

Case Report | DOI: https://doi.org/10.31579/2834-8389/041
Olfactory Neuroblastoma of the Nasal Cavity Managed with Modified Draf III and adjunctive Radiotherapy: Case Report and Literature Review*
1 College of Medicine, King Saud bin Abdulaziz University for Health Sciences, P.O, Box 3660, Saudi Arabia.
2 Consultant Otolaryngology, Department Otolaryngology, King Abdulaziz Medical City, P.O. Box 22490, Saudi Arabia.
3 Consultant Anatomic Pathology. Department Anatomic Pathology, King Abdulaziz Medical City, P.O. Box 22490, Saudi Arabia.
4 Consultant Radiation Oncology, Radiation Oncology Department, King Abdullah Specialized Children’s Hospital, P.O. Box 22490, Saudi Arabia.
*Corresponding Author: Almehizia Abdulmohsin, College of Medicine, King Saud bin Abdulaziz University for Health Sciences, P.O, Box 3660, Saudi Arabia.
Citation: Abdulmohsin A, Al-Bahkaly Sameer., Abdul L Khan., Altaleb Osama., Salem A, (2025), Olfactory Neuroblastoma of the Nasal Cavity Managed with Modified Draf III and adjunctive Radiotherapy: Case Report and Literature Review., International Journal of Clinical Case Reports, 4(1); DOI:10.31579/2834-8389/041
Copyright: © 2025, Almehizia Abdulmohsin. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 January 2025 | Accepted: 07 February 2025 | Published: 21 February 2025
Keywords: bronchial asthma; atrial fibrillation; maternal sexuality; hypertension
Abstract
Olfactory neuroblastoma is a rare neoplasm that grows in epithelia cells of olfactory tissue. It is related to many tumor oncogenes such as MYC. We present and discuss a rare case of ONB on the elderly with typical symptoms but different treatment approaches.
Case Presentation
A 71-year-old Caucasian man presented to the emergency department with headache, generalized fatigue, and nasal pain and swelling. There was nasal bleeding, discharge, and signs of chronic infection. The patient could not stand nor move, and he had occasional high blood pressure readings (over 200 mmHg) and shortness of breath with coughing. The patient was known to have a case of ONB in the right nasal cavity, as well as bronchial asthma, atrial fibrillation, and hypertension. Twenty years ago, he had undergone a nephrectomy for suspicion of cancer. On physical examination, the patient’s weight and height were recorded as 104 kg and 175 cm, respectively. His vitals were stable, and he was afebrile. With regard to the otorhinolaryngology examination, his throat was clear, with no signs of congestion, and he did not feel pain in the ears. Endoscopic examination disclosed a polypoid mass in the right nasal cavity, and a biopsy was taken. In the chest, he had bilateral equal breath sounds without added sounds. The rest of the examinations were unremarkable, and the patient did not have a history of trauma. Magnetic resonance imaging (MRI) revealed the presence of a large tumor on the right side of the nasal cavity that extended to the nasopharynx and ethmoid air cells as well as the medial wall of the right maxillary sinus and the antrum, which caused bulging into the right maxillary sinus (Figure 2). It obstructed sinonasal flow and led to opacification and mucosal thickening; it was isointense on T1 to cerebral parenchymal and heterogenous on T2-weighted images. Both diffusion-weighted images and the apparent diffusion coefficient (ADC) map revealed a hypocellularity pattern of the lesion. The tumor extended posteriorly and bulged into the sphenoid sinus. Moreover, abnormal signal intensity and enhancement were observed in both the frontal bone and olfactory groove bone. Computerized tomography (CT) of the brain and sinuses showed a large lesion in the ethmoid cells and right nasal cavity (Figure 1),
Figure 1: Preoperative CT Scan and MRI of brain and sinuses. (A) sagittal view, (B) axial post-contrast T1 , (C) Coronal post-contrast T1. It shows the extension of ONB in the patient.
with the left ethmoid involved. The lesion extended to the nasopharynx and bulged into the right sphenoid and maxillary sinuses. After contrast injection, the lesion exhibited a strong enhancement in the CT imaging. Mucous retention was observed in the maxillary, sphenoid, and frontal sinuses on the right side. The intracranial area was spared. This case report is staged C according to the Kadish system (Table 1).
Stage | Definition |
A | Confounded to nasal cavity. |
B | Extended to paranasal sinus. |
C | The tumor reached the brain tissues. |
D | Regional or distal metastasis. |
Table 1: Kadish Tumor Staging.
The patient underwent endoscopic tumor resection with RT. There was moderate blood loss (about 1200 ml), but no postoperative complications arose. The patient was treated with 32 postoperative RT sessions. After histological examination, it was found that the tumor was formed of variable-sized nests of small uniform basaloid cells with eosinophilic fibrillary cytoplasm. No mitoses were seen, and there was no necrosis. The intervening stroma was highly vascularized. On immunohistochemistry analysis, the lesional cells were observed to be positive for CD56, synaptophysin, and chromogranin. The lesional cells were negative for CD99, myogenin, pan CK, and EMA. The S100 highlighted sustentacular cells. The Ki-67 proliferation index was low. The features of the olfactory neuroblastoma can be observed in (Figure 2).
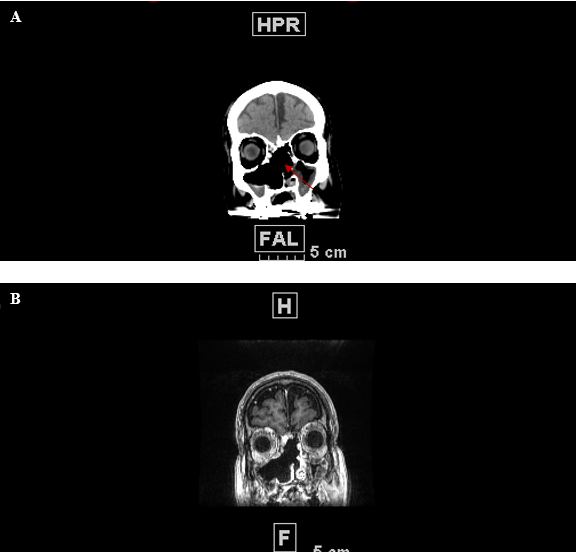
Figure 2: Nasal mucosa with and extended tumor, which is mostly arranged as variable sized nests of tumor cells arrowed (A:H&E, Scanning magnification). Tumor cells nests were formed of fairly uniform cells showing hyperchromatic nuclei and a slightly eosinophilic cytoplasm, and the intervening stroma is vascular (B: H&E,x40 MAGNIFICATION). Upon immunohistochemistry, the tumor cells were strongly positive for synaptophysin (C), CD56 (D), and chromogranin (E). Sustentacular cells are highlighted with S100 (F).
After one month of the procedure, the patient was followed up with an MRI (Figure 3), which showed that the nasal cavity and nasopharynx tumor had been widely resected. However, it was observed that the nasal cavity, right maxillary sinus, and the ethmoid air cells were deformed, and the nasal septum was partially resected. The remaining ethmoid air cells were bilaterally filled with fluid/blood, and some thickening and enhancement of the mucosa were observed. Furthermore, there was also an enhancement in the nasal cavity and septum as well as nasopharynx along the surgical bed. These changes were probably due to postoperative changes, but the presence of underlying residual tumor couldn’t be excluded nor confirmed at this stage. The bilateral maxillary and sphenoid sinuses were filled with fluid and blood. There was a mucosal thickening in both maxillary sinuses. In contrast, the intracranial site was unchanged, and the only alterations observed were due to multiple old ischemic lesions. The patient is scheduled for a follow up on MRI and endoscopic examination after two years.
Discussion
ONB manifestations are classified as nasal, neurological, oral, facial, and ophthalmological. The most common symptoms are unilateral nasal obstruction (70%) and epistaxis (46%) [8-9]. Other symptoms are elevated cortisol in serum, blood glucose, and 24-hours urinary cortisol levels as well as high adrenocorticotropic hormone levels [8]. Unusual symptoms include severe proximal weakness, lethargy, and lower extremity edema [8]. Kadish and colleagues established a clinical staging system in 1975 for ONB (Table 1). At stage A, the tumor is confounded to the nasal cavity; at stage B, the tumor extends to the paranasal sinus; and at stage C, the tumor reaches the brain tissues [9]. Moreover, Mortia et al. added stage D to the system, to include a regional or distal metastasis [10]. Thus, this staging system was extremely helpful to categorize ONB and is still widely used. In contrast, Hyams developed a pathological staging system to classify ONB, with up to four grades. Grade 1 is considered a mild disease whereas grade IV is considered a severe form of ONB [11]. A total of 62% of ONB cases are classified as grade I and
II on the Hyams staging system [12-13], and Malouf et al. noticed that patients who had a high-grade ONB also had larger tumor and lymph node involvement [14-15]. Christopher et al. revised both staging systems: the Kadish and Hyams; they found that both advanced Kadish and Hyams staging predicted a poorer patient outcome and, thus, recommended aggressive approaches for treatment [16]. A study recently published showed ONB metastasis to submandibular area [ 17] Another staging system was proposed by Dulguerov and colleagues, and it is based on a tumor, lymph node, and metastasis (TNM) approach [18] and uses computed tomography (CT) and magnetic resonance imaging (MRI). It can be used on patients before and after surgery. Originally, lateral rhinotomy was the only available treatment for ONB [19], but later a new treatment protocol was proposed, which consisted of craniofacial surgery followed by radiotherapy therapy (RT) [18]. Nevertheless, the most suitable treatment is still under debate [19]. Recently, new studies have suggested that a minimally invasive approach, such as endoscopic surgery, is better because it reduces surgery duration, complications, and hospital stay period [20-21]. Adam Folbe et al. conducted a large multicentered study evaluating the efficacy of an endoscopic approach of ONB; in comparison with traditional approaches, they found similar results only when the procedure was done in certain patients by an experienced hand. However, it also provides magnified multiangled views of the tumor and lower morbidity [20]. Suriano et al. reported that endoscopic resection was related to lower morbidity [22]. Moreover, endoscopic surgery is a feasible treatment for advanced ONB (advanced according to the Kadish staging system) [22-23]. In contrast, Draf III, also known as modified endoscopic Lothrop procedure, was described in the mid-1990s; it provides access to frontal sinuses by median drainage and removal of inferior and superior structures on the frontal sinus as well as the removal of the inferior part of interferential septum [23]. We approached this case using the Draf III procedure, medial maxillectomy, bilateral ethmoidectomy, high septal resection, and navigation of sinuses. We started with the navigation of sinuses to debulk the mass and draw landmarks from the right olfactory fossa to nasal cavity. Then, we widened the right maxillary for cleaning. Subsequently, we performed a medial maxillectomy and completely removed the inferior turbinate. Additionally, we removed the medial wall of the right maxilla because the mass was engulfing the inferior turbinate as well as the nasolacrimal apparatus. We proceeded to remove the tumor from the anterior ethmoidal area and then penetrated the lamella to reach the posterior ethmoid to remove the tumor in the sphenoid sinus. Next, we performed a high septal resection to perform the Draf III procedure, which was used to clean the left frontal sinus. Then, we lowered down the septum and interseptal frontal sinuses. On the left side, we went through the maxilla to perform a maxillectomy to remove the tumor section present in the ethmoid. Domenico and colleagues assessed treatment characteristics and the outcomes of ONB in a tabular form, where they included several papers from Dulguerov and Calcateraa (1992) to Lapierre et al. (2016) [24]. Dulguerov and Calcateraa reported that craniofacial resection was favorable among patients. Furthermore, they found that 93% (of the 12 subjects) were disease-free when they combined surgery and radiation [25]. John Hopkin’s experience involved managing ONB with craniofacial resection with complete tumor resection and using a chemotherapy treatment with compounds such as cisplatin in advanced disease palliation [26]. Alotaibi and colleagues studied single-center experiences on ONB and found that surgery with adjuvant radiation therapy is the best treatment modality [27]. Of late, there is a consensus that RT is important for eradicating tumors. However, the optimal RT volume is difficult to determine in most patients [24], and radiation dose varies according to literature. The references doses of RT are 45 Gy preoperative and 50-60 Gy postoperative [28], and doses between 65-70 Gy should be given for definitive radiotherapy [29]. Spaulding et al. advocated the use of preoperative radiotherapy of 50 Gy and craniofacial surgery for ONB in stage A and B tumors according to the Kadish staging system [30], whereas Broich and Urdaneta recommended using surgery and RT for all stages of Kadish’s system [31-32]. Survival of the patient is crucial, and it is one of the most important determiners when choosing a treatment. Eden and coworkers reported no significant difference in patient survival when using preoperative and postoperative RT, but they noticed an improvement in local tumor control [33]. Nevertheless, there is clear data in the literature that confirms that surgery followed by RT increases survival rate [34]. For example, Nalee Kim and colleagues found that patients who were treated with surgery followed by RT exhibited a 46.7% 5-year progression-free (PFS) survival compared to the 5-year PFS of 19.4% of patients who were treated with surgery alone [34]. In the last ten years, the role of chemotherapy in ONB has been studied. Porter et al. used chemotherapy as adjunctive for severe cases. They reported that the survival rate and local occurrence was not significantly affected, but they consider that both the knowledge and use of chemotherapy in ONB will be expanded in the future [35]. In this case report, we carefully studied the patient history, considered different alternatives for the treatment, and finally opted for an aggressive approach with endoscopic surgery followed by extensive radiotherapy.
Conclusion
We report a case of ONB that was cured using an endoscopic surgery approach followed by extensive radiotherapy. Thus, we have contributed to the information available about this rare cancer and the possible treatments that can be used on patients.
Acknowledgment
We would like to extend our gratitude to the King Abdullah International Medical Research Center (KAIMRC), pathology department and radiology department KAMC. And radiotherapy department in KASCH, for guidance and cooperation.
Funding
This study did not receive funding from any institution or organization.
The funder is involved in manuscript writing and approval of publication.
References
- Olfactory Neuroblastoma of the Nasal Cavity Managed with Modified Draf III and adjunctive Radiotherapy: Case Report and Literature Review*
View at Publisher | View at Google Scholar - Leon-Soriano, E., Alfonso, C., Yebenes, L., Garcia-Polo, J., Lassaletta, L., & Gavilan, J. (2016). Bilateral Synchronous Ectopic Ethmoid Sinus Olfactory Neuroblastoma: A Case Report. American Journal of Case Reports, 17, 268–273.
View at Publisher | View at Google Scholar - Thompson, L.D.R. (2009). Olfactory Neuroblastoma. Head and Neck Pathology, 3(3), 252–259.
View at Publisher | View at Google Scholar - Berger, L., Luc, R. & Richard, D. (1924) L’esthesioneuroepitheliome olfactif. Bull.Assoc. Fr. Etude Cancer 13, 410–421
View at Publisher | View at Google Scholar - Weiss, G.J., Liang, W.S., Izatt, T., Arora, S., Cherni, I., … Raju, R.N. (2012). Paired Tumor and Normal Whole Genome Sequencing of Metastatic Olfactory Neuroblastoma. PLoS ONE, 7(5), e37029.
View at Publisher | View at Google Scholar - Mao, L., Xia, Y., Zhou, Y., Dai, R., Yang, X., Wang, Y., Duan, S., Qiao, X., Mei, Y., & Hu, B. (2009) Activation of Sonic Hedgehog Signaling Pathway in Olfactory Neuroblastoma. Oncology, 77, 231-243.
View at Publisher | View at Google Scholar - Gallia, G.L., Zhang, M., Ning, Y., Haffner, M.C., Batista, D., … Binder, Z.A. (2018). Genomic analysis identifies frequent deletions of Dystrophin in olfactory neuroblastoma. Nature Communications, 9(1).
View at Publisher | View at Google Scholar - Batacchi, Z., Andeen, N.K., & Trikudanathan, S. (2018). An unusual manifestation of olfactory neuroblastoma. BMJ Case Reports, bcr-2017-221661. https://doi.org/10.1136/bcr-2017-221661
View at Publisher | View at Google Scholar - Kadish, S., Goodman, & M., Wang, C.C. (1976) Olfactory neuroblastoma. A clinical analysis of 17 cases. Cancer, 37(3), 1571-1576.
View at Publisher | View at Google Scholar - Morita, A., Ebersold, M.J., Olsen, K.D. et al. (1999) Esthesioneuroblastoma: Prognosis and management. Neurosurgery, 32(5), 706-714; discussion 714-715
View at Publisher | View at Google Scholar - Hyams, V.J. Tumors of the upper respiratory tract and ear. In: Hyams VJ, Batsakis JG, Michaels L, eds. Atlas of Tumor Pathology. 2nd series, Fascile 25. Washington, DC: Armed Forces Institute of Pathology, 1988:240-248.
View at Publisher | View at Google Scholar - Lee, A., Goldstein, D.P., Irish, J., Gentili, F., & Perez-Ordonez, B. (2007) Noncontiguous bilateral esthesioneuroblastoma: A case report. Skull Base, 17(6), 405-407.
View at Publisher | View at Google Scholar - Hirose, T., Scheithauer, B.W., Lopes, M.B. et al (1995) Olfactory neuroblastoma. An immunohistochemical, ultrastructural, and flow cytometric study. Cancer, 76(1), 4-19
View at Publisher | View at Google Scholar - Malouf, G.G., Casiraghi, O., Deutsch, E., Guigay, J., Temam, S., Bourhis, J. (2013) Low- and high-grade esthesioneuroblastomas display a distinct natural history and outcome. European Journal of Cancer 49, 1324-1334.
View at Publisher | View at Google Scholar - Hansen EK, Roach M. Handbook of evidence-based radiation oncology. New York: springer; 2018 Jun 17.
View at Publisher | View at Google Scholar - Christopher Miyamoto, R., Gleich, L.L., Biddinger, P.W., Gluckman, J.L. (2000) Esthesioneuroblastoma and sinonasal undifferentiated carcinoma: impact of histological grading and clinical staging on survival and prognosis. The Laryngoscope. 110(8), 1262-1265.
View at Publisher | View at Google Scholar - Appukutty S, Di Palma S, Whitaker S, Wood K. Olfactory Neuroblastoma Presenting as a Submandibular Mass. American Journal of Laboratory Medicine. 2019 May 9;4(2):35-9.
View at Publisher | View at Google Scholar - Dulguerov, P., Allal, A.S., Calcaterra, T.C. (2001) Esthesioneuroblastoma: a meta-analysis and review. The lancet oncology 2(11), 683-690.
View at Publisher | View at Google Scholar - Polin, R.S., Sheehan, J.P., Chenelle, A.G., Munoz, E., Lamer, J., Phillips, C.D., Cantrell, R.W., Laws, E.R., Newman, S.A., Levine, P.A., Jane, J.A. (1998) The role of preoperative adjuvant treatment in the management of esthesioneuroblastoma: the University of Virginia experience. Neurosurgery, 42(5), 1029-1037.
View at Publisher | View at Google Scholar - Weber, R., Draf, W., Kratzsch, B., Hosemann, W., Schaefer, S.D. (2001) Modern concepts of frontal sinus surgery. The Laryngoscope. 111(1), 137-146.
View at Publisher | View at Google Scholar - Folbe, A., Herzallah, I., Duvvuri, U., Bublik, M., Sargi, Z., Snyderman, C. H., … Casiano, R. (2009). Endoscopic endonasal resection of esthesioneuroblastoma: A multicenter study. American Journal of Rhinology and Allergy, 23(1), https://doi.org/10.2500/ajra.2009.23.3269
View at Publisher | View at Google Scholar - Suriano, M., De Vincentis, M., Colli, A., et al. (2007) Endoscopic treatment of esthesioneuroblastoma: A minimally invasive approach combined with radiation therapy. Otolaryngology–Head and Neck Surgery 136, 104-107.
View at Publisher | View at Google Scholar - Walch, C., Stammberger, H., Anderhuber, W., et al. (2000) The minimally invasive approach to olfactory neuroblastoma: Combined endoscopic and stereotactic treatment. Laryngoscope 110, 635-640.
View at Publisher | View at Google Scholar - Cante, D., Piva, C., Sciacero, P., Franco, P., Petrucci, E., Casanova, B.V, et al. (2017) Olfactory neuroblastoma treated with minimally invasive surgery and adjuvant radiotherapy: a case report and review of the literature. BJR Case Rep 3, 20170077.
View at Publisher | View at Google Scholar - Dulguerov, P., & Calcaterra, T. (1992). Esthesioneuroblastoma: The UCLA Experience 1970-1990. The Laryngoscope, 102(8), 843-849.
View at Publisher | View at Google Scholar - Resto, V.A., Eisele, D.W., Forastiere, A. , Zahurak, M. , Lee, D. & Westra, W.H. (2000), Esthesioneuroblastoma: The Johns Hopkins experience. Head Neck, 22, 550-558.
View at Publisher | View at Google Scholar - Alotaibi HA, Priola SM, Bernat AL, Farrash F. Esthesioneuroblastoma: Summary of Single-center Experiences with Focus on Adjuvant Therapy and Overall Survival. Cureus. 2019 Jun;11(6).
View at Publisher | View at Google Scholar - Eich, H.T., Staar, S., Micke, O., Eich, P.D., Stützer, H., & Müller, R.P. (2001) Radiotherapy of esthesioneuroblastoma. International Journal of Radiation Oncology* Biology* Physics, 49(1), 155-160.
View at Publisher | View at Google Scholar - Brady LW, Wazer DE, Perez CA. Perez & Brady's principles and practice of radiation oncology. Lippincott Williams & Wilkins; 2013 May 6.
View at Publisher | View at Google Scholar - Spaulding, C.A., Kranyak, M.S., Constable, W.C., & Stewart, F.M. (1998) Esthesioneuroblastoma: a comparison of two treatment eras. International Journal of Radiation Oncology* Biology* Physics, 15(3), 581-90.
View at Publisher | View at Google Scholar - Urdaneta, N., Fischer, J.J., & Knowlton, A. (1998) Olfactory neuroblastoma. Observations on seven patients treated with radiation therapy and review of the literature. American journal of clinical oncology, 11(6), 672-8.
View at Publisher | View at Google Scholar - Bmich, G., Pagliari, A., & Ottaviani, F. (1997) Esthesioneuroblastoma: a general review of the cases published since the discovery of the tumor in 1924. Anticancer Res. 17, 2683-2706.
View at Publisher | View at Google Scholar - Eden, B.V., Debo, R.F., Larner, J.M., Kelly, M.D., Levine, P.A., Stewart, F.M., Cantrell, R.W., & Constable, W.C. (1994) Esthesioneuroblastoma. Long term outcome and patterns of failure—the University of Virginia experience. Cancer, 73(10), 2556-2562.
View at Publisher | View at Google Scholar - Kim, N., Lee, C. G., Kim, E. H., Kim, C.-H., Keum, K. C., Lee, K.-S., … Suh, C.-O. (2019). Patterns of failures after surgical resection in olfactory neuroblastoma. Journal of Neuro-Oncology, 141(2), 459-466.
View at Publisher | View at Google Scholar - Porter, A.B., Bernold, D.M., & Giannini, C., et al. (2008) Retrospective review of adjuvant chemotherapy for esthesioneuroblastoma. Journal of Neuro-Oncology 90(2), 201-204.
View at Publisher | View at Google Scholar
