

Research Article | DOI: https://doi.org/10.31579/2835-8147/093
Patient-Level Stroke Outcomes Following Linkage of a Statewide Stroke Registry to Administrative Claims Data
- Raed Hailat *
- Michael P Thompson
- Adrienne Nickles
- J. Adam Oostema
- J. Adam Oostema
- Mathew J Reeves
1Michigan State University, Department of Epidemiology and Biostatistics.
2University of Michigan, Department of Cardiac Surgery.
3Michigan Department of Health and Human Services.
4Michigan State University, Department of Emergency Medicine.
5Michigan State University, Department of Epidemiology and Biostatistics.
*Corresponding Author: 10.31579/2835-8147/093
Citation: Raed Hailat, Michael P Thompson, Adrienne Nickles, J. Adam Oostema, J. Adam Oostema, et al, (2025), Patient-Level Stroke Outcomes Following Linkage of a Statewide Stroke Registry to Administrative Claims Data, Clinics in Nursing, 4(6); DOI:10.31579/2835-8147/093.
Copyright: © 2025, Raed Hailat. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 16 October 2025 | Accepted: 31 October 2025 | Published: 13 November 2025
Keywords: alzheimer’s disease; theta burst stimulation; neuromodulation
Abstract
Background:
Collection of patient-level outcomes data following hospital discharge is challenging for stroke registries. Data linkage to administrative claims data is a potential solution to obtain outcomes data. We aimed to generate data on 30-day, 90-day and 1-year outcome events following hospitalization for stroke using linked data in Michigan.
Methods:
We probabilistically linked clinical data from a 5-year cohort (2016-2020) of all index acute stroke discharges (ICD-10 I61-I63) from 31 hospitals participating in Michigan’s Acute Stroke program (MiSP) to a representative statewide multi-payer claims database. We used the linked data to generate data on 30-day, 90-day, and 1-year event rates including hospital readmissions, stroke recurrence, post-acute care services (i.e., facility-based rehabilitation and home health), and out-patient visits. Mortality data was only available for Medicare fee-for- service beneficiaries. Outcomes were stratified by age, race, stroke type, and stroke severity.
Results:
Of the 46,330 MiSP stroke discharges, 23,918 (51.6%) were linked to the claims database. Readmission and stroke recurrence rates were 14.1% and 3.3%, respectively, at 30 days, increasing to 42.2% and 8.3% at one year. By 30 days about a quarter of subjects had used facility-based rehab and another quarter had used home health; home health utilization increased to 44.7% by one year. At all time points Black patients had significantly higher readmission rates compared to whites, but higher stroke recurrence rates were only observed at the 1-year mark. At 30 days, utilization of post-acute care services did not differ by race, but utilization rates were significantly higher in Blacks at 90 days and one year. In contrast utilization of outpatient services was significantly higher among White patients at all time points.
Conclusions:
Linkage between acute stroke registry and claims data provides an important source of surveillance data for stroke outcomes up to 1-year post discharge. This data allows for real-time monitoring of healthcare outcomes and potentially leads to interventions to improve stroke care.
Introduction
The large volume of data collected in the national Get With The Guideline-Stroke (GWTG-S) program–now exceeding 9 million stroke discharges from more than 2,600 hospitals has allowed for the detailed examination of trends in quality of stroke care and outcomes up to the point of hospital discharge.1, 2 Yet, for stroke patients the majority of functional recovery and return to community participation occurs after hospital discharge.3 Collection of outcomes data following hospital discharge has been difficult for large stroke registries to sustain, but a potentially feasible and sustainable way to track patient outcomes is through data linkage to administrative databases that can provide information on patient outcomes including mortality, readmissions, recurrence and post-acute care utilization.4-6 Data linkage can serve an important surveillance function by providing real-time data on cardiovascular disease that can be used to track patient outcomes and improve population health.7 Therefore, using linked data from a 5-year cohort of acute stroke discharges from a representative stroke registry in Michigan, we aimed to generate descriptive data on 30-day, 90- day and 1-year outcome event rates and stratify the data by age, race, stroke type, and stroke severity.
Methods
This report adheres to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.8 The study was based on 5-year cohort of prospectively collected data of index acute ischemic and hemorrhagic stroke discharges (ICD-10 I61-I63) collected between January 2016 and December 2020 by 31 hospitals participating in the Michigan Stroke Program (MiSP). The MiSP data was probabilistically linked to a representative statewide claims database (Michigan Value Collaborative [MVC]) that included Medicare fee-for service (FFS) and private insurer data, using date of birth, sex, admission date, discharge date, and hospital ID. Both MiSP and MVC datasets were deidentified. Clinical data including demographics (age, race, sex), stroke type (ischemic and hemorrhagic), discharge disposition, and stroke severity (National Institute of Health Stroke Scale [NIHSS]) were based on MiSP data. The MVC dataset included all post-acute health services claims submitted to the insurance provider during the 12-month period following hospital discharge for the index event. These services include services (in- patient rehabilitation (IRF), skilled nursing facility (SNF), home health care (HHC), outpatient medical visits (OP), and hospital readmissions. Mortality data were only available for FFS beneficiaries. More information on study databases is available in the supplement. The index stroke events were defined as the patient’s first-stroke discharge during the 5-year study period. We excluded patients that died during hospitalization or were discharged to hospice care or against medical advice (Figure S1 Supplement).The claims data were used to calculate 30-day, 90-day and 1-year event rates of all-cause hospital readmissions- defined as any subsequent hospitalization within one year of the discharge date of the index event, stroke recurrence- defined as any subsequent stroke-related hospital discharge occurring within one year of the index stroke, use of post-acute care services (i.e., IRF, SNF, and HHC), and use of OP visits- defined as any outpatient claim for primary or specialty care. Home time- defined as post discharge time spent alive and out of an inpatient care setting (i.e., hospital, IRF, SNF, or Long term acute care hospital), was only calculated for FFS beneficiaries since mortality data were available for this group.9 One year Kaplan-Meier curves for mortality, all-cause readmission, and stroke recurrence were generated. We stratified outcomes according to age, race, stroke type and severity. Data analysis was done using SAS software v9.4 (Cary, NC).
Results
Data linkage was conducted between the 46,330 MiSP and 30,685 MVC acute stroke discharges and resulted in 19,382 matched index strokes. The final linked cohort were predominantly older (>65 years, 78.5%), white (79.7%), female (52.2%), and insured by Medicare FFS (62.9%) (Table 1).
Variable | Value | Distribution N (%) |
Age category | <65> | 4,167 (21.5) |
65-74 | 5,672 (29.2) | |
75-84 | 5,589 (28.8) | |
>=85 | 3,954 (20.4) | |
Race | White | 15,457 (79.7) |
Black | 2,833 (14.6) | |
Other* | 255 (1.3) | |
Not documented | 837 (4.3) | |
Latino ethnicity | No/Unable to determine | 18,665 (96.3) |
Yes | 717 (3.7) | |
Sex | Male | 9,265 (47.8) |
Female | 10,117 (52.2) | |
Insurance | Private (Preferred Provider Organization (PPO)and Health Maintenance Organization (HMO)) | 3,140 (16.2) |
Medicare Advantage (MA) | 4,051 (20.9) | |
Medicare FeeFor Service (FFS) | 12,191 (62.9) | |
Stroke type | Ischemic | 16,921 (87.3) |
| Hemorrhagic | 2,461 (12.7) |
Admission NIHSS | 0 | 2,985 (15.4) |
| 1-4 | 7,937 (41.0) |
| 5-15 | 4,955 (25.6) |
| 16-20 | 830 (4.3) |
| >20 | 733 (3.8) |
| Not documented | 1,942 (10.0) |
Discharge disposition | Home | 9,710 (50.1) |
| Skilled Nursing Facility (SNF) | 4,821 (24.9) |
| Inpatient Rehabilitation Facility (IRF) | 4,148 (21.4) |
| Long Term Care Hospital (LTCH) | 122 (0.6) |
| Not determined | 581 (3.0) |
Table 1: Descriptive characteristics of a 5-year cohort of linked index stroke events (N=19,382).
The majority of index hospitalizations were ischemic stroke (87.3%), with a predominance of minor stroke (NIHSS <5> Outcome (N=19,382)* 30-day event rate n (%) 90-day event rate n (%) 1-year event rate n (%) All cause readmission 2,724(14.1) 4,833 (24.9) 8,169(42.2) Stroke recurrence** 641 (3.3) 991 (5.1) 1,614(8.3) Inpatient rehabilitation facility utilization 4,822(24.9) 4,946 (25.5) 5,171(26.7) Skilled nursingfacility utilization 5,449(28.1) 6,049 (31.2) 6,765(34.9) Home health utilization 5,336(27.5) 7,436 (38.4) 8,659(44.7) Outpatient visit*** 8,999(46.4) 13,720 (70.8) 16,539 (85.3) Mortality^ 486 (4.0) 1,109 (9.1) 2,416(19.8) Home time-Median days (IQR)** 22.0 (26.0) 79.0 (40.0) 347.0 (94.0)
Table 2: Thirty-day, 90-day, and 1-year post stroke discharge outcome event rates among a 5-year cohort of 19,382 linked stroke events.

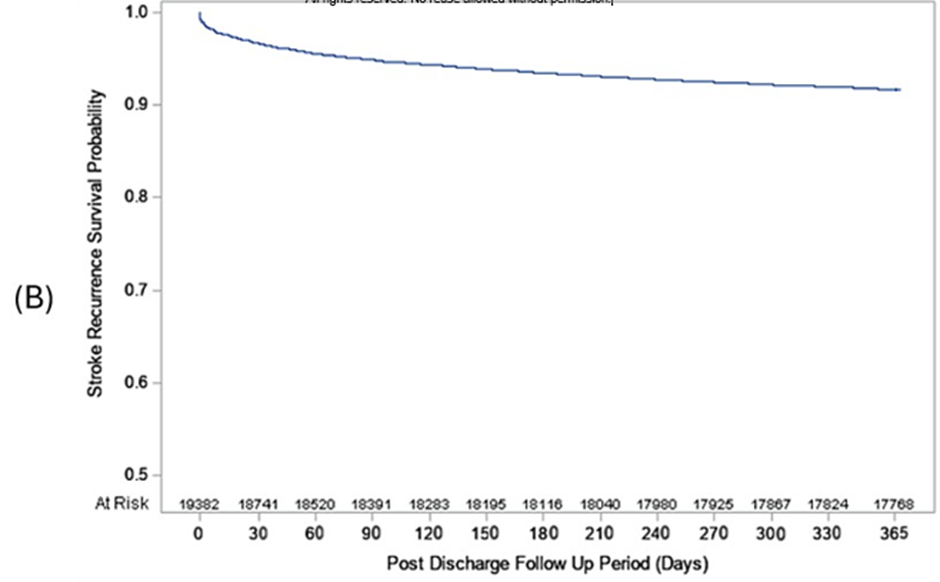
Only 3.3% of the linked population had a recurrent stroke event (defined as a hospital readmission with a primary discharge diagnosis of stroke) within 30 days; this increased to 5.1% at 90 days and to8.3% at one year (Table 2 and Figure 1B).
In terms of use of post-acute services, 24.9%, 28.1%, 27.5% of the linked cohort utilized IRF, SNF, and HHC within 30 days of hospital discharge, respectively (Table 2). While IRF and SNF utilization rates increased only slightly at 90 days (25.5% and 31.2%, respectively), HHC utilization increased substantially to 38.4% at 90 days and 44.7% by one year (Table 2). By 30 days, 90 days, and one year of follow-up, 46.4%, 70.8%, and 85.3% of the cohort had at least one OP visit, respectively. For the 12,185 Medicare FFS linked index events, mortality rates were 4.0%, 9.1%, and 19.8% at 30 days, 90 days, and one year post discharge, respectively (Table 2 and Figure 1C).

Median home time was 22, 79, and 347 days at 30 days, 90 days, and one year, respectively (Table 2). Compared to the <65 xss=removed xss=removed>
the ≥65 years old group over the entire one year follow up period, but IRF utilization did not differ; OP services were utilized at a higher rate up to 90 days post discharge compared to the <65 xss=removed xss=removed>15) had the highest all-cause readmission rates but stroke recurrence did not differ by severity (Table S4). Utilization of health care services was strongly impacted by stroke severity; IRF and HHC utilization rates were the highest among patients with moderate stroke (NIHSS 5-15), while SNF utilization was highest in patients with severe stroke patient group, and OP utilization was highest among mild stroke (NIHS < 5>
Discussion
We generated descriptive data on 30-day, 90-day and 1-year outcome event rates using linked data from a 5-year cohort of acute stroke discharges from Michigan. Our data fulfills the American Heart Associations call for real time collection and analysis of cardiovascular disease surveillance data which is important to identify at-risk groups, and drive advancements in prevention and treatment strategies, including precision health and policy development.7 The overall stroke outcome event rates generated in this analysis were generally similar to those previously published. Our 30-day and 1-year readmission rates were very similar to those reported by a recent meta-analysis that found pooled 30-day and 1-year all-cause stroke readmission rates of 17.4% and 42.5%, respectively.10 Our 30-day, 90-day, and 1-year stroke recurrence rates were also similar to a report that examined 2017 Medicare FFS cases with ischemic stroke that found 30-day, 90-day, and 1-year recurrence rates of 2.4%, 4.0%, and 7.6%, respectively.11 With respect to health care utilization post hospital discharge, our 30-day utilization rates for IRF were similar but SNF and HHC rates were above what a nationally representative GWTG-S population study conducted between 2003 and 2011 reported on.12 However, the GWTG-S study collected their data at the point of discharge, whereas our data was based on actual claims accrued during the 30 days post discharge period which explains the higher 30-day rates of SNF and HHC utilization. We observed increasing rates of SNF and HHC utilization from 30 days to 90 days which points to the fact that many patients initially discharged without these services end up using them. Regarding OP visits, our rates are similar to utilization rates reported by a nationally representative claims database of commercially insured Americans from 2009 to 2015, where 70.8% of acute stroke patients had a primary care visit within 90 days post discharge.13 The value of obtaining patient outcome data from data linkage has been illustrated by previous studies that have linked the GWTG-S registry to Medicare fee-for-service (FFS) data.14-22 However, these reports do not include stroke patients younger than 65 years or Medicare Advantage beneficiaries which are a rapidly growing population.5, 23-25 Data on post discharge OP medical visits utilization is also very important to track adherence to OP treatment and secondary prevention efforts. Of the remaining outcomes examined, our 30-day, 90-day, and 1-year mortality rates were similar to rates of prior FFS population with minor stroke, where 30-day, 90-day and 1-year all- cause mortality were reported as 3.7%, 7.6%, and 17.2%, respectively.20 The calculated median 90-day and 1-year median home time estimates of 79 and 347 days were similar to prior data report that also used Medicare FFS population (90-day: 79 days; 1-year: 349 days).17 Home time can be used to track stroke recovery post discharge as it is recognized as a valid proxy measure of functional recovery in prior studies.17, 26-30 The ability to stratify the outcomes data by race and stroke severity shed light at the importance of data linkage in enabling these stratifications which are usually not able to be generated from claims data alone. It also emphasizes the important differences in event rates and use of post discharge services across subgroups which is relevant to developing patient specific post discharge follow up plans.31, 32 This study found important difference by age and race. We found as expected that older age groups had higher readmission rates, but it was unexpected to find lower stroke recurrence rates in older subjects. Prior studies of stroke recurrence in the young versus older patients are relatively unusual; the South London Stroke registry reported no difference in stroke recurrence rates between <65>
Acknowledgments
None
Sources of Funding
Supported by American Heart Association grant #909423/Dr. Raed Hailat/2022
Disclosures
Support for the Michigan Value Collaborative is provided by Blue Cross Blue Shield of Michigan as part of the BCBSM Value Partnerships program; however, the opinions, beliefs and viewpoints expressed by the author do not necessarily reflect those of BCBSM or any of its employees.
References
- Reeves MJ, Fonarow GC, Smith EE, et al. Twenty Years of Get With The Guidelines- Stroke: Celebrating Past Successes, Lessons Learned, and Future Challenges. Stroke 2024; 55: 1689-1698. 20240513. DOI: 10.1161/STROKEAHA.124.046527.
View at Publisher | View at Google Scholar - Xian Y, Li S, Jiang T, et al. Twenty Years of Sustained Improvement in Quality of Care and Outcomes for Patients Hospitalized With Stroke or Transient Ischemic Attack: Data From The Get With The Guidelines-Stroke Program. Stroke 2024; 55: 2599-2610. 20241021. DOI: 10.1161/STROKEAHA.124.048174.
View at Publisher | View at Google Scholar - Lee KB, Lim SH, Kim KH, et al. Six-month functional recovery of stroke patients: a multi-time-point study. Int J Rehabil Res 2015; 38: 173-180. 2015/01/21. DOI: 10.1097/MRR.0000000000000108.
View at Publisher | View at Google Scholar - Yu AY, Holodinsky JK, Zerna C, et al. Use and Utility of Administrative Health Data for Stroke Research and Surveillance. Stroke 2016; 47: 1946-1952. 2016/05/14. DOI: 10.1161/STROKEAHA.116.012390.
View at Publisher | View at Google Scholar - Patorno E, Schneeweiss S, George MG, et al. Linking the Paul Coverdell National Acute Stroke Program to commercial claims to establish a framework for real-world longitudinal stroke research. Stroke Vasc Neurol 2022; 7: 114-123. 2021/11/10. DOI: 10.1136/svn-2021-001134.
View at Publisher | View at Google Scholar - Williams BA, Voyce S, Sidney S, et al. Establishing a National Cardiovascular Disease Surveillance System in the United States Using Electronic Health Record Data: Key Strengths and Limitations. J Am Heart Assoc 2022; 11: e024409. 20220412. DOI: 10.1161/JAHA.121.024409.
View at Publisher | View at Google Scholar - Roger VL, Sidney S, Fairchild AL, et al. Recommendations for Cardiovascular Health and Disease Surveillance for 2030 and Beyond: A Policy Statement From the American Heart Association. Circulation 2020; 141: e104-e119. 20200129. DOI: 10.1161/CIR.0000000000000756.
View at Publisher | View at Google Scholar - von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med 2007; 4: e296. DOI: 10.1371/journal.pmed.0040296.
View at Publisher | View at Google Scholar - Prvu Bettger J, Thomas L and Liang L. Comparing Recovery Options for Stroke Patients. 2019. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI).
View at Publisher | View at Google Scholar - Zhong W, Geng N, Wang P, et al. Prevalence, causes and risk factors of hospital readmissions after acute stroke and transient ischemic attack: a systematic review and meta- analysis. Neurol Sci 2016; 37: 1195-1202. 2016/05/01. DOI: 10.1007/s10072-016-2570-5.
View at Publisher | View at Google Scholar - Leifheit EC, Wang Y, Goldstein LB, et al. Trends in 1-Year Recurrent Ischemic Stroke in the US Medicare Fee-for-Service Population. Stroke 2022; 53: 3338-3347. 2022/10/11. DOI: 10.1161/STROKEAHA.122.039438.
View at Publisher | View at Google Scholar - Prvu Bettger J, McCoy L, Smith EE, et al. Contemporary trends and predictors of postacute service use and routine discharge home after stroke. J Am Heart Assoc 2015; 4 2015/02/26. DOI: 10.1161/JAHA.114.001038.
View at Publisher | View at Google Scholar - Leppert MH, Sillau S, Lindrooth RC, et al. Relationship between early follow-up and readmission within 30 and 90 days after ischemic stroke. Neurology 2020; 94: e1249-e1258. 2020/02/23. DOI: 10.1212/WNL.0000000000009135.
View at Publisher | View at Google Scholar - Xian Y, Wu J, O'Brien EC, et al. Real world effectiveness of warfarin among ischemic stroke patients with atrial fibrillation: observational analysis from Patient-Centered Research into Outcomes Stroke Patients Prefer and Effectiveness Research (PROSPER) study. BMJ 2015; 351: h3786. 2015/08/02. DOI: 10.1136/bmj.h3786.
View at Publisher | View at Google Scholar - Reeves MJ, Fonarow GC, Smith EE, et al. Representativeness of the Get With The Guidelines-Stroke Registry: comparison of patient and hospital characteristics among Medicare beneficiaries hospitalized with ischemic stroke. Stroke 2012; 43: 44-49. 2011/10/08. DOI: 10.1161/STROKEAHA.111.626978.
View at Publisher | View at Google Scholar - O'Brien EC, Greiner MA, Xian Y, et al. Clinical Effectiveness of Statin Therapy After Ischemic Stroke: Primary Results From the Statin Therapeutic Area of the Patient-Centered Research Into Outcomes Stroke Patients Prefer and Effectiveness Research (PROSPER) Study. Circulation 2015; 132: 1404-1413. 2015/08/08. DOI: 10.1161/CIRCULATIONAHA.115.016183.
View at Publisher | View at Google Scholar - Fonarow GC, Liang L, Thomas L, et al. Assessment of Home-Time After Acute Ischemic Stroke in Medicare Beneficiaries. Stroke 2016; 47: 836-842. 2016/02/20. DOI: 10.1161/STROKEAHA.115.011599.
View at Publisher | View at Google Scholar - Fonarow GC, Smith EE, Reeves MJ, et al. Hospital-level variation in mortality and rehospitalization for medicare beneficiaries with acute ischemic stroke. Stroke 2011; 42: 159-
View at Publisher | View at Google Scholar - 166. 2010/12/18. DOI: 10.1161/STROKEAHA.110.601831.
View at Publisher | View at Google Scholar - Kaufman BG, O'Brien EC, Stearns SC, et al. The Medicare Shared Savings Program and Outcomes for Ischemic Stroke Patients: a Retrospective Cohort Study. J Gen Intern Med 2019; 34: 2740-2748. 2019/08/28. DOI: 10.1007/s11606-019-05283-1.
View at Publisher | View at Google Scholar - Kaufman BG, Shah S, Hellkamp AS, et al. Disease Burden Following Non- Cardioembolic Minor Ischemic Stroke or High-Risk TIA: A GWTG-Stroke Study. J Stroke Cerebrovasc Dis 2020; 29: 105399. 2020/12/02. DOI: 10.1016/j.jstrokecerebrovasdis.2020.105399.
View at Publisher | View at Google Scholar - Song S, Fonarow GC, Olson DM, et al. Association of Get With The Guidelines-Stroke Program Participation and Clinical Outcomes for Medicare Beneficiaries With Ischemic Stroke. Stroke 2016; 47: 1294-1302. 2016/04/16. DOI: 10.1161/STROKEAHA.115.011874.
View at Publisher | View at Google Scholar - Reeves MJ, Fonarow GC, Xu H, et al. Is Risk-Standardized In-Hospital Stroke Mortality an Adequate Proxy for Risk-Standardized 30-Day Stroke Mortality Data? Findings From Get With The Guidelines-Stroke. Circ Cardiovasc Qual Outcomes 2017; 10 2017/10/13. DOI: 10.1161/CIRCOUTCOMES.117.003748.
View at Publisher | View at Google Scholar - Lichtman JH, Leifheit-Limson EC and Goldstein LB. Centers for medicare and medicaid services medicare data and stroke research: goldmine or landmine? Stroke 2015; 46: 598-604. 2015/01/17. DOI: 10.1161/STROKEAHA.114.003255.
View at Publisher | View at Google Scholar - Ekker MS, Boot EM, Singhal AB, et al. Epidemiology, aetiology, and management of ischaemic stroke in young adults. Lancet Neurol 2018; 17: 790-801. 2018/08/22. DOI: 10.1016/S1474-4422(18)30233-3.
View at Publisher | View at Google Scholar - Centers for Medicare and Medicaid Services, Medicare and Medicaid enrollment reports, https://data.cms.gov/summary-statistics-on-beneficiary-enrollment/medicare-and-medicaid- reports/medicare-monthly-enrollment (2023).
View at Publisher | View at Google Scholar - Yu AYX, Rogers E, Wang M, et al. Population-based study of home-time by stroke type and correlation with modified Rankin score. Neurology 2017; 89: 1970-1976. 2017/10/13. DOI: 10.1212/WNL.0000000000004631.
View at Publisher | View at Google Scholar - Yu AYX, Fang J, Porter J, et al. Hospital-based cohort study to determine the association between home-time and disability after stroke by age, sex, stroke type and study year in Canada. BMJ Open 2019; 9: e031379. 2019/11/14. DOI: 10.1136/bmjopen-2019-031379.
View at Publisher | View at Google Scholar - Quinn TJ, Dawson J, Lees JS, et al. Time spent at home poststroke:
View at Publisher | View at Google Scholar - Mishra NK, Shuaib A, Lyden P, et al. Home time is extended in patients with ischemic stroke who receive thrombolytic therapy: a validation study of home time as an outcome measure. Stroke 2011; 42: 1046-1050. 2011/02/26. DOI: 10.1161/STROKEAHA.110.601302.
View at Publisher | View at Google Scholar - Gattellari M, Goumas C, Jalaludin B, et al. Measuring stroke outcomes for 74 501 patients using linked administrative data: System-wide estimates and validation of 'home-time' as a surrogate measure of functional status. Int J Clin Pract 2020; 74: e13484. 2020/02/01. DOI: 10.1111/ijcp.13484.
View at Publisher | View at Google Scholar - Kernan WN, Viera AJ, Billinger SA, et al. Primary Care of Adult Patients After Stroke: A Scientific Statement From the American Heart Association/American Stroke Association. Stroke 2021; 52: e558-e571. 20210715. DOI: 10.1161/STR.0000000000000382.
View at Publisher | View at Google Scholar - Boehme C, Toell T, Lang W, et al. Longer term patient management following stroke: A systematic review. Int J Stroke 2021; 16: 917-926. 20210520. DOI: 10.1177/17474930211016963.
View at Publisher | View at Google Scholar - Mohan KM, Crichton SL, Grieve AP, et al. Frequency and predictors for the risk of stroke recurrence up to 10 years after stroke: the South London Stroke Register. J Neurol Neurosurg
View at Publisher | View at Google Scholar - Psychiatry 2009; 80: 1012-1018. 20090521. DOI: 10.1136/jnnp.2008.170456.
View at Publisher | View at Google Scholar - Kwok GYR, Chen RWR, Leow TA, et al. Recurrent ischemic stroke in young adults: A multicenter cohort study, systematic review, and meta-analysis. Int J Stroke 2025: 17474930251340799. 20250428. DOI: 10.1177/17474930251340799.
View at Publisher | View at Google Scholar - Albright KC, Zhao H, Blackburn J, et al. Racial differences in statin adherence following hospital discharge for ischemic stroke. Neurology 2017; 88: 1839-1848. 20170412. DOI: 10.1212/WNL.0000000000003910.
View at Publisher | View at Google Scholar - Sheehan OC, Dhamoon MS, Bettger JP, et al. Racial differences in persistence to secondary prevention medication regimens after ischemic stroke. Ethn Health 2022; 27: 1671- 1683. 20210701. DOI: 10.1080/13557858.2021.1943321.
View at Publisher | View at Google Scholar - Shen YC, Chen G and Hsia RY. Community and Hospital Factors Associated With Stroke Center Certification in the United States, 2009 to 2017. JAMA Netw Open 2019; 2: e197855. 20190703. DOI: 10.1001/jamanetworkopen.2019.7855.
View at Publisher | View at Google Scholar
