

Research Article | DOI: https://doi.org/10.31579/2835-8147/046
Neuroprotective Effects of Vitamin D Supplementation on Outcomes in Traumatic Brain Injury: A Systematic Review and Meta-Analysis
- Fatemeh Vosoughian 1,8*
- Mahdi Mehmandoost1 1,8*
- Hengameh Yousefi 2
- Amirmohammad Bahri 3
- Khatere Mokhtari 4
- Tohid Emami-Meybodi 5,8
1Student Research Committee, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Student Research Committee, School of Medicine, Islamic Azad University, Kerman Branch, Kerman, Iran
3Student Research Committee, School of Medicine, Iran University of Medical Science, Tehran, Iran
4Department of Cell and Molecular Biology and Microbiology, Faculty of Biological Science and Technology, University of Isfahan, Isfahan, Iran
5Neuroscience Research Center, Iran University of Medical Sciences, Tehran, Iran
6School of Medicine, Alborz University of Medical Sciences, Karaj, Iran
7Neurology Department, Tehran university of medical sciences, Tehran, Iran
8Functional Neurosurgery Research Center, Research Institute of Functional Neurosurgery, Shohada Tajrish Neurosurgical Center of Excellence, Shahid Beheshti University of Medical Sciences, Tehran, Iran
9Physical Medicine and Rehabilitation resident, Functional Neurosurgery Research Center (FNRC), Shahid Beheshti University of Medical Science
10Microbiology student, at Tehran’s Azad University of Medical Science
11Neurosurgery resident in Shohade-E-Tajrish Hospital, Functional Neurosurgery Research Center (FNRC), Shahid Beheshti University of Medical Science
*Corresponding Author: Farzan Fahim, Functional Neurosurgery Research Center, Research Institute of Functional Neurosurgery, Shohada Tajrish Neurosurgical Center of Excellence, Shahid Beheshti University of Medical Sciences, Tehran, Iran, Neurosurgery resident in Shohade-E-Tajr
Citation: Farzan Fahim, Fatemeh Vosoughian, Mahdi Mehmandoost, Hengameh Yousefi, Amir Mohammad Bahri, et al, (2025), Neuroprotective Effects of Vitamin D Supplementation on Outcomes in Traumatic Brain Injury: A Systematic Review and Meta-Analysis, Clinical Research and Reviews, 4(4); DOI:10.31579/2835-8147/046.
Copyright: © 2025, Farzan Fahim. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 June 2025 | Accepted: 14 July 2025 | Published: 25 August 2025
Keywords: traumatic brain injury; vitamin D; vitamin E; neuroprotection; systematic review; meta- analysis
Abstract
Background:
Traumatic brain injury (TBI) remains a leading cause of morbidity and mortality worldwide, with secondary brain damage driven by inflammation and oxidative stress. Vitamin D is increasingly recognized for potential neuroprotective effects in TBI, while data regarding vitamin E remain limited.
Objective:
To systematically review and meta-analyze the effects of vitamin D supplementation, and qualitatively review evidence for vitamin E, on clinical and functional outcomes after moderate to severe TBI.
Methods:
A comprehensive search was carried out in PubMed, Scopus, Embase, Web of Science, and Google Scholar up to January 2025. Studies reporting on vitamin D or E supplementation in clinical TBI were eligible. Risk of bias was assessed using JBI checklists. A meta-analysis of randomized controlled trials reporting pre- and post-treatment GCS scores following vitamin D supplementation was performed with a fixed-effect model.
Results:
From 4,546 records, nine clinical studies met criteria; three RCTs on vitamin D (n=151 patients) were included in the meta-analysis, which found that vitamin D supplementation significantly improved GCS scores versus controls (SMD = 1.02, 95% CI: 0.68-1.36, p < 0.0001; I² = 0%). Narrative analysis suggested that vitamin D may improve functional outcomes, reduce inflammatory biomarkers, and lower mortality in select studies. Evidence for vitamin E in TBI is currently limited to a small number of heterogeneous studies, with early data suggesting possible benefits for acute recovery and oxidative stress reduction, but insufficient for quantitative synthesis.
Conclusion:
Vitamin D supplementation may confer short-term improvement in neurological and functional outcomes following moderate to severe TBI. Existing evidence for vitamin E is insufficient to support robust conclusions. Larger, rigorously designed RCTs particularly for vitamin E are required to clarify effectiveness, optimal dosing, and long-term outcomes.
Introduction
Traumatic brain injury (TBI) is a major public health concern and remains one of the leading causes of morbidity, mortality, and long-term disability worldwide, affecting nearly 69 million people annually, particularly in low- and middle-income countries [1, 2]. The primary mechanical impact is followed by complex secondary injury cascades, characterized by neuroinflammation, oxidative stress, and disruption of blood–brain barrier function—all of which contribute to further neuronal loss and neurological deterioration [3-5]. Severity assessment and monitoring of prognosis in TBI are typically performed using the Glasgow Coma Scale (GCS), a widely used tool for both clinical care and research [3]. A growing body of evidence highlights the pivotal roles of inflammatory cytokines and oxidative stress markers—including TNF-α, IL-1β, and IL-6—in determining the severity and outcomes of TBI [6, 7]. Despite advances in acute care, options for modulating secondary brain injury and improving patient prognosis remain limited, driving interest in novel therapeutic strategies [8, 9]. Among potential interventions, antioxidant vitamins have gained considerable research attention. Vitamin D, beyond its classical roles in calcium homeostasis, has demonstrated immunomodulatory, anti- inflammatory, and neuroprotective effects in both pre-clinical and clinical studies [10-12]. Animal studies indicate that vitamin D supplementation can attenuate cerebral edema, lower oxidative damage, and improve neuronal recovery after TBI [13, 14]. Human studies further suggest that vitamin D deficiency is common after TBI, and lower serum vitamin D levels may be associated with increased risk of unfavorable outcomes [15-17]. Early phase clinical trials have shown that vitamin D supplementation improves neurological function, reduces inflammatory markers, and may decrease duration of mechanical ventilation and ICU stay in patients with moderate to severe TBI [18-22], although methodological heterogeneity and small sample sizes limit definitive conclusions. Vitamin E, a fat-soluble antioxidant, is another candidate neuroprotectant investigated mostly in animal models, where it has been shown to reduce lipid peroxidation and improve functional and cognitive outcomes after TBI [15, 23]. However, clinical evidence for vitamin E supplementation in TBI remains sparse and heterogeneous, mostly limited to small-scale studies and those employing combination antioxidant regimens [24, 25]. A few randomized trials suggest vitamin E may reduce acute oxidative stress and possibly mortality, but the overall quality and consistency of available human data are low [24, 25]. Despite these promising findings, major gaps persist in the literature. Most studies are limited by small sample sizes, lack of standardization in dosing and timing of supplementation, and inadequate reporting of long-term and patient-centered outcomes. Notably, while there is more robust data for vitamin D, evidence for clinical efficacy of vitamin E remains insufficient for meta-analytic synthesis [24, 25]. However, despite encouraging preliminary evidence, robust data from large-scale randomized controlled trials are still lacking. Critical questions remain regarding optimal dosing, timing of supplementation, ideal target populations, long-term functional outcomes, and the comparative efficacy of vitamin D versus vitamin E in TBI. Addressing these important gaps is essential for developing clear, evidence-based clinical recommendations. Therefore, the present systematic review and meta-analysis aims to (i) quantitatively evaluate the effects of vitamin D supplementation on neurological and clinical outcomes in TBI patients, and (ii) provide a qualitative synthesis of current evidence for vitamin E supplementation. By identifying strengths, limitations, and future research directions, this study seeks to clarify the therapeutic potential of these antioxidants in the management of TBI.
Methods
Study Design and Registration
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The study protocol was prepared a priori and registered in PROSPERO (Registration ID: 1088575).
Information Sources and Search Strategy
A comprehensive search was performed in PubMed, Scopus, Embase, Web of Science, and Google Scholar, covering records from database inception until January 31, 2025. The search strategy combined Medical Subject Headings (MeSH) and relevant free-text keywords related to vitamin D, vitamin E, traumatic brain injury (TBI), prognosis, functional recovery, and management. The full search strategy for each database is available in Supplementary Table S1. In addition, the reference lists of all included articles and relevant reviews were screened to identify further eligible studies.
Eligibility Criteria
Studies were included if they:
• Enrolled human participants;
• Investigated the effects of vitamin D and/or vitamin E supplementation (including relevant MeSH terms);
• Reported clinical or functional outcomes for adult TBI patients (such as Glasgow Coma Scale [GCS], Glasgow Outcome Scale [GOS/GOS-E], mortality, ICU/hospital stay, or inflammatory/oxidative biomarkers);
• Were published as English-language, full-text original articles.
Studies were excluded if they:
• Were animal or in vitro investigations, case reports, conference abstracts, reviews, meta-analyses, protocols, or editorials;
• Focused exclusively on other vitamins without separate data for vitamin D or E;
• Lacked extractable or relevant outcome data.
Study Selection
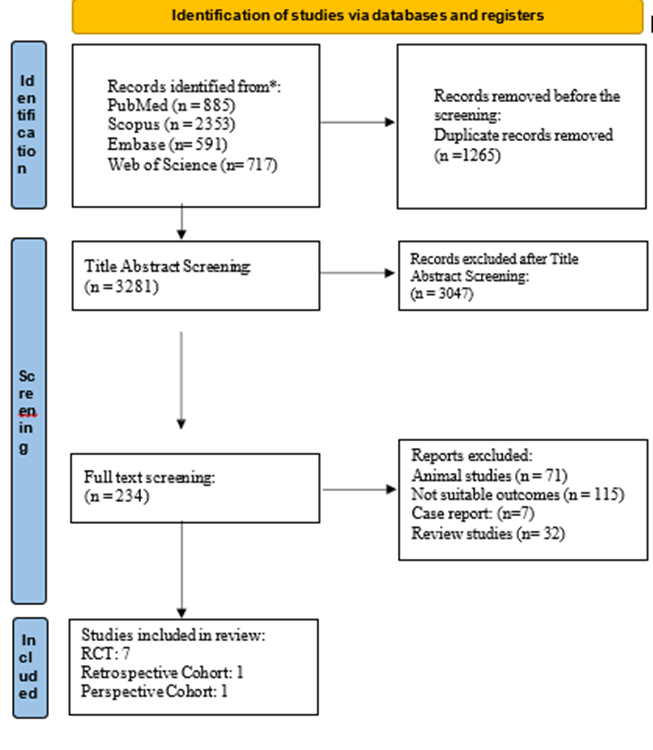
Duplicate records were removed using EndNote, and the remaining unique articles were imported into Rayyan for title and abstract screening by two independent reviewers. Full texts of potentially eligible studies were then retrieved and assessed according to the inclusion and exclusion criteria. Discrepancies at any stage were resolved by consensus or, if necessary, by consultation with a third reviewer. The study selection process is illustrated in the PRISMA flow diagram (Figure 1).
Data Extraction
Two reviewers independently extracted data using a standardized, pilot-tested data extraction form. The following variables were collected: first author, year, country, study design, sample size, patient demographics (age, sex, TBI severity), intervention details (supplement type, dose, route, duration), comparator(s), relevant clinical outcomes (GCS, GOS/GOS-E, mortality, hospital and ICU stay, mechanical ventilation duration, biomarkers, adverse events), follow-up, funding sources, and reported conflicts of interest. Any discrepancies in data extraction were resolved through discussion or, if necessary, adjudication by a third reviewer.
Risk of Bias Assessment
Study Num of positive answers
Num of negative answers
Num of partial/unclear answers
Study Num of positive answers
Num of negative answers
Num of partial/unclear answers
Final status
Sharma et al. 2020 | 12 | - |
| 1 | Low |
Razmkon et al. 2011 | 7 | 2 |
| 4 | Low |
Arabi et al. 2020 | 5 | 4 |
| 2 | Moderate |
Aminmansour et al. 2012 | 10 | 1 |
| 2 | Low |
Zhang 2018 | 8 | - |
| 5 | Low |
Masbough et al. 2024 | 8 | 1 |
| 4 | Low |
Shafiei et al. 2022 | 11 | - |
| 2 | Low |
|
|
| Cohort studies |
|
|
Lee et al. 2019 | 8 | - |
| 3 | Low |
Guan et al. 2017 | 9 | 1 |
| 1 | Low |
Each included study was independently assessed for risk of bias by two reviewers using the appropriate Joanna Briggs Institute (JBI) Critical Appraisal Checklist: the JBI checklist for randomized controlled trials for RCTs and the JBI checklist for cohort studies for cohort designs. Disagreements were resolved through consensus or a third reviewer. No study was excluded based on high risk of bias. The risk of bias assessments are summarized in Table 1.
The risk of bias assessment JBI Critical Appraisal checklists
Data Synthesis and Statistical Analysis
A quantitative meta-analysis was performed for randomized controlled trials (RCTs) that reported pre- and post-intervention GCS scores in vitamin D and control groups. Standardized mean differences (SMD) with 95% confidence intervals (CIs) were calculated. Given the low degree of observed heterogeneity (I²< 25>
Robustness of findings was evaluated by leave-one-out sensitivity analyses. Publication bias was assessed through funnel plot inspection and Egger’s regression test. Where data permitted, meta-regression was conducted to assess the influence of age and sex on outcome effect sizes.
All statistical analyses were performed using R (version 4.4.2) with the “meta” and “metafor” packages. For vitamin E supplementation, due to insufficient and heterogeneous evidence, only a qualitative synthesis was conducted.
Outcomes Primary outcome:
• Change in Glasgow Coma Scale (GCS) following vitamin D or E supplementation.
Secondary outcomes:
• Glasgow Outcome Scale (GOS or GOS-E);
• Mortality;
• Duration of ICU stay, hospital stay, and mechanical ventilation;
• Inflammatory and oxidative stress biomarkers;
• Safety and adverse effects.
Ethics
No ethics approval was required for this systematic review and meta-analysis as only previously published, de-identified data were used.
Results
Study Selection
A total of 4,546 records were identified through database searching. After removal of 1,265 duplicates, 3,281 unique articles were screened by title and abstract using Rayyan. Of these, 28 articles were assessed in full text, and nine studies were included in the final analysis (Figure 1).
Study Characteristics
Nine studies, including six randomized controlled trials and three cohort studies, were published between 2011 and 2024. Sample sizes ranged from 35 to 497 participants. Most studies assessed vitamin D supplementation (oral or intramuscular, with doses ranging from 50,000 to 300,000 IU), while two studies examined vitamin E (intramuscular or intravenous). TBI severity ranged from moderate to severe (admission GCS scores 3–12). Participants were predominantly male (approximately 70–80%), with ages primarily between 30 and 50 years. Full study details are provided in Table 1.
Risk of Bias
The Joanna Briggs Institute (JBI) Critical Appraisal checklists showed most studies to be at low risk of bias, with two studies assessed as moderate due to incomplete blinding or outcome reporting (Table 1).
Quantitative Synthesis (Meta-Analysis)
Three randomized controlled trials [18, 21, 22] (n=151; intervention: 78, control: 73) reported change in Glasgow Coma Scale (GCS) and were included in the meta-analysis. The pooled standardized mean difference (SMD) for GCS improvement with vitamin D versus control was 1.02 (95% CI: 0.68 to 1.36, p
< 0 xss=removed xss=removed xss=removed xss=removed>
(estimate = 0.021, p = 0.701) or female proportion (estimate = 16.319, p = 0.178) on treatment outcome
(Table 2, Supplementary Figure S1).
Functional and Clinical Outcomes
Glasgow Outcome Scale (GOS/GOS-E):
Vitamin D-sufficient patients demonstrated higher rates of favorable GOS at 3 and 6 months post-TBI (17), and Lee et al. (19) observed more patients achieving GOS-E ≥6 in the supplemented group at both timepoints. Masbough et al. (20) found that vitamin D increased odds of favorable GOS-E at three months (P = 0.017). In Razmkon et al. (24), vitamin E led to higher GOS at discharge (P = 0.04); differences faded by later follow-up.
Mortality:
Lower mortality was observed in the vitamin E group in Razmkon et al. [24] (P = 0.04), and Shafiei et al.
[21] reported a lower (but not statistically significant) mortality with vitamin D. Adjunctive vitamin D with progesterone decreased mortality compared to progesterone alone or placebo [18].
Secondary Outcomes
Mechanical Ventilation and ICU/Hospital Stay:
Vitamin D significantly reduced mechanical ventilation duration (Sharma et al.: 6.19 ± 1.64 vs. 9.07 ±
2.18 days, P < 0 xss=removed>
Readmission and Complications:
Vitamin D-sufficient patients experienced lower 30-day readmission (9.5% vs. 13.7%) and hospital- acquired pneumonia (5.0% vs. 13.6%) [17].
Inflammatory and Oxidative Biomarkers:
Vitamin D reduced IL-6, TNF-α, and IL-2, and increased IFN-γ in Sharma et al [22]. Masbough et al. [20] noted a significant reduction in neutrophil-to-lymphocyte ratio (NLR). Vitamin E (Zhang et al. [25]) reduced markers of oxidative stress (NTF-κB, OH , O , MDA, AOPP) and nerve injury (NSE, S100B), with increased antioxidant enzymes (SOD, GPx, CAT).

Human (Number of each group, sex, age) | Total N=497 neurosurgery patients (12.1?used by trauma)
Deficientvit D (12-20 ng/ml): n=182(F=77, age M=49.5) Traumatic patients: n=24 (13.2%)
Sufficientvit D: n=315(F=148, age M=58)Traumatic patients: n=36 (11.4%)
Severely Deficient vit D (lessthan 12 ng/ml): n= 59 (F=30, age M=48.9) Traumatic patients: n=12 (20.3%) | N=35 F=28.6%, M=71.4% Age=16-65,Mean age =36.4y Treatment, n=20 Placebo, n=15 | Total N=100 F=17 M= 83 Mean age = 31.6 y (16-83)
Group A (Low-Dose Vitamin C), n=26
Group B (High-Dose Vitamin C), n=23
Group C (Vitamin E), n=24 mean age: 36.8 (16-73) F=4 M=20
Group D (Placebo), n=27 | ||||||
based GCS | Not mentioned | Mean pre-GCS: Case=7.09 ± 2.21 Control=6.28± 2.36
First day meansGCS: Case:7.00 ± 2.14 Control: 5.66 ± 1.82 | Admission GCS meanTotal= 6.3 Group C (Vit E) = 6.5 | ||||||
operation/ non-operation, details | 103 (56.6%) deficient patients and 200 (63.5%) sufficient patients had surgery during NCCU stay. | 62.8% of patients underwent surgery | All of the patients received intracranial pressure management. | ||||||
Severity of Trauma(GCS) | At the 3-monthfollow-up, 34.6% (N=63)of deficient and 25.1% (N=79) of sufficient groups had lower GOS score (1-3).
At the 3-month follow-up, 65.4% (N=119) of deficient and 74.9% (N=236) of sufficient groups had higher GOS scores(4-5). | Seventh day meansGCS. Treatment=12.63 ± 1.42 Placebo=8.72 ± 1.84 | Not mentioned | ||||||
Treatment (Dose, taper, placebo) Vitamin E, D | Those who were found to be vitamin D deficient were treated with 50,000 U of ergocalciferol orally or via feeding tube weekly. | The treatment group regimen consists of a 120,000 IU single dose of vitamin D, and the control group regimen includes 8 mg of saccharide as a placebo. | Group A, low-dose vitamin C (500 mg/d IV) for 7 days;
Group B, high-dose vitamin C (10 g IV on thefirst [admission] day and repeated on the fourthday, followed by vitamin C 4 g/d IV for the remaining 3 days); Group C, vitaminE (400 IU/dIM) for 7 days; Group D, placebo | ||||||
The duration of treatment and followup | Vitamin D treatment continued during the hospital stay.
3 months of follow-up visits in the clinic | Single-dose treatment, and follow-up after 7 days of treatment. | Treatment for 7 days and follow-up at 2 months and 6 months after discharge. | ||||||
Findings Effects on prognosis and Outcomes and efficacy
|
1.2) A sufficient group had a lower admission rate after30 days of discharge (9.5% vs 13.7%)
1.1) Deficient group werelikely to havelower GOS scores(1-3) than sufficient group (34.6% vs 25.1%).
2.1) Severely deficient patients had a higher rateof hospital pneumonia than other patients (13.6%vs 5.0%). 2.1) At 3-month follow-up, Low GOS Score group had been more likely to be vitamin d deficient (44.5% vs33.5%), staying longer in the NCCU (5.3±6.5 vs 3.2±4.1 days) and overall hospital stay (9.1±10.5 vs 5.7±5.5 days), longer dependent on mechanical ventilation(2.9±6.6vs0.7±3.2 days), developing urinary tract infection (12%5.1%)or pneumonia(13.4%vs3.1%)
Overall, the study suggests that patients admitted to the NCCU without vitamin D deficiency were more than 1.7 times more likely to achieve a GOS score of 4 or 5 (moderate or low disability) than those who were deficient in vitamin D. | 2.1) Seven days after admission, the GCS score elevated by about 3.86 units whiledecreasing by 0.19units in the control group.
The length of mechanical ventilation and ICU stay was lower in the treatment group (6.19 vs 9.07 days).
The GOSEscore was higher in the vitamin D group.
The pre-intervention vitamin D level in the case group was 18.30, which rose to 39.15 post-intervention by day 7.
2.2) Thevitamin D level in thecontrol group was 15.15 before the intervention and reached 27.30 by day 7 after the intervention. |
The significant impactof vitamin E is strongest at discharge, and that the difference decreases at 2 months and decreases furtherat 6 months of follow-up.
The numberof patients in a vegetative state (GOS 2) was higher in the vitamin E group. | ||||||
ESR/CRP/Albmin | None. | Diminished levelsof Cytokines such as IL-6, TNF-α, IL-2, and enhanced levelsof IFN-γ werenoted in the vitamin D group, contrary to the placebo. | Not mentioned | ||||||
Limitations | Single institution Weak to detect subtle GOS Score in different groups, differences in neurological condition of patients, disability in assessing one-third of patients' GOS Score at the 3- month follow-up not evaluating the vitamin D levelafter discharge. They suggest that future research would be improved by including measurements of vitamin D levels at follow-up afterthe patients haveleft the hospital. not blinding the assessment of the GOSScore and vitaminD level | Small sample size, dominant male patients, short-term follow-up | The authors claimed to have chosen an imprecise secondary oxidative index of the brain injury. The perilesional edemamay be affected by oxygenation, vascular sufficiency, and other uncontrollable factors. They also mentioned the lack of advanced monitoring methods (except the intraventricular intracranial pressure monitoring). Small sample size | ||||||
Seyed Mostafa Arabi | Jong Min Lee1 | Bahram Aminmansour | Cheng Zhang | ||||||
2020 | 2019 | 2012 | 2018 | ||||||
randomized control trial | Retrospective study | randomized clinical trial | RCT | ||||||
| * | * |
| ||||||
10.1186/s13063-020-04622-6 | 10.1016/j.wneu.2019.02.244 | 10.4103/2277-9175.100176 | 10.4103/2221-6189.233014 | ||||||
N=74 Age=18-65 | N=345 Control, n=64 Age=55.91y, Male=53
Supplement, n=180 Age=56.76y, Male=132 | N=60 Placebo, n=20, male =12 (60%) GCS mean= 6.3 ±0.88, Progesterone, n=20 male=16 (80%) GCS mean =6.31 ± 0.87 Progesterone-vitamin D, n=20 male=16 (80%) GCS mean =6 ± 0.88 | N: 84 intervention group:42 F= 14 M=28 Age M= 25 to 49 years control group:42 F= 13 M=29 Age M= 25 to 49 years | ||||||
(GCS 7–8 and 8–9) |
Control group GCS=12.36 Supplement group GCS=13.14 | Progesterone=6.3 Progesterone + vit D=6 Placebo=6.3 | GCS= 3-12 points | ||||||
Not mentioned | Not mentioned | 45% of placebo patients, 40% of progesterone +vit D patients, 30% of progesterone patients had surgical procedure. | Not mentioned | ||||||
Study protocol and results have not been published | GOS score Control=6.81 Supplement=7.16 | Placebo = 9.16 ± 1.11, Progesterone =10.25± 1.34, Progesterone-vitamin D= 11.27 ± 2.27 | Not mentioned | ||||||
The experimental group received 100,000 IU of vitamin D as an oral drop, and the control group 1000 IU of vitamin D as a placebo daily for 5 days. | If a patient had a vitamin D deficiency (less than 30 ng/mL), Cholecalciferol was immediately injected at 100,000 IU intramuscularly; If oral medication were possible on the day following intramuscular injection, 0.5 mg/day of Alfacalcidol was also administered | The progesterone group received 1 mg/kg of progesterone intramuscularly every 12 hours for 5 days, The progesterone-vitamin D group received 1 mg/kg of progesterone intramuscularly every 12 hours for 5 days and 5 µg/kg of vitamin D daily for 5 days. The placebo group received both placebos intravenously. | Patients in the intervention group were given a large dose of vitamin C and vitamin E based on the above routine treatment: 1st-4th day, Vitamin C 4.0 g, intravenous drip, 2 times a day; 5th-7th day, vitamin C 3.0 g, intravenous drip, 2 times a day; Vitamin E 100 mg, muscle injection, 1 time a day were given for the first 7 days. | ||||||
Treatment 5 days Follow up day 5-28 | Single injection 1 week and 3 months post-TBI follow-up | Five-days treatment 3-month follow-up | 7-day treatment | ||||||
The study protocol and results have not been published | 1.1) Mean vitamin D level in 345 patients At admission were 13.62 ng/ml. There was no correlation between the initial vitamin D level and GOS-E in all TBI patients. During the first week, there was no significant variation in GOS-E score between the control and the supplement groups in all kinds of TBI severity.
2.1) However, at the three-month follow-up, the supplement group had a higher GOS-E score than the control group. The same results were achieved for the Mini-Mental Status Examination (MMSE) and Clinical Dementia Rating (CDR) score as cognitive outcomes.
Patients with total TBI and mild-to-moderate TBI who received supplements exhibited greater functional recovery at the 3-month follow-up compared to the control group. Notably, the supplementation regimen did not impact the recovery rate, as measured by the GOS-E score, among patients with severe TBI.
Serum levels of vitamin D significantly increased from 14.03 ng/mL at admission to 37.42 ng/mL at 3 months post-TBI in the supplement group(P<0> Thus, the increase in the Serum level of vitamin D was greater in the supplement group than in the control group (P <0> 2.2) Vitamin level changed from 13.57 ng/mL at admission to 16.77 ng/mL at 3 months post-TBI (P=0.021) in the control group. | 2.1) 3 months after the intervention, there was a significant variation among the GCS means of the 3 groups with the dominance of progesterone-vitamin D group (P-value = 0.001). The recovery rate based on the GOS score in the progesterone-vitamin D group was higher than the other groups. There was a significant difference in mortality among the groups, with a lower rate in the progesterone- vitamin D group than in the other groups. | 2.1) Analysis on the 3rd and 7th days post-treatment revealed that the intervention group exhibited significantly reduced levels of several biomarkers associated with nerve injury (NSE, S100B, NGB, UCH-L1), iron metabolism (Tf, Ft), and oxidative stress (NTF-κB, OH , O , MDA, AOPP) compared to the control group. Conversely, the intervention group demonstrated significantly elevated serum concentrations of antioxidant enzymes (SOD, GPx, and CAT) at these time points.
Administering high doses of vitamin C and vitamin E appears to be a therapeutic strategy for patients with acute craniocerebral injury, potentially mitigating nerve damage, reducing oxidative stress, and enhancing neurotrophic support. | ||||||
Study protocol and results have not been published | Not mentioned | Not mentioned | Not mentioned, | ||||||
| |||||||||
Chemiluminescence method for measuring vitamin D instead of the gold standard technique, Potential blood transfusion and albumin injection in some patients interfere with the biochemistry test. The potential need for surgery other than brain surgery in patients, this factor could affect the study outcomes. | The supplement group was approximately three times larger than the control group.
The control group had twice the number of patients involved in car accidents as drivers, which could negatively impact functional outcomes due to the diffuse nature of such injuries.
The educational levels of the two groups differed, which could have affected cognitive outcomes. | Small sample size Single-center study | None. | ||||||
| The exclusion of mortality cases, which accounted for a significant portion of severe TBI patients (40%), could have influenced the reported outcomes for the severeTBI and total TBI groups. |
|
| ||||||
Table 2: Characteristics of Included Studies
Covariate | No. of Studies | Estimate | Estimate SE | P Value | R² | τ² | I² |
Age | 3 | 0.021 | 0.0544 | 0.701 | 0 | 0.094 | 44.258 |
Female | 3 | 16.319 | 12.125 | 0.178 | 100 | 0 | 0 |
Table 3: Meta-regression results for the influence of age and gender on GCS outcomes
Farnoosh Masbough | Sajjad Shafiei |
2024 | 2022 |
RCT | RCT |
|
|
10.30476/ijms.2023.99465.3156. | |
N: 35 (vitamin D3 level less than30 ng/ml) | N: 84 |
Age 18-65 | interventiongroup (n=42) |
| F=12 M=30 |
Intervention:19 | Age M= 36.76±16.12 |
F=1 M=18 | control group (n=42) |
Age M= 37.68±13.39 | F=9 M=33 |
control groups:16 | Age M= 41.92±16.79 |
F= 3 M=13 |
|
Age M= 38.12±15.11 |
|
between 3 to 12 | GCS<13> Interventional group: 8.64±2.29 Placebo group: 8.42±2.93 |
Not mentioned. | Not mentioned. |
The mean GCSin the vitaminD group was statistically increased (P=0.001). | Interventional group: 13.50±1.85 Placebo group: 10.97±2.37 |
a single IM dose of 300,000 IU of vitaminD3 | oral singledose (150,000 units)of vitamin D and the placebo upon admission. |
Single dose 3-month follow-up | Single dose 3-month follow-up |
2.1) Analysis of GOS-E scores at three months revealed a statistically significant improvement in the vitamin D3 group compared to the control group (P=0.017) (five times more likely than the control group) | The GCS upon discharge significantly improved in both groups. 2.1) The mean GCS was significantly higherin the intervention group compared to the controls. The t-test indicated no significant differences between the intervention and control groups regarding the duration of mechanical ventilation (13.62±13.87 days vs. 16.42±12.33 days) and the mean length of hospital stay (19.37±13.24 days vs. 22.67±13.39 days). |
Not mentioned. | Not mentioned. |
single-center design | Small sample size |
Figure 2: Forest plot showing the standardized mean difference (SMD) in GCS scores between vitamin D-supplemented groups and control groups. A fixed-effect model was used due to low heterogeneity (I² = 0%).
Discussion
Summary of Main Findings
In this systematic review and meta-analysis, the efficacy of vitamin D and vitamin E supplementation in patients with traumatic brain injury (TBI) was assessed across nine studies, including six randomized controlled trials and three cohort studies published between 2011 and 2024. Quantitative synthesis of three RCTs demonstrated a significant benefit of vitamin D on neurological recovery, with a pooled SMD of 1.02 (95% CI: 0.68–1.36, p < 0 xss=removed>
Interpretation in the Context of Previous Research
The observed neurological improvement with vitamin D supplementation is consistent with findings from prior clinical and preclinical studies, which have suggested a role for vitamin D in modulating
neuroinflammation and promoting neurorecovery [17, 19-22]. The anti-inflammatory cytokine profile following vitamin D administration—including reduced IL-6, TNF-α, and IL-2 with increased IFN-γ [20, 22]—may help attenuate the secondary injury cascade, supporting previous reports of its neuroprotective effects [4, 7, 22]. Similarly, the positive impact of vitamin D on functional outcomes (as indicated by higher GOS/E scores) aligns with earlier evidence that adequate vitamin D status is associated with better post-TBI prognosis [17, 19]. Vitamin E demonstrated reductions in oxidative stress biomarkers (such as MDA, AOPP, NTF-κB) and neuronal injury markers (NSE, S100B), which concurs with its established antioxidative mechanisms [10, 11, 25]. The observed decrease in mortality in vitamin E groups [24] supports the hypothesis that antioxidant therapy may confer survival benefits in severe TBI, as previously reported in related translational studies [11]. Of note, adjunctive treatment with vitamin D and progesterone was associated with lower mortality compared to progesterone alone or placebo [18], suggesting potential synergistic effects, as also noted in experimental models [14, 26]. However, not all studies reported significant improvements in all outcomes, and variations in dosing, timing, and study population characteristics likely contributed to heterogeneity.
Clinical Implications
The present findings highlight the potential role of vitamin D supplementation—and to a lesser extent vitamin E—in improving neurological recovery and reducing complications following moderate-to-severe TBI. Considering the low risk profile and high prevalence of vitamin D deficiency among critically ill patients, routine screening and early correction may be considered as part of neurocritical care protocols [17, 22]. Nevertheless, current evidence does not yet support universal high-dose vitamin supplementation for all TBI patients; further individualized assessment remains necessary.
Limitations
Several limitations must be noted. The total number of high-quality randomized controlled trials remains limited, with only three studies comprising the meta-analysis of GCS outcomes. Sample sizes were small in several studies, reducing statistical power. There was heterogeneity in vitamin dosing regimens (ranging from 50,000 to 300,000 IU for vitamin D), modes of administration (oral, intramuscular, intravenous), and follow-up durations (most limited to three months or less). Some studies combined vitamin supplementation with other interventions (e.g., progesterone), complicating attribution of effects.
Risk of bias was generally low, but some studies had issues related to incomplete blinding or outcome reporting. Finally, publication bias cannot be entirely excluded, despite negative findings on formal testing (Egger’s test, funnel plot).
Future Directions and Conclusion
Larger, multicenter RCTs with standardized vitamin supplementation protocols, longer follow-up, and consistent outcome definitions are required to validate these findings and clarify long-term benefits. Research should also explore the potential for combination therapies (e.g., vitamin D with progesterone) and optimal patient selection.
In summary, evidence supports a beneficial effect of vitamin D—and possibly vitamin E—on early neurological recovery and some clinical outcomes following moderate-to-severe TBI, though routine use awaits confirmation in further high-quality studies.
Conclusion:
This systematic review and meta-analysis provide moderate-quality evidence that vitamin D supplementation, and possibly vitamin E, confer measurable benefits on early neurological recovery and selected clinical outcomes in patients with moderate-to-severe traumatic brain injury. Despite statistically significant improvements—particularly in Glasgow Coma Scale scores—across available randomized trials, the current evidence base is restricted by methodological heterogeneity, limited sample sizes, and predominantly short-term follow-up. Accordingly, while routine correction of vitamin D deficiency may be justified as part of comprehensive neurocritical care, universal high-dose supplementation cannot yet be broadly recommended. Further large-scale, rigorously designed clinical trials are warranted to clarify optimal dosing strategies, long-term efficacy, and potential synergistic effects with other neuroprotective agents.
Declarations
Ethical approval and consent to participate:
Not applicable
Consent for publication:
All authors approve this statement
Availability of data and materials:
Not applicable
Competing interests:
The authors have no competing interests.
Funding:
This study did not receive any financial support.
Author contributions
Conceptualization: F.V, Data curation: H.Y, M.M, Formal analysis: M.M, A.Z, Investigation: I.S, T.E,
K.M Methodology: K.M, A.B, Project administration: F.F, Writing – original draft: M.M, Sh.M, Sh.N, S.O, Writing – review and editing: F.V, A.Z.
Acknowledgements:
Not applicable
References
- Dewan MC, Rattani A, Gupta S, Baticulon RE, Hung YC. et al. (2019). Estimating the global incidence of traumatic brain injury. Journal of neurosurgery;130(4):1080-1097.
View at Publisher | View at Google Scholar - Guan B, Anderson DB, Chen L, Feng S, Zhou H. Global, regional and national burden of traumatic brain injury and spinal cord injury, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. BMJ open. 2023;13(10):e075049.
View at Publisher | View at Google Scholar - Basak D, Chatterjee S, Attergrim J, Sharma MR, Soni KD, Verma S, et al. Glasgow coma scale compared to other trauma scores in discriminating in-hospital mortality of traumatic brain injury patients admitted to urban Indian hospitals: A multicentre prospective cohort study. Injury. 2023;54(1):93-9.
View at Publisher | View at Google Scholar - Lozano D, Gonzales-Portillo GS, Acosta S, de la Pena I, Tajiri N, Kaneko Y, et al. Neuroinflammatory responses to traumatic brain injury: etiology, clinical consequences, and therapeutic opportunities. Neuropsychiatric disease and treatment. 2015;11:97-106.
View at Publisher | View at Google Scholar - Werner C, Engelhard K. Pathophysiology of traumatic brain injury. British journal of anaesthesia. 2007;99(1):4-9.
View at Publisher | View at Google Scholar - Morganti-Kossmann MC, Satgunaseelan L, Bye N, Kossmann T. Modulation of immune response by head injury. Injury. 2007;38(12):1392-400.
View at Publisher | View at Google Scholar - Woodcock T, Morganti-Kossmann MC. The role of markers of inflammation in traumatic brain injury. Frontiers in neurology. 2013;4:18.
View at Publisher | View at Google Scholar - Alexander MP. Mild traumatic brain injury: pathophysiology, natural history, and clinical management. Neurology. 1995;45(7):1253-60.
View at Publisher | View at Google Scholar - Bratton SL, Chestnut RM, Ghajar J, McConnell Hammond FF, Harris OA, Hartl R, et al. Guidelines for the management of severe traumatic brain injury. IX. Cerebral perfusion thresholds. Journal of neurotrauma. 2007;24 Suppl 1:S59-64.
View at Publisher | View at Google Scholar - Cao W, Carney JM, Duchon A, Floyd RA, Chevion M. Oxygen free radical involvement in ischemia and reperfusion injury to brain. Neuroscience letters. 1988;88(2):233-8.
View at Publisher | View at Google Scholar - Hall ED, Vaishnav RA, Mustafa AG. Antioxidant therapies for traumatic brain injury. Neurotherapeutics : the journal of the American Society for Experimental NeuroTherapeutics. 2010;7(1):51-61.
View at Publisher | View at Google Scholar - Tan Q, Wang Y, Zhang G, Lu B, Wang T, Tao T, et al. The metabolic effects of multi-trace elements on parenteral nutrition for critically ill pediatric patients: a randomized controlled trial and metabolomic research. Translational pediatrics. 2021;10(10):2579-93.
View at Publisher | View at Google Scholar - Lin AM, Fan SF, Yang DM, Hsu LL, Yang CH. Zinc-induced apoptosis in substantia nigra of rat brain: neuroprotection by vitamin D3. Free radical biology & medicine. 2003;34(11):1416-25.
View at Publisher | View at Google Scholar - Tang H, Hua F, Wang J, Yousuf S, Atif F, Sayeed I, et al. Progesterone and vitamin D combination therapy modulates inflammatory response after traumatic brain injury. Brain injury. 2015;29(10):1165- 74.
View at Publisher | View at Google Scholar - Aiguo W, Zhe Y, Gomez-Pinilla F. Vitamin E protects against oxidative damage and learning disability after mild traumatic brain injury in rats. Neurorehabilitation and neural repair. 2010;24(3):290- 8.
View at Publisher | View at Google Scholar - Chen G, Shi J, Qi M, Yin H, Hang C. Glutamine decreases intestinal nuclear factor kappa B activity and pro-inflammatory cytokine expression after traumatic brain injury in rats. Inflammation research : official journal of the European Histamine Research Society [et al]. 2008;57(2):57-64.
View at Publisher | View at Google Scholar - Guan J, Karsy M, Brock AA, Eli IM, Manton GM, Ledyard HK, et al. Vitamin D status and 3-month Glasgow Outcome Scale scores in patients in neurocritical care: prospective analysis of 497 patients. Journal of neurosurgery. 2018;128(6):1635-41.
View at Publisher | View at Google Scholar - Aminmansour B, Nikbakht H, Ghorbani A, Rezvani M, Rahmani P, Torkashvand M, et al. Comparison of the administration of progesterone versus progesterone and vitamin D in improvement of outcomes in patients with traumatic brain injury: A randomized clinical trial with placebo group. Advanced biomedical research. 2012;1:58.
View at Publisher | View at Google Scholar - Lee JM, Jeong SW, Kim MY, Park JB, Kim MS. The Effect of Vitamin D Supplementation in Patients with Acute Traumatic Brain Injury. World neurosurgery. 2019;126:e1421-e6.
View at Publisher | View at Google Scholar - Masbough F, Kouchek M, Koosha M, Salarian S, Miri M, Raoufi M, et al. Investigating the Effect of High-Dose Vitamin D3 Administration on Inflammatory Biomarkers in Patients with Moderate to Severe Traumatic Brain Injury: A Randomized Clinical Trial. Iranian journal of medical sciences. 2024;49(10):643-51.
View at Publisher | View at Google Scholar - Shafiei S, Zaheriani MS, Sahfizad M, Ehteshami S, Mosazadeh M, Haddadi K. Neuroprotective Effects of Vitamin D on Patients With Traumatic Brain Injury: A Clinical Trial. IrJNS. 2022;8(1):4
View at Publisher | View at Google Scholar - EP.
View at Publisher | View at Google Scholar - Sharma S, Kumar A, Choudhary A, Sharma S, Khurana L, Sharma N, et al. Neuroprotective Role of Oral Vitamin D Supplementation on Consciousness and Inflammatory Biomarkers in Determining Severity Outcome in Acute Traumatic Brain Injury Patients: A Double-Blind Randomized Clinical Trial. Clinical drug investigation. 2020;40(4):327-34.
View at Publisher | View at Google Scholar - Inci S, Ozcan OE, Kilinç K. Time-level relationship for lipid peroxidation and the protective effect of alpha-tocopherol in experimental mild and severe brain injury. Neurosurgery. 1998;43(2):330-5; discussion 5-6.
View at Publisher | View at Google Scholar - Razmkon A, Sadidi A, Sherafat-Kazemzadeh E, Mehrafshan A, Jamali M, Malekpour B, et al. Administration of vitamin C and vitamin E in severe head injury: a randomized double-blind controlled trial. Clinical neurosurgery. 2011;58:133-7.
View at Publisher | View at Google Scholar - Zhang C, Li J-M, Hu J-L, Zhou X. The effects of large doses of vitamin C and vitamin E on nerve injury, neurotrophic and oxidative stress in patients with acute craniocerebral injury. Journal of Acute Disease. 2018;7(2).
View at Publisher | View at Google Scholar - Cekic M, Sayeed I, Stein DG. Combination treatment with progesterone and vitamin D hormone may be more effective than monotherapy for nervous system injury and disease. Frontiers in neuroendocrinology. 2009;30(2):158-72.
View at Publisher | View at Google Scholar
