

Review Article | DOI: https://doi.org/10.31579/2835-8147/047
Nipah Virus Infections
1 Department of Microbiology, AIIH&PH, Kolkata, BN Campus, JC-27 and 27 B, Sector 3, Saltlake, Kolkata-700106, India.
2 Associate Professor, Microbiology, AIIMS, Deoghar, India.
3 Assistant Professor, Community Medicine, Diamond Harbour Govt. Medical College and Hospital, West Bengal, India.
4 Senior Registrar, Department of Medicine, Apollo Multispecialty Hospitals, Kolkata, India.
*Corresponding Author: Sayan Bhattacharyya, Associate Professor, Microbiology, AIIH&PH, Kolkata -700106, India.
Citation: Bhattacharyya S, Kumar SK, Majumdar S, Dutta M., (2023), Nipah Virus Infections, Clinics in Nursing, 2(5) DOI:10.31579/2835-8147/047
Copyright: © 2023, Bhattacharyya S. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 September 2023 | Accepted: 21 September 2023 | Published: 29 September 2023
Keywords: Nipah, Pteropus, Malaysia, Kerala
Abstract
A burning topic in the Indian subcontinent is the outbreak of Nipah virus that has affected Kerala in India for the fourth time since 2018. As this virus can directly infect humans and gives rise to non-specific symptoms, thorough history taking and high alertness of suspicion are the keys to diagnosis. The lack of preventive and curative measures towards an infection that has nearly 70% mortality rate brings to light the gravity of the situation, along with the need for thorough research into its pathophysiology and appropriate course of management.
Introduction
Nipah virus is a zoonotic virus which can cause infections like encephalitis or infection of the brain, along with involvement of other organs like lungs [1]. The virus causes almost annual outbreaks in India and Bangladesh. This year also, cases have been reported in Kerala, India. Mortality after the infection is quite high. Bats act as the reservoir hosts of the virus. The infection may also spread by contaminated fruits and date palm sap containing secretions of the bats. The 2018 annual review of the WHO R&D Blueprint list of priority diseases mentions that there is urgent need for speedy research and development for Nipah virus [2].
The agent:
The virus is an enveloped RNA virus having negative sense polarity. It belongs to the family Paramyxoviridae and genus Henipavirus, with other members of this genus being the Hendra virus and Cedar virus. Nipah virus can be very large in size. There are 2 strains of the virus: - the Bangladesh strain (NiV-BD) and the original Malaysian strain or NiV-M [3]. Probably the strains of NiV-BD genotype diverged during 1995 from the original Malaysian strain and thus formed two sub lineages. The RNA genome of the virus has 6 genes: nucleocapsid (N), phosphoprotein (P), matrix (M), fusion glycoprotein (F), attachment glycoprotein (G) and the long polymerase (L) genes. The F and G proteins are responsible for the cellular attachment and viral entry into host cell [4]. The virus is endemic in about 8 percent bats spread across at least 9 states of India like Kerala, Karnataka, Tamil Nadu, Maharashtra, Bihar and West Bengal. It is also seen in bats in Puducherry, an Indian Union Territory. The present outbreak in Kerala this year has been due to the Bangladesh strain. Interestingly the present NiV strain has high mortality and consequently less communicability.
Epidemiology:
The disease has been named after the village “Kampung Sungai Nipah” in Malaysia in 1998, where it was first reported in pig farmers. This term actually means ‘by the side of the river Nipah’. It is believed that during the first outbreak, the infection spread to pigs from bats, and then to man. Pigs may have served as amplifying hosts of the virus. Fruit bats or flying foxes of genus Pteropus (especially Pteropuspoliocephalus) serve as reservoir hosts for the infection. Infection can also spread from man to man. Since the virus can survive well in substrates rich in sugar, like fruit pulp or date palm sap, consumption of contaminated fruit can be the cause behind infections. The infection follows approximately the ecological distribution of the Pteropus bats.
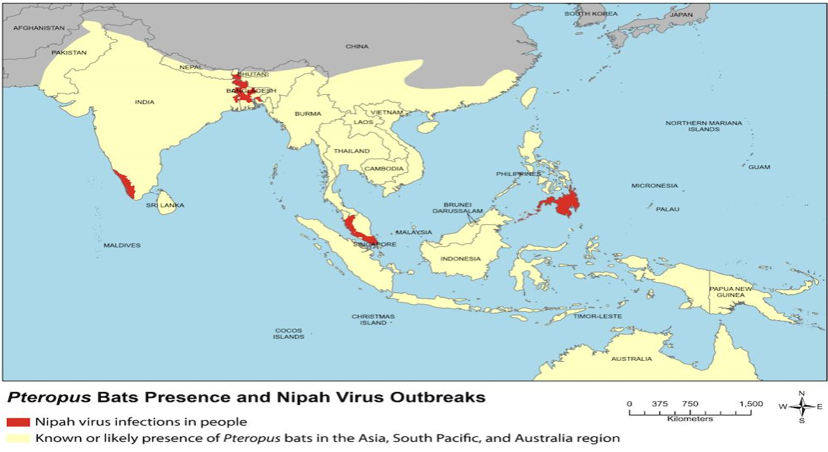
Figure 1. Presence of bats and Nipah outbreaks (source: - www.asm.org)
In Malaysia, after the initial infection, spread from man to man occurred in nosocomial setting. Since then, no outbreak has been reported from Malaysia. After 1998, cases were reported in Singapore. In fact, between September 1998 and May 1999, there were about 300 cases and 100 deaths in Malaysia and Singapore [4]. Again, an outbreak was reported in Bangladesh in 2001, and after that from India in 2004 and 2007 (Siliguri and Nadia in West Bengal, respectively) and then in Kerala. In 2004 Siliguri there were 66 cases and 45 deaths, while in Nadia a smaller outbreak was reported with 5 cases and all of them died (100% mortality). In the 2001 Siliguri outbreak, about 75
Clinical features
The incubation period of the infection is about 4 to 14 days with a usual maximum incubation period of 21 days. However, an incubation period of as long as 45 days has also been reported. The virus enters via nostrils into lungs, and from there it spreads to spleen, kidney and the brain. There is initially fever, headache, malaise, nausea and vomiting followed by seizures and unconsciousness. Features of encephalitis set in within a week, with commonest symptoms being altered mental state, segmental myoclonus, areflexia, hypotonia, gaze palsy and limb weakness [9]. Usually, human infection presents as an encephalitic syndrome marked by fever, headache, drowsiness, disorientation, mental confusion, coma, and potentially death. Sequelae like personality changes, depression and memory loss are seen in about 20% of the survivors. Features like fatigue and focal neurological deficits are also seen. Case fatality rate is about 40-70%. The lesser communicability of the virus may be due to its high case fatality. Some differences have bene found in Malaysian and Indo-Bangladesh strains as regards clinical features. A higher mortality rate has been found in India and Bangladesh (70%) when compared to Malaysia (40%). Respiratory illness is found in approximately 70% of patients in India and Bangladesh whereas no significant respiratory involvement was encountered in Malaysia.
Pathogenesis:
Initially the virus multiplies in the lymphoid and respiratory organs after entry. The glycoprotein G of NiV binds to the cellular receptor Ephrin-B2 and sometimes receptor Ephrin-B3, which are expressed in high levels in the brain, followed by lungs, placenta, prostate, and blood vessels in various other tissues [9]. This receptor distribution is the reason behind the clinical and pathological features seen in NiV infection. Ephrin-B2 plays a very important role in the migration of neuron precursors during embryogenesis. So, it is highly conserved between different classes of animals and the receptor similarity with bats and pigs is almost 95–96%. This explains the wide host range found with NiV. The central nervous system is infected primarily via the haematogenous route, although evidence of direct invasion through olfactory nerves has been found in pigs. The high mortality of NiV can be due to its evasion of the innate immune response. The P gene products of the virus can inhibit interferon activity [9].
Laboratory diagnosis:
Early diagnosis of NiV infection can be very challenging owing to the non-specific early symptoms of the infection in man. However, early detection and diagnosis are still crucial to increase the chances of survival among infected persons, to prevent onward transmission to other hosts, and also to manage outbreak response efforts [1]. Samples like nasopharyngeal swab, serum, urine and CSF (Cerebrospinal fluid) can be obtained for Laboratory diagnosis of Nipah virus infections. Specimens for serological testing should be collected later in the course of infection, about 10–14 days after onset of first symptoms. The NCDC, India, recommends throat swabs in viral transport medium, urine, blood, and CSF as acceptable samples for diagnosis. Samples must be collected safely and then transported in triple container packaging at 2–8 °C [9]. ELISA can be used for screening, but scientists rely on RT-PCR for confirmation (real time reverse transcriptase PCR). ELISA has got less specificity. The source of antigen in ELISA to detect IgM and IgG Nipah-specific antibodies in patients’ sera, is the Nipah virus culture on Vero CCL-81 cell line. Whole genome sequencing can also be used for definitive diagnosis. Swabs from contaminated fruits can also be tested for presence of the virus, as has been done in Kerala this time around. In India, Niv testing facilities are present in NIV, Pune and also in Kerala in 2 places, Kozhikode as well as at the Virology Institute at Thonnakkal [5].

Figure 2: Martaban/martaman Bananas which are at high risk of being contaminated with NiV. (Image courtesy: - authors and Miss Ankita Halder).
Data Extraction
Nipah Virus (NiV) has been classified as a biosafety level 4 or Risk Group 4 pathogen, which implies that specimens containing the virus are to be handled using special containment and barrier precaution measures [10].
Vigilance and containment measures: -
- Caution has to be exercised for a period of 42 days after the first case (twice the maximum incubation period). Isolation of the cases are needed and imposition of strict containment measures may be necessary. Contacts should be traced and tested.
- Health workers should adopt personal protective equipment like mask and gloves. This year in Kerala strict containment measures and lockdown were also carried out to curb the spread of cases.
- Date sap collection facilities using bamboo sticks, and wells should always be covered.
- Contact with sick animals should be avoided.
Treatment: - There is no specific treatment for Nipah virus infections. A monoclonal antibody m102.4 has shown some efficacy in 50-60
Prevention
A clinical trial has been launched by The National Institute of Allergy and Infectious Diseases (NIAID), for development of a vaccine against infection with Nipah virus [12]. This trial which is at a very early stage involves an experimental vaccine that is manufactured by Moderna, Inc., Cambridge, Massachusetts, USA. The vaccine is based on a messenger RNA (m-RNA). NIAID was sponsoring the Phase 1 clinical study, being run at the NIH (National Institutes of Health) Clinical Center in Bethesda, Maryland. However, at present there is no approved vaccine against Nipah virus infection. In India, a vaccine against this virus is under consideration by the Indian Council of Medical Research (ICMR) [13]. General precautions like hand washing, physical distancing and protective masks can help in preventing transmission of Nipah Virus cases. One should wear personal protective equipment while coming in contact with cases and infected animals [13]. Additionally, many methods have been occasionally used successfully by date palm sap collectors to restrict access of bats to date palm trees and sap [15].
Conclusion
Nipah virus is a zoonotic virus that can also spread from man to man. Proper suspicion of the cases and a concerted one health approach can go a long way in controlling the spread of cases.
Acknowledgement
The authors would like to acknowledge the help received from Miss Ankita Halder, MSc. Applied Nutrition student, AIIH&PH, Kolkata for sending pictures of the martaman bananas.
References
- Nipah Virus
View at Publisher | View at Google Scholar - Nipah Virus.
View at Publisher | View at Google Scholar - Conroy G. Nipah virus outbreak: what scientists know so far.
View at Publisher | View at Google Scholar - What You Need to Know About Nipah Virus.
View at Publisher | View at Google Scholar - Nipah cases detected belong to Bangladesh strain: Minister. https://www.thehindu.com/news/national/kerala/nipah-cases-detected-belong-to-bangladesh-strain-minister/article67302575.ece. last accessed 25.09.23.
View at Publisher | View at Google Scholar - Banerjee S, Gupta S, Kodan P, Mittal A, Ray Y, Nischal N, et al. Nipah virus disease: A rare and intractable disease. Intractable Rare Dis Res 2019; 8(1): 1–8.
View at Publisher | View at Google Scholar - Nipah Virus.
View at Publisher | View at Google Scholar - Nipah Virus.
View at Publisher | View at Google Scholar - Aditi, Shariff M. Nipah virus infection: A review. Epidemiol Infect. 2019 Jan;147: e95.
View at Publisher | View at Google Scholar - Factsheet on Nipah virus disease.
View at Publisher | View at Google Scholar - Bossart KN, Geisbert TW, Feldmann H, Zhu Z, Feldmann F, Geisbert JB, et al. A neutralizing human monoclonal antibody protects African green monkeys from Hendra virus challenge. Sci Transl Med. 2011;3(105):105ra103.
View at Publisher | View at Google Scholar - NIH launches clinical trial of mRNA Nipah virus vaccine
View at Publisher | View at Google Scholar - Kaul R. ICMR considers developing vaccine against Nipah
View at Publisher | View at Google Scholar - Stay Safe from Nipah Virus: Effective Prevention Strategies.
View at Publisher | View at Google Scholar - Luby SP, Gurley ES, Hossain MJ. TRANSMISSION OF HUMAN INFECTION WITH NIPAH VIRUS. In: Institute of Medicine (US). Improving Food Safety Through a One Health Approach: Workshop Summary. Washington (DC)
View at Publisher | View at Google Scholar - National Academies Press
View at Publisher | View at Google Scholar
