

Research Article | DOI: https://doi.org/10.31579/2834-796X/079
Mortality rate and initial type of care for peripheral arterial disease of the lower limbs in Brazil.
- Wagner Ramos Borges 1*
- Pedro Henrique Cordeiro Mota 2
- Alice Sarno Menezes 2
- Pedro Lucas Leal Pamponet Kuhn 2
- Breno Leal Mota Silva 2
- Sara Garcia Menezes 2
- Larissa de Araújo Regis 2
- Lucas Rodrigues Leite de Oliveira 2
- Matheus Oliveira Figueiredo 2
- Rafael Domingues Sampaio Menezes 2
- Maria Eliza Marchi 2
1 PhD in Medicine, Professor of Escola Bahiana de Medicina e Saúde Pública, full member Sociedade Brasileira de Angiologia e de Cirurgia Vascular e Colégio Brasileiro de Cirurgiões, Brazil
2 Escola Bahiana de Medicina e Saúde Pública, Applied Regional Anatomy Academic Monitoring, Brazil
*Corresponding Author: Wagner Ramos Borges, PhD in Medicine, Professor of Escola Bahiana de Medicina e Saúde Pública, full member Sociedade Brasileira de Angiologia e de Cirurgia Vascular e Colégio Brasileiro de Cirurgiões, Brazil.
Citation: Wagner R. Borges, Alice S. Menezes, Mota Silva BL, Sara G. Menezes, Larissa de Araújo Regis, et al, (2025), Mortality rate and initial type of care for peripheral arterial disease of the lower limbs in Brazil., International Journal of Cardiovascular Medicine, 4(1); DOI:10.31579/2834-796X/079
Copyright: © 2025, Wagner Ramos Borges. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 November 2024 | Accepted: 16 December 2024 | Published: 06 January 2025
Keywords: mortality; peripheral artery disease; urgency
Abstract
There is a therapeutic arsenal available to vascular surgeons for the treatment of peripheral arterial disease, but the associated lethality is not insignificant. The aim of this study was to evaluate the behavior of mortality rate and the initial type of care provided to these patients. This is an observational, retrospective and descriptive study of data available in the public health registry system in Brazil from 2004 to 2023. A total of 114,417 angioplasty interventions and 47,502 open revascularization interventions were documented. The records indicate that the absolute number of deaths associated with angioplasty reached 1,314, while for revascularization cases, this figure was 1,723. The lethality rate for the procedures was 1.3% and 3.4%, respectively. There was a predominance of urgent/emergency surgeries to the detriment of elective surgeries. Mortality rates were not insignificant for both surgeries, despite the predominance of a less invasive technique. Deficiencies in the recording of vascular health data have fragmented the accuracy of the data as well as exposing the reality, and further studies on the subject are needed.
Introduction
Cardiovascular diseases are the main cause of morbidity and mortality today. Atherosclerosis is the most important single causal factor and is characterized as a progressive multifactorial disease caused by genetic and acquired factors, with lipid accumulation and the development of fibrosis and obstruction in the arteries
Atherosclerosis, the morphological variant of arteriosclerosis, is a chronic, progressive and systemic process resulting from an inflammatory and fibro proliferative response that attacks the vascular endothelium. It is a multifactorial disease of civilization that increasingly affects younger people and is responsible for 95% of coronary heart disease, 85% of intermittent claudication of the lower limbs and 75% of strokes. For the lower limbs, it is believed to be underestimated due to the fact that the atherosclerotic process remains subclinical and asymptomatic for a long time, affecting 20% of people over the age of 70.
According to the Framingham study, the average annual incidence of symptomatic peripheral arterial disease is 26 per 10,000 men and 12 per 10,000 women, increasing with age (between the 6th and 7th decade of life). It affects more white people and is more common in diabetics. In general, the estimated incidence of peripheral arterial disease of the lower limbs is 500 to 1,000 new cases per million inhabitants per year. Among these patients, the primary amputation rate ranges from 10 to 40%. In those diagnosed with coronary disease, the presence of peripheral atherosclerotic disease is an independent risk factor for a fatal event, increasing this risk by 25%.
Peripheral arterial disease is the most common disease in vascular surgery, affecting 2% of people under 60 and 5% of those over 70. 90% are of atherosclerotic etiology, preferentially affecting arterial bifurcations and arterial attachment points such as the adductor canal. Conventional surgical treatment, characterized by revascularization with veins, has a patency rate of close to 70% and 50% when prostheses are used. When the graft fails and gangrene progresses, amputation is the only option.
Endovascular treatment is making rapid progress. In the iliac aortic territory, it has good results and is similar to open surgery in short (less than 3 cm), stenosing, concentric and non-calcified lesions. Morbidity and mortality are lower and it is therefore the first choice. In the infrapatellar territory, the indication is still restricted and amputation is still the last choice in this segment when gangrene progresses or revascularization attempts fail. [1,2,3,4,5]
Therefore, there is a therapeutic arsenal available to the vascular surgeon for the treatment of peripheral arterial disease of the lower limbs, but it is not insignificant that there is a mortality rate that significantly impacts the outcome of patients, and many are admitted at an advanced stage of the disease (already with ulceration or pain at rest), reducing the chance of cure as well as increasing the possibility of major amputation.
It is salutary to consider that endovascular techniques are associated with shorter hospital stays and seem to have a lower surgical risk, but the patency of angioplasties, stent thrombosis, the progression of atherosclerotic disease and reinterventions when compared to surgical treatment may reflect on the mortality rate, whether or not it is related to surgery or the patient's comorbidities.
Objective
To analyze mortality rates and the nature of care (elective or urgent/emergency) for peripheral arterial disease of the lower limbs in Brazil.
Materials and Methods
This is an observational, retrospective and descriptive study of secondary data extracted from the Brazilian hospital information system (DataSUS) on patients hospitalized between 2004 and 2023 with a documented diagnosis of chronic lower limb arteriopathy.
The data obtained was processed using Microsoft Excel software, where graphs were constructed for the data collected, which can be checked via the TabNet portal, at the following access link: https://datasus.saude.gov.br/.
The mortality rate of extremity angioplasty and proximal and distal femoral-popliteal revascularization between 2004 and 2023 was calculated by dividing the number of deaths by the number of inpatients listed in the health data system of the public health service in Brazil, which serves approximately 80% of the population. The number of hospitalized patients in the period corresponds to the number of patients with proven hospitalization in the health system. As the data, although audited, is not associated with a single electronic medical record that was not available at the beginning of the decade in Brazil, it is possible that there is repetition of procedures, mainly reintervention, in this figure.
The nature of care refers to the way in which the patient enters the Brazilian public health system. Urgency/Emergency is when the patient entered the Emergency Unit of any hospital in the public health network in the national territory and elective refers to when this entry took place via an outpatient clinic, i.e. it is not necessarily an emergency case.
This study used public health data made available by DATASUS, which is Brazil's health user data control system, and did not identify sensitive data, which is why it did not need to be analyzed by the ethics committee.
Results
Between 2004 and 2023, a total of 114,417 angioplasty interventions and 47,502 open revascularization procedures were documented in Brazil. The records indicate that the absolute number of deaths associated with angioplasty reached 1,314, while for revascularization cases this figure was 1,723. The mortality rate for these procedures was 1.3% and 3.4%, respectively.
There is a clear upward trend in angioplasties and a decrease in open revascularization surgeries. As for the number of deaths, there was an increase associated with angioplasty and a corresponding reduction for revascularization cases. Consequently, the mortality rate showed a downward trend in revascularization procedures (down from 4% in 2004 to 1.9% in 2023), to a greater extent than that observed in angioplasty (from 2.3% in 2004 to 1% in 2023), although the less invasive procedure still has a lower mortality rate.
In both surgeries, the emergency route was the predominant one. The average prevalence of emergency revascularization was 70% compared to the elective nature of the same procedure and in the case of angioplasty the average prevalence of emergency was 66%.
In the Southeast, there were a significant number of hospitalizations for both procedures, totaling 47,561 (41.2% of the total) for angioplasty and 23,730 (49.9% of the total) for revascularization. In absolute terms, there was a substantial 28-fold increase (from 389 to 10,939 over the period) in the number of angioplasty procedures over the period analyzed, while revascularization saw a 1.5-fold reduction, from 2,680 to 1,723. This is the most industrialized region of the country, with the highest socio-economic status, the largest proportion of the Brazilian population and the highest per capita income, as well as the largest number of hospitals and specialized professionals.
The mortality rate related to angioplasty showed a certain constancy over the years, while that related to revascularization showed a marked downward trend, from 4% in 2004 to 2% in 2023. With regard to the variation according to the type of care, it should be noted that the lethality rate for angioplasty procedures carried out in emergency situations was more than double (with a 2.3-fold disparity) that observed for elective procedures. Such a discrepancy was not seen in the revascularization sphere, which was characterized by minimal variation in this respect.
Angioplasties totaled 36,968, compared to 72,564 urgent procedures (a 66% preponderance of urgent procedures), while for open revascularization, elective procedures accounted for 9,714, compared to 23,320 urgent procedures (a 71% preponderance), showing urgency as the choice in both interventional contexts.
Considering the difference in the type of care provided, it can be seen that angioplasty performed in urgent situations has a mortality rate that is twice as high (1.39% in urgent cases and 0.65% in elective cases, revealing a disparity of 2.1 times) as that observed in elective procedures.
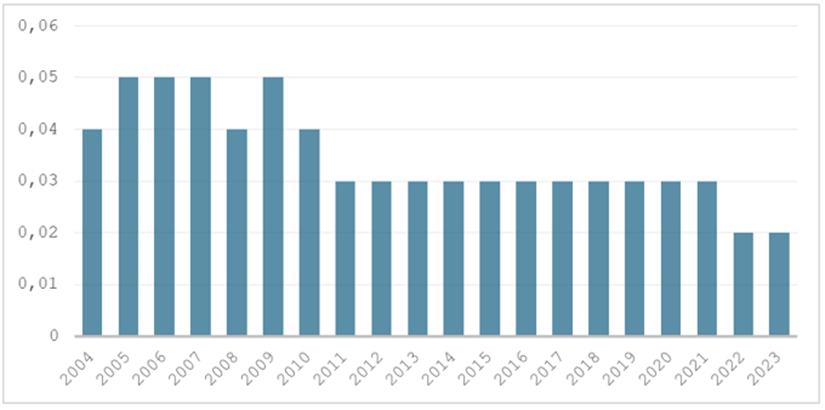
Table 1. Mortality rate associated with femoro-popliteal and distal thromboendarterectomy between 2004-2023.
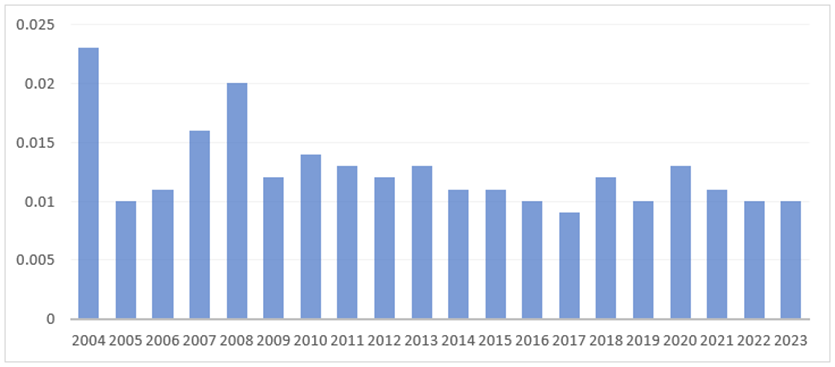
Table 2. Mortality rate associated with distal femoro-popliteal angioplasty between 2004-2023.
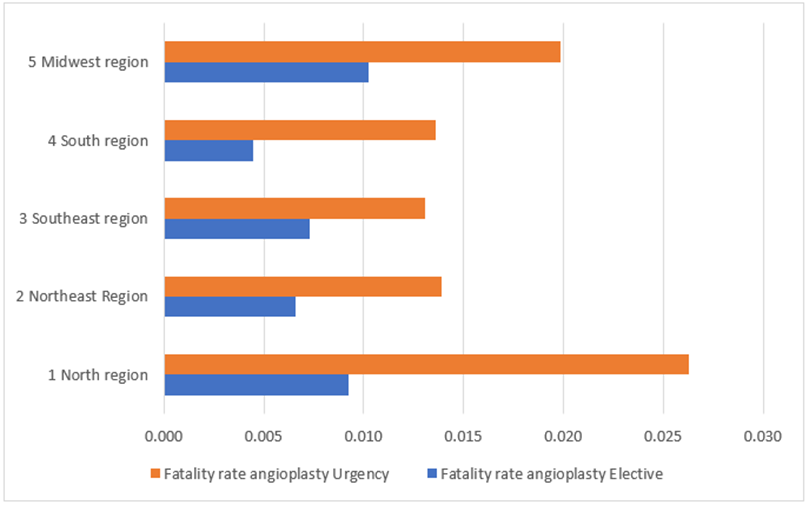
Table 3. Mortality rate according to the type of care associated with distal femoro-popliteal angioplasty between 2004-2023.
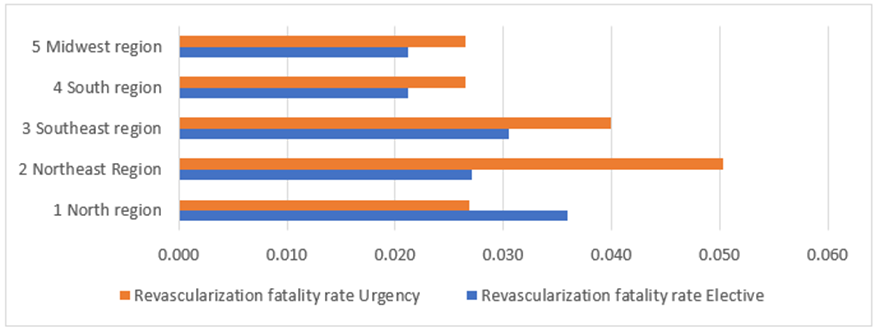
Table 4. Mortality rate according to the type of care associated with femoro-popliteal and distal endarterectomy thrombus between 2004-2023.
Discussion
The benefits of the best surgical technique chosen for the treatment of peripheral arterial disease are still being debated in a context in which minimally invasive procedures, whether exclusively endovascular or hybrid, are gaining ground and conventional surgery is progressively reducing in number, either because of the greater surgical risk inherent in the surgical technique or because of the patient's comorbidities.
In both situations, mortality rates are not insignificant. Over the last 30 years, angioplasty has grown and become significantly more common than open revascularization, twice as often. One explanation for this pattern could be the choice of a less invasive intervention measure, especially for high-risk patients, the main target group for surgical intervention, less bleeding, shorter hospital stays and the possibility of adding a hybrid technique. [6.7.8]
However, the reintervention rate for endovascular procedures is higher. This is because angioplasty, with or without a balloon, has a variable patency over time depending on the type of material used and the vascular territory treated. These reinterventions are expressed in the higher number of angioplasty procedures seen in the results, since readmission for surgery was not specified in the data analysis. [9.10]
Surgical techniques may present a greater risk of complications, but they have greater patency and, when associated with the endovascular technique, seem to be a good option for higher risk patients. Surgery brings with it greater exposure to surgical complications, but we must not forget the greater frequency of infections with arterial substitutes, as well as greater bleeding and the availability/viability of vascular substitutes. [11,12,13,14]
In both techniques, the mortality rates (3.4% vs. 1.3%) are not only due to the procedure itself but also to associated comorbidities such as hypertension, diabetes mellitus, dyslipidemia, coronary artery disease, chronic or acute kidney disease, infections and others.
It is clear that there is a predominance of emergency care in the cases presented. Even though peripheral arterial disease can remain asymptomatic for a long time, we observed a low efficiency of the Brazilian health system because patients are treated surgically in more advanced stages of the disease (Fontaine III or IV – Fontaine classification for pefipheral artery disease), showing that there is underreporting, lack of diagnosis or late diagnosis, and/or public policies for early diagnosis and intervention.
Also noteworthy is the simplicity of recording procedures, making it impossible to analyze cases in detail. There is no distinction between the extent of the disease treated (femoral, popliteal, infrapatellar or distal femoro-popliteal or femoro-popliteal), all of which are classified as femoro-popliteal diseases. There was also a lack of specificity about the procedure performed, and it was not possible to know if there were hybrid procedures or if there were repeated procedures due to readmissions, mainly due to infection or failure of revascularization.
There is no specific cause of death in the public health data registry. This is extremely serious because patients with arteriopathy usually have other pathologies and cardiovascular disease is the main cause of death.
Conclusion
Endovascular procedures seem to have become the first choice (endovascular first) for the treatment of peripheral arterial disease of the lower limbs in Brazil, to the detriment of open techniques which have decreased over the last 30 years, but mortality rates are not insignificant.
There is a lack of data on vascular medical importance in the Brazilian public health registry system (DATASUS), so more studies are needed, including intervention studies, to corroborate the findings suggested in this analysis.
Conflict of interest
The authors declare no conflict of interest.
References
- Lacroix P, Aboyans V, Desormais I, Kowalsky T, Cambou JP, Constans J, Rivière AB: (2013). Chronic kidney disease and the short-term risk of mortality and amputation in patients hospitalized for peripheral artery disease. J Vasc Surg 58: 966–971.
View at Publisher | View at Google Scholar - Couto M, Figueróa A, Sotolongo A, Pérez R, Ojeda JM: (2015). Endovascular Intervention in the Treatment of Peripheral Artery Disease. Bol Asoc Med P R 107:47–51.
View at Publisher | View at Google Scholar - Pobehová J, Spak L, Pobeha P, Joppa P, Sabol F, Frankovičová M: (2014). Comparison of the results of surgical and endovascular treatment in patients with peripheral arterial disease of the lower extremities in the femoropopliteal region. Rozhl Chir 93: 416–423.
View at Publisher | View at Google Scholar - Smith AD, Hawkins AT, Schaumeier MJ, de Vos MS, Conte MS, Nguyen LL: (2016). Predictors of major amputation despite patent bypass grafts. J Vasc Surg 63: 1279–1288.
View at Publisher | View at Google Scholar - Rand T, Lammer J, Rabbia C, Maynar M, Zander T, Jahnke T, Müller-Hülsbeck S, Scheinert D, Manninen HI: (2011). Percutaneous transluminal angioplasty versus turbostatic carbon-coated stents infrapopliteal arteries: InPeria II trial.Radiology 261:634–642.
View at Publisher | View at Google Scholar - Farber A. (2018). Chronic Limb-Threatening Ischemia. New England Journal of Medicine. Jul 12;379(2):171–180.
View at Publisher | View at Google Scholar - Schanzer A, Conte MS. (2010). Critical limb ischemia. Vol. 12, Current Treatment Options in Cardiovascular Medicine. p. 214–229.
View at Publisher | View at Google Scholar - Farber A, Menard MT, Conte MS, Kaufman JA, Powell RJ, Choudhry NK, et al. (2022). Surgery or Endovascular Therapy for Chronic Limb-Threatening Ischemia. New England Journal of Medicine. Dec 22;387(25):2305–2316.
View at Publisher | View at Google Scholar - Tunis SR, Bass EB, Steinberg EP. (1991). The Use of Angioplasty, Bypass Surgery, and Amputation in the Management of Peripheral Vascular Disease. New England Journal of Medicine. Aug 22;325(8):556–562.
View at Publisher | View at Google Scholar - Becker F, Robert-Ebadi H, Ricco JB, Setacci C, Cao P, de Donato G, et al. (2011). Chapter I: Definitions, Epidemiology, Clinical Presentation and Prognosis. European Journal of Vascular and Endovascular Surgery. Dec;42:S4–12.
View at Publisher | View at Google Scholar - Nehler MR, Duval S, Diao L, Annex BH, Hiatt WR, Rogers K, et al. (2014). Epidemiology of peripheral arterial disease and critical limb ischemia in an insured national population. J Vasc Surg. Sep;60(3):686-695.e2.
View at Publisher | View at Google Scholar - Conte MS. (2010). Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) and the (hoped for) dawn of evidence-based treatment for advanced limb ischemia. J Vasc Surg. May;51(5):69S-75S.
View at Publisher | View at Google Scholar - Rooke TW, Hirsch AT, Misra S, Sidawy AN, Beckman JA, Findeiss LK, et al. (2011). ACCF/AHA Focused Update of the Guideline for the Management of Patients With Peripheral Artery Disease (Updating the 2005 Guideline). J Am Coll Cardiol. 2011 Nov;58(19):2020–2045.
View at Publisher | View at Google Scholar - Bradbury AW, Moakes CA, Popplewell M, Meecham L, Bate GR, Kelly L, et al. (2023). A vein bypass first versus a best endovascular treatment first revascularisation strategy for patients with chronic limb threatening ischaemia who required an infra-popliteal, with or without an additional more proximal infra-inguinal revascularisation procedure to restore limb perfusion (BASIL-2): an open-label, randomised, multicentre, phase 3 trial. The Lancet. May;401(10390):1798–1809.
View at Publisher | View at Google Scholar
