

Review Article | DOI: https://doi.org/10.31579/ 2835-8147/008
Polymastia: What you Should Know. From One Man Case Discovered by Chance
- Bellahsene-Bendib *
- Y. Achir
- D. Aiche
- C. Aimeur
Medical imaging service, University Hospital Center Mustapha-Bacha, Algiers.
*Corresponding Author: S. Bellahsene-Bendib, Medical imaging service, University Hospital Center Mustapha-Bacha, Algiers.
Citation: S. Bellahsene-Bendib, Y. Achir, D. Aiche, C. Aimeur (2023), Polymastia: what you should know. From one man case Discovered by Chance, Clinics in Nursing, 2(1) DOI:10.31579/ 2835-8147/008
Copyright: © 2023 S. Bellahsene-Bendib, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 January 2023 | Accepted: 31 January 2023 | Published: 17 February 2023
Keywords: polymastia; supernumerary breasts; brest ridges; ct scan
Abstract
Lavender belongs to the genus Lavandula and the family Lamiaceae. Among the factor affecting the quality of lavender plant chemotype, are harvesting and storage conditions. No further study has been done on drying conditions and time in Ethiopia so far. The fresh leaf of the Lavender cultivar was subjected to sun and shade drying conditions and four drying days (0,5, 10, and 15). From each sample, the essential oil was extracted. The extracted essential oil was subjected to physical parameters analysis: - essential oil content (volume by weight and weight by weight), specific gravity, and refractive index. Local lavender shows a higher essential oil content and moisture content than the flowering lavender cultivar. All physical properties of essential oils except specific gravity, show significant differences in all cases between cultivar, drying conditions, drying days, and interaction effect of all cases. This shows drying conditions and drying days affect the quality of lavender essential oils. Therefore, this study provides evidence (information) that drying herbs on different drying days and drying conditions affect the essential oil content and physical properties of essential oil.
Introduction
Supernumerary breasts (SB) represent the most common congenital breast defect. They can affect both sexes. They include polymastia (PM) and polythelia. Polymastia is characterized by the presence of more than two mammary glands associated or not with a nipple or an areola. Polythelia is defined by the presence of one or more supernumerary nipples with or without areolas. Supernumerary breasts result from the absence of regression of residual breast tissue located along the breast ridges or primitive milky lines, extending from the axillary region to the inguinal fold and located on either side of the trunk (Fig. 1) [1]. Polymastia commonly sits along the breast ridges and much more rarely outside. We report a case of polymastia of the abdominal wall discovered fortuitously in a 77-year-old man during an abdominopelvic CT scan.

Figure 1: Milky line extending from the axillary region to the inguinal crease.
The interest of our article is to make known the existence of this type of breast malformation often unrecognized by the radiologist, in particular in men, especially since this accessory breast tissue can present the same pathologies as breast tissue in a normal situation or be associated with other malformations or systemic neoplasms, particularly renal and urinary [1].
Observation
This is a 77-year-old patient who was referred to us for an abdominal CT scan as part of the exploration of a suspicious thickening of the gallbladder wall, detected during a previous ultrasound. This patient had no particular history other than insulin-dependent diabetes and functional colopathy. The CT scan performed without and with injection of contrast product revealed gallbladder parietal thickening without infiltration of the adjacent hepatic parenchyma or associated locoregional lymphadenopathy. He also showed at the level of the anterior abdominal wall, at the level under the umbilical, two small solid formations, under the skin, roughly triangular, of symmetrical arrangement with respect to the median line, leaning against the fascia superficialis and located on the trajectory breast ridges. These formations were isodense to muscle structures either spontaneously or after iodine injection. They measured 41 x 13.5 mm large axes on the right and 35 x 11.5 mm on the left. Their contours, jagged in appearance, strongly evoked the crests of Duret. The skin covering in contact with them was slightly thickened but regular (Fig. 2). There were no other associated anomalies on the sections performed. Faced with this CT appearance, we concluded to the diagnosis of ectopic mammary glands rather than secondary subcutaneous localizations raised in the first place because of the clinical context of our patient.

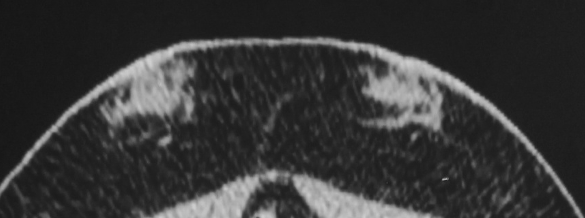
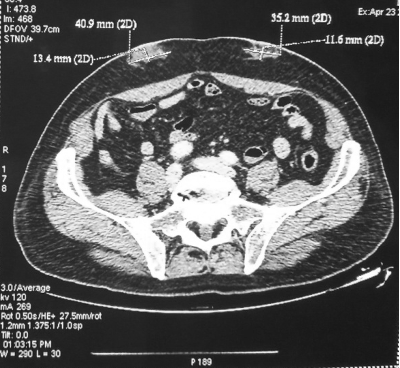
Figure 2: Abdominal CT slices with contrast. Appearance of subcutaneous ectopic mammary glands of the anterior abdominal wall (a). Bilateral and symmetrical location with respect to the midline. Roughly triangular shape. Crenellated contours evoking Duret ridges (b). Discreet size asymmetry in favor of the right gland (c). Localized skin thickening opposite (a-c).
We completed the exploration with an ultrasound of the abdominal wall performed using a superficial probe. It showed two oval areas, under the skin, fairly well circumscribed, with a long transverse axis parallel to the skin covering, with hyper and hypoechogenic tissue echostructure, without visible milk ducts. There was no associated posterior attenuation, mass or collection, or underlying muscle infiltration. The adjacent skin covering was also discreetly thickened (Figure. 3).
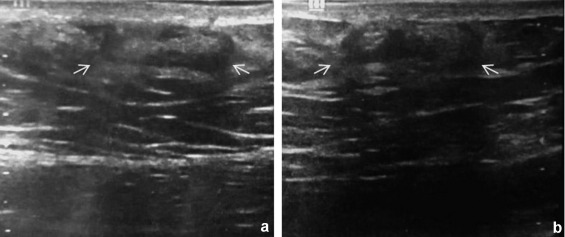
Picture 3: Ultrasound focused on the abdominal wall. Right (a) and left (b) right (a) and left (b) subcutaneous oval formations with long transverse axis, fairly well limited, with hyper and hypoechoic solid echostructure. Absence of obvious milk ducts. Moderate and regular thickening of the overlying skin covering.
On inspection of the abdomen, we did not find any cutaneous swelling, nipple or areolar plaque. There were a few nevi, scattered around the abdomen, predominantly above the umbilical, but none was located opposite the CT lesions (Figure. 4). There was also no erythema, induration or mass on palpation. The patient reported no sensitivity at this level.

Figure 4: Scattered abdominal cutaneous naevi predominantly above the umbilical level.
At the end of our interpretation, we concluded that there was bilateral and symmetrical, uncomplicated polymastia of the abdominal wall, without associated nipple or areola.
The treating surgeon decided to remove the suspected gallbladder without intervention on the polymastia given the absence of symptoms and the age of our patient. Only simple ultrasound monitoring was recommended depending on the clinical evolution.
Discussion
PM are congenital breast malformations. They are less common than polythelia. Well known since antiquity as a sign of fertility and femininity, they are considered a curiosity in man. These are minor abnormalities but likely to be complicated by the same pathologies as normal breast tissue. More rarely, they can be the marker of malformations and/or systemic pathologies, in particular urogenital [2,3].
Epidemiology
Supernumerary breasts (SB) are rare, occurring in 02 to 6% of the general population and are more common in Asian and black populations. They can affect both sexes but are more rarely reported in men [4,5].
Embryology
Supernumerary breasts are the expression of an incomplete embryological involution of the primordial mammary cell groups located along the mammary ridges. In humans and mammals, breast development begins in the fourth embryonic week with the formation of a mammary ridge or lacteal line located on either side of the ventral side of the embryo and extending from the future armpit to the future inguinal fold (Figure. 1). Along this ridge, five to seven pairs of mammary buds will develop symmetrically and depending on the species. During human development, the thoracic mammary buds located on the mid-clavicular line evolve into mammary glands while the other buds gradually involute. Around the seventh week, only two primary buds of the pectoral seat persist in humans, which will give rise to the two mammary glands. In some cases, extra-thoracic buds may persist as vestigial structures and develop along the mammary ridge, giving rise to accessory breasts [6]. Much more rarely, breast tissue develops outside the milk line or exceptionally within internal organs. This is caused by cells spilling out from small breast crest diverticula which subsequently lose contact with it [7].
Supernumerary breasts may be more or less developed and furnished with glandular tissue (5). They were classified in 1915, by Kajava [8], into eight categories, still in use today:
‒ Class 1: Full breast with glandular tissue, areola and nipple
‒ Class 2: Glandular tissue and nipple without areola
‒ Class 3: Glandular tissue and areola without any nipple
‒ Class 4: Glandular tissue alone
‒ Class 5: Areola and nipple without glandular tissue, replaced by fatty tissue
(pseudomamma)
‒ Class 6: Nipple only (true polythelia)
‒ Class 7: Areola only (areolar polythelia)
‒ Class 8: Plate of hairs only (hairy polythelia)
Polymastia is characterized by the development of a mammary gland with or without nipple and/or areola (grades 1 to 4). Our case corresponded to class 4. True polymastia or fully functional breast (class 1) is exceptional.
Location
About 67% of the supernumerary mammary glands, sit at the thoracic level (above or below the eutopic glands) or abdominal and 20% at the axillary level especially in women. At the abdominal level, they are most often located between the epigastrium and the umbilical, the seat below the umbilical being extremely rare (5%). The other locations, inguinal or on the inner thigh, are also uncommon [2,9,10]. PM in an aberrant position, located outside the mammary line, have been reported in different regions (face, neck, shoulder, arm, parasternal region, back, flank, hip, buttocks, ano-perineal region, vulva, posterior aspect of the thigh or sole) [11-14]. Exceptional localizations at the level of internal organs have also been described: pulmonary, cardiac and mesenteric. the diagnosis of which was made only after anatomopathological study of excision specimens [15,16].
Number, size and distribution
The PM, is of variable number: one to two most often, being able to reach sometimes five, six or even ten glands. It is bilateral in a third of cases, generally perfectly symmetrical. The size of the PM can vary from 1.3 to 46 cm. When they are paired, their development is generally unequal, predominant on the right in men and on the left in women [2,9,17]. In our observation, the PM was bilateral, with a perfectly symmetrical distribution on either side of the midline with indeed a right gland of slightly larger size than the left gland (Fig. 2).
Clinical
Unlike polythelia, which is easily identifiable from birth, PM, in the absence of the nipple or areola, the most frequent case, goes unnoticed in men, whatever their age, and in the majority of cases in women. Its discovery is then fortuitous and generally late, during a clinical examination or following an imaging examination [1] as in the case of our patient. Its diagnosis can also be linked to an underlying breast pathology . In one third of women, polymastia only becomes evident at the time of hormonal changes (puberty, menstruation, gestation, lactation, menopause) with the appearance of more or less significant subcutaneous swelling, tenderness or engorgement with milky discharge in the event of an associated nipple [3,12].
Imaging
The supernumerary glandular tissue has the same radiological appearance as the normal gland, regardless of the imaging technique used [18,19]. Ultrasound, thanks to real time and color Doppler, most often makes it possible to differentiate the supernumerary breast from other tumoral pathologies. The ectopic tissue appears with an echostructure similar to the normal mammary parenchyma comprising the connective-glandular tissue of echogenic appearance, the adjacent hypoechoic fatty lobules as well as the well individualized galactophoric ducts in women but poorly developed in men in the normal state. normal. The predominance of fatty tissue, especially in pseudomamma (Kajava category 5), may sonically mistake them for a lipoma, thus misrecognizing or delaying the diagnosis of PM. In mammography, the tonality of the accessory mammary glands is comparable to breast tissue in normal position with alternating light fatty and connective -glandular fluid tones. On MRI, supernumerary glandular tissue appears as a mass or non-mass, signal and contrast comparable to normal breast tissue with minimal, moderate or marked enhancement [20,21].
Scanner performance is considered poor in breast exploration. After reviewing the literature, we have not found, to our knowledge, any case of polymastia detected on the scanner. In our patient, the diagnosis of PM was facilitated by the rather triangular morphology of the two subcutaneous masses, their bilateral and symmetrical distribution, their crenellated contours evoking Duret ridges and the localized skin thickening at the contact which had made us evoke a areolar plate.
Differential diagnoses
The diagnosis of PM is difficult because of its often atypical appearance and its sometimes unusual ectopic locations. In women, hormonal variations are an argument in favor of PM. In humans, in the absence of swelling, nipple or areolar plaque, PM goes, like our patient, completely unnoticed . In case of isolated swelling, the PM can be confused with various pathologies such as lipoma, neurofibroma, vascular malformation, neoplasia or any other tumor [22]. The clinical search for a rudimentary nipple, often mistaken for a nevus or a pigment spot opposite, is important to guide the diagnosis. It will be supplemented by ultrasound exploration and, depending on the case, by cross-sectional imaging (MRI/CT). Indeed, imaging can provide certain diagnostic arguments in favor of supernumerary breasts such as the location of the lesion along the path of the mammary ridges, their bilateral and symmetrical distribution when they are pairs and their morphological appearance. In case of persistent diagnostic doubt, a guided biopsy with a view to a histological study is then necessary [2].
Genetic
Supernumerary breasts are usually sporadic. Familial forms are reported in 6 to 11%. An autosomal dominant genetic transmission, linked to the X chromosome would be involved, with incomplete penetrance and variable expressivity [5,10].
Associations
The supernumerary mammary glands would be, as in our patient, frequently associated with cutaneous nevi [2]. They would also be but in a discussed way in particular in the event of associated nipple, the markers of various malformations, essentially reno-urinary and cardiovascular, more incidentally gastrointestinal, bone, neurological, dental, cutaneous or complex genetics. They would also be linked to various hematological disorders and uro-genital neoplasms [3,5,23-26]. For this, some authors recommend the systematic search for urinary and cardiovascular abnormalities [27]. Our patient had no malformative or neoplastic pathology in his history or detectable on CT or ultrasound.
Complications
The accessory glandular tissue can present the same pathologies (inflammatory, tumoral or dystrophic) as the breast tissue in a normal situation. Malignant degeneration is rare, estimated between 0,2 and 0,6% of all breast cancers [28]. It predominates in women in the postmenopausal period and in axillary localizations. Very rare in humans, this possibility should be considered. The majority of polymastia cancers are represented by ductal carcinomas followed by medullary and lobular carcinomas. Their prognosis seems worse than for breasts in a normal situation due to the frequently associated diagnostic delay [29,30].
Therapeutic care
The management of PM is controversial. Some authors opt for systematic excision of ectopic breast tissue to prevent malignant degeneration [12,30]. Others, given the low neoplastic risk, prefer abstention and only intervene in the event of an aesthetic handicap, troublesome symptoms or secondary complications. Regular monitoring is therefore recommended [30], which was the case in our patient.
Conclusion
Polymastia is a congenital breast abnormality that can affect both sexes. It should not be ignored by the radiologist. Less common in men, it predominates in the thorax and abdomen with subumbilical location considered uncommon. Usually asymptomatic in men, PM often goes unnoticed, especially in the absence of nipple and/or areola, resulting in late diagnosis. Imaging can, as in our case, incidentally detect PM. It is therefore necessary for the radiologist to know its eventuality, its radiological presentation as well as its complications and/or possible associations. In our case, the scanner enabled us to evoke the diagnosis of PM of the abdominal wall in a male patient, thanks to the morphological appearance of the two subcutaneous masses, comparable to that of the mammary glands in a normal situation, at their location on the lacteal line and their very evocative bilateral and symmetrical distribution. The scanner also allowed us to eliminate malformative or neoplastic pathology associated in particular renal and urinary.

References
- Grossl NA (2000). Supernumerary breast tissue: historical perspectives and clinical features. South Med J 93(1):29-32
View at Publisher | View at Google Scholar - Bouchereau M (1906). Of polymastia in man; of its frequency in the Lyon population. In: Bulletin of the Anthropological Society of Lyon (25):56-63.
View at Publisher | View at Google Scholar - Firmin-Lefebvre D, Misery L (2013). Pathology of the male breast. Annals of Dermatology and Venereology (140):436-43.
View at Publisher | View at Google Scholar - Schmidt H (1998). Supernumerary nipples: prevalence, size, sex and side predilection - a prospective clinical study. Eur J Pediatr 157:821-3.
View at Publisher | View at Google Scholar - Urbani CE, Betti R (1995). Familial aberrant mammary tissue: a clinicoepidemiological survey of 18 cases. Dermatology 190:207-9.
View at Publisher | View at Google Scholar - Khoummane N, Yousfi M (2014). Seins surnuméraires axillaires bilatéraux. Pan Afr Med J 17:45.
View at Publisher | View at Google Scholar - Beler F(1990). Development and anatomy of the breast. In Mitchell GW Jr. Basser LW (eds): The female breast and its disorders. Baltimore, Williams & Wilkins.
View at Publisher | View at Google Scholar - Kajava Y(1915). «The proportions of supernumerary nipples in the Finnish population» Duodecim 1:143-70.
View at Publisher | View at Google Scholar - Blanchard R (1885). On a case of polymastia and the significance of supernumerary breasts. Bulletins and Memoirs of the Anthropological Society of Paris 8:226-39.
View at Publisher | View at Google Scholar - Teixeira IP, Azzopardi C, Chowdhury R, Zsolt O, Castro M, Teh J(2020). Ectopic breast tissue presenting as an enlarging abdominal mass. Radiol Case Rep15(6): 733-40.
View at Publisher | View at Google Scholar - Koltuksuz U, Ayden E (1997). Supernumerary breast tissue: a case of pseudomamma on the face. J Pediatr Surg 32:1377-8.
View at Publisher | View at Google Scholar - Chan NG, Penswick JL, Labelle E, Driman DK (2007). Ectopic breast tissue presenting as an anal polyp. Can J Surg 50(6).
View at Publisher | View at Google Scholar - Baradwan S, Wadi KA (2018). Unilateral ectopic breast tissue on vulva in postpartum woman: A case report. Medicine (Baltimore) 97(6):e9887.
View at Publisher | View at Google Scholar - Balakrishnan T, Madaree A (2010). Case report: ectopic nipple on the sole of the foot, an unexplained anomaly. J Plast Reconstr Aesthet Surg 63(12):2188-90.
View at Publisher | View at Google Scholar - Mahmodlou R, Sugumaran RK, Sepehrvand N (2015). Away from the milky way: An extremely rare case of pulmonary ectopic breast. Lung India. 32(1):60-3.
View at Publisher | View at Google Scholar - Sasaki K, Parwani AV, Demetris AJ, Sasatomi E (2010). “Heterotopic breast epithelial inclusion of the heart: report of a case”. American Journal of Surgical Pathology34(10):1555-9.
View at Publisher | View at Google Scholar - Hiremath B, Subramaniam N, Chandrashekhar N(2015). Giant accessory breast: a rare occurrence reported, with a review of the literature Case Reports 2015:bcr2015210918.
View at Publisher | View at Google Scholar - Lim HS, Kim SJ, Baek JM, et al (2017). Sonographic Findings of Accessory Breast Tissue in Axilla and Related Diseases. J Ultrasound Med 36(7):1469‐1478.
View at Publisher | View at Google Scholar - Laor T, Collins MH, Emery KH, Donnelly LF, Bove KE, Ballard ET (2004). MRI appearance of accessory breast tissue: a diagnostic consideration for an axillary mass in a peripubertal or pubertal girl. Am J Roentgenol 183(6):1779-81.
View at Publisher | View at Google Scholar - DeFilippis EM, Arleo EK (2014). The ABCs of accessory breast tissue: basic information every radiologist should know. AJR Am J Roentgenol 202(5):1157-62.
View at Publisher | View at Google Scholar - Adler DD, Rebner M, Pennes DR (1987). Accessory breast tissue in the axilla: mammographic appearance. Radiology 163(3):709-11.
View at Publisher | View at Google Scholar - Husain M, Khan S, Bhat A, Hajini F (2014). Accessory breast tissue mimicking pedunculated lipoma. BMJ Case Rep 2014:bcr 2014204990.
View at Publisher | View at Google Scholar - Brown J, Schwartz RA (2004). Supernumerary nipples and renal malformations: a family study. J Cutan Med Surg 8(3):170-2.
View at Publisher | View at Google Scholar - Rajaratnam K, Kumar PD, Sahasranam KV (2000). « Supernumerary nipple as a cutaneous marker of mitral valve prolapse in Asian Indians ». Am J Cardiol 86(6):695-7.
View at Publisher | View at Google Scholar - Dogana M, Kabaa S, Borab A, Bulana K, Kocaman S (2015). Supernumerary nipples, congenital scoliosis, occult spina bifida, tethered cord and diastematomyelia. Eastern Journal of Medicine 20:46-8.
View at Publisher | View at Google Scholar - Cohen PR, Kurzrock R (1995). Miscellaneous genodermatoses: Beckwith-Wiedemann syndrome, Birt-Hogg-Dube syndrome, familial atypical multiple mole melanoma syndrome, hereditary tylosis, incontinentia pigmenti, and supernumerary nipples. Dermatol Clin. 13(1):211‐229.
View at Publisher | View at Google Scholar - Lewis EJ, Crutchfield CE, Prawer SE (1997). Accessory nipples and associated conditions. Pediatr Dermatol 14:333-4.
View at Publisher | View at Google Scholar - Senatore G, Zanotti S, Cambrini P, Montroni I, Pellegrini A, Montanari E, Santini D, Taffurelli M (2010). Ectopic breast fibroadenoma. Case report. G Chir 31(3):96-9.
View at Publisher | View at Google Scholar - Yamamura J, Masuda N, Kodama Y, Yasojima H, Mizutani M, Kuriyama K and Sekimoto M (2012). Male breast cancer originating in an accessory mammary gland in the axilla: A case report. Case Rep Med 286210.
View at Publisher | View at Google Scholar - Zhang S, Yu Yh, Qu W, Zhang Y, Li J (2015). Diagnosis and treatment of accessory breast cancer in 11 patients. Oncology Letters 10:1783-8.
View at Publisher | View at Google Scholar
