

Case report | DOI: https://doi.org/10.31579/2834-796X/065
Pneumopericardium a Rare Complication of Pericardiocentesis
*Corresponding Author: Amit Mandal, Department of Cardiology, Christian Medical College, Vellore, Tamil Nadu, India.
Citation: Amit Mandal (2024), Pneumopericardium a Rare Complication of Pericardiocentesis, International Journal of Cardiovascular Medicine, 3(3); DOI:10.31579/2834-796X/065
Copyright: © 2024, Amit Mandal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 May 2024 | Accepted: 11 June 2024 | Published: 17 June 2024
Keywords: pneumopericardium; pericardiocentesis; echocardiography
Abstract
Pneumopericardium is a rare complication of pericardiocentesis and defined as the presence of air in the pericardial space. Pneumopericardium usually occurs after trauma. However, pneumopericardium due to iatrogenic procedures, such as pericardiocentesis, is very rare. Immediate recognition and treatment are crucial and chest X-ray, thorax computerized tomography and transthoracic echocardiography helps in making a diagnosis. Herein, we report the case of a 48-year-old female with cardiac tamponade who developed pneumopericardium after pericardiocentesis.
Introduction
Pneumopericardium is a rare condition in which there is air in the pericardial space. It usually occurs after trauma. However, iatrogenic pneumopericardium during pericardiocentesis is rare. Imaging methods are the mainstay in making the diagnosis of pneumopericardium. Posteroanterior chest radiography reveals the typical finding of radiolucent rim separating the pericardium from the heart. Echocardiography can demonstrate mobile air bubbles around the pericardium. Chest tomography is the gold standard for definitive diagnosis. Herein, we report the case of a 48-year-old female with cardiac tamponade who developed pneumopericardium after pericardiocentesis.
Case Presentation
A 46-year-old lady was admitted with worsening of breathing difficulty for two weeks. She had a history of pulmonary tuberculosis four years back and has taken six months of anti-tubercular medication. Physical examination revealed stable vital signs.
Posteroanterior chest radiograph showed cardiomegaly without any lung lesion. (Figure 1) An emergent ECHO cardiogram showed moderate Pericardial effusion (posteriorly 17mm, anteriorly 4mm, laterally 6mm) There was no RA/RV diastolic collapse seen. (Figure 2)

Figure 1: chest radiograph showing cardiomegaly without any lung lesion.
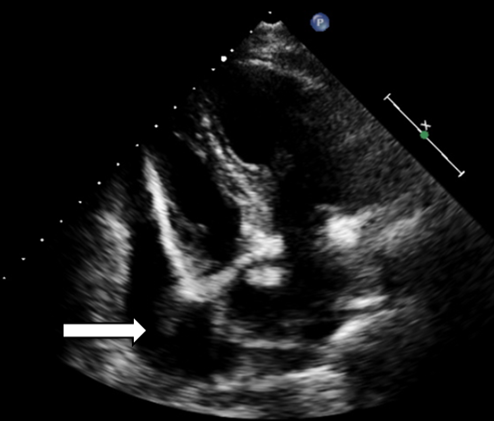
Figure 2: Transthoracic echo showing pericardial effusion. (white arrow)
He was taken up for pericardiocentesis under Local Anaesthesia. After instillation of 2% xylocaine in the subxiphoid area, the micropuncture needle was used to enter pericardial cavity, and with the use of guidewire, 6F sheath and 6F Pigtail catheter was inserted and 800 ml straw coloured pericardial fluid was drained and was sent for analysis. Echo showed no pericardial fluid and procedure was stopped. Sheath and pigtail were removed. Subsequently, the patient's resting dyspnea was resolved. Sputum and pericardial fluid cultures and smear for AFB and other organisms were negative. The pericardial fluid was a lymphocyte dominant exudate, containing protein 6.4 g/dL, albumin 3.5 g/dL, lactate dehydrogenase 194 U/L and white blood cell 200 cells/µL (lymphocyte 94%). Polymerase chain reaction for Mycobacterium tuberculosis deoxyribonucleic acid was negative.
Next day the patient developed a pleuritic chest pain with respiratory distress with hypotension. Follow up chest radiograph showed a lucency around the cardiac silhouette with 'continuous diaphragm sign', limited superiorly by the cardiac pedicle, which was not seen in previous radiograph with reduction in cardiac size. (Figure 3). Emergency CT Thorax revealed pneumopericardium. (Fig 4) In view of pneumopericardium with hemodynamic compromise she was taken up for pericardiocentesis again and final flouro showed minimal residual air in the pericardial cavity. Recheck echo showed normal biventricular function and no features of cardiac tamponade. Subjective symptoms and radiological signs of pneumopericardium disappeared five days later. (Fig 5) The patient’s clinical syndrome was treated with steroids and antitubercular therapy.
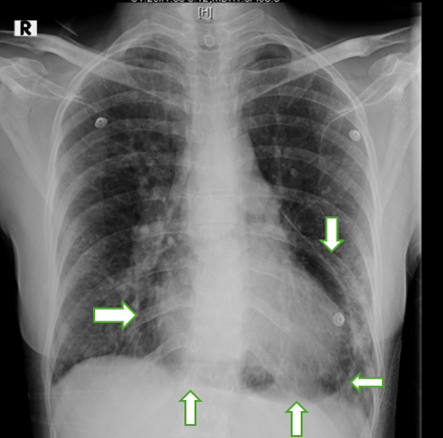
Figure 3: Chest radiograph showing a lucency around the cardiac silhouette with ‘continuous diaphragm sign' (white arrow)

Figure 4a & 4b: CT Thorax revealed pneumopericardium (white arrow)
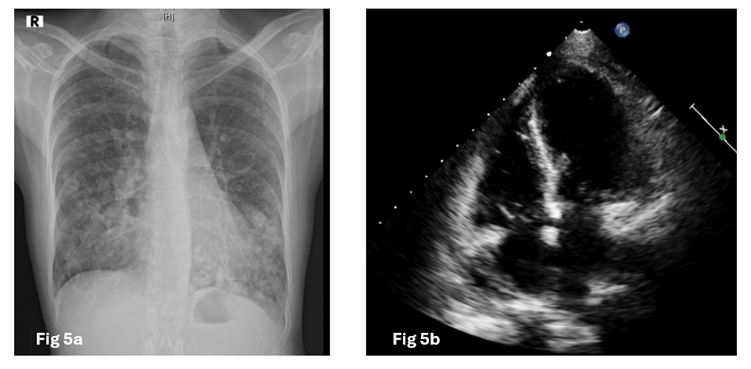
Figure 5a: (Chest radiograph) 5b (Transthoracic echo) showing no signs of pneumopericardium.
Discussion
Pneumopericardium is defined as an accumulation of air-fluid level in the pericardial cavity. It is a rare but can be life-threatening entity. There are multiple causes for development of pneumopericardium such as penetrating or blunt chest trauma, pericardium infections with gas forming organisms, iatrogenic and invasive procedures, abnormal communications such as fistula between the pericardium and hallow organs, or even spontaneously without any underlying cause in healthy adult.[1–3] Iatrogenic pneumopericardium occurring after therapeutic pericardiocentesis is very rare.[4] During pericardiocentesis, pneumopericardium can be caused by direct pleuropericardial connection or reverse air leakage from the catheter.[5]
Clinical manifestations are variable and very unspecific like pain, dyspnea, palpitation. Sometimes patients could be asymptomatic making early detection of the disease before hemodynamic instability a real challenge.[6] Tension pneumopericardium can be fatal. Physical examination may show tachycardia, distended neck veins, and hypotension. Pathognomonic signs such as the mill wheel murmur “bruit de moulin” can be heard as a succession splash and traducing shaking movement of the heart within pericardial cavity on cardiac auscultation.[6] Chest radiographs reveal air as a radiolucent rim separating the pericardium from the heart, called “Continuous diaphragm sign.[7]
TTE findings can show two pathognomic signs: “The air gap sign” traducing a cyclic disappearance of the cardiac shape during systole coinciding with a cycling appearance of air within the pericardium during this phase as the volume of cardiac cavities decreases [8,9]and “The swirling bubbles sign” representing the presence of an air-fluid interface with continuous churning movements in pericardial cavity due to heart activity and which is revealed in echocardiography by several tiny bright echogenic spots in the pericardial sac evoking micro air bubbles[7,10] Chest CT can confirm the diagnosis and is the mainstay of diagnosis of pneumopericardium in obscure cases. It offers further information concerning mechanisms and associate lesions.
Usually, pneumopericardium resolves spontaneously. [2,11] In the presence of acute hemodynamic instability suggesting cardiac tamponade, an emergent pericardiocentesis with hemodynamic monitoring are required to promptly restore hemodynamic stability, followed by pericardial fenestration and drainage[12]
In the case of iatrogenic pneumopericardium following pericardiocentesis for pericardial effusion, a re-pericardiocentesis is indicated if hemodynamic conditions are unstable. Watchful waiting for spontaneous absorption of air under a close monitoring is indicated in the absence of acute and life-threatening tension pneumopericardium.[2]
Iatrogenic pneumopericardium is rarely reported after pericardiocentesis, but it can lead to tension pneumopericardium, which is a life-threatening condition. Physicians should be aware of this serious complication of pericardiocentesis and take extra precautions.
Conclusion
Iatrogenic pneumopericardium caused by pericardiocentesis is very rare. However, in case of hemodynamic worsening despite complete evacuation of a hemodynamically significant pericardial effusion, it should be considered in the differential diagnosis because immediate recognition and treatment are crucial. Surgery is preferred in cases of direct breach between the pericardial cavity and hollow organs apart from lungs to close channel between pericardium and air.
References
- Lee YJ, Jin SW, Jang SH, Jang YS, Lee EK, Kim YJ, et al. (2001). A case of spontaneous pneumomediastinum and pneumopericardium in a young adult. Korean J Intern Med. Sep 1;16(3):205–209.
View at Publisher | View at Google Scholar - Iskander S, Amar H, Audrey B, Fabien D. (2016). Pneumopericardium: A Rare Complication of Pericardiocentesis. J Cardiovasc Ultrasound. Mar;24(1):55–59.
View at Publisher | View at Google Scholar - Hymes WA, Itani KM, Wall MJ, Granchi TS, Mattox KL. (1994). Delayed tension pneumopericardium after thoracotomy for penetrating chest trauma. Ann Thorac Surg. Jun 1;57(6):1658–1660.
View at Publisher | View at Google Scholar - Yuce M, Sari I, Davutoglu V, Ozer O, Usalan C. (2010). Bubbles around the Heart: Pneumopericardium 10 Days after Pericardiocentesis. Echocardiography. 27(9):E115–6.
View at Publisher | View at Google Scholar - Mullens W, Dupont M, De Raedt H. (2007). Pneumopericardium after pericardiocentesis. Int J Cardiol. May;118(2):e57.
View at Publisher | View at Google Scholar - Continuous left hemidiaphragm sign revisited: a case of spontaneous pneumopericardium and literature review - PubMed [Internet]. [cited 2024 May 22]. Available from: https://pubmed.ncbi.nlm.nih.gov/12231618/
View at Publisher | View at Google Scholar - Bejvan SM, Godwin JD. (1996). Pneumomediastinum: old signs and new signs. AJR Am J Roentgenol. May;166(5):1041–8.
View at Publisher | View at Google Scholar - Kerut EK, Hannawalt C, Everson CT, Nanda NC. (2014). The air gap sign. Echocardiogr Mt Kisco N. Mar;31(3):400–401.
View at Publisher | View at Google Scholar - Reid CL, Chandraratna AN, Kawanishi D, Bezdek WD, Schatz R, Nanna M, et al. (1983). Echocardiographic detection of pneumomediastinum and pneumopericardium: the air gap sign. J Am Coll Cardiol. Mar;1(3):916–921.
View at Publisher | View at Google Scholar - Antonini-Canterin F, Nicolosi GL, Mascitelli L, Zanuttini D. (1996). Direct demonstration of an air-fluid interface by two-dimensional echocardiography: a new diagnostic sign of hydropneumopericardium. J Am Soc Echocardiogr Off Publ Am Soc Echocardiogr. 9(2):187–189.
View at Publisher | View at Google Scholar - Uluçam MZ. (2013). An extremely rare combination: pneumopericardium, pneumoperitoneum, and subcutanous emphysema-a case report. Cardiol Ther. Jun;2(1):103–110.
View at Publisher | View at Google Scholar - Cummings RG, Wesly RL, Adams DH, Lowe JE. (1984). Pneumopericardium resulting in cardiac tamponade. Ann Thorac Surg. Jun;37(6):511–518.
View at Publisher | View at Google Scholar
