

Research Article | DOI: https://doi.org/10.31579/2835-8147/073
Physiology of Menstruation
1Riggs Pharmaceuticals Department of Pharmacy University of Karachi Pakistan.
2Assistant Professor Dow University of Health Sciences Karachi Pakistan.
3Associate Professor, Department of Pathology Dow University of Health Sciences, Karachi, Pakistan.
4Pharmaceutical Inc OPJS University Rajasthan India.
*Corresponding Author: Rehan Haider, Riggs Pharmaceuticals Department of Pharmacy University of Karachi Pakistan
Citation: Rehan Haider, Zameer Ahmed, Sambreen Zameer, Geetha K. Das, (2025), Physiology of Menstruation, Clinics in Nursing, 4(1); DOI:10.31579/2835-8147/073
Copyright: © 2025, Rehan Haider. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 December 2024 | Accepted: 06 January 2025 | Published: 13 January 2025
Keywords: physiology of period; period, hypothalamic-pituitary-ovarian pivot; hormonal regulation, generative energy; endometrial changes; dysmenorrhea; menorrhagia; amenorrhea
Abstract
The plant structure of the period is a complex interaction of hormonal, vascular, and uterine changes that ensure generative well-being. Menstruation happens as contained the period, a monthly hormonal era that prepares the female physique for potential gestation. The process includes the hypothalamic-pituitary-ovarian stalk, which organizes the release of gonadotropins, the luteinizing birth control method (LH), and the smallest living organism-exciting birth control method (FSH). These hormones organize the development and development of ovarian follicles and the repetitive setting of the endometrium to construct a cordial environment for information that is designed to mislead or persuade.
When implantation does not happen, hormonal levels, specifically estrogen, and progesterone, decline, superior to the breakdown of the endometrial interlining and allure banishing through the vaginal waterway. This process, famous as menstruation, is followed by changes in vascular blockage, fabric renovation, and invulnerable responses to assert equilibrium and act in advance of the after phase. Factors such as age, stress, energy environments, and behavior can influence the evenness and traits of menstruation. Understanding the study of animals of the period is important for labeling irregularities to a degree dysmenorrhea, menorrhagia, and amenorrhea, which can display fundamental strength issues. Advances in generative endocrinology and microscopic biology touch determine visions into this lively process, permissive better diagnostic and healing approaches to menstrual strength.
Introduction
Definition
Menstruation is the weekly extorting from the uterus that comes out through the vulva for 4–7 days all 28–32 days all the while the generative history of a she, accompanying an average deficit of about 20–60 ml of ancestry. It has been noticed that about two-the third step in the baseball diamond of adult women have period unending from 21–35 days. The sane period is a fixedly the matched phase of stimulatory and inhibitory belongings that influence the release of a sole mature oocyte from a pool of a great number of millenaries of earliest oocytes. An assortment of determinants enhance the rule concerning this process containing hormones and paracrine and autocrine determinants that are still being recognized. For a better understanding, of the study of the animal period, which is contingent on complex neurohormonal pathways, can be detached into endocrine, ovarian, and uterine eras.
The Endocrine Cycle
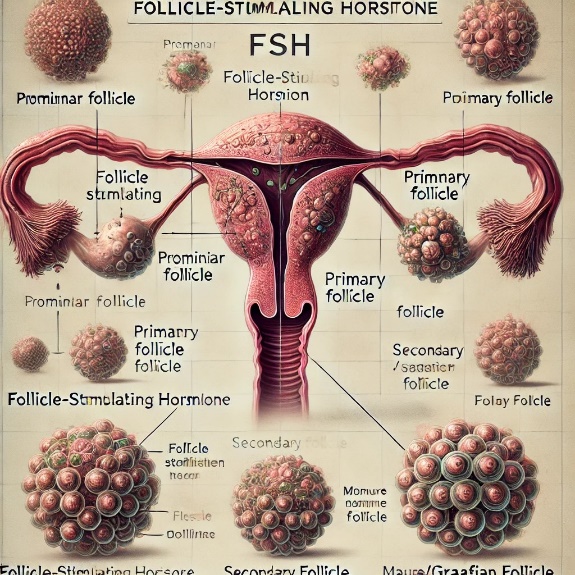
The female period is determined by a complex interplay of hormones. The ruling hormones complicated in the period are gonadotropin-delivering birth control method (GnRH), gonadotropin hormones namely. Blood vessel-exciting birth control method (FSH) and luteinizing birth control method (LH), estrogen, and progesterone. GnRH is emitted in pulses for one hypothalamus. FSH and LH (gonadotropins) are hidden for one beginning flap of the pituitary gland, and estrogen and progestin are emitted at the level of the ovary. GnRH excites the release of LH and FSH from the beginning pituitary that in proper sequence, excites the release of estrogen and progestin at the level of the ovary. LH induces androgen combined by theca containers. This androgen is moved into granulosa containers; and under the influence of FSH, this androgen is convinced into estrogens by activation of aromatase and p450 enzymes. In inmates accompanying overdone androgen result, sane follicular development is shy and the result is polycystic ovarian disease from uneven eras, hyperandrogenism and unproductiveness. LH provokes increase, distinction, and release of follicular theca containers; and increases LH receptors on granulosa cells. FSH simplifies the incidence of 15–20 follicles each period (Fig. 8.14). FSH discharge is the topmost and ultimate fault-finding all the while the first temporal length of the event or entity's existence of the follicular stage of the menstrual era.
It stimulates estradiol discharge by upregulating the discharge of androgens for one theca externa and by encouraging the aromatase catalyst receptors on granulosa cells. FSH further induces the verbalization of FSH receptors by follicles. As estradiol levels increase bashed of FSH, estradiol Downregulates the discharge of FSH. Estrogen levels peak towards the completion of the follicular state of the period. At this crucial moment, estrogen utilizes a beneficial response on LH produces a moving preovulatory LH surge. This LH surge is necessary for ovulation. Under the influence of LH, the basic oocyte enters the ending stage of the first meiotic separation and divides into a subordinate oocyte and the first opposite carcass. After ovulation, the empty smallest living organism is described as mass luteum, (Fig. 8.15A) that produces extreme levels of progesterone accompanying tinier amounts of estrogen discharge. High progesterone levels expend negative response on GnRH and afterward, GnRH beat commonness decreases. This leads to an appearance of FSH and LH levels. In the lack of implantation, the entirety luteum degenerates to form the substance albicans (Fig. 8.16) causing a decline in two together estrogen and progesterone levels. This enters the estrogen and progesterone aggregation is followed by period. After retraction grieving, the early occurrences of the follicular development is begun by a rise in FSH levels at the first era of the phase that happens on account of a decrease in progesterone and estrogen levels at the end of the prior era and the after the expulsion of the hindrance of FSH by these ovarian hormones. The music of the period depends on the hypothalamic-pituitary-ovarian point around which something revolves, since the amount of ancestry deficit is weak on the condition of the uterus.
Hormonal Regulation
Hypothalamus
Gonadotropin-delivering birth control method (GnRH), a neurohormone is a decapeptide hidden for one peptidergic neuron in the middle importance and bent-core in the hypothalamus and brought to the prior pituitary for one opening containers. As noticed above, it is hidden in a pulsatile method.
Pituitary
The gonadotropins, FSH, and LH are presented apiece beginning pituitary containers. Anterior pituitary has two types of secretory containers, acidophilic and basophilic containers (established hematoxylin and eosin stains). Gonadotropins are hidden in one basophilic container. Both the gonadotropins are glycoproteins.
Ovary
Ovarian function happens in a repetitive form and has two phases—the follicular proliferative aspect and the secretory luteal state. Sex hormones like estrogen, progesterone, few number of androgens and peptides like inhibin and activing are announced from the ovary and are the reason for rational period.
Uterus
The uterine era has two phases—the proliferative aspect and the secretory step. This phase is dependent on the ovarian hormones.
Ovarian Cycle
In the beginning, skilled are about 2 heaps earliest follicles in the ovary; and by adolescence, these decrease to about 300,000 in number on account of willing degeneration of follicles. In the generative existence, about 400 follicles ovulate; and by midlife depression, the ovary will have a thick stromal fabric accompanying only a few follicles surplus.
Follicular Phase
Folliculogenesis
After the onset of adolescence, the middle from two points 15 and 20 earliest follicles adds up to basic follicles accompanying each ovarian era. The follicular time of the menstrual cycle starts from the first epoch of the period as far as ovulation. The basic aim of the follicular chapter is to cultivate a practicable blood vessel worthy of having ovulation. In the beginning, the smallest living organism consists of a basic oocyte between a coating of cuboidal or tubular granulosa containers. Zona pellucida is a dense coating composed of glycoproteins and acid proteoglycans that is present betwixt the oocyte and granulosa containers.
As the blood vessel evolves from the earliest smallest living organism into a primary unilaminar smallest living organism, the basic oocyte determines its tumor. At this stage of the incident, the stromal containers encircling the follicle, again enhance more sticking out. For an oocyte to evolve correctly, it must be among a tier of granulosa cells. Gap connections are present between the oocyte and encircling granulosa containers. Transportation of amino acids, nucleotides, and lipid forerunners into the oocyte takes place from these break connections. Growth factors to a degree equipment-ligand and GDF-9 is too necessary for oocyte tumors. Once oocyte tumor is achieved, the granulosa cells escalate to form diversified tiers. The blood vessel at this stage is famous as a basic multilaminar smallest living organism. This step of follicular development is helpless upon FSH. FSH induces the conception of granulosa containers and increases the number of FSH receptors on each granulosa container, accordingly emphasizing its belongings. The theca cells encircling the blood vessel change into two tiers—the theca interna and the theca externa. It is now grasped that LH drives the distinction of theca cells. The basic multilaminar blood vessel evolves further to form the Graafian smallest living organism (Fig. 10.1). The Graafian smallest living organism is from an abundant, fluid-filled cavity, and an eccentric oocyte. The granulosa containers can also be detached into two groups—the zona granulosa which is a thin tier near the periphery of the blood vessel and the halo radiata that encloses the oocyte. The oocyte suffers the first meiotic breach, bestowing rise to a subordinate oocyte and the first opposed bulk. The subordinate oocyte is immediately seized in metaphase of the second meiotic split and remnants like that until propagation.
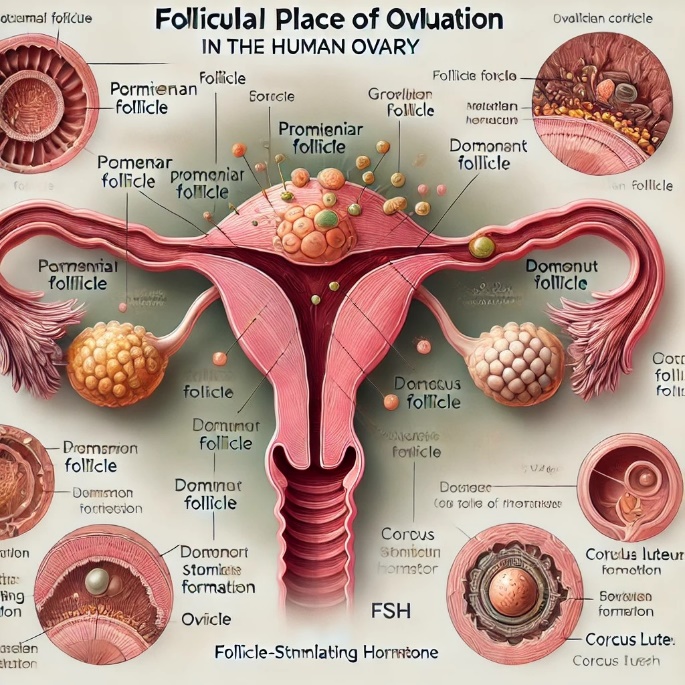
Figure 10.1: Follicular Place of ovulation
As said earlier, the first meiotic split performs to be begun by LH pursuing granulosa containers, even though the exact system of operation is secret. It is supposed that satire levels prevent the formation of cells by dividing the oocyte. In the lack of LH, cAMP is moved from the granulosa containers into the oocyte. It is theorized that LH blocks cAMP transport into the oocyte, accordingly killing restriction of the formation of cells by dividing and admitting the formation of cells by dividing to pass. Oocytes further sustain cytoplasmic development, an order of changes in protein combination and construction that prepares the oocytes for embryogenesis in the occurrence of breeding. The Graafian smallest living organism shows the ending stage of follicular growth before ovulation. LH surge is necessary for ovulation: Shortly before ovulation, the blood vessel swells and expands a shame (feeble-throw point) at the outskirts of the ovary. At ovulation, the same ruptures, issuing the subordinate oocyte and halo radiata into the peritoneal crater expected distracted apiece fallopian hose. The zona granulosa and theca containers wait in the ovary and add up to the staple luteum. The entire luteum produces progesterone and, as long as of procreation, specifies the necessary progesterone just before the amniotic sac is working. In the omission of fertilization, the extent of a being's life of compilation luteum is 14 days. If propagation and after the opinion of blastocyst does not happen, the body of the text luteum goes through apoptosis; and following in position or time various months, enhances the staple albicans, a silvery scar.To a rational degree, individual blood vessel develops into the a main smallest living organism, appropriated for ovulation, while the surplus follicles go through atresia. It is no secret in what way or manner the main blood vessel is picked; still, it has been noticed that the main smallest living organism forever means a plethora of FSH receptors.
Folliculogenesis
Early Follicular Phase
The folliculogenesis starts as the period ceases and the level of two together the gonadotropins (FSH and LH) is depressed. FSH controls follicular distinction and tumor. The earliest smallest living organism resides in an oocyte and an alone coat with metallic material pivot-formed containers famous as granulosa containers. As follicles mature, the diameter of the oocyte increases, and the shape of the granulosa containers changes to cuboids. With the duplication of cuboidal granulosa containers, the earliest smallest living organism enhances the basic smallest living organism. In the basic blood vessel, the granulosa containers are divided by a cellar sheet from the stromal containers that change into theca containers. As the blood vessel evolves, a fluid-suffused crater performs inside that holds two peptides— inhibin and activin.
Both FSH and local estrogen influence the increase of granulosa containers, which increases the estrogen result. This causes success in the proliferative change in the endometrium. By having five of something epochs, the FSH level reaches its peak, and an excerpt of the main blood vessel is certain by epochs 5 to 7. By era 7, the estrogen level starts climbing. The rise in FSH causes a rise in inhibin and this restrains the FSH. This rise in estrogen and inhibin result helps in tumor and development of the main blood vessel.
Midfollicular Phase
At this time, the raised level of estrogen and inhibin causes about the negative response on pituitary FSH and a definite response on pituitary LH.
Late Follicular Phase
There is a creeping rise in LH; and this raised level ahead accompanying the local estrogen results in the smallest living organism, influencing the granulosa containers to produce few progesterone. Sufficient estrogen level induces an LH surge that itself causes a drop in estrogen level. The peak estrogen level is visualized 48 hours before ovulation and LH peak happens about 24–36 hours before ovulation. With individual blood vessel flattering main, atresia starts in the rest of the failing earliest follicles. With the LH surge, progesterone level persists to rise and this has a negative response on FSH, though inhibin has a negative response on FSH has no specific effect on LH. The fall in FSH causes success a decline in the level of inhibin and a rise in the peptide activin of a preovulatory smallest living organism (Graafian blood vessel).
Ovulation
There is a perforation in the feeble inflated follicular obstruction and a slow release of oocytes happens in addition to the follicular fluid.
Luteal Phase
With the release of an oocyte, the blood vessel is immediately popular as the body of text luteum (Latin: Yellow crowd). It derives allure name from a yellow shade, which starts accumulating in the preovulatory stage. The luteal state starts from ovulation and ends for 14 days. In this stage, the progesterone level rises as androgen results in the theca containers of the failing blood vessels, that are approaching atresia; and these androgens take aromatized apiece granulosa containers in the follicles to progesterone. Some amount of inhibin is more freed. A rise in progesterone and estrogen causes success in the secretory stage of the endometrium. Corpus luteum (CL) remnants mature from 19 to 26 days. The means of deterioration of CL is secret till immediately. This results in a fall of progesterone and estrogen and a period takes place. Fall in these two hormones and still of inhibin results in a helpful response means and starts the hypothalamus to release GnRH for the follicular aspect of the next period.
Uterine Cycle
Cyclical changes in the endometrium form the endometrium for principle, as long as of breeding. However, the period starts with the deficiency of breeding. The endometrium is detachedinto two tiers. The superior functional coating meets withchanges during the whole of the period and is dropped all along the period, while the lower basalis tier debris is perpetual all the while the period; and from it regenerates the functional coating each period. The uterine endometrial era may be detached into three aspects—proliferative, secretory, and menstrual states. The conception starts from the completion of the period just before ovulation. Increasing levels of estrogen encourage the conception of functionalis from stem containers of basalis. There is the conception of endometrial glands and stromal combinational fabric. Endometrial glands are lengthened accompanying narrow lumens and their epithelial containers hold little oxygen. Glycogen, nevertheless, is not hidden all along the follicular step. Spiral channels lengthen and span the time of endometrium (Figure 10.2 and 10.3). The secretory development starts (Figure. 10.4) at ovulation and ends (Figure 10.5 and 10.6) as far as the menstrual aspect of the next phase. At the origin of luteal time, progesterone induces the endometrial glands to emit organic compounds composed of carbon, muck, and added meanings. These glands enhance indirectly and have abundant lumens on account of raised secretory action. The spiral channels longer into the detail tier of the endometrium.
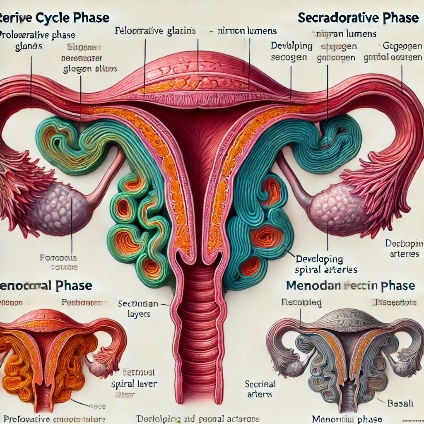
Figure 10.2: Proliferative endometrium (Dr Yadav, RML Hospital)
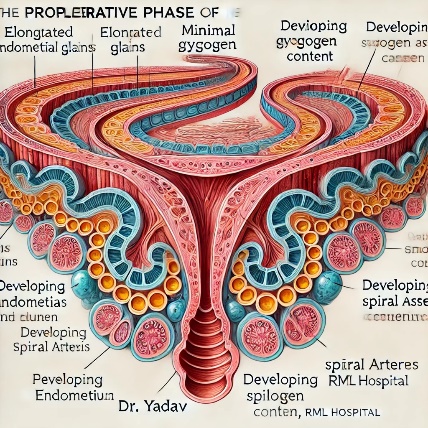
Figure 10.3: Proliferative endometrium (Dr Yadav, RML Hospital)
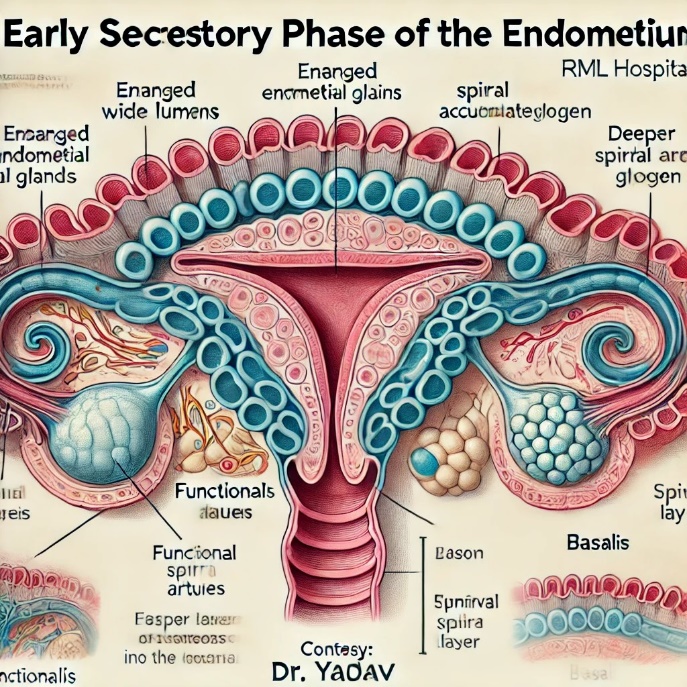
Figure 10.4: Early secretory endometrium (Dr Yadav, RML Hospital
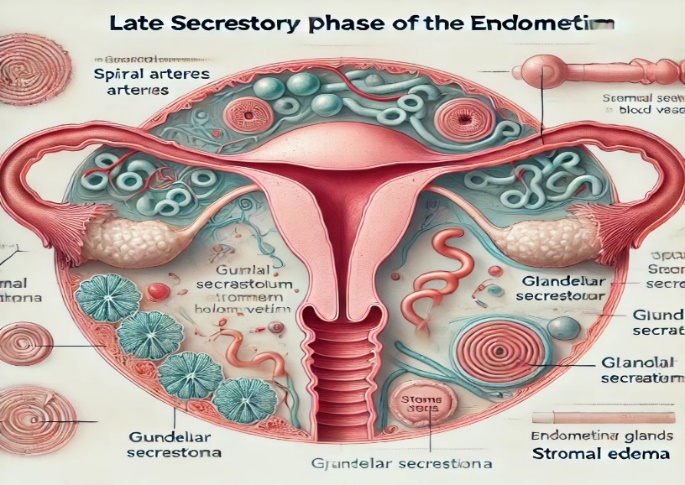
Figure 10.5: Late secretory endometrium (Dr Yadav, RML Hospital)
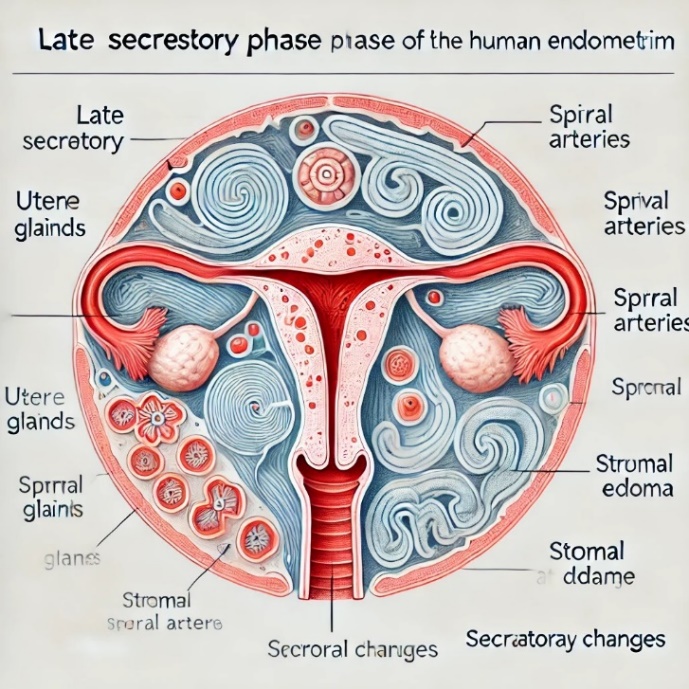
Figure 10.6: Late secretory endometrium (Dr Yadav, RML Hospital) in the deficiency of breeding per day 23 of the menstrual phase, the mass luteum starts to degenerate, and as a consequence ovarian birth control method levels decrease.
The menstrual stage starts as the spiral channels rupture subordinate to blood deficiency, issuing ancestry into the uterine crater, and the apoptosed endometrium is sloughed off. This consistently ends for 3 to 5 days. During this ending, the functional coating of the endometrium is entirely yielded. Arterial and unmodified blood, bits of endometrial stroma, and glands are present in the menstrual flow. Bleeding happens as blood vessel extorting and venous bleeding and is created by the withdrawal of estrogen and progesterone support to the endometrium. As estrogen and progesterone levels decrease, the endometrium goes through a loop.
Uterine Endometrial Cycle (Timing in Table 10.1) a. Proliferative or follicular aspect: Estradiol (from the ovarian follicles) causes proliferative change in the uterine endometrium (epoch 7–14). All the endometrial tissues enhance density.
b. Secretory or luteal stage: Progesterone (from the bulk luteum) causes secretory changes in the endometrium (era 15–26) to sustain fertilized female reproductive cells for sinking.
The survey of the period is likely in (Fig. 10.7).
Ovulation and Fertilization
The timing of ovulation is crucial for favorable understanding.The arable ending starts about 4–5 days before ovulation and ends about 24–48 hours following in position or time. This is because the old age of semen is nearly 3–4 days, and of the cell is reasonable for
Time Interval of Events | Events | Days |
|---|---|---|
Estrogen secretion | 7 – 14 | |
Onset of LH surge | 12 – 15 | |
Estrogen peak | 11 – 14 | |
LH peak | 12 – 15 | |
Progesterone rise | 15 – 26 |
Table 10.1: Showing Events at Different Parts of the Cycle:
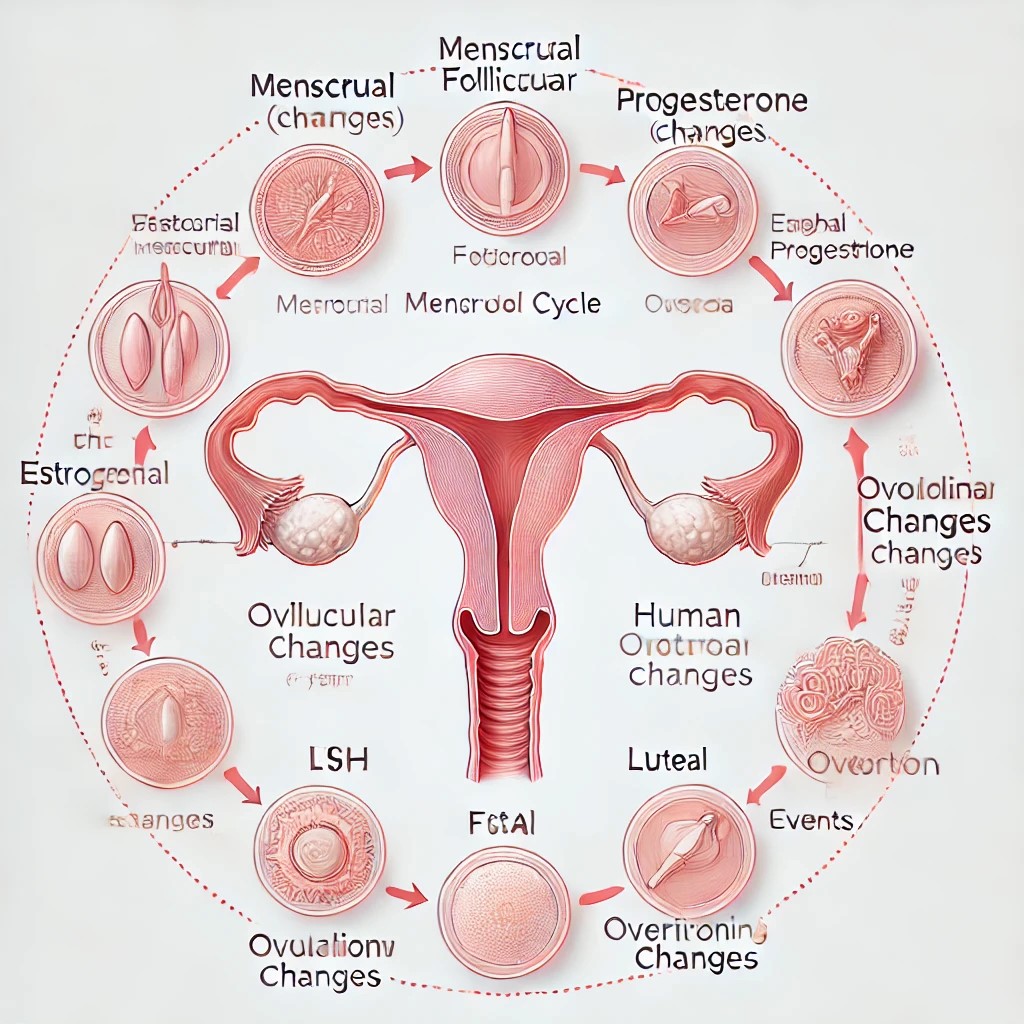
Figure 10.7: Overview of menstrual cycle
Research Methodology
Study Design:
This study adopts an inclusive information review approach, combining verdicts from peer-reviewed journals, dispassionate studies, and textbooks on the menstrual research of animals.
Data Sources:
The basic beginnings involve PubMed, Scopus, and Web of Science databases, directed on articles written inside the last ten of something.
Procedure:
Key processes to a degree hormonal management, endometrial changes, and ovarian eras were resolved. Data were classified apiece menstrual developments: menstrual, follicular, ovulation, and luteal.
Instruments and Techniques:
Hormonal levels were calculated through dispassionate assays assigned to source studies, and histological data of the endometrium were resolved to story verdicts.
Ethical Considerations:
As this is a review study, the moral go-ahead was optional; however, all assigned to source studies hewed to moral research principles.
Discussion
The corporal processes of the period explain a carefully brought into harmony hormonal interaction:
Hormonal Regulation: The hypothalamic-pituitary-ovarian pivot rules menstrual cyclicity. The beat of estrogen and progesterone detracts from ovulatory eras and endometrial development.
Endometrial Dynamics: The periodic changes in the uterine interlining highlight the significance of hormonal influence in fitting the uterus for potential opinion.
Clinical Relevance: Insights into the menstrual study of animals can aid in diagnosing and considering environments to a degree amenorrhea, dysmenorrhea, and weird uterine grieving.
Limitations
The study depends on subordinate data that concede the possibility limit the outlook of direct remarks. Further practical studies are urged to extend the understanding of hormonal vacillations in diverse communities.
Implications for Practice
Healthcare providers can use these verdicts to better instruction on menstrual strength and control disorders efficiently. Public health drives stress the significance of menstrual proficiency.
Conclusion
The study of plants of the period is a complex but well-organized process including hormonal organizing, ovarian exercise, and endometrial renovation. This study specifies a detailed understanding of these machines, laying an endowment for trying menstrual fitness issues and advancing generative comfort. Future research bears devote effort to something the impact of material and behavior determinants on menstrual plant structure.
Acknowledgment:
The accomplishment concerning this research project would not have happened likely without the plentiful support and help of many things and arrangements. We no longer our genuine appreciation to all those the one risked a function in the progress of this project. I herewith acknowledge that:
I have no economic or added individual interests, straightforwardly or obliquely, in some matter that conceivably influence or bias my trustworthiness as a journalist concerning this study
Conflicts of Interest:
The authors declare that they have no conflicts of interest.
Conflict-of-Interest Disclosure Statement
We, the authors of the book named “Stem Cells Research, Cloning, and Gene Therapy”, herewith disclose the following:
Dr. Rehan Haider, Ph.D: I disclose no conflict of interest concerning this script.
Dr. Zameer Ahmed, Ph.D: I acknowledge no conflict of interest concerning this book.
Dr. Sambreen Zameer, Ph.D: I acknowledge no conflict of interest concerning this script.
Dr. Geetha Kumari Das, Ph.D: I disclose no conflict of interest concerning this script
Financial Support and Protection:
No external funding for a project was taken to assist with the preparation of this manuscript
References
- Guyton, A. C., Hall, J. E. (2016). Textbook of scientific body structure. Philadelphia, PA: Saunders.
View at Publisher | View at Google Scholar - Barrett, k. E., Barman, S. M., Boitano, S., Brooks, H. L. (2019). Ganong's overview of medical physiology. New York, the Big Apple: McGraw-Hill schooling.
View at Publisher | View at Google Scholar - Kumar, V., Clark, M. (2017). Kumar & Clark's scientific medicinal drug. Philadelphia, PA: Elsevier.
View at Publisher | View at Google Scholar - Strauss, J. F., Barbieri, R. L. (2017). Yen & Jaffe's Reproductive Endocrinology: physiology, Pathophysiology, and medical control. Philadelphia, PA: Elsevier.
View at Publisher | View at Google Scholar - Speroff, L., Fritz, M. A. (2017). Scientific Gynecologic Endocrinology and Infertility. Philadelphia, PA: Wolters Kluwer.
View at Publisher | View at Google Scholar - Sherwood, L. (2017). Human body structure: From Cells to systems. Boston, MA: Cengage studying.
View at Publisher | View at Google Scholar - Barrett, k. E. (2019). Ganong's review of scientific physiology. The Big Apple, New York: McGraw-Hill education.
View at Publisher | View at Google Scholar - Johnson, M. H., Everitt, B. J. (2017). Vital duplicate. Chichester, United Kingdom: Wiley-Blackwell.Goodman, H. M. (2018). fundamental clinical Endocrinology. Big Apple, NY: McGraw-Hill training.
View at Publisher | View at Google Scholar - Griffin, J. E., Ojeda, S. R. (2019). Textbook of Endocrine body structure. The big apple, New York: Oxford University Press.
View at Publisher | View at Google Scholar - Melmed, S., Polonsky, k. S. (2019). Williams Textbook of Endocrinology. Philadelphia, PA: Elsevier.
View at Publisher | View at Google Scholar - Molina, P. E. (2019). Endocrine body structure. The Big Apple, New York: McGraw-Hill training.
View at Publisher | View at Google Scholar - Plant, T. M., Zeleznik, A. J. (2019). Knobil and Neill's body structure of reproduction. San Diego, CA: Academic Press.
View at Publisher | View at Google Scholar - Strauss, J. F., Williams, C. J. (2019). Reproductive Endocrinology. Philadelphia, PA: Elsevier.Thakker, R. V. (2019). Genetic Endocrinology. New York, NY: CRC Press.
View at Publisher | View at Google Scholar - Wilson, J. D., Foster, D. W. (2019). Williams Textbook of Endocrinology. Philadelphia, PA: Elsevier.
View at Publisher | View at Google Scholar - Yen, S. S. C., Jaffe, R. B. (2019). Reproductive Endocrinology: body structure, Pathophysiology, and scientific management. Philadelphia, PA: Elsevier. Zipf, W. B. (2019). Pediatric Endocrinology. Big apple, New York: Springer.
View at Publisher | View at Google Scholar
