

Research Article | DOI: https://doi.org/10.31579/ 2835-835X/010
Investigation of pain among oncology patients and the effect of satisfaction and clinical features
- Paraskevi Theofilou *
General Hospital of Thoracic Diseases SOTIRIA, Athens, Greece
*Corresponding Author: Paraskevi Theofilou, General Hospital of Thoracic Diseases SOTIRIA, Athens, Greece
Citation: Paraskevi Theofilou, (2023) Investigation of pain among oncology patients and the effect of satisfaction and clinical features. Clinical Trials and Case Studies.2(1); DOI:10.31579/ 2835-835X/010
Copyright: © 2023 Paraskevi Theofilou, this is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 January 2023 | Accepted: 07 February 2023 | Published: 14 February 2023
Keywords: oncology; patients; pain; satisfaction
Abstract
Measuring patients’ pain in the last decades is an important tool for assessing the impact on their quality of life and mental health. The purpose of this study is to assess the level of pain among oncology patients by providing health services outpatient pain in a General Hospital as well as the satisfaction and clinical factors affecting this level. In the context of gathering research data, Greek brief Pain Inventory was used. The study included 156 patients (74 males και 82 females). A correlation was found between satisfaction level and pain in the patients of the study (p <0.05). No relation was found between clinical factors and pain level (p>0.05). Pain level of these patients is influenced by their satisfaction.
Introduction
Almost half of patients living with poorly managed pain experience significant costs to their daily lives (Cousins et al., 2004). Unmanageable pain can have long-term physiological and psychological consequences, such as increased susceptibility to depression, lower quality of life, reduced independence, and reduced functioning in activities of daily living (Coker et al., 2010; Lapane, Quilliam, Chow, & Kim, 2012). Chronic pain is also associated with enormous financial, physical, and psychological costs (Kohr & Sawhney, 2005). It is estimated that the annual cost of pain management in Canada exceeds $10 billion (Reltsma et al., 2011). Persistent pain can lead to reduced productivity at work, resulting in financial costs to the economy and the individual (Lynch, 2011). Pain can limit activities and negatively affect mental health and interpersonal relationships, thus reducing quality of life (McCarberg et al., 2008).
Effective pain management includes pain control, assessment (continuous assessment and reassessment), diagnosis, documentation (timely and appropriate), treatment (pharmacological and non-pharmacological interventions), and continuous assessment of care (Registered Nurses' Association of Ontario [RNAO], 2007). Pain management should also include ongoing education and training of staff, patients, and patients' families about pain experiences and related primary and secondary interventions (Health Care Association of New Jersey, 2006, RNAO, 2007). Primary interventions would be preventive - for example, education for patients with chronic pain that includes pain management techniques. Secondary interventions refer to the immediate treatment of pain at the time of onset, such as medication for patients complaining of pain from a broken bone. Nurses play a key role in effective pain management (Ferrell, 2005; RNAO, 2007) and factors influencing effective pain management among healthcare professionals are well documented (Brown, 2004; Prkachin, Solomon & Ross, 2007). However, despite decades of extensive research, ineffective pain management is still ubiquitous in health care in Canada and many other countries, such as the United Kingdom (Maier et al., 2010; Wadensten, Fröjd, Swenne, Gordh & Gunningberg, 2011) and the United States (Carr, Reines, Schaffer, Polomano, & Lande, 2005).
Many studies have used multidisciplinary interventions as pain management strategies for people with chronic pain and have reported effective pain relief. For example, education for people with chronic pain was used in conjunction with pain relief strategies such as pharmacological treatment, relaxation and exercise often delivered by a multidisciplinary team. Because chronic pain is excruciating, persistent and has physical and psychosocial effects, interprofessional teamwork approaches have been extremely important (AGS Panel on Persistent Pain in Older Persons, 2002). The long-term efficacy of pain relief was not satisfactory and needs to be further investigated in research.
According to qualitative studies, people with chronic pain perceive that social support has been effective in managing their pain. For example, talking with their family or friends and participating in patient groups were effective in managing pain (Kengen Traska et al., 2012; West et al., 2012). However, the effectiveness of social supports has not been examined in trials. Social resources that remain close to people with chronic pain can function for long periods of time at minimal cost. In contrast, Dysvik, Natvig, Eikeland, and Lindstrøm (2005) found that the most important stressors in people with chronic pain were family life and social activities. Social interactions with family members or friends for people experiencing pain, as well as the effects of these interactions, are complex. However, supporting families to help them cope with pain and protect them from future crises could be a worthwhile approach for nurses (Lewandowski, Morris, Draucker & Risko, 2007; West et al., 2011). This area should be looked into further.
Although high pain intensity has been reported in people living in nursing facilities (Takai, Yamamoto-Mitani, Okamoto, Koyama, & Honda, 2010), there has been a lack of extensive research focusing on people living in nursing facilities or people with dementia or mental illness. Pain often has psychological consequences, such as depression, anxiety, or the behavioral and psychological symptoms of dementia (Husebo, Ballard, & Aarsland, 2011; Smalbrugge, Jongenelis, Pot, Beekman, & Eefsting, 2007). A systematic review described only three studies that supported the idea that pain management reduced the disorder (Husebo et al., 2011). However, intervention for vulnerable people should be explored. Further studies are important.
The purpose of this study is to assess the level of pain among oncology patients by providing health services outpatient pain in a General Hospital as well as the clinical factors and satisfaction affecting this level.
Method
In this research, the following tools were used to collect the data:
1.Greek Brief Pain Inventory (Mystakidou et al., 2001). It includes 9 questions about the pain someone feels in the last 24 hours. Respondents use an 11-point Likert-type scale (0 = no pain, 10 = the worst pain imaginable) to rate the intensity of their pain as "worst", "minimum" or "moderate" during the last 24 hours, as well as the moment of calibration (4 questions). Also, patients indicate the location of their pain on a schematic diagram of the anterior and posterior surface of the body. Other questions (3) concern the experience of pain beyond the usual, taking analgesic drugs or other treatment and the extent to which, these relieve the pain. It includes two main components, one of which expresses the average severity of pain in the last 24 hours (average of 4 questions) and the other the degree to which the pain affects daily life (general activity, walking, work, mood, enjoyment of life, interpersonal relationships, sleep) of the individual. The range for the former is 0-40 and for the latter 0-70 (mean of 7 responses based on an 11-point Likert-type scale, 0 = does not interfere, 10 = completely interferes), with higher scores reflecting greater mean severity and impact of pain respectively.
2.The Patient Satisfaction Questionnaire - Short Form (PSQ-18) was also used to extract the data of the present study. This questionnaire is a widely used research tool for the quantitative assessment of patient satisfaction. It has been in use since 1976 and consists of 18 research topics related to medical care, technical service quality, interpersonal relationships, communication, financial aspects of care, time with the doctor, accessibility, and care provided (Ware, Snyder, Wright, 1976). Answers are given on a 5-point Likert scale and range from "strongly agree" (1) to "strongly disagree" (5) (Partheniadis et al., 2022).
3.In addition to the aforementioned questionnaire, there were questions related to the demographic and clinical characteristics of the sample, e.g., gender, age, type of cancer, coexisting diseases, etc.
This is a cross-sectional study. The research population was all patients of the pain department of a General Hospital. The sample for the research was the patients who would visit the clinic for the second time. This particular sample is a sample of convenience. Patients were selected based on the inclusion criteria for the study, which are as follows:
• The patient's consent
• Age over eighteen years
• Diagnosed with cancer
• Ability to communicate in the Greek language
• His (patient's) general state of health allows him to take part in the study
All research participants were informed in writing and verbally and signed a consent form. The collection of the sample was preceded by written approval from the Scientific Committee of the Hospital, following a relevant request of the researcher.
The data were collected with the help of special questionnaires. The researcher was responsible for the data collection, informed the patients orally about the aims of the study and then completed the questionnaires by interview, which were accompanied by a letter stating information about the purpose of the study, anonymity and data confidentiality, as well as the voluntary nature of participation. Completing the questionnaires meant acceptance of participation and informed consent, while their completion time did not exceed 15 minutes. The response rate was 100%.
For the presentation of the results related to the responses of the patients to the questionnaires, who participated in the research, a frequency analysis was carried out. Additionally, the descriptives command was run to examine the averages. Quantitative variables are presented as mean (± standard deviation) while qualitative variables are presented as frequency (%). Also, a test of normality of the sample was performed using the Kolmogorov Smirnov test. In order to investigate possible associations between pain and clinical factors, non-parametric and parametric tests were performed (Spearman/Pearson correlation analysis, Mann-Whitney test/Independent samples t test, Kruskal Wallis test/One-Way anova). Both instruments used in this research showed very good reliability (Cronbach a), ranging from 0.85 for the satisfaction questionnaire and 0.78 for the pain questionnaire. Statistical analysis was performed with the IBM SPSS Statistics 23 statistical program. A p value less than 0.05 was considered to indicate statistical significance.
Results
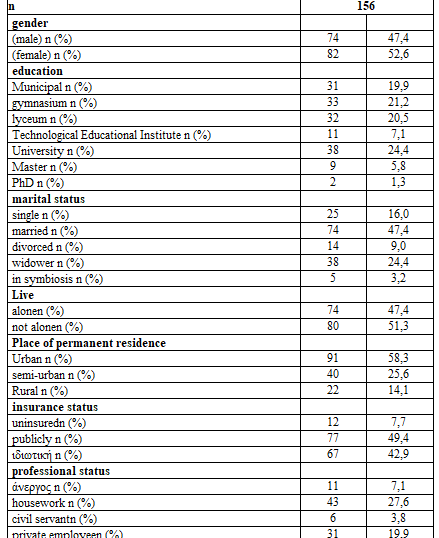
One hundred and fifty-six patients (74 men and 82 women) with an average age of 58.73±13.47 years participated in the research. The majority of them were married (47.4%), 24.4% widowed, 16.0% single while 9.0% were divorced. Eighty patients stated that they do not live alone and 74 patients stated that they do live alone.
Regarding their educational level, 31 patients were elementary school graduates (19.9%), 33 patients were high school graduates (21.2%), 32 patients declared that they were high school graduates (20.5%) while 49 had a university degree/ TEI (higher education) (31.5%). Only 11 patients had master's/doctoral degrees (7.1%).
Regarding the professional status of the patients, the majority (65 patients) declared that they are retired (41.7%), 31 private employees (19.9%), 6 public employees (3.8%), 43 patients were engaged in household (27.6%) and 11 also declared themselves unemployed (7.1%). The majority of patients resided in an urban area (58.3%), 22 patients (14.1%) in a rural area and 40 patients (25.6%) in a semi-urban area.
Regarding the insurance status of the sample, 77 patients (49.4%) had public insurance, 67 patients (42.9%) had private insurance and 12 patients (7.7%) declared uninsured.
In detail, all socio-demographic characteristics are presented in table 1.
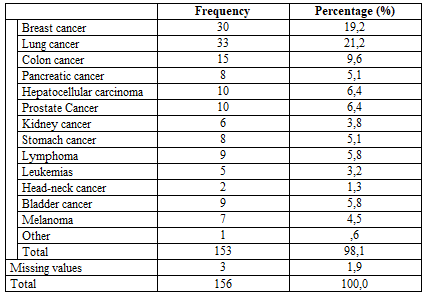
In table 2, the results of the cancer types are presented. The majority of patients (21.2%) had lung cancer, 19.2% (30 patients) had breast cancer, while 15 patients (9.6%) had colon cancer
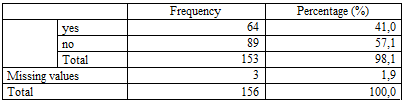
Based on the results in table 3, 64 patients (41.0%) had comorbidities and 89 patients (57.1%) had no comorbidities.
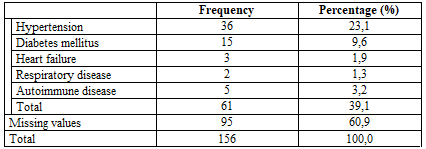
Based on the results of Table 4, the majority of patients (23.1%) also suffered from hypertension in addition to cancer while 15 patients (9.6%) suffered from diabetes mellitus.

In table 5, the results of the descriptive elements of the questionnaire are presented. The effect of pain on everyday life reached 5.67±2.87, while the severity of pain in the last 24 hours reached 5.44±1.34.

In the table above, the values of the Kolmogorov-Smirnov test regarding the normality of the sample are displayed. There was no normality in any of the dimensions (p<0>0.05).
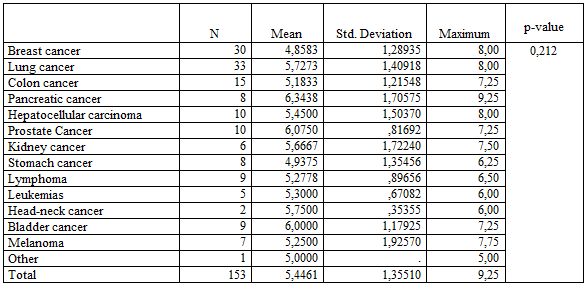
The results of table 7 did not show that there was a statistically significant difference (p=>0.05) between types of cancer regarding the severity of pain in the last 24 hours.
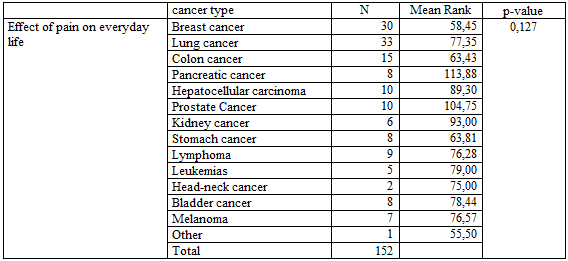
The results of table 8 did not show that there was a statistically significant difference (p=>0.05) between types of cancer regarding satisfaction and the effect of pain on everyday life.

The results of table 9 did not show that there was a statistically significant difference (p=>0.05) between coexisting diseases and those without regarding the severity of pain in the last 24 hours.

The results of table 10 did not show that there was a statistically significant difference (p=<0>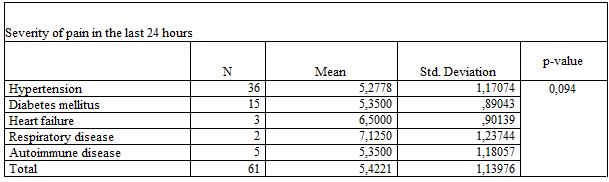
The results of table 11 did not show that there was a statistically significant difference (p=>0.05) between coexisting diseases regarding the severity of pain in the last 24 hours
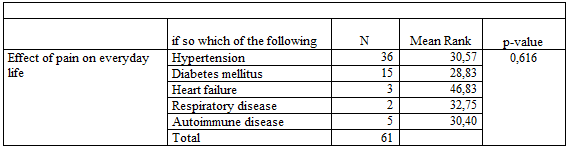
The results of table 12 did not show that there was a statistically significant difference (p=>0.05) between coexisting diseases regarding the effect of pain on everyday life.
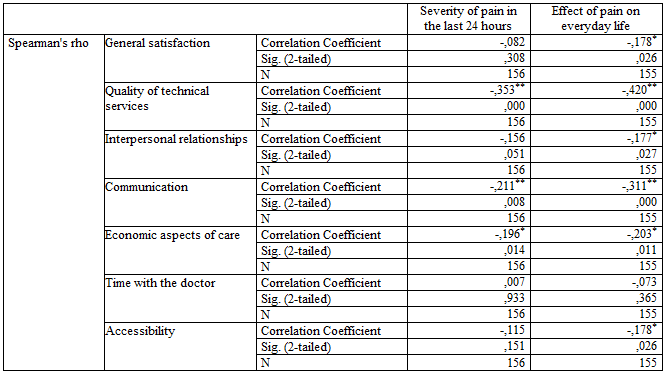
Regarding the correlation between satisfaction and pain (table 13), there was a statistically significant (p<0>
There was also no statistically significant correlation between age and pain severity in the last 24 hours (p=0.958, r=0.004).
On the contrary, a statistically significant and negative correlation of age with general patient satisfaction (p= -0.241, r=0.002), interpersonal relationships (p= -0.281, r=0.000), communication (p= -0.335, r =0.000), time with doctor (p= -0.231, r=0.004) and accessibility (p= -0.207, r=0.010).
Discussion
The findings from the said research study are significant and can be summarized as follows:
A correlation is observed between the level of satisfaction and pain in the patients who participated in the research with those who show higher satisfaction having less pain severity and less impact on their daily activity.
Much of the literature dealing with pain and patient satisfaction has focused on satisfaction with pain management, not satisfaction with pain level. A large proportion of patients with cancer pain, e.g., 80% (Beauregard, Pomp & Choiniere, 1998) to 99% (Panteli & Patistea, 2007) and postoperative pain, e.g., 75% reported a high level of satisfaction with pain management rather than pain intensity. Similar study results have been found in other countries, such as the Netherlands, Sweden and China (Beauregard et al., 1998; de Wit, van Dam, Vielvoye-Kerkmeer, Mattern & Abu-Saad, 1999; Hurwitz, Morgenstern & Yu, 2005; Jensen, Mendoza, Hanna, Chen, & Cleeland, 2004). Possible explanations for this asymmetry are varied.
A comprehensive framework such as the biopsychosocial model of health care will be based on a single guiding principle: that the goal of addressing the physical, social, and psychological aspects of chronic disease is to help patients with chronic conditions and the entire population, regardless of from a person's chronic illness or current state of health.
Regarding the limitations of the present research, it is noted that the results obtained from the said study can be further investigated in samples from other hospital contexts, private or even public, giving the possibility to control the variables under study, to compare the results, so that more general conclusions can be drawn. However, it should be noted that this study was conducted in only one hospital and therefore, because the sample is small, the results cannot be generalized.
References
- Achterberg,W.P.,Gambassi,G.,Finne-Soveri,H.,Liperoti,R., Noro, A., Frijters, D. H. et al. (2010). Pain in European Long-Term Care Facilities: Cross-national study in Finland, Italy and the Netherlands. Pain, 148, 70–74.
View at Publisher | View at Google Scholar - Adams, M.P. Holland, L.N. & Urban, C.Q. (2011). Pharnacology for nurses. A Pathophysiologic approach. 3rd edition. Pearson, USA. 219, 211
View at Publisher | View at Google Scholar - American Pain Foundation, (2010). Breakthrough Cancer Pain. Mending the break in the continuum of care. 24, 2012. 2, 5, 7
View at Publisher | View at Google Scholar - American Pain Foundation, (2010). A reporter’s guide: Covering Pain and Its Management. . 4-7, 9
View at Publisher | View at Google Scholar - AGS Panel on Persistent Pain in Older Persons. (2002). The managementofpersistentpaininolderpersons.Journalof American Geriatrics Society, 50, 205–224.
View at Publisher | View at Google Scholar - Anand, D., Kaushal, S. K., and Gupta, S. C. (2012). A Study on Status of Client Satisfaction in Patients Attending Government Health Facilities in Agra District. Indian Journal of Community Health, 24 (3), 209-214
View at Publisher | View at Google Scholar - Antón, Α. (2012). Pain in clinical oncology: patient satisfaction with management of cancer pain. European Journal of Pain 16, (3).
View at Publisher | View at Google Scholar - Austrian, J. S., Kerns, R. D. & Reid, M. C. (2005). Perceived barriers to trying self-management approaches for chronic pain in older persons. Journal of the American Geriatrics Society, 53, 856–861.
View at Publisher | View at Google Scholar - Baker SK. (1998) Improving Service and Increasing Patient Satisfaction Family Practice Management; July-August, [Last accessed on 2015 Aug 17].
View at Publisher | View at Google Scholar - Baker R, & Fraser R. (1995). Development of review criteria: linking guidelines and assessment of quality. BMJ, 311, 370-373.
View at Publisher | View at Google Scholar - Beauregard L, Pomp A, Choiniere M. (1998) Severity and impact of pain after day-surgery. Can J Anaesth. 45(4):304–311.
View at Publisher | View at Google Scholar - Census of India. 2001. [Last accessed on 2015 Aug 17].
View at Publisher | View at Google Scholar - Bennett, M. Forbes, K. & Faull, C. (2005). The Principles of Pain Management. In: Faull, C. Carter, Y. & Daniels, L. 2006. Handbook of Palliative Care. 2nd edition. Blackwell Publishing Ltd. United Kingdom. 114, 120-121, 123-124, 126, 128-131
View at Publisher | View at Google Scholar - Berenson, S. (2006). Complemetary and Alternative Therapies in Palliative Care. Edit. In: Ferrell, B.R. & Coyle, N. 2006. Textbook of Palliative Nursing. 2nd edition. Oxford University Press, Inc. USA. 493
View at Publisher | View at Google Scholar - Boyer, L., Franc¸ois, P., Doutre, E., Weil, G. and Labarere, J. (2006), “Perception and use of the results of patient satisfaction surveys by care providers in a French teaching hospital”, International Journal for Quality in Health Care, Vol. 18 No. 5, pp. 359-364.
View at Publisher | View at Google Scholar - Brown, D. (2004). A literature review exploring how healthcare professionals contribute to the assessment and control of postoperative pain in older people. Journal of Clinical Nursing, 13(S2), 74–90.
View at Publisher | View at Google Scholar - Burke, K.M. Mohn-Brown, E.L. & Eby, L. (2011). Medical Surgical Nursing Care. 3rd edition. Pearson: USA. 133, 151, 153, 181, 265, 267-268, 281, 303
View at Publisher | View at Google Scholar - Carr, D. B., Reines, D. H., Schaffer, J., Polomano, R. C., & Lande, S. (2005). The impact of technology on the analgesic gap and quality of acute pain management. Regional Anesthesia in Pain Medicine, 30(3), 286–291.
View at Publisher | View at Google Scholar - Cleary PD, McNeil BJ. Patient satisfaction as an indicator of quality care. Inquiry. 1988;25(1):25–36. [PubMed] [Google Scholar]
View at Publisher | View at Google Scholar - Cleary, P. and Edgman-Levitan, S. (1997), “Health care quality: incorporating consumer perspectives”, Journal of the American Medical Association., Vol. 278 No. 19, pp. 1608-1612.
View at Publisher | View at Google Scholar - Cleeland CS. (1993) Strategies for improving cancer pain management. J Pain Symptom Manage.;8(6):361–364.
View at Publisher | View at Google Scholar - Clemes, M.D., Ozanne, L.K. and Laurensen, W.L. (2001), “Patients’ perceptions of service quality dimensions: an empirical examination of health care in New Zealand”, Health Marketing Quarterly, Vol. 19 No. 1, pp. 3-22.
View at Publisher | View at Google Scholar - Courtenay, M. & Carey, N. (2008). The Impact and effectiveness of Nurse-Led Care in the management of acute and chronicpain:Areviewoftheliterature.JournalofClinical Nursing, 17, 2001–2013.
View at Publisher | View at Google Scholar - Cordon, D. (1999). Critical pathways: A road to institutionalizing pain management. Science direct. 11(4):252-259.
View at Publisher | View at Google Scholar - Cousins, M. J., Brennan, F., & Carr, D. B. (2004). Pain relief: A universal human right. Pain, 112(1–2), 1–4.
View at Publisher | View at Google Scholar - Coker, E., Papaioannou, A., Kaasalainen, S., Dolovich, L., Turpie, I., & Taniguchi, A. (2010). Nurses’ perceived barriers to optimal pain management in older adults on acute medical units. Applied Nursing Research, 23(3), 139–146.
View at Publisher | View at Google Scholar - Coyle, J. and Williams, B. (1999), “Seeing the wood for the trees: defining the forgotten concept of patient dissatisfaction in the light of patient satisfaction research”, Leadership in Health Services,
View at Publisher | View at Google Scholar - Crowe, R., Gage, H., Hampson, S., Hart, J., Kimber, A., Storey, L. and Thomas, H. (2002), “The measurement of satisfaction with healthcare: implications for practice from a systematicreviewoftheliterature”, HealthTechnology Assessment, Vol.6No.32, pp.1-244.
View at Publisher | View at Google Scholar - Dawson R, Spross JA, Jablonski ES, Hoyer DR, Sellers DE, Solomon MZ. (2002) Probing the paradox of patients' satisfaction with inadequate pain management. J Pain Symptom Manage. 23(3):211–220.
View at Publisher | View at Google Scholar - Deming W. E. (1993). The New Economics for Industry, Government and Education. Cambridge: MIT Press.
View at Publisher | View at Google Scholar - Dewar, A. (2006). Assessment and management of chronic pain in the older person living in the community. Australian Journal of Advanced Nursing, 24, 33–38.
View at Publisher | View at Google Scholar - Donabedian A. (1982). Exploration in Quality Assessment and Monitoring: The criteria and Standards of Quality. II. Ann Arbor, MI: health Administration Press.
View at Publisher | View at Google Scholar - Donabedian, A. (1980), “The definition of quality and approaches to its assessment”, Explorations in Quality Assessment and Monitoring, Vol. 1, Health Administration Press, Ann Arbor, MI.
View at Publisher | View at Google Scholar - de Wit R, van Dam F, Vielvoye-Kerkmeer A, Mattern C, Abu-Saad HH. (1999) The treatment of chronic cancer pain in a cancer hospital in The Netherlands. J Pain Symptom Manage. 17(5):333–350.
View at Publisher | View at Google Scholar - Du, S., Yuan, C., Xiao, X., Chu, J., Qiu, Y. & Qian, H. (2011). Self-management programs for chronic musculoskeletal pain conditions: A systematic review and meta-analysis. Patient Education and Counseling, 85, e299–e310.
View at Publisher | View at Google Scholar - Ferrell, B. (2005). Ethical perspectives on pain and suffering. Pain Management Nursing, 6(3), 83–90.
View at Publisher | View at Google Scholar - Finnerup, N. B., Sindrup, S. H. & Jensen, T. S. (2010). The Evidence for Pharmacological Treatment of Neuropathic Pain. Pain, 150, 573–581
View at Publisher | View at Google Scholar - Flexner A. (1910). A medical education in the United States and Canada: A report to the Carnegie Foundation for the advancement of teaching. Bulletin No 4, Boston, The Merrymount Press.
View at Publisher | View at Google Scholar - Fox, J.G. and Storms, D.M. (1981), “A different approach to sociodemographic predictors of satisfaction with health care”, Social Science & Medicine. Part A: Medical Sociology, Vol. 15 No. 5, pp. 557-64.
View at Publisher | View at Google Scholar - Gilbert, G.R. and Veloutsou, C. (2006), “A cross-industry comparison of customer satisfaction”, The Journal of Services Marketing, Vol. 20 No. 5, pp. 298-307.
View at Publisher | View at Google Scholar - Gilbert, G.R., Veloutsou, C., Goode, M.M.H. and Moutinho, L. (2004), “Measuring customer satisfaction in the fast food industry: a cross-national approach”, The Journal of Services Marketing, Vol. 18 Nos 4/5, pp. 371-383.
View at Publisher | View at Google Scholar - Gillespie, S. M. & Friedman, S. M. (2007). Fear of Falling in New Long-Term Care Enrollees. Journal of the American Medical Directors Association, 8, 307–313.
View at Publisher | View at Google Scholar - Golas, M. (2016). Patient Satisfaction with Pain Level in Patients with Cancer. Pain Management Nursing 17, (3).
View at Publisher | View at Google Scholar - Gotlieb, J.B., Grewal, D. and Brown, S.W. (1994), “Consumer satisfaction and perceived quality: complimentary or divergent constructs”, Journal of Applied Psychology, Vol. 79 No. 6, pp. 875-885.
View at Publisher | View at Google Scholar - Groves E.W. (1908). A plea for a Uniform Registration of Operation Results. Br. J. Med, 2, 1008-1009.
View at Publisher | View at Google Scholar - Hawthorne, G. (2006), Review of Patient Satisfaction Measures, Australian Goverment Department of Health and Ageing, Canberra.
View at Publisher | View at Google Scholar - Hardy, G., West, M. and Hill, F. (1996), “Components and predictors of patient satisfaction”, British Journal of Health Psychology, Vol. 1, pp. 65-85.
View at Publisher | View at Google Scholar - Health Care Association of New Jersey. (2006). Pain management guideline. Hamilton, NJ: Health Care Association of New Jersey, US Department of Health and Human Services, Agency for Healthcare Research and Quality – National Guidelines Clearinghouse. Retrieved September 18, 2013,
View at Publisher | View at Google Scholar - Heidegger, T., Saal, D. and Nuebling, M. (2006), “Patient satisfaction with anaesthesia care: what is patient satisfaction, how should it be measured, and what is the evidence for assuring high patient satisfaction”, Best Practice and Research Clinical Anaesthesiology, Vol. 20 No. 2, pp. 331-346.
View at Publisher | View at Google Scholar - How Satisfied are Your Patients? Family Practice Management. 1998. Apr, [Last accessed on 2015 Aug 17].
View at Publisher | View at Google Scholar - Hulka, B., Zyzanski, S., Cassel, J. and Thompson, S. (1970), “Scale for the measurement of attitudes towards physicians and primary medical care”, Medical Care, Vol. 8 No. 5, pp. 429-436.
View at Publisher | View at Google Scholar - Hurwitz EL, Morgenstern H, Yu F. (2005) Satisfaction as a predictor of clinical outcomes among chiropractic and medical patients enrolled in the UCLA low back pain study. Spine (Phila Pa 1976) 30(19):2121–2128.
View at Publisher | View at Google Scholar - Husebo, B. S., Ballard, C. & Aarsland, D. (2011). Pain Treatment of Agitation in Patients with Dementia: A Systematic Review. International Journal of Geriatric Psychiatry, 26, 1012–1018.
View at Publisher | View at Google Scholar - Jensen MP, Mendoza T, Hanna DB, Chen C, Cleeland CS. (2004) The analgesic effects that underlie patient satisfaction with treatment. Pain. 110(1–2):480–487.
View at Publisher | View at Google Scholar - Johannes, C. B., Le, T. K., Zhou, X., Johnston, J. A. & Dworkin,R.H.(2010).ThePrevalenceofChronicPainin United States Adults: Results of an Internet-Based Survey. The Journal of Pain, 11, 1230–1239.
View at Publisher | View at Google Scholar - Dysvik, E., Natvig, G. K., Eikeland, O. J. & Lindstrøm, T. C. (2005). Coping with chronic pain. International Journal of Nursing Studies, 42, 297–305.
View at Publisher | View at Google Scholar - Fink, R. & Gates, R. (2006). Pain Assessment. Edit. In: Ferrell, B.R. & Coyle, N. 2006. Textbook of Palliative Nursing. 2nd Edition. Oxford Press Inc. USA. 99, 102, 106, 110
View at Publisher | View at Google Scholar - Fitzpatrick, R. and Hopkins, A. (1983), “Problems in the conceptual framework of patient satisfaction research: an empirical exploration”, Sociology of Health & Illness, Vol. 5 No. 3, pp. 297-311.
View at Publisher | View at Google Scholar - Gonzalez, N., Quintana, J.M., Bilbao, A., Escobar, A., Aizpuru, F., Thompson, A., Esteban, C., Sebastian, J.A.S. and de la Sierra, E. (2005), “Development and validation of an in-patient satisfaction questionnaire”, International Journal for Quality in Health Care, Vol. 17 No. 6, pp. 465-472.
View at Publisher | View at Google Scholar - Hawthorne, G. (2006), Review of Patient Satisfaction Measures, Australian Goverment Department of Health and Ageing, Canberra.
View at Publisher | View at Google Scholar - Hood, C. (1995), “The new public management in the 1980s: variations on a theme”, Journal of Accounting, Organizations and Society, Vol. 20 Nos 2/3, pp. 93-109.
View at Publisher | View at Google Scholar - Jenkinson C, Coulter A, Bruster S, Richards N, Chandola T. (2003) Patients' experience and satisfaction with Health Care: Results of a questionnaire study of specific aspects of care. Quality Safety Health Care, VOL 11:335-339 .
View at Publisher | View at Google Scholar - José M. Q.,Nerea, G.,Amaia, B., Felipe, A., Antonio, E.,Cristóbal, E., José, A., S., Emilio, S. and Andrew, T. (2006). Predictors of patient satisfaction with hospital health care, Health Services Research, Vol: 6, NO.102
View at Publisher | View at Google Scholar - Juran J. (1998). Juran on Planning for Quality. Νέα Υόρκη:The Free.
View at Publisher | View at Google Scholar - Ibrahim A, Chompikul J, Isaranurug S. (2008) Patient satisfaction with health services at the outpatient department of Indira Gandhi memorial Hospital, Male’Maldives. Journal of public health and development. 6(1): 144-152.
View at Publisher | View at Google Scholar - Iftikhar, A., Allah N., Shadiullah, K., Habibullah, K., Muhammad, A., R.,Muhammad, H., K. (2011). PREDICTORS OF PATIENT SATISFACTION,Gomal Journal of Medical Sciences, Vol: 9, No. 2, pp.: 183188.
View at Publisher | View at Google Scholar - International Association for Hospice and Palliative Care. Opioid analgesics. http://www.hospicecare.com/manual/pain3.html Consulted March 24, 2012.
View at Publisher | View at Google Scholar - Kalso, E. & Vainio, A. (1993). Kipu. Duodecim: Helsinki. 197, 198
View at Publisher | View at Google Scholar - Käypä hoito recommendations. Palliative (symptomatic) care of (imminently) dying patients.
View at Publisher | View at Google Scholar - Kasunee, C. (2017). Patient satisfaction of services of the out-patient department, Base Hospital, Panadura. Journal of the College of Community Physicians of Sri Lanka 23, (2).
View at Publisher | View at Google Scholar - KengenTraska,T.,Rutledge,D.N.,Mouttapa,M.,Weiss,J.& Aquino, J. (2012). Strategies Used for Managing Symptoms by Women with Fibromyalgia. Journal of Clinical Nursing, 21, 626–635.
View at Publisher | View at Google Scholar - Kleinsorge, I.K. and Koenig, H.F. (1991), “The silent customers: measuring customer satisfaction in nursing homes”, Journal of Health Care Marketing, Vol. 11 No. 4, pp. 2-13.
View at Publisher | View at Google Scholar - Koch, H. (1991). Total Quality Management in Health Care, Longman.
View at Publisher | View at Google Scholar - Kohr, R., & Sawhney, M. (2005). Advanced practice nurses’ role in the treatment of pain. Canadian Nurse, 101(3), 30–34.
View at Publisher | View at Google Scholar - Kumari R, Idris M, Bhushan V, Khanna A, Agarwal M et al (2009). Study on patient satisfaction in the government allopathic health facilities of lucknow district, India. Indian J. Comm. Med. 34(1):35-42.
View at Publisher | View at Google Scholar - Larsen, D. (2007). Pain Management in Nursing: What Does It Mean? [Cited 18 Mar 2014.]
View at Publisher | View at Google Scholar - Lapane, K. L., Quilliam, B. J., Chow, W., & Kim, M. (2012). The association between pain and measures of well-being among nursing home residents. Journal of the American Medical Directors Association, 13(4), 344–349
View at Publisher | View at Google Scholar - Larsen, D.L., Attkisson, C.C., Hargreaves, W.A. and Nguyen, T.D. (1979), “Assessment of client/patient satisfaction: development of a general scale”, Evaluation and Program Planning, Vol. 2 No. 3, pp. 197-207.
View at Publisher | View at Google Scholar - Lee, P.-M., Khong, P. and Ghista, D.N. (2006), “Impact of deficient healthcare service quality”, The TQM Magazine, Vol. 18 No. 6, pp. 563-571.
View at Publisher | View at Google Scholar - Lesage, P. & Portenoy, R.K. (1999) Trends in Cancer Pain Management. Cancer Control; Journal of the Moffit Cancer Center. Vol. 6, No 2.
View at Publisher | View at Google Scholar - Lewandowski, W., Morris, R., Draucker, C. B. & Risko, J. (2007). Chronic Pain and the Family: Theory-Driven Treatment Approaches. Issues in Mental Health Nursing, 28, 1019–1044.
View at Publisher | View at Google Scholar - Lin, B. and Kelly, E. (1995), “Methodological issues in patient satisfaction surveys”, International Journal of Health Care Quality Assurance, Vol. 8 No. 6, p. 32.
View at Publisher | View at Google Scholar - Linder-Pelz, S. (1982), “Toward a theory of patient satisfaction”, Social Science & Medicine, Vol. 16 No. 5, pp. 577-582.
View at Publisher | View at Google Scholar - Lynch, M. E. (2011). The need for a Canadian pain strategy. Pain Research and Management, 16(2), 77–80.
View at Publisher | View at Google Scholar - Maier, C. H., Nestler, N., Richter, H., Hardinghaus, W., Poqatzki-Zahn, E., Zenz, M., & Osterbrink, J. (2010). The quality of pain management in German hospitals. Deutsches Arzteblatt International, 107(36), 607–614.
View at Publisher | View at Google Scholar - McCaffery, M. & Beebe, A. (1989). Pain. Clinical Manual for Nursing Practice The C.V. Mosby Company, USA. 1, 4, 19, 20, 47, 172, 188-190,
View at Publisher | View at Google Scholar - McCarberg, B. H., Nicholson, B. D., Todd, K. H., Palmer, T., & Penles, L. (2008). The impact of pain on quality of life and the unmet needs of pain management: Results from pain sufferers and physicians participating in an Internet survey. American Journal of Therapeutics, 15(4), 312–320.
View at Publisher | View at Google Scholar - Medical Center of McKinney, (2012). Therapeutic touch.
View at Publisher | View at Google Scholar - Meterko, M., Nelson, E.C., Rubin, H.R., Batalden, P., Berwick, D.M., Hays, R.D. and Ware, J.E. Jr (1990),“Patientjudgments ofhospitalquality:reportofapilotstudy”,MedicalCare,Vol.28 No. 9, pp. S1-S56.
View at Publisher | View at Google Scholar - Milutinovic D, Simin D, Brkic N, Brkic S. (2012) The patient satisfaction with nursing care quality: the psychometric study of the Serbian version of PSNCQ questionnaire. Scand J Caring 26:598-606.
View at Publisher | View at Google Scholar - Mystakidou, K., Mendoza, T., Tsilika, E., Befon, S., Parpa, E., Bellos, G., Vlahos, L., Cleeland, C. (2001). Greek brief pain inventory: validation and utility in cancer pain. Oncology 60(1): 35-42
View at Publisher | View at Google Scholar - Nakamura, M., Nishiwaki, Y., Ushida, T. & Toyama, Y. (2014). Prevalence and Characteristics of Chronic Musculoskeletal Pain in Japan: A Second Survey of People with or without Chronic Pain. Journal of Orthopaedic Science, 19, 339–350.
View at Publisher | View at Google Scholar - Nguyen, T.D., Attkisson, C.C. and Stegner, B.L. (1983), “Assessment of patient satisfaction: development and refinement of a service evaluation questionnaire”, Evaluation and Program Planning, Vol. 6 Nos 3-4, pp. 299-313.
View at Publisher | View at Google Scholar - Nguyen Thi PL, Briançon S, Empereur F, Guillemin F. (2002) Factors determining inpatient satisfaction with care. Soc Sci Med 54(4):493-504.
View at Publisher | View at Google Scholar - Nuñez, D. E., Keller, C. & Ananian, C. D. (2009). A Review of the Efficacy of the Self-Management Model on Health Outcomes in Community-Residing Older Adults with Arthritis. Worldviews on Evidence-Based Nursing, 6, 130–148.
View at Publisher | View at Google Scholar - Oakland, J. (1991). Total Quality Management, 2η έκδοση, Heinemann.
View at Publisher | View at Google Scholar - O’Connor, S.J. and Shewchuk, R. (2003), “Commentary – patient satisfaction: what is the point?”, Health Care Management Review, Vol. 28 No. 1, pp. 21-24.
View at Publisher | View at Google Scholar - Oliver, S. & Ryan, S. (2004). Effective Pain Management for Patients with Arthritis. Nursing Standard, 18, 43–52; quiz 54, 56.
View at Publisher | View at Google Scholar - Otani K, Herrmann PA, Kurz RS. (2011) Improving patient satisfaction in hospital care settings. Health Serv Manage Res 24(4):163-169.
View at Publisher | View at Google Scholar - Oyvind A. B., Ingeborg, S., S., &Hilde, H., I. (2011). Overall patient satisfaction with hospitals: effects of patient-reported experiences and fulfillment of expectations, British Medical Journal Quality Safety
View at Publisher | View at Google Scholar - Panteli V, Patistea E. (2007) Assessing patients' satisfaction and intensity of pain as outcomes in the management of cancer-related pain. Eur J Oncol Nurs. 11(5):424–433.
View at Publisher | View at Google Scholar - Parasuraman A., Zeithaml V. & Berry L. (1988). Servqual: A Muliple-Item Scale for Measuring Perceptions of Service Quality. Journal of Retailing, 64, 12-40.
View at Publisher | View at Google Scholar - Partheniadis, S., Intas, G., Nikolopoulou, V., Theofilou, P. (2022). The role of demographic features in patients’ satisfaction from healthcare: A cross sectional study using PSQ-18. EC Nursing & Healthcare, 4.11, 1-15
View at Publisher | View at Google Scholar - Pascoe, G.C. (1983), “Patient satisfaction in primary health care: a literature review and analysis”, Evaluation and Program Planning, Vol. 6 Nos 3-4, pp. 185-210.
View at Publisher | View at Google Scholar - Planton,J.&Edlund,B.J.(2010).RegulatoryComponentsfor Treating Persistent Pain in Long-Term Care. Journal of Gerontological Nursing, 36, 49–56.
View at Publisher | View at Google Scholar - Prkachin, K. M., Solomon, P. E., & Ross, J. (2007). Underestimation of pain by health-care providers: Towards a model of the process of inferring pain in others. Canadian Journal of Nursing Research, 39(2), 88–106.
View at Publisher | View at Google Scholar - Radwany, S.M. & Von Grueningen, V.E. 2012. Palliative and End-of-Life Care For Patients With Ovarian Cancer. Clinical Obstetrics and Gynecology. Vol. 55, Consulted on May 17, 2012. 176-177, 180
View at Publisher | View at Google Scholar - Rama M, Kanagaluru S. K. (2011) A STUDY ON THE SATISFACTION OF PATIENTS WITH REFERENCE TO HOSPITAL SERVICES, International Journal of Business Economics & Management Research, Vol.:1, NO. 3
View at Publisher | View at Google Scholar - Rashmi, & Vijaykumar, B. (2010). Assessment of the Quality of Service Given by Health Care Provider about Tuberculosis in RNTCP. Indian journal of community medicine : official publication of Indian Association of Preventive & Social Medicine, 35(2), 368–369.
View at Publisher | View at Google Scholar - Rau, K. (2017). Cancer-related pain: a nationwide survey of patients' treatment modification and satisfaction in Taiwan. Japanese Journal of Clinical Oncology 14, (11).
View at Publisher | View at Google Scholar - Registered Nurses’ Association of Ontario. (2007). Assessment and management of pain. Nursing best practice guideline: Shaping the future of nursing.Toronto: Author. Retrieved August 18, 2014,
View at Publisher | View at Google Scholar - Reid, M. C., Papaleontiou, M., Ong, A., Breckman, R., Wethington, E. & Pillemer, K. (2008). Self-Management Strategies to Reduce Pain and Improve Function among Older Adults in Community Settings: A Review of the Evidence. Pain Medicine, 9, 409–424.
View at Publisher | View at Google Scholar - Reltsma, M. L., Tranmer, J. E., Buchanan, D. M., & Vandenkerkhof, E. G. (2011). The prevalence of chronic pain and pain-related interference in the Canadian population from (1994). Chronic Diseases and Injuries in Canada, 31(4), 157–164. Retrieved August 18, 2014,
View at Publisher | View at Google Scholar - Richardson, C., Adams, N. & Poole, H. (2006). Psychological Approaches for the Nursing Management of Chronic Pain: Part 2. Journal of Clinical Nursing, 15, 1196–1202.
View at Publisher | View at Google Scholar - Shin, S. Y. & Kolanowski, A. M. (2010). Best Evidence of Psychosocially Focused Nonpharmacologic Therapies for Symptom Management in Older Adults with Osteoarthritis. Pain Management Nursing, 11, 234–244.
View at Publisher | View at Google Scholar - Sitzia, J. (1999), “How valid and reliable are patient satisfaction data? An analysis of 195 studies”, International Journal for Quality in Health Care, Vol. 11 No. 4, pp. 319-328.
View at Publisher | View at Google Scholar - Smalbrugge, M., Jongenelis, L. K., Pot, A. M., Beekman, A. T. & Eefsting, J. A. (2007). Pain among Nursing Home Patients in the Netherlands: Prevalence, Course, Clinical Correlates, Recognition and Analgesic Treatment–an Observational Cohort Study. BMC Geriatrics, 7, 3.
View at Publisher | View at Google Scholar - Sodani PR, Sharma K. (2011) Assessing Indian public health standards for community health centers: a case study with special reference to essential newborn care services. Indian J Public Health. 55(4):260-266.
View at Publisher | View at Google Scholar - Sofaer, S. and Firminger, K. (2005), “Perceptions of the quality of health services”, Annual Review of Public Health, Vol. 26 No. 1, pp. 513-559.
View at Publisher | View at Google Scholar - Strasser, S., Aharony, L. and Greenberger, D. (1993), “The patient satisfaction process: moving toward a comprehensive model”, Medical Care Review, Vol. 50 No. 2, pp. 219-245.
View at Publisher | View at Google Scholar - Takai, Y., Yamamoto-Mitani, N., Okamoto, Y., Koyama, K. & Honda, A. (2010). Literature Review of Pain Prevalence among Older Residents of Nursing Homes. Pain Management Nursing, 11, 209–223.
View at Publisher | View at Google Scholar - Taylor, S.A. (1999), “Distinguishing service quality from patient satisfaction in developing health care marketing strategies”, Hospital and Health Services Administration, Vol. 39 No. 2, pp. 221-236.
View at Publisher | View at Google Scholar - The British Pain Society. (2010). Cancer Pain Management.. 5-6, 75
View at Publisher | View at Google Scholar - Thomas, E.M. & Weiss, S.M. (2012) Nonpharmacological Interventions with Chronic Cancer Patient in Adults. Cancer Control Vol. 7 N.o 2, 2000.
View at Publisher | View at Google Scholar - Tonio S, Joerg K, Joachim K. (2011) Determinants of patient satisfaction: a study among 39 hospitals in an in-patient setting in Germany. International Journal for Quality in Health Care, 23(5):503-509 .
View at Publisher | View at Google Scholar - Turris, S.A. (2005), “Unpacking the concept of patient satisfaction: a feminist analysis”, Journal of Advanced Nursing, Vol. 50 No. 3, pp. 293-298.
View at Publisher | View at Google Scholar - Urden, K.D. (2002), “Patient satisfaction measurement: current issues and implications”, Outcomes Management, Vol. 6 No. 6, pp. 125-31.
View at Publisher | View at Google Scholar - van Campen, C., Sixma, H., Friele, R.D., Kerssens, J.J. and Peters, L. (1995), “The quality of care and patient satisfaction: a review of measuring instruments”, Medical Care Research and Review, Vol. 52 No. 1, pp. 109-33.
View at Publisher | View at Google Scholar - Ware E., Snyder K., Wright R. & Davies R. (1976) Defining and measuring patient satisfaction with medical care. Evaluation and Program Planning6, 247-263.
View at Publisher | View at Google Scholar - White B. (1999) Measuring Patient Satisfaction: How to Do It and Why to Bother Family Practice Management.
View at Publisher | View at Google Scholar - Woodruff, R. 2004. Palliative medicine. Evidence-based symptomatic and supportive care for patients with advanced cancer. 4th edition. United Kingdom: Oxford. 54, 69, 73, 74, 76, 78
View at Publisher | View at Google Scholar - Wrede-Seaman, L. (2001). Treatment options to manage pain at the end of life. American Journal of Hospice and Palliative Care. Vol. 18 No. 2. 2001. 89, 97, 106
View at Publisher | View at Google Scholar - Wadensten, B., Fröjd, C., Swenne, C. L., Gordh, T., & Gunningberg, L. (2011). Why is pain still not being assessed adequately? Results of a pain prevalence study in a university hospital in Sweden. Journal of Clinical Nursing, 20(5–6), 624–634.
View at Publisher | View at Google Scholar - Ware, J.E., Snyder, M.K., Wright, W.R. and Davies, A.R. (1983), “Defining and measuring patient satisfaction with medical care”, Evaluation and Program Planning, Vol. 6 Nos 3-4, pp. 247-263.
View at Publisher | View at Google Scholar - Ware, J.E. Jr and Snyder, M.K. (1975), “Dimensions of patient attitudes regarding doctors and medical care services”, Medical Care, Vol. 13 No. 8, pp. 669-682.
View at Publisher | View at Google Scholar - West, C., Stewart, L., Foster, K. & Usher, K. (2012). The Meaning of Resilience to Persons Living with Chronic Pain:AnInterpretiveQualitativeInquiry.JournalofClinical Nursing, 21, 1284–1292.
View at Publisher | View at Google Scholar - West, C., Usher, K. & Foster, K. (2011). Family Resilience: Towards a New Model of Chronic Pain Management. Collegian, 18, 3–10.
View at Publisher | View at Google Scholar - Williams, B. (1994), “Patient satisfaction: a valid concept?”, Social Science & Medicine, Vol. 38 No. 4, pp. 509-516.
View at Publisher | View at Google Scholar
