Measurement of Body mass index
The height and weight of each participant were measured. BMI was calculated by dividing the weight in kilograms by the square of the height in meters [14].
2.6 Statistical analysis
SPSS-24 software was used, where the average, standard deviation and P value were extracted, by calibrating the results of the study groups and using the binary variance method.
Results
Table 1 illustrates the general description of the women in the current study, where the average age was (31.42 ± 5.93) and BMI (27.03± 5.03). Twenty-three of them were over 35 years old. Nineteen were >25 in BMI.
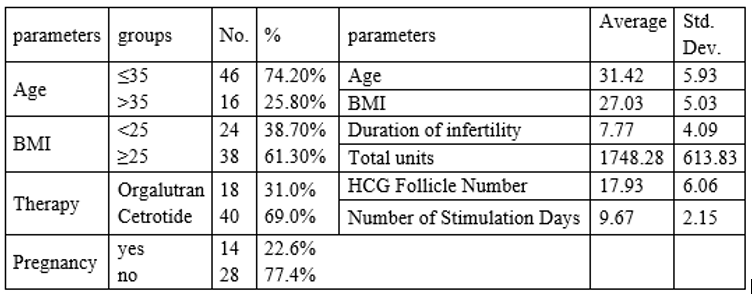
Table 2 demonstrates that the relationship between age and hormone concentration. Although the levels of E2 and LH hormones in >35 group were increased, and the level of HCG E2, Inhibin B, Prolactin, and FSH decreased, all these results were insignificant.
The decrease of hormones AMH (p. value= 0.048) in <=35 group and the increase of hormone TSH (p. value = 0.050) in >35 group were significant.
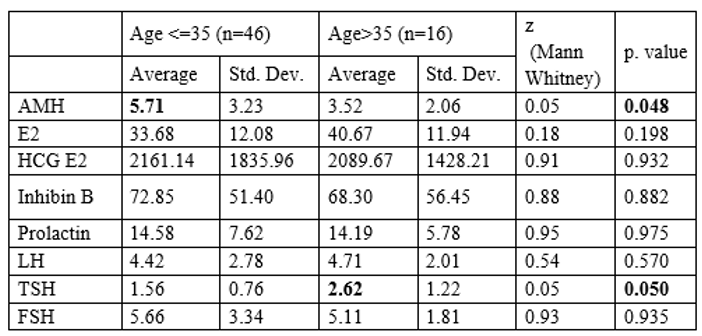
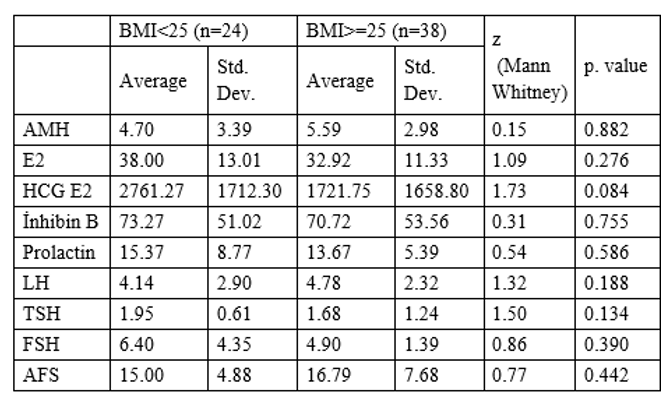
Table 3 represents the relationship between BMI and hormone concentration. Although the levels of AMH and LH increased, and the rest of the hormones decreased with the increase in weight, all these results were insignificant.
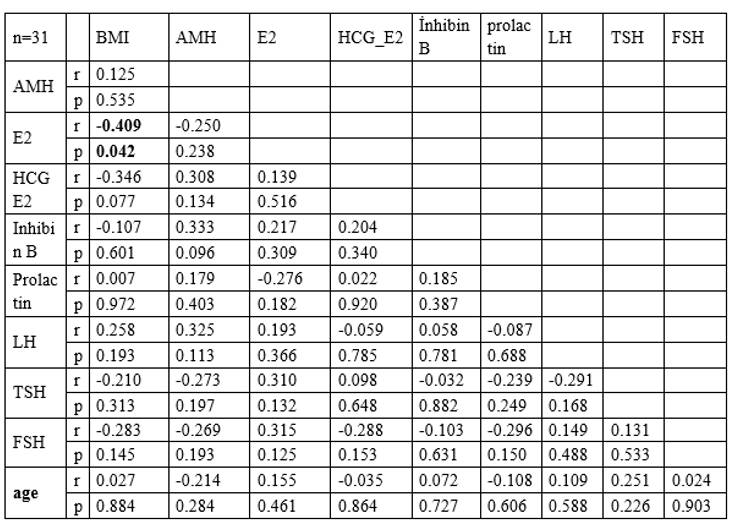
The relationships among all terms were shown in Table 4, here we notice Significant BMI-related variable was Negative (decreasing due to BMI increase) with E2 (r=-0.409; P. value = 0.042), with an insignificant negative association with HCG E2, Inhibin B, TSH, and FSH, with an insignificant positive association with prolactin AMH, LH, and age.
Age-related in negative with AMH, HCG_E2, and prolactin or positive with BMI, inhibin, FSH, LH and TSH, but there were insignificant. AMH changed positively with HCG E2, inhibin B, prolactin, and LH, and negatively with rest hormones and age.
Discussion
Weight gain and a high body mass index are important signs of PCOS [15]. One of the most significant aspects of PCOS syndrome is the link between functional and reproductive changes, which is where obesity plays a significant role. It follows a metabolic pathway that results in peripheral testosterone, which, in addition to the ovaries, is another source of this hormone [16].
The relationship between weight gain and ovulation is inverse, as weight gain may cause increased deposition of grease around the ovaries, which leads to cysts of eggs inside the ovaries, lack of ovulation, menstrual irregularities, and delayed pregnancy [17]. This increase in weight may be due to the possibility of a significant increase in the concentration of total cholesterol in the serum, which results from a rise in the concentration of low-density lipoproteins (LDL) in the serum, in addition to the increase in the concentration of triglycerides due to the syndrome, which leads to Significant increase in weight and disorder in the distribution of fat [18].
Polycystic ovary syndrome is associated with hormonal activity that accompanies young ages (25-35 years) and premenopausal age, and both periods may be related to hormonal instability [19]. Women with PCOS suffer from disturbances in menstrual periods, as these disorders lead to increase the hormonal levels such as androgen hormones (male hormone) then ovulation stops. In addition, the menstrual cycle disorder and irregular menstrual periods Oligomenorrhea or absence of menstruation lead to a disorder in the ovulation process and then the occurrence of infertility [20]. Also, decreased secretion of oestrogen and progesterone leads to thickening of the endometrium, and the condition may develop into endometrial hyperplasia which may cause uterine cancer [21].
PCOS is associated with a high rate of infertility in females. Hypothyroidism caused by a drop in the hormone tri-iodide thyronine (T3) and an increase in the concentration of thyroid-stimulating hormone (TSH), which promotes an increase in the secretion of testicular fat and the occurrence of infertility, may be responsible for high infertility in women with polycystic ovaries. Moreover, a high level of TSH interferes with oestrogen metabolism and lowers the liver's ability to produce (SHBG), which raises the level of free testosterone [22]. It could also Be the primary source of steroid hormones, including androgens, the rise in total cholesterol concentration in polycystic ovarian syndrome patients has a significant impact on the infertile situation [23].
Obesity and increased BMI play a role in infertility due to the imbalance in the secretion of gonadotrophic-releasing hormone (GnRH) or due to the imbalance of the hypothalamic-pituitary axis, which may provoke an increase in the ratio of luteinizing hormone to follicle- follicle stimulating hormone. As a result, stimulates the theca cells of the ovaries to secrete higher levels of testosterone, which may cause an imbalance in the growth and development of the ovarian follicles [24].
Several earlier papers' findings suggest that in the group of women with PCOS, an increase in the corpus luteum-releasing hormone (LHRH) concentration is balanced by a decrease in the concentration of FSH [25]. The needed amount of LH function is to promote the act of ovulation and then encourage the corpus luteum to generate the steroid hormone steroidogenesis, despite the fact that excessive levels of it (LH) suppress the activity of aromatase and inhibit the growth of the oocyte. According to this study, the level of the LH is higher in the follicular phase when compared to a sample Control, which causes hormonal disturbance and prevents ovulation [26].
The pituitary gland and the hypothalamus are among the main organs that regulate the mechanism through which the endocrine system works [27]. The hypothalamus also stimulates the production of gonadal nutrients from the pituitary gland through the pulsating production of hormones that release the gonads' nutrients [28]. When the pulse repetition rate (release rate) of the hormones released by the gonadal nutrients increases, this leads to stimulation of the reproduction of the beta sub-unit of the luteinizing hormone more than the ovarian follicle-stimulating hormone. Reproduction of the beta subunit of LH, thus reducing the production of LH more than FSH [29].
The positive feedback relationship between estradiol and LH stimulates the process of ovulation within the ovarian cells, as estradiol stimulates the response of follicular receptors necessary for the growth and development of the follicle, the increase in oestrogen secretion in the ovary (and adrenergic as well) in the pre-ovulation phase stimulates the hypothalamus to secrete GnRH, which stimulates the anterior lobe the pituitary gland to secrete LH, which affects the ovarian vesicles, where theca cell produces androgens and then converts them into oestrogens with the effect of the FSH hormone [30]. Oestrogens are made from cholesterol in the ovaries as well. Any imbalance in one or more of the roles played by estradiol may lead to a defect in the cycle. An increase in the level of estradiol when it is associated with low levels of progesterone may lead to an increase in the response of the Gonadotrophic -releasing hormone (GnSH-R) and thus may It leads to a rise in the level of (LH) and then produces a second anovulation [31].
LSH secretion and its impact on the cells of the pituitary gland are both inhibited by prolactin. As a result, ovulation is inhibited, the ovaries are rendered ineffective, and oestrogen levels are decreased. This hormone has a stimulating effect on the corpus luteum in the ovaries. The prolactin hormone, also known as luteotrophic hormone (LTH), is one of the gonadotropin hormones as a result [32]. Many people experience an increase in oestrogen levels along with a decrease in prolactin levels, which draws a connection between oestrogens and the release of the hormone of love and raises its concentration in the blood [33].
The majority of women are not aware that beyond their thirties, fertility falls and that as the mother's age increases, the success of assisted reproductive procedures (ARP) likewise substantially declines. The quantity of ovarian follicles declines with age, and they also become less responsive to FSH. Ovulation becomes less effective, predictable, and regular than in prior years. A woman's reproductive cycle will begin to shift between the ages of 38 and 42(34].
When estimating the concentration of AMH according to weight levels, it is noted that there are no significant differences in the concentration of the AMH hormone for healthy women. Because the AMH hormone reduce the sensitivity of the ovarian follicles to the FSH hormone and has a regulatory role for the growth of the follicles and reduces the activity of enzymatic action and the number of recipients of the FSH hormone as it works on reducing the secretion of testosterone from the interstitial cells, so it has nothing to do with weight changes, as AMH is a brake on FSH, which affects weight levels [35].
When estimating the concentration of the oestrogen hormone according to weight levels, it is noted that there are no significant differences in the concentration of the oestrogen hormone, and this is because obesity is most prevalent in the Middle Ages [36]. The steroidal sex hormones are necessary for obtaining and maintaining pregnancy, and oestrogen is not limited to its effect on reproduction and sex functions but also has other effects, including giving secondary sexual characteristics and its importance in tissue construction and bone formation [37].
When estimating the concentration of the follicle-stimulating hormone (FSH) according to weight levels, it is noted that there is a non-significant decrease in the FSH concentration in women who are overweight [38]. The causes of changes in BMI were either a result of disease or exercise, or as a result of an imbalance in the nutritional process, such as loss of appetite, which is often accompanied by a nervous condition, especially when they suffer from menopause, and this would cause an imbalance that affects the ovulation process [39].
There is a rise in the concentration of LH with weight gain, and this is due to the increase in BMI that impedes the ovulation process because obesity leads to the production of more low-density lipoproteins for cholesterol, which is considered one of the harmful fats in the body, which works to cause an imbalance in most of the functions of the body systems through its deposition in its vessels blood vessels, their narrowing, decreased blood flow to these organs, and consequently a lack of hormone secretions, especially the reproductive system [40].
The decrease in the concentration of the prolactin hormone with weight gain is because the prolactin hormone has many biological functions, including secretory, immunological, and regulator of osmosis [41]. Recent research also indicated that prolactin is one of the most important hormones that participate in the regulation of reproduction through its primary role in early embryonic implantation and maintaining it during propagation [42]. Excessive secretion of prolactin is the most common among women suffering from polycystic ovary syndrome [PCOS], which leads to imbalance and abnormal increase in body weight [43].
Conclusion
BMI is positively affected by a woman's age and PCOS, this increase in weight affects the production of hormones and the ratio between them. Age affect the increase in the production of inhibin, FSH, LH and TSH, therefore the relationship between AMH and age is negative.
Declarations
Funding
The author declare that no funds, grants, or other support were received during the preparation of this manuscript.
Authors’ contribution
All parts were done by corresponding author.
Competing interests
The author declares no competing interests.
Conflict of interest
The author declares no competing interests.
References
- Guyton A.C. and Hall J. E. (2010). Textbook of Medical Physiology .11th edition.
View at Publisher | View at Google Scholar - Fowler P.A., Sorsa l., Harris W., and Mason H.D., (2003) Ovarin gandotrophin surge at the hating factor (G.n.s.A.f), J. of Reproduction.126 :689-699.
View at Publisher | View at Google Scholar - Broer S. L., Van Disseldorp J., Broeze K. A., Dolleman M., Opmeer B., et al. (2012).
View at Publisher | View at Google Scholar - Fanchin R1, Schonäuer LM, Righini C, Frydman N, Frydman R, et. al., (2003) Comparison of Specificity and Sensitivity of AMH and FSH in Diagnosis of Premature Ovarian Failure.
View at Publisher | View at Google Scholar - Kebbewar Molecular Diagnostic & Genetic Lab, by NCYHBG, 2015.
View at Publisher | View at Google Scholar - Faddy MJ, Gosden RG, Gougeon A, Richardson SJ, Nelson JF., (1992) Accelerated disappearance of ovarian follicles in midlife: Implications for forecasting menopause. Hum Reprod. 7:1342-1346.
View at Publisher | View at Google Scholar - Aziz R., Woods K S, Reyna R., et al., (2004). The prevalence and features of the polycystic ovary syndrome in an unseleted population, J. Clin Endocrinol and Metabol, 89(6): 2745- 2749.
View at Publisher | View at Google Scholar - Essach, P. A ., Wickham E P & Nestler J. E.(2007). The metabolic Syndrome in polycystic ovary Syndrome . Clinical Obstetrics and Gynecology, 50:205-225.
View at Publisher | View at Google Scholar - Howard S. and Jacobs S., (1995) ((Poly Cystic Ovary Syndrome aetiology and management) Current opinion inobestet and Gynecol, 7 :P: 203-208
View at Publisher | View at Google Scholar - Goldenberg, N., Glueck C. (2008).
View at Publisher | View at Google Scholar - Norman R.J., Dewailly D., Legro R.S. and Hickey T.E. (2007). Polycystic ovary syndrome. Lancet 37(9): 697-685.
View at Publisher | View at Google Scholar - SchroderA.K., Tauchert,S., Ortmann O., Diedrich k., and Weiss J.M., (2004).Insulin resistence in patients with polycystic ovary syndrome. Ann.Med.,36(6): 426-439.
View at Publisher | View at Google Scholar - Al-Ardi M.H. (2022). The Role of Hormones and Toxoplasma gondii Infection to Change the Secondary Sex Ratio. Iraqi Journal of Science, 63(7): 2850-2860.
View at Publisher | View at Google Scholar - Al-Ardi M.H. (2021). The role of Toxoplasma gondii in concentration of some sex hormones in infertile individual. Journal of medical & pharmaceutical Sciences, 5(1): 72-82.
View at Publisher | View at Google Scholar - Hoeger K. M., Dokras A., and Piltonen T. (2021). Update on PCOS: consequences, challenges, and guiding treatment. The Journal of Clinical Endocrinology & Metabolism, 106(3): e1071-e1083.
View at Publisher | View at Google Scholar - Rudnicka E., Suchta K., Grymowicz M., Calik-Ksepka A., Smolarczyk K., et. al., (2021). Chronic low-grade inflammation in pathogenesis of PCOS. International journal of molecular sciences, 22(7): 3789.
View at Publisher | View at Google Scholar - Barber T. M., and Franks S. (2021). Obesity and polycystic ovary syndrome. Clinical endocrinology, 95(4): 531-541.
View at Publisher | View at Google Scholar - Hu L., Ma L., Xia X., Ying T., Zhou M., et. al., (2022). Efficacy of bariatric surgery in the treatment of women with obesity and polycystic ovary syndrome. The Journal of Clinical Endocrinology & Metabolism, 107(8): e3217-e3229.
View at Publisher | View at Google Scholar - Kim C. H., Chon S. J., and Lee S. H. (2020). Effects of lifestyle modification in polycystic ovary syndrome compared to metformin only or metformin addition: a systematic review and meta-analysis. Scientific reports, 10(1): 1-13.
View at Publisher | View at Google Scholar - Abbara A., Eng P. C., Phylactou M., Clarke S. A., Hunjan T., et. al., (2019). Anti-müllerian hormone (AMH) in the diagnosis of menstrual disturbance due to polycystic ovarian syndrome. Frontiers in endocrinology, 10: 656.
View at Publisher | View at Google Scholar - Park Y. J., Shin H., Jeon S., Cho I., and Kim Y. J. (2021). Menstrual cycle patterns and the prevalence of premenstrual syndrome and polycystic ovary syndrome in Korean young adult women. In Healthcare, Vol. 9(1): p. 56.
View at Publisher | View at Google Scholar - Fatima M., Amjad S., Ali Sr H. S., Ahmed T., Khan S., et. al., (2020). Correlation of subclinical hypothyroidism with polycystic ovary syndrome (PCOS). Cureus, 12(5).
View at Publisher | View at Google Scholar - Raj D., Pooja F. N. U., Chhabria P., Kalpana F. N. U., Lohana S., et. al., (2021). Frequency of subclinical hypothyroidism in women with polycystic ovary syndrome. Cureus, 13(9).
View at Publisher | View at Google Scholar - Li C., Xing C., Zhang J., Zhao H., Shi W., et. al., (2021). Eight-hour time-restricted feeding improves endocrine and metabolic profiles in women with anovulatory polycystic ovary syndrome. Journal of translational medicine 19(1): 1-9.
View at Publisher | View at Google Scholar - Le M. T., Le V. N. S., Le D. D., Nguyen V. Q. H., Chen C., et. al., (2019). Exploration of the role of anti‐Mullerian hormone and LH/FSH ratio in diagnosis of polycystic ovary syndrome. Clinical Endocrinology, 90(4), 579-585.
View at Publisher | View at Google Scholar - Khmil M., Khmil S., and Marushchak M. (2020). Hormone imbalance in women with infertility caused by polycystic ovary syndrome: is there a connection with body mass index? Open Access Macedonian Journal of Medical Sciences, 8(B), 731-737.
View at Publisher | View at Google Scholar - Garg A., Patel B., Abbara A., and Dhillo W. S. (2022). Treatments targeting neuroendocrine dysfunction in polycystic ovary syndrome (PCOS). Clinical Endocrinology, 97(2): 156-164.
View at Publisher | View at Google Scholar - Szczuko M., Kikut J., Szczuko U., Szydłowska I., Nawrocka-Rutkowska J., Ziętek M., and Saso L. (2021). Nutrition strategy and life style in polycystic ovary syndrome—Narrative review. Nutrients, 13(7): 2452.
View at Publisher | View at Google Scholar - Abbara A., and Dhillo W. S. (2021). Targeting elevated GnRH pulsatility to treat polycystic ovary syndrome. The Journal of Clinical Endocrinology & Metabolism, 106(10): e4275-e4277.
View at Publisher | View at Google Scholar - Zhu J. L., Chen, Z., Feng W. J., Long S. L., and Mo Z. C. (2019). Sex hormone-binding globulin and polycystic ovary syndrome. Clinica chimica acta, 499: 142-148.
View at Publisher | View at Google Scholar - Vaez S., Parivr K., Amidi F., Rudbari N. H., Moini A., and Amini N. (2023). Quercetin and polycystic ovary syndrome; inflammation, hormonal parameters and pregnancy outcome: A randomized clinical trial. American Journal of Reproductive Immunology, 89(3): e13644.
View at Publisher | View at Google Scholar - Vural F., Vural B., Kardaş E., Ertürk Coşkun A. D., and Yildirim İ., (2023). The diagnostic performance of antimullerian hormone for polycystic ovarian syndrome and polycystic ovarian morphology. Archives of Gynecology and Obstetrics, 307(4): 1083-1090.
View at Publisher | View at Google Scholar - He Y., Wang Q., Li X., Wang G., Zhao J., et al., (2020). Lactic acid bacteria alleviate polycystic ovarian syndrome by regulating sex hormone related gut microbiota. Food & function, 11(6): 5192-5204.
View at Publisher | View at Google Scholar - Zhang C., Liu J., Lai M., Li J., Zhan J., et al., (2019). Circular RNA expression profiling of granulosa cells in women of reproductive age with polycystic ovary syndrome. Archives of Gynecology and Obstetrics, 300: 431-440.
View at Publisher | View at Google Scholar - Dewailly D., Barbotin A. L., Dumont A., Catteau-Jonard S., and Robin, G. (2020). Role of anti-Müllerian hormone in the pathogenesis of polycystic ovary syndrome. Frontiers in Endocrinology, 11: 641.
View at Publisher | View at Google Scholar - Bahri Khomami M., Joham A. E., Boyle J. A., Piltonen T., Silagy M., et al., (2019). Increased maternal pregnancy complications in polycystic ovary syndrome appear to be independent of obesity—A systematic review, meta‐analysis, and meta‐regression. Obesity Reviews, 20(5): 659-674.
View at Publisher | View at Google Scholar - D'Alterio M. N., Sigilli M., Succu A. G., Ghisu V., Laganà A. S. et al., (2021). Pregnancy outcomes in women with polycystic ovarian syndrome. Minerva Obstetrics and Gynecology, 74(1): 45-59.
View at Publisher | View at Google Scholar - Kelley A. S., Smith Y. R. and Padmanabhan, V. (2019). A narrative review of placental contribution to adverse pregnancy outcomes in women with polycystic ovary syndrome. The Journal of Clinical Endocrinology & Metabolism, 104(11): 5299-5315.
View at Publisher | View at Google Scholar - Hu S., Xu B., Long, R., and Jin L. (2021). The effect of polycystic ovary syndrome without hyperandrogenism on pregnancy‐related outcomes: a retrospective cohort study. BJOG: An International Journal of Obstetrics & Gynaecology, 128(6):1003-1010.
View at Publisher | View at Google Scholar - Yan Q., Qiu D., Liu X., Xing Q., Liu R., et al., (2022). The incidence of gestational diabetes mellitus among women with polycystic ovary syndrome: a meta-analysis of longitudinal studies. BMC Pregnancy and Childbirth, 22(1), 1-12.
View at Publisher | View at Google Scholar - Valdimarsdottir R., Wikström A. K., Kallak T. K., Elenis E., Axelsson O., et al., (2021). Pregnancy outcome in women with polycystic ovary syndrome in relation to second-trimester testosterone levels. Reproductive BioMedicine Online, 42(1): 217-225.
View at Publisher | View at Google Scholar - Liu S., Mo M., Xiao S., Li L., Hu X., et al., (2020). Pregnancy outcomes of women with polycystic ovary syndrome for the first in vitro fertilization treatment: A retrospective cohort study with 7678 patients. Frontiers in Endocrinology, 11, 575337.
View at Publisher | View at Google Scholar - Debras E., Fernandez H., Neveu M. E., Deffieux X., and Capmas P. (2019). Ovarian drilling in polycystic ovary syndrome: Long term pregnancy rate. European Journal of Obstetrics & Gynecology and Reproductive Biology: X, 4, 100093.
View at Publisher | View at Google Scholar
