

Review Article | DOI: https://doi.org/DOI: 10.31579/2835-835X/040
Non-compaction of the left ventricle revealed by de novo heart failure in adults: a clinical case with a literature review.
1 Department of Cardiology, IBN Rochd University Hospital, Casablanca, Morocco
*Corresponding Author: M. Charfo bacharou, Department of Cardiology, IBN Rochd University Hospital, Casablanca, Morocco
Citation: M. Charfo bacharou, Be. Ovaga, B. Mohammed sidi, P.M Mulendele, M. Njie, M. Haboub, l. Azzouzi (2023), non-compaction of the left ventricle revealed by de novo heart failure in adults: a clinical case with a literature review, Clinical Trials and Case Studies; 2(5): DOI: 10.31579/2835-835X/040
Copyright: © 2023 M. Charfo bacharou, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 August 2023 | Accepted: 20 September 2023 | Published: 16 October 2023
Keywords: Echocardiography; Magnetic resonance imaging; Noncompaction of the left ventricle; Thrombus.
Abstract
Introduction
Rare cardiomyopathy left ventricle non-compaction (LVNC) or excess trabeculation is an unclassified heart disease related to the cessation of the normal process of myocardial development during the first trimester of pregnancy. Familial forms account for approximately half of the cases, and men are the most affected. The usual clinical presentation corresponds to the classic triad, which includes heart failure, arrhythmias, and thromboembolic manifestations.
Case Presentation
Here, we describe the case of a 56-year-old man with no pathological history who consulted for dyspnea, and in whom transthoracic echocardiography and magnetic resonance imaging have made it possible to retain the diagnosis of an excess of trabeculations complicated by heart failure and an apical thrombus.
Conclusion
LVNC is a rare cardiomyopathy that frequently affects men and is diagnosed using echocardiography and in borderline cases, supplemented by cardiac MRI.
Introduction
Ventricular non-compaction is a rare cardiomyopathy characterized morphologically by excess trabeculations separated by deep recesses of the ventricular wall [1]. This wall is made of a bilayer comprising a thin layer under epicardial and compacted layers, and a thick layer under endocardial and uncompacted [1-2]. The apex, the median segment of the lateral and lower walls, represents the most frequent localization related to embryogenesis imperfecta [1, 3]. LVNC occurs either in isolation or in combination with other congenital heart diseases, neuromuscular disorders, or mitochondrial disorders [1,3-4]. The clinical spectrum is broad, ranging from asymptomatic forms to tables of heart failure, ventricular arrhythmias, and/or thromboembolic events [3-4]. Diagnosis is based on echocardiography and magnetic resonance imaging (MRI), which can be difficult in borderline forms [1-3]. The prognosis is highly variable and is determined by functional status and clinical and morphological parameters [3-5].
We report a case of LV non-compaction in a 56-year-old adult with no history of cardiology, managed in the heart failure unit of the cardiology department.
Case presentation
A 56-year-old adult smoker presented with stage II NYHA (New York Heart Association) dyspnea associated with swelling of the lower limbs that had been progressing for six months. He was married, the father of two children, the eldest of five siblings, and the collaterals who would be healthy. There was no evidence of heart disease or sudden death in the patient’s family. On examination, the patient was in good general condition and hemodynamically stable, with a blood pressure of 100/70 mmHg and heart rate of 98 beats per minute. He weighed 90 kg, and his height was 178 cm. The sounds of the heart were regular with a left galloping sound, a burst of pulmonary B2, and an Apexian systolic murmur of intensity 2/6th. The lungs were free. The electrocardiogram was recorded in sinus rhythm at 98 cycles/min, and the axis of the heart deviated to the left with a left anterior hemiblock (Figure 1).
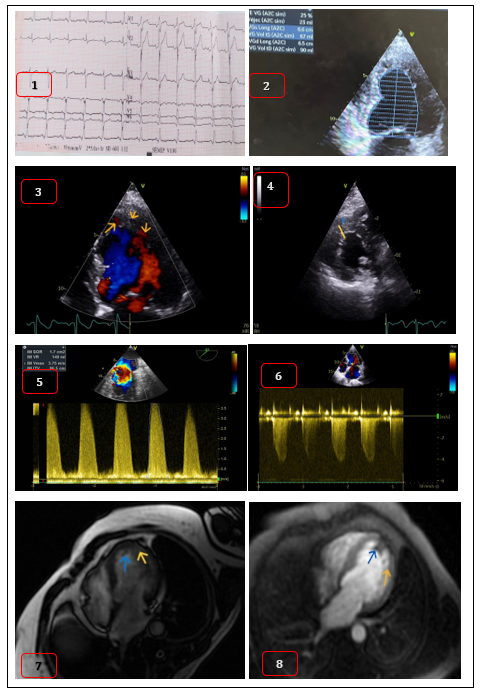
Transthoracic echocardiography revealed dilation of the left heart chambers (diastole left ventricle=44 ml/m²) and severe impairment of LV systolic function with a left ventricle ejection fraction (LVEF) of 25% (Figure 2). The myocardium had a spongy appearance, indicative of significant trabeculations separated by a localized recess along the apical cuff extending to the anterolateral wall (Figure 3). The subendocardial uncompacted zone (NCZ) measured 12 mm compared with 5 mm for a subepicardial compacted zone (CZ), that is, an NCZ/CZ ratio of 2.4 according to the Jenni criteria (Figure 4). One could note the filling of these recesses by blood flow to the color Doppler. The right ventricle (DV) had normal morphology and good function. The valves were thin, and there was severe mitral regurgitation with posterior mitral valve ballooning (Figure 5) and significant pulmonary hypertension at 73 mmHg (Figure 6). Cardiac MRI showed an enlarged LV with severe systolic dysfunction (LVEF at 26.7%) and a large network of trabeculations predominant in the apical, lateral, and inferior areas (Figure 7). Inhomogeneous hypoperfusion was also observed under inferomedian and apical endocardial conditions, dense endocardial fibrosis without specific coronary distribution, and apical thrombus (Figure 8). The NCZ/CZ ratio was 2.57. The VD was undilated with an ejection fraction of 53.49%. Coronary angiography showing a dystrophic and pathological bisecting artery.
The patient was administered a diuretic, angiotensin-converting enzyme (ACE) inhibitor, anti-aldosterone, beta-blocker, and sodium-glucose co-transport inhibitor. Mitral plasty associated with the primary implantation of a cardiac defibrillator (ICD) for primary prevention is also indicated. The family survey of relatives who were all asymptomatic revealed the sister's isolated non-compaction of the LV.
Figures:
- Electrocardiogram was recorded in sinus rhythm at 98 cycles/min, and the axis of the heart deviated to the left with a left anterior hemiblock.
- TTE show LV systolic function with a left ventricle ejection fraction of 25%.
- Multiples trabeculations separated by a localized recess along the apical cuff extending to the anterolateral wall.
- TTE parasternal short axis view showed NCZ/CZ ratio of 2.4 according to the Jenni criteria.
- TTE show severe mitral regurgitation.
- TTE show pulmonary hypertension at 73 mmHg.
- Cardiac MRI show a large network of trabeculations predominant in the apical, lateral, and inferior areas.
- Cardiac MRI show endocardial fibrosis without specific coronary distribution, and apical thrombus.
Discussion
LVNC is a rare cardiomyopathy that can affect all ages, from fetuses to adults. The incidence of this disease varies according to age and the population studied, it is estimated between 0.05 -0.014% [1-2, 6]. Men are more affected than women with a male-to-female ratio of 2:3, the average age of occurrence is 40-50 years [1-2, 4]. Cardiomyopathy is not classified by the WHO or European Society of Cardiology. LVNC is considered a genetic cardiomyopathy by the American Heart Association [2-3]. The familial form accounts for 13-50%, which warrants routine family screening, particularly for first-degree relatives [1-4]. The mutation in the MYH7 sarcomere gene is most frequently associated with LVNC, which is usually autosomal dominant or X-linked [1, 3]. Our patient was a 56-year-old man with no history of heart disease, who was found by family screening to have LVNC in his sister.
The etiology of LVNC has not yet been elucidated, and current data on myocardial development do not support the conventionally accepted hypothesis of cessation of the embryological process of progressive LV compaction over 5-8 weeks, which would explain the persistence of excess trabeculations separated by deep crypts and communicating with the lumen of the LV [1-3, 7]. Stopping this process would be the origin of the LV appearance with the double layer, a thin subepicardial and compacted layer, and a spongy, thick subendocardial, and uncompacted layer defining the LVNC [1,6]. It can be isolated or associated with congenital heart, mitochondrial, or neuromuscular diseases [1,7]. Moreover, current data on myocardial development do not support the hypothesis of stopping the formation of a compacted myocardium from an uncompacted myocardium [7].
The clinical presentation varies from asymptomatic forms to the classic triad, including the table of insufficiency, cardiac arrhythmias, and sometimes fatal or thromboembolic events [2-3]. In our patient, these were the symptoms and signs of heart failure, with dyspnea, edema, and lower limbs. Heart failure is found in 50-73% of LVNC cases and results from either systolic or diastolic dysfunction [1, 3]. Systolic dysfunction is secondary to a decrease in the coronary reserve, leading to hypoperfusion of the subendocardial layer, as demonstrated in positron emission tomography studies [1]. Diastolic dysfunction is the result of a compliance disorder induced by excess trabeculation, with a restrictive echocardiography profile [3, 8]. The electrical abnormalities observed are variable, including atrial fibrillation in 25%, supraventricular tachycardias, Wolf Parkinson white syndrome, branch block, and sometimes fatal ventricular arrhythmias in 18-47% of cases of LVNC [1, 3, 4]. These arrhythmias are related to fibrosis due to excess trabeculation and a progressive decrease in ventricular ejection fraction or dilation of the left atrium [1, 5]. Thromboembolic events (cerebral ischemia, myocardial infarction, and mesenteric) are encountered in 13%–38% of cases and are secondary to the presence of deep recess separating trabeculations, severe alteration of systolic function, or dilation of the ventricular cavity [1, 4]. Our patient did not have arrhythmia; however, an apical thrombus was found on cardiac MRI.
Transthoracic echocardiography is the reference diagnostic method by Jenni's 3 criteria, that is, the presence of two myocardial layers (compacted and uncompacted), endocardial trabeculations separated by deep crypts highlighted in color Doppler, and an uncompacted/compacted ratio >2:1 in end-systole [1,3]. Cardiac MRI, with Petersen's criteria, complements echocardiography in borderline cases and the absence of a good acoustic window, with good resolution to differentiate the two layers of the wall [1,3, 7]. The preferred locations are the apex, inferomedian, and lateromedian segments, as in our patient [1, 3-4]. Our patient presents all three criteria with a bilayer and an NCZ/CZ ratio of 2.4 on echocardiography and 2.57 on MRI. Our patient had severe mitral regurgitation and pulmonary hypertension.
There is no specific treatment for LVNC cardiomyopathy; the treatment is similar to that for heart failure, arrhythmias, and anticoagulation according to current recommendations [1, 3]. Our patient was treated with medical treatment for heart failure, an indication for an ICD for primary prevention associated with mitral plasty. Prognosis is variable, annual mortality is 2.16%, and it is influenced by age at presentation, NYHA functional status, occurrence of sustained ventricular arrhythmia, end-diastolic diameter LV, and ZNC/ZC ratio [3-6, 9].
Conclusion
Unclassified cardiomyopathy (LVNC) is a probable genetic pathology that must be considered in front of an excess of trabeculations to echocardiography or a picture of heart failure in a young adult.
Patient Consent
Written informed consent was obtained from the patient for the publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethics Approval
As per international standard or university standard written ethical approval has been collected and preserved by the author(s).
Conflicts of interest disclosure
The authors have no conflicts of interest.
References
- Towbin JA, Jefferies JL. (2017). Cardiomyopathies due to left ventricular noncompaction, mitochondrial and storage diseases, and inborn metabolic errors 15;121(7):838–54.
View at Publisher | View at Google Scholar - S.Fennira et al. (2019). Non compaction du ventricule gauche : ce qu’il faut savoir. Ann Cardiol Angeiol Tome 68, Numéro 2, avril, P : 120-124.
View at Publisher | View at Google Scholar - Oechslin E, Jenni R. (2011). Left ventricular non-compaction revisited: a distinct phenotype with genetic heterogeneity European Heart Journal. 1;32(12):1446–56.
View at Publisher | View at Google Scholar - Toader D, Paraschiv A, Tudorașcu P, Tudorașcu D, Bataiosu C, Balșeanu A. Left ventricular noncompaction—a rare cause of triad: heart failure, ventricular arrhythmias, and systemic embolic events: a case report. Journal of Medical Case Reports. 2021 Jun 8;15(1):316.
View at Publisher | View at Google Scholar - Demir E, Bayraktaroğlu S, Çinkooğlu A, Candemir A, et al. (2022). Characteristics and long-term survival of patients with left ventricular non-compaction cardiomyopathy. ESC Heart Failure.9(6):4219–29.
View at Publisher | View at Google Scholar - Hirono K, Takarada S, Miyao N, Nakaoka H, et al. (2022). Thromboembolic events in left ventricular non-compaction: comparison between children and adults: a systematic review and meta-analysis. Open Heart.9(1): e001908.
View at Publisher | View at Google Scholar - Petersen SE, Jensen B, Aung N, Friedrich MG, et al. (2023). Excessive Trabeculation of the Left Ventricle. JACC: Cardiovascular Imaging. 16(3):408–25.
View at Publisher | View at Google Scholar - S.Lahmiti et al. (2012). Non-compaction du ventricule droit : à propos de deux cas. Ann Cardiol Angeiol (Paris).
View at Publisher | View at Google Scholar - Gerard H, Iline N, Martel H, Nguyen K, Habib G.et al. (2022). Prognosis of Adults with Isolated Left Ventricular Non-Compaction: Results of a Prospective Multicentric Study. Front Cardiovasc Med.2; 9:856160.
View at Publisher | View at Google Scholar
