

Research | DOI: https://doi.org/10.31579/2835-835X/099
Newborn of a diabetic mother result of investigation at the neonatology department of Constantine University Hospital “6-month retrospective study”
- S Hadjit, *
- R Bourgheda
- MT Tercha
- N Zerrouki
- H Boumaraf
lecturer B in Pediatrics.
*Corresponding Author: S Hadjit, lecturer B in Pediatrics.
Citation: S Hadjit, R Bourgheda, MT Tercha, N Zerrouki, H Boumaraf, (2025), World Class Iraqi Pediatric Experiences: Bridging Modern Excellence with Mesopotamian Legacy, Clinical Trials and Case Studies, 4(1); DOI:10.31579/2835-835X/099
Copyright: © 2025, S Hadjit. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 November 2024 | Accepted: 11 December 2024 | Published: 13 January 2025
Keywords: diabetes; pregnancy; macrosomia; neonatal complications
Abstract
Introduction: Infants born to “NDM” diabetic mothers are exposed to a significantly higher risk of perinatal morbidity and mortality. The objective of this study is to describe the epidemiological aspect of NDM, evaluate the morbidity of NDMs and identify the main maternal and neonatal risk factors.
Materials And Methods: Retrospective survey with a descriptive and analytical aim of NDMs hospitalized in the neonatology department CHU Constantine from 01/01/22 to 30/06/22. Newborns died were excluded from the study.
Results: Among 4135 births surveyed, 321 (7.76%) cases of NDM. 90% gestational diabetes, 7.7% chronic diabetes and 2 cases of corticosteroid-induced diabetes. Associated maternal pathologies: pregnancy-related hypertension15.9%, chronic hypertension 7.2%, preeclampsia 5.2%, dysthyroidia 5.3%, urogenital infection 4.6% and Antiphospholipid syndrome 1.9%. 95% of pregnancies monitored 78.1 % high births. 55.1% male cases, 74.2 full-term born, 25.8% premature, 76% had a birth weight between 2500-4000g. 93.7ù NDMs admitted at an age <48H for: respiratory distress 30.9%, infection (maternal-fetal, nosocomial) 14.3%, jaundice 14%, IUGR 11.5%, macrosomia 10.2%, perinatal asphyxia 4.7%, malformation syndrome 4%, hypoglycemia 3.1%, hemorrhagic syndromes 2.5% and 2% hypertrophic cardiomyopathy. The average length of hospitalization was 6.5 days.
Conclusion: NDM remains a child at risk. Efforts must be focused on balancing maternal diabetes. Thus, improving maternal-fetal prognosis will require the involvement of a multidisciplinary team before conception, during pregnancy and childbirth, and postpartum.
Introduction
Babies born to diabetic mothers are exposed to a significantly higher risk of numerous complications: congenital malformation, perinatal mortality, prematurity, macrosomia, fetal trauma, respiratory distress, metabolic disorders (hypoglycemia, hypocalcaemia, hyperbilirubinemia, etc.) [1-2].
The prognosis of these newborns can be improved thanks to better management based on pregnancy programming with normoglycemic conception and rigorous monitoring by multidisciplinary collaboration [2].
Objective
Describe the epidemiological aspect of newborns of diabetic mothers (NDM).
Evaluate the morbidity of NDM.
Identify the main maternal and neonatal risk factors.
Materials and Methods
Retrospective survey with a descriptive and analytical aim of NDMs hospitalized in our department from 01/01/22 to 30/06/22, using a pre-established form which provides information on the characteristics of newborns maternal history, the progress of pregnancy and childbirth.
Deceased newborns are excluded from the study. The statistical analysis of the collected data was done using Excel.
Results
Among 4135 births surveyed, 321 (7.76%) cases of NDM.
1.1. Characteristics of mothers
1.1.1. Maternal diabetes
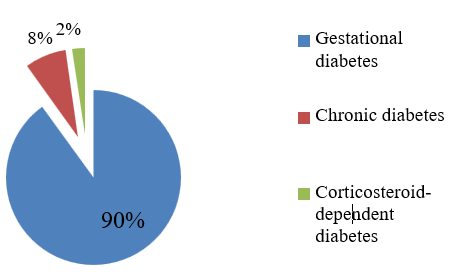
Figure 1: Distribution of the population accordingto maternal diabetes
1.1.2. Associated maternal pathologies
| Anti-phospholipid syndrome | 1.9 |
| urogenital infection | 4.6 |
| Dysthyroidism | 5.3 |
| Preeclampsia | 5.2 |
| Chronic hypertension | 7.2 |
| Pregnancy-induced hypertension | 15.9 |
Figure 2: Distribution of the population according to maternal pathologies
1.1.3. Course of pregnancy and childbirth
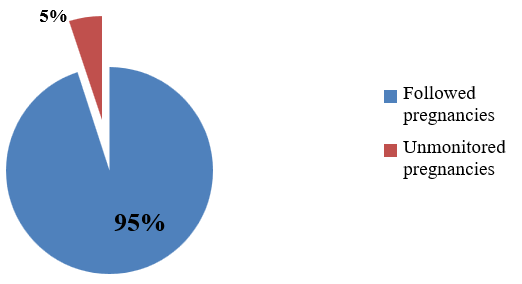
Figure 3: Distribution of the population according to pregnancy monitoring
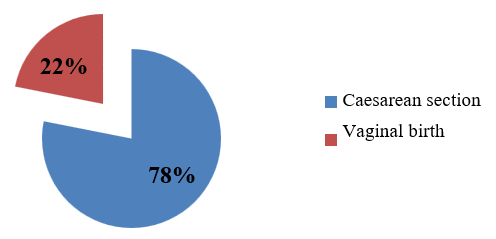
Figure 4: Distribution of the population according to route of delivery
1.2 Characteristics of newborns
- Gestational age
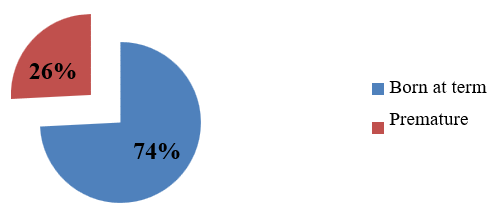
Figure 5: Distribution of the population according to gestational age
1.2.2. Birth weight
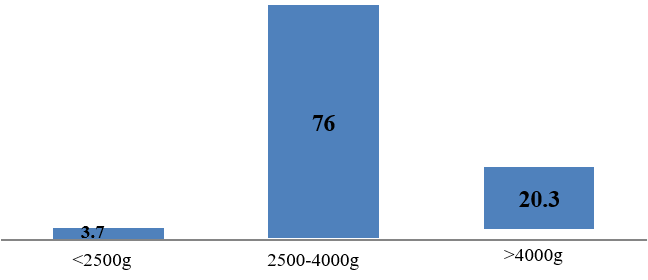
Figure 6: Distribution of the population according to birth weight
1.2.3. Sex
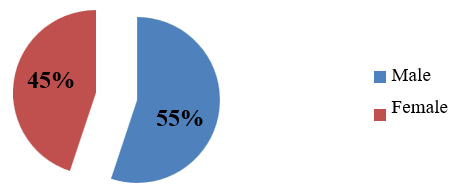
Figure 7: Distribution of the population according to sex
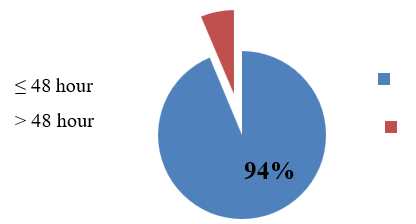
Figure 8: Distribution of the population according to age of hospitalization
1.2.5. Causes of hospitalization
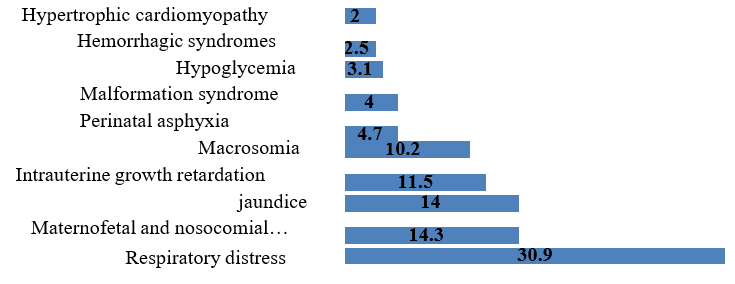
Figure 9: Distribution of the population according to causes of hospitalization
1.2.6. Length of hospitalization
The length of hospitalization varied from 1 to 21 days with an average stay of 6,5 days.
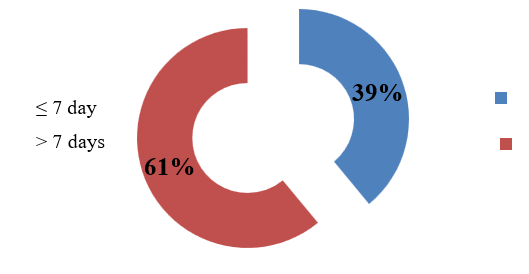
Figure 10: Distribution of the population according to length of hospitalization
Results
Among 4135 births surveyed, 321 (7.76%) cases of NDM.
1.1. Characteristics of mothers
1.1.1. Maternal diabetes
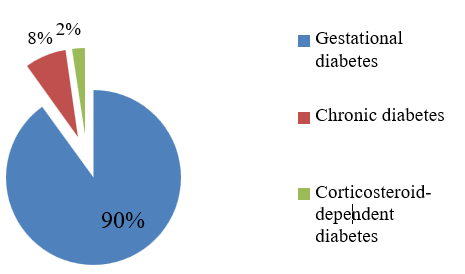
Figure 1: Distribution of the population accordingto maternal diabetes
1.1.2. Associated maternal pathologies
| Anti-phospholipid syndrome | 1.9 |
| urogenital infection | 4.6 |
| Dysthyroidism | 5.3 |
| Preeclampsia | 5.2 |
| Chronic hypertension | 7.2 |
| Pregnancy-induced hypertension | 15.9 |
Figure 2: Distribution of the population according to maternal pathologies
1.1.3. Course of pregnancy and childbirth
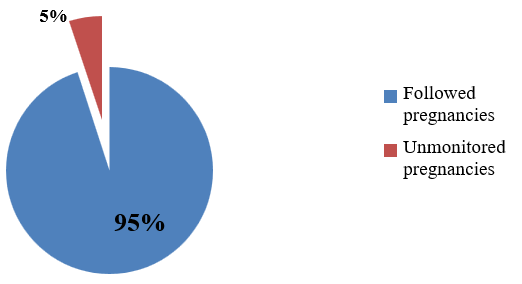
Figure 3: Distribution of the population according to pregnancy monitoring
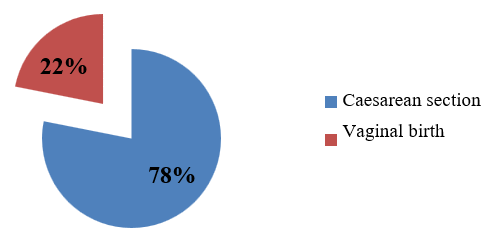
Figure 4: Distribution of the population according to route of delivery
1.2 Characteristics of newborns
- Gestational age
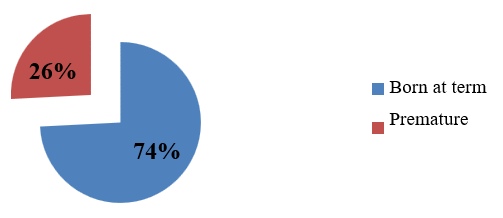
Figure 5: Distribution of the population according to gestational age
1.2.2. Birth weight
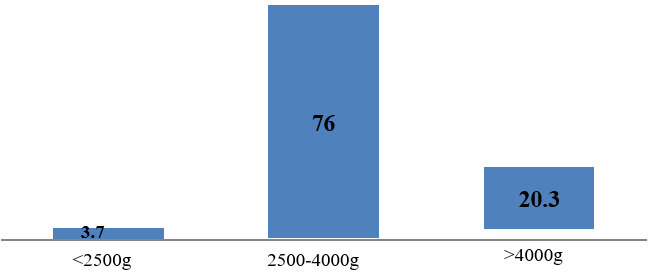
Figure 6: Distribution of the population according to birth weight
1.2.3. Sex
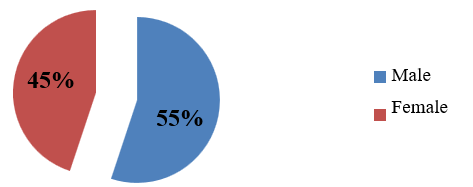
Figure 7: Distribution of the population according to sex
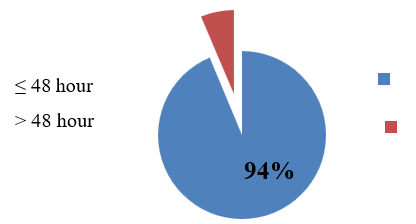
Figure 8: Distribution of the population according to age of hospitalization
1.2.5. Causes of hospitalization
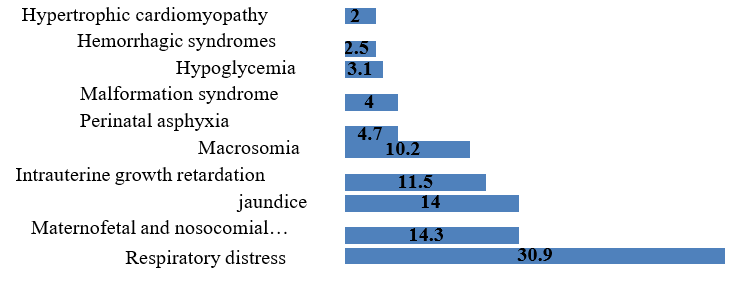
Figure 9: Distribution of the population according to causes of hospitalization
1.2.6. Length of hospitalization
The length of hospitalization varied from 1 to 21 days with an average stay of 6,5 days.
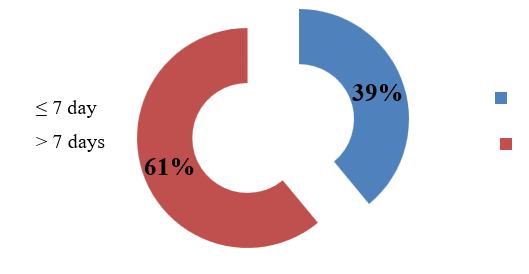
Figure 10: Distribution of the population according to length of hospitalization
Discussion
Diabetes constitutes a major public health problem worldwide. The incidence of diabetes during pregnancy is constantly increasing in the current context of the obesity and non insulin-dependent diabetes pandemic. Around 3 to 10% of pregnancies are marked by a glycemic regulation disorder [2-3]. The frequency during pregnancy in our series is 7.7%, close to that reported in the literature.
The cesarean rate is 78.1%, it seems that knowledge of diabetes in parturients influences delivery methods, the increase in the cesarean rate had already been reported by other authors: Abdelmoneim (84%) [4], Peace Opara et al (80%) [5] and Boiro et al (87,8%) [6].
Among neonatal complications, macrosomia is one of the most common with a high incidence of 45% [2]. In the case of maternal diabetes, macrosomia is classically attributed to fetal hyperinsulinism reactive to maternal hyperglycemia [7], due to the anabolic effect of insulin, in our study represents 10.2%.
The frequency of prematurity during diabetic pregnancy is increasingly increased (23-26%) [8], ours corroborates this (25.8%). The main associated factors are poor glycemic control and the occurrence of eclampsia [8-9]. In the study of Cordero et al in the USA, the rate of prematurity was 14?fore 34 weeks [10].
NDMs are usually at greater risk of developing neonatal respiratory distress. Three causes are possible: prematurity, surfactant maturation abnormalities and cesarean births which increase the risk of respiratory distress due to delayed resorption of pulmonary fluid [9,11].
Hypoglycemia was predominant and significantly secondary to macrosomia, as was poor maternal glycemic control peripartum [2-3].
The prevalence of congenital malformations varies between 2 and 7% in the literature [1]. Cordero et al, report 5% of congenital malformations [10]. The risk is higher in patients with pre-gestational diabetes but the malformations described in gestational diabetes are similar to those reported in pre-gestational diabetes: cardiac, skeletal and cerebral [2,9,11]. Our study reports a 4% rate of congenital malformations.
Conclusion
NDM remains a child at risk. Efforts must be focused on balancing maternal diabetes. Indeed, the existence of pre-gestational diabetes is the factor most associated with neonatal complications. Thus, improving maternal-fetal prognosis will require the involvement of a multidisciplinary team before conception, during pregnancy and childbirth, and postpartum.
Expression of interest
The authors declare that they have no conflict of interest relating to this article.
References
- Mitanchez D (2010). Particularités de la prise en charge du nouveau-né de mère avec diabète gestationnel. Environnement pédiatrique. J Gynécologie Obstétrique Biol Reprod. 2010 ;39:S281–8.
View at Publisher | View at Google Scholar - Saint-Faust M, Simeoni U (2012). Devenir des enfants nés de mère diabétique. Médecine Mal Métaboliques. 2012; 6:300–4.
View at Publisher | View at Google Scholar - Senouci H, Benomeur . K (2017). Nouveau né de mère diabétique] [Thesis].
View at Publisher | View at Google Scholar - Kheir AE, Berair R, Gulfan IG, Karrar MZ, Mohammed ZA (2012). Morbidity and mortality amongst infants of diabetic mothers admitted into Soba university hospital, Khartoum, Sudan. Sudan J Paediatr. 2012; 12:49.
View at Publisher | View at Google Scholar - Opara PI, Jaja T, Onubogu UC (2010). Morbidity and mortality amongst infants of diabetic mothers admitted into a special care baby unit in Port Harcourt, Nigeria. Ital J Pediatr. 2010; 36:77.
View at Publisher | View at Google Scholar - Boiro D, Guéye M, Seck N, Ndongo AA, Thiongane A, Niang B, et al (2017). Les nouveau-nés de mère diabétique au service de néonatologie du chu de Dakar (Sénégal). J Pédiatrie Puériculture. 2017 ;30:150–5.
View at Publisher | View at Google Scholar - VAMBERGUE A, BARNAS A, LANGLOIS C, DERUELLE P (2014). Le métabolisme des lipides au cours de la grossesse diabétique : Endocrinopathies et grossesse. Métabolisme Lipides Au Cours Grossesse Diabét Endocrinopathies Grossesse. 2014; 18:111–6.
View at Publisher | View at Google Scholar - Lepercq J, Timsit J (2005). Diabètes préalables à la grossesse : complications périnatales. Arch Pédiatrie. 2005;12:763–5.
View at Publisher | View at Google Scholar - Mimoso G, Oliveira G (2017). Morbilidade Neonatal na Diabetes Gestacional: Coincidência ou Consequência do Consenso de 2011. Acta Médica Port. 2017 ;30:589–98.
View at Publisher | View at Google Scholar - Cordero L, Treuer SH, Landon MB, Gabbe SG (1998). Management of infants of diabetic mothers. Arch Pediatr Adolesc Med. 1998 ;152:249–54.
View at Publisher | View at Google Scholar - Prakash GT, Das AK, Habeebullah S, Bhat V, Shamanna SB (2017). Maternal and Neonatal Outcome in Mothers with Gestational Diabetes Mellitus. Indian J Endocrinol Metab. 2017;21:854–8.
View at Publisher | View at Google Scholar
