

Research Article | DOI: https://doi.org/10.31579/2835-835X/023
Meta-Analysis of the Effectiveness and Safety of Ciprofol versus Propofol for Induction of Anesthesia
1 Department of Pharmacy, Yongchun County Hospital, Fujian;
2 Department of Pharmacy, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital;
3 Department of Anesthesiology, Fujian Provincial Hospital, Shengli Clinical Medical College of Fujian Medical University, Fuzhou, People’s Republic of China;
4 Fujian Provincial Institute of Emergency Medicine, Fujian Provincial Key Laboratory of Emergency Medicine, Fujian Provincial Key Laboratory of Critical Medicine, Fujian Provincial Co-constructed Laboratory of “Belt and Road”, Fuzhou, People’s Republic of China.
*Corresponding Author: : Xiaochun Zheng, Diagnosis and Treatment Center „Dr Victor Babes”, Bucharest, Romania
Citation: Huaiyuan Wang, Xiaoxia Wei, Yanlan Feng, Zhenzhen Yang, Yanling Liao, et al, (2023), Meta-Analysis of the Effectiveness and Safety of Ciprofol Versus Propofol for Induction of Anesthesia, Clinical Trials and Case Studies, 2(2); DOI:10.31579/2835-835X/023
Copyright: Huaiyuan Wang, Xiaoxia Wei, Yanlan Feng, Zhenzhen Yang, Yanling Liao, et al, (2023), Meta-Analysis of the Effectiveness and Safety of Ciprofol Versus Propofol for Induction of Anesthesia, Clinical Trials and Case Studies, 2(2); DOI:10.31579/2835-835X/023
Received: 06 April 2023 | Accepted: 16 April 2023 | Published: 23 April 2023
Keywords: epididymal cyst; transillumination; management
Abstract
Background and Objective: Ciprofol is a recently developed γ-aminobutyric acid receptor stimulant, which has been shown to be more effective than propofol. With the publication of data from studies on the induction of general anesthesia, the safety and efficacy of ciprofol compared with those of propofol in the induction and maintenance of anesthesia are hoped to be determined through a systematic review and meta-analysis.
Methods: Relevant databases for randomized controlled trials that may be eligible were searched. Dichotomous data were pooled in a random effects model as the mean difference between the relative risk (RR) and the 95% confidence interval (CI) of the continuous variable to estimate the treatment effect. Review Manager 5.4.1 for Windows was used for data statistics.
Results: The induction success rate was 100% in the ciprofol and propofol groups (RR 1.00, 95% CI [0.99, 1.01], p = 0.71). No significant difference was shown in the time of successful induction (MD 2.85, 95% CI [−11.34, 10.22], p = 0.92). No significant difference was also shown in the disappearance time of the eyelash reflex (MD −0.10, 95% CI [−8.30, 8.10], p = 0.98). No significant difference was found in the occurrence of post-induction hypoxia (OR 1.24, 95% CI [0.54, 2.86], p= 0.61). No significant difference was observed in bradycardia (OR 0.84, 95% CI [0.52, 1.38], p = 0.66) nor hypotension (OR 0.64, 95% CI [0.34, 1.20], p = 0.17). The ciprofol group was suggested to be of better performance than the propofol group in the BIS mean (MD −2.25, 95% CI [0.86, 0.99], p = 0.04). The two groups statistically differed in (OR 0.09, 95% CI [0.04, 0.19], p < 0.00001).
Conclusions: Compared with propofol, ciprofol had similar effects in the induction of anesthesia, with no statistically significant differences in the time to successful induction and time to disappearance of the eyelash reflex. It also performed better than the propofol group in BIS in response to depth of anesthesia. The probability of hypoxia, bradycardia, or hypotension during ciprofol induction was similar to that during propofol induction, and propofol had a greater advantage in terms of the more common injection pain. Further large-scale and long-term studies are needed to compare the efficacy and safety of the two schemes.
Introduction
The sedative-hypnotic agent propofol is a short-acting γ-aminobutyric acid (GABA) receptor stimulant commonly used for the induction and maintenance of general anesthesia [1] due to its rapid onset, short duration of action, and subsequent rapid awakening during treatment. However, propofol also depresses the circulatory and respiratory systems, and it has been associated with injection pain and other adverse events [2-4]. Therefore, clinical anesthesiologists need to be able to select alternative medications that maximize patient safety and comfort without compromising the effectiveness of the induction of anesthesia. Ciprofol is a recently developed GABA receptor stimulant formulated in an injectable emulsion of medium- and long-chain triglycerides, similar to that used for propofol [5]. It could be used as an anesthetic and sedative, and it performs more effectively than propofol. Intravenous induction of general anesthesia and patient sedation have been promised. Clinical studies have shown that ciprofol had a dose-related sedative-hypnotic effect with a rapid onset and offset, whose potency was 4–6 times greater than that of isoproterenol [6] and whose residual side effects were fewer after a single therapeutic dose administration. In general, the adverse effects observed after treatment with ciprofol and propofol are similar, mainly including respiratory depression, hypotension, sinus bradycardia, and injection pain. Some evidence also indicated that ciprofol may exhibit a lower incidence of injection site pain and adverse respiratory reactions than propofol. Injection pain may depend on the concentration of propofol in the injectable emulsion [7]. ciprofol prepared at a lower concentration in the aqueous phase of the emulsion shows higher lipid solubility and potency than propofol. For the same level of anesthesia, the lipid in the ciprofol emulsion is lower than that in the propofol emulsion. Although ciprofol has been developed only recently, data on its use for induction of general anesthesia are being published. Therefore, the present systematic review and meta-analysis aimed to determine the safety and efficacy of ciprofol compared with those of propofol in the induction and maintenance of anesthesia. The results could further provide evidence for the clinical use of ciprofol.
2.Method
.1 Literature retrieval strategy
Based on the PRISMA statement, potentially eligible studies in English and Chinese were searched in PubMed, EMBASE, Cochrane Library, Web of Science, Vipers Chinese Science and Technology Journal Database, CNKI Database, Sinomed Literature Database Online, and Wanfang Database from the time of database creation to September 2022. A search strategy of subject terms plus free words was used as follows: “(ciprofol OR HSK3486) AND (propofol OR disoprofol OR diprivan OR disoprivan OR fresofol OR ivofol OR recofol OR aquafol OR 2,6-Diisopropylphenol OR ICI-35868) AND (induction OR induction of general anesthesia),” including their different terms and synonyms. References to the included literature were checked, and the authors were consulted for any additional information. The database search results were retrieved, and duplicate studies were removed by NoteExpress software. The titles and abstracts of the search records were screened by three independent reviewers to exclude irrelevant articles while considering articles that may be included. Disagreements that arose were resolved through discussion to reach consensus. The full texts for potential inclusion in the study were retrieved. Three reviewers independently retrieved the full texts, and only those studies that met the criteria were included.
2.2 Inclusion and exclusion criteria
All included studies met the following inclusion criteria: (1) studies regarding the relationship between ciprofol and induction of anesthesia; (2) all populations in the study receiving surgery or bronchoscopy and gastroscopy and colonoscopy; (3) induction doses of ciprofol and propofol at 0.4 and 2.0 mg/kg, respectively; and (4) studies providing the mean age, predominant race, and characteristics (i.e., weight, height, and sex) of patients.
Studies were excluded if they contained one of the following exclusion criteria: (1) review article, abstract, animal trial, or phase I clinical trial; (2) incomplete information regarding sample size, patient age, or race (and this information could not be obtained from the authors); and (3) non-randomized controlled trial (RCT).
2.3 Data extraction
Data extraction was performed independently by two researchers, and all data were cross-validated. If the results of the data extraction were inconsistent, the two researchers reviewed the original study and discussed it to reach agreement. If they still disagreed, other researchers read the study and made the final decision on whether the study should be included. The following clinical features were extracted: data on the name of first author; year of publication, sample size; sex ratio; mean age; type of operation; induction success rate; time of successful induction (mean and standard deviation); disappearance time of eyelash reflex (mean and standard deviation); mean BIS (mean and standard deviation); and number of occurrences of hypoxia, hypotension, tachycardia, and injection pain. If needed, the authors of the included studies were consulted for further information.
2.5 Quality assessment
The quality of retrieved RCTs was assessed in accordance with the Cochrane Handbook for Systematic Reviews of Intervention 5.1.0 (updated March 2011)[8]. The bias risk assessment contained the following areas: sequence generation (selection bias), allocation sequence concealment (selection bias), blinding of participants and personnel (implementation bias), blinding of outcome assessments (measurement bias), incomplete outcome data (follow-up bias), selective outcome reporting (reporting bias), and other potential sources of bias. The authors’ judgments were categorized as “low risk,” “high risk,” or “uncertain risk” of bias. The quality assessment form provided in the evaluation manual [8] were used.
2.6. Treatment effect measurement
In studies comparing the efficacy and safety of ciprofol and propofol, the main outcome measures were as follows: induction success rate, time of successful induction, disappearance time of eyelash reflex, BIS mean, and safety results. The safety indicators included hypoxia, hypotension, bradycardia, and injection pain.
Successful induction, which was defined as not requiring any alternative sedative/anesthetic or a supplemental study drug dose after study administration, was initiated (MOAA/S ≤ 1; no alternative hypnotics).
2.7. Handling of missing data
In the case of missing standard deviation of the mean change from baseline, the results were calculated from standard errors or 95% confidence intervals (CIs) in accordance with Altman [9].
2.8 Data integration
Dichotomous data were pooled in a random effects model as the mean difference between the relative risk (RR) and the 95% CI of the continuous variable to estimate the treatment effect. Studies were weighted by the inverse of the outcome variance, and all analyses were performed by random effects models. Review Manager 5.4.1 for Windows was used for data statistics.
2.9 Heterogeneity assessment
Heterogeneity was measured by I2 and chi-square tests; the latter was used to test for the presence of significant heterogeneity, and the former was used to quantify the variability of effect estimates due to heterogeneity (if present). Moreover, the I2 test was interpreted in accordance with the recommendations of the Cochrane Handbook of Systematic Reviews and Meta-analyses (0%–40%, probably insignificant; 30%–60%, probably representing moderate heterogeneity; 50%–90%, probably representing significant heterogeneity; and 75%–100%, considerable heterogeneity). Significant heterogeneity was considered on the chi-square tests (p < 0>
2.10. Publication bias
According to Egger et al. [10, 11], publication bias assessment is unreliable for publications fewer than 10 pooled studies. Therefore, in the present study, the presence of publication bias could not be assessed by Egger funnel plot asymmetry test.
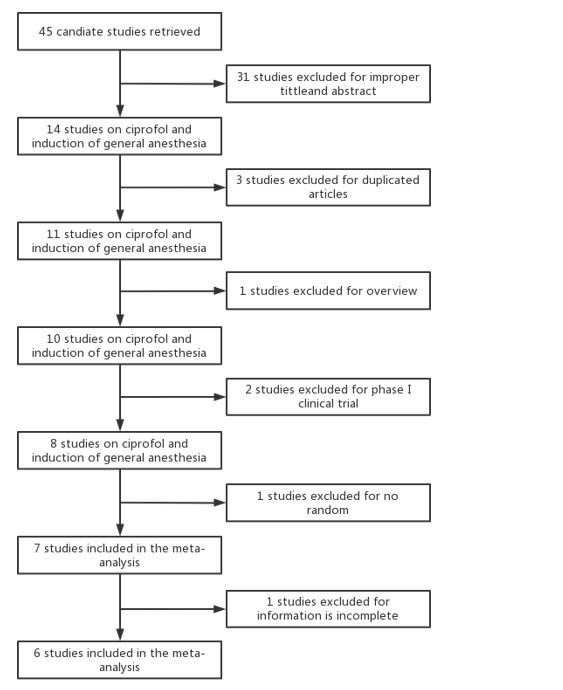
Figure 1: Flowchart of article screening process.
Results
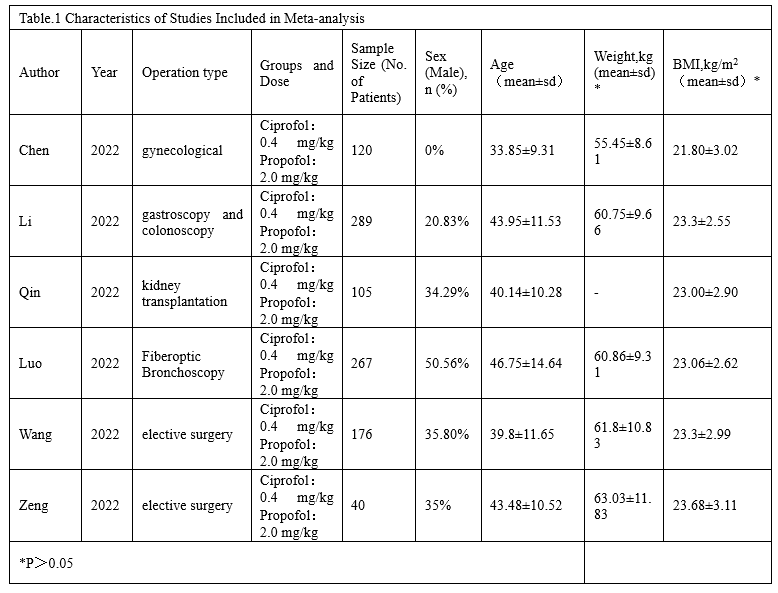
The detailed process of literature screening is shown in Fig. 1. Among the 45 studies determined, six were strictly RCTs [12-17]. A total of 997 patients (n = 508 in the ciprofol group and n = 489 in the propofol group) were involved in these six studies for meta-analysis. All included studies were recently published in English. The sample size was 40–289 patients, including two elective operations, one renal transplantation, one gynecological operation, one gastroscopic operation, and one bronchoscopic operation. The characteristics of the six included studies are shown in Table 1, with doses of 0.4 mg/kg in the ciprofol group and 2.0 mg/kg in the propofol group. The mean age ranged from 33 years to 46 years, with female predominance in the sex ratio. No statistical differences were found in weight and body mass index.
The quality of the included RCTs ranged from moderate to high quality according to the Cochrane Risk of Bias Assessment Tool. A summary of the quality assessment domains included in the study is shown in Figure 2.
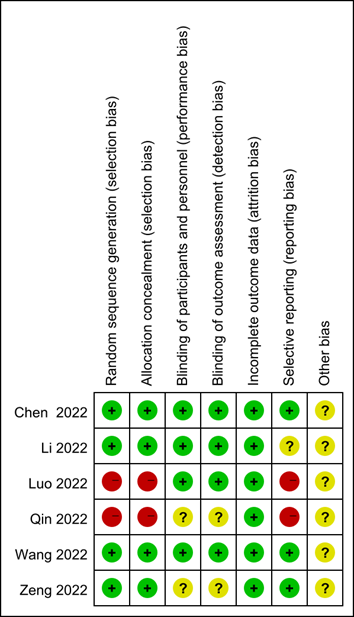
Figure 2: Summary of bias risk according to the Cochrane Risk of Bias Assessment Tool. “+” = low risk of bias; “−” = high risk of bias; and “?” = minimal information to determine bias risk.
- Comparison of the effects of ciprofol and propofol
In the included studies, the success rate of induction was 100% in both groups (RR 1.00, 95% CI [0.99, 1.01], p = 0.71; Figure 3a). No significant difference was shown in the time of successful induction (MD 2.85, 95% CI [−11.34, 10.22], p = 0.92; Figure 3b). No significant difference was also shown in the disappearance time of eyelash reflex (MD −0.10, 95% CI [−8.30, 8.10], p = 0.98; Figure 3c). However, the BIS mean of the ciprofol group was better than that of the propofol group (MD −2.25, 95% CI [0.86, 0.99], p = 0.04; Figure 3d). In terms of efficacy, no statistical difference was observed in the success rate of induction and induction time between the ciprofol and propofol groups. Even the depth of anesthesia in the ciprofol group was better than that in the propofol group. Furthermore, no heterogeneity was found in the success rate of induction (I2 = 0, p > 0.1), whereas considerable heterogeneity was observed in all other indicators (I2 75%–100%, p < 0>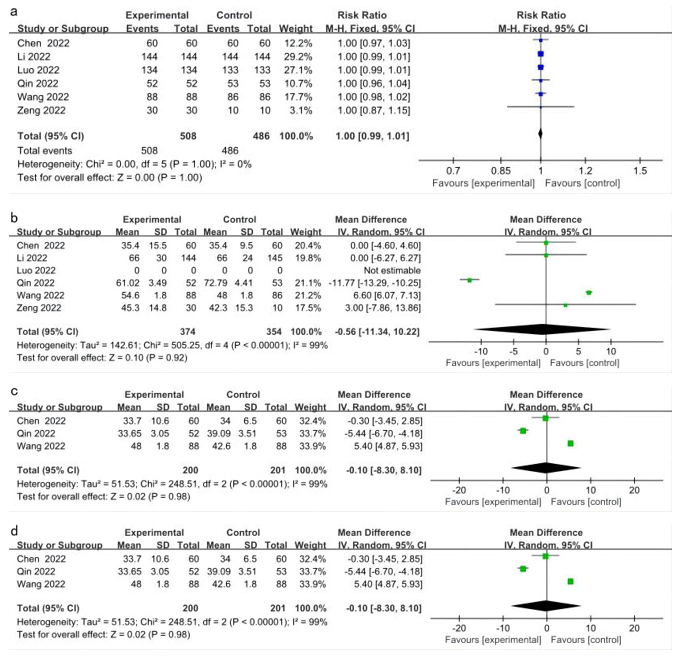
Figure 3: Forest plot of efficacy after induction in ciprofol and propofol groups. a. Induction success rate. b. Time of successful induction. c. Disappearance time of eyelash reflex. d. BIS mean.
3.2. Security
No significant difference could be found in the incidence of the following adverse reactions with respect to ciprofol (Figure 4): hypoxia (OR 1.24, 95% CI [0.54, 2.86], p = 0.61), bradycardia (OR 0.84, 95% CI [0.52,
4. Discussion
4.1. Efficacy of ciprofol versus propofol
This meta-analysis showed that ciprofol exerted similar effects as propofol in terms of inducing anesthesia. No significant difference could be found in the time of successful induction and disappearance time of eyelash reflex. Moreover, the mean BIS in the ciprofol group was lower than that in the propofol group. However, a large heterogeneity was observed in all of the above datasets, and the heterogeneity may have originated from the different assessment intervals in different studies. Li and Zeng assessed anesthesia success in cycles of approximately 30 seconds and obtained a large standard deviation. Although Wang also assessed the depth of anesthesia in 30 seconds, the author was able to obtain the timepoint at which the patient lost or was about to lose consciousness quickly by continuously observing the BIS to monitor the patient, thus obtaining a smaller standard deviation and greater weighting. Similarly, Qin used the disappearance of eyelash reflex and BIS ≤ 60 as successful induction endpoint. All the other studies regarded MOAA/S ≤ 1 as successful induction endpoint. However, the above two studies showed huge differences in the time of successful induction and disappearance time of lash reflex, probably because Wang conducted pretreatment with sedative midazolam and sufentanil before administration, although the specific effects of combined sedation of midazolam with propofol and ciprofol still need to be confirmed in more trials. Meanwhile, a 100% induction success rate was achieved in both groups, indicating that induction of anesthesia with either of the two drugs at the beginning of the study did not require additional supplemental sedation in achieving MOAA/S ≤ 1. This finding is consistent with the data from phase I trials of the drugs [18].
4.2. Safety of ciprofol and propofol
Safety-related indicators showed less heterogeneity than the efficacy indicators, probably because the safety-related indicators were mainly monitored by instruments, thus avoiding the influence of subjective factors of the investigator. Certain heterogeneity was mainly caused by the different outcome criteria developed between studies. In terms of hypotension induction, Li and Wang set the criterion at a 30
References
- Grasshoff C, Antkowiak B, (2004). Propofol and Sevoflurane Depress Spinal Neurons In Vitro via Different Molecular Targets. ANESTHESIOLOGY. 11-01;101(5):1167-1176.
View at Publisher | View at Google Scholar - Qiu Q., Choi SW, Wong SSC, Irwin MG, Cheung CW, (2016). Effects of intra-operative maintenance of general anaesthesia with propofol on postoperative pain outcomes - a systematic review and meta-analysis. ANAESTHESIA. 10-01;71(10):1222-1233.
View at Publisher | View at Google Scholar - Rochette ., Hocquet AF., Dadure C., Boufroukh D., Raux O., Lubrano JF., et al. (2008). Avoiding propofol injection pain in children: a prospective, randomized, double-blinded, placebo-controlled study. BRIT J ANAESTH. 09-01;101(3):390-394.
View at Publisher | View at Google Scholar - MARIK PE, (2004). Propofol: Therapeutic Indications and Side-Effects. CURR PHARM DESIGN. -01-01;10(29):3639-3649.
View at Publisher | View at Google Scholar - James R, Glen JB. Synthesis. (1980). biological evaluation, and preliminary structure-activity considerations of a series of alkylphenols as intravenous anesthetic agents. J MED CHEM. 12-01;23(12):1350-1357.
View at Publisher | View at Google Scholar - Qin L, Ren L., Wan S., Liu G., Luo X., Liu Z., et al. (2017). Design, Synthesis, and Evaluation of Novel 2,6-Disubstituted Phenol Derivatives as General Anesthetics. J MED CHEM. 05-11;60(9):3606-3617.
View at Publisher | View at Google Scholar - Desousa K., (2016). Pain on propofol injection: Causes and remedies. INDIAN J PHARMACOL. 11-01;48(6):617.
View at Publisher | View at Google Scholar - Hartling L., Schellenberg ES., Shulhan J., Dryden DM., (2012). Approaches to risk of bias assessments in non-Cochrane reviews.
View at Publisher | View at Google Scholar - Altman DG., Bland JM., (2005). Standard deviations and standard errors. BMJ-BRIT MED J. 10-15;331(7521):903.
View at Publisher | View at Google Scholar - Egger M., Smith GD., Schneider M., (1997)Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ-BRIT MED J. 013;315(7109):629-634.
View at Publisher | View at Google Scholar - Terrin N., Schmid CH., Lau J., Olkin I., (2003). Adjusting for publication bias in the presence of heterogeneity. STAT MED. 07-15;22(13):2113-2126.
View at Publisher | View at Google Scholar - Li J, Wang X., Liu J., Wang X., Li X., Wang Y., et al. (2022). Comparison of ciprofol (HSK3486) versus propofol for the induction of deep sedation during gastroscopy and colonoscopy procedures: A multi‐centre, non‐inferiority, randomized, controlled phase 3 clinical trial. BASIC CLIN PHARMACOL.131(2):138-148.
View at Publisher | View at Google Scholar - Qin K., Qin W., Ming S., Ma X., Du X., (2022). Effect of ciprofol on induction and maintenance of general anesthesia in patients undergoing kidney transplantation. EUR REV MED PHARMACO. 01-01;26(14):5063-5071.
View at Publisher | View at Google Scholar - Wang X., Wang X., Liu J., Zuo Y., Zhu Q., Wei X., et al. (2022). Effects of ciprofol for the induction of general anesthesia in patients scheduled for elective surgery compared to propofol: a phase 3, multicenter, randomized, double-blind, comparative study. EUR REV MED PHARMACO. 01-01;26(5):1607-1617.
View at Publisher | View at Google Scholar - Luo Z., Tu H., Zhang X., Wang X., Ouyang W., Wei X., et al. (2022). Efficacy and Safety of HSK3486 for Anesthesia/Sedation in Patients Undergoing Fiberoptic Bronchoscopy: A Multicenter, Double-Blind, Propofol-Controlled, Randomized, Phase 3 Study. CNS DRUGS. 03-01;36(3):301-313.
View at Publisher | View at Google Scholar - Zeng Y., Wang D., Lin Z., Liu J., Wei X., Deng J., et al. (2022). Efficacy and safety of HSK3486 for the induction and maintenance of general anesthesia in elective surgical patients: a multicenter, randomized, open-label, propofol-controlled phase 2 clinical trial. EUR REV MED PHARMACO. 01-01;26(4):1114-1124.
View at Publisher | View at Google Scholar - Chen B., Yin X., Jiang L., Liu J., Shi Y., Yuan B., (2022) The efficacy and safety of ciprofol use for the induction of general anesthesia in patients undergoing gynecological surgery: a prospective randomized controlled study. BMC ANESTHESIOL. 08-03;22(1):245.
View at Publisher | View at Google Scholar - Liao J., Li M., Huang C., Yu Y., Chen Y., Gan J., et al. (2022). Pharmacodynamics and Pharmacokinetics of HSK3486, a Novel 2,6-Disubstituted Phenol Derivative as a General Anesthetic. FRONT PHARMACOL. 02-03;13:830791.
View at Publisher | View at Google Scholar - Karshikoff B., Lekander M., Soop A., Lindstedt F., Ingvar M., Kosek E., et al. (2022). Modality and sex differences in pain sensitivity during human endotoxemia. Brain, Behavior, and Immunity. 05-01;46:35-43.
View at Publisher | View at Google Scholar - Campesi I., Fois M., Franconi F., (2012). Sex and Gender Aspects in Anesthetics and Pain Medication. Berlin, Heidelberg: Springer Berlin Heidelberg. p. 265-278.
View at Publisher | View at Google Scholar
