

Research Article | DOI: https://doi.org/10.31579/2834-8087/020
Inducible Nitric Oxide Synthase Expression in Benign and Malignant Breast Lesions; Evaluation of Correlation with Prognostic Factors and Survival analysis
1 Cancer Research Center, Shohada-e Tajrish Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2 Department of Biology, Roudehen Branch, Islamic Azad University, Roudehen, Iran.
3 School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Zahra Tahmasebi Fard, Department of Biology, Roudehen Branch, Islamic Azad University, Roudehen, Iran.
Citation: Mahsa Ahadi, Zahra Tahmasebi Fard, Masoud Baikpour, (2023), Inducible Nitric Oxide Synthase Expression in Benign and Malignant Breast Lesions; Evaluation of Correlation with Prognostic Factors and Survival analysis, Archives of Clinical Investigation, 2(3); DOI:10.31579/2834-8087/020
Copyright: © 2023, Zahra Tahmasebi Fard. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 February 2023 | Accepted: 24 May 2023 | Published: 02 June 2023
Keywords: breast cancer; nitric oxide synthase; human epidermal growth factor receptor 2; estrogen receptor; progesterone receptor
Abstract
Studies have suggested a dose dependent biphasic role for nitric oxide (NO) in tumorigenesis. The present study aimed to conduct further investigations on this subject by comparing inducible NOS (iNOS) expression between normal breast tissues, benign lesions and malignant tumors. The obtained tissue specimens were prepared and underwent immunohistochemical analyses to evaluate the expression of iNOS, HER2, ER and PR. A total of 110 participants were included in this survey. iNOS expression showed a negative correlation with ER (p=0.008) and PR (p=0.016) and a positive association with HER2 expression (p=0.007). Strong staining had a significant correlation with the patients’ diagnosis (p=0.034) and lymph node involvement (p=0.023). Univariate analyses found negative ER (HR=17.7, p<0.001), negative PR (HR=16.0, p<0.001), grade-3 tumors (HR=4.0, p=0.011) and triple negativity (HR=26.1, p<0.001) to be associated with lower survivals. Multivariate analysis showed that the lesion being triple negative had the worst effect on survival of patients (HR=47.4, p=0.003), followed by positive iNOS expression (HR=7.9, p=0.007) and grade-3 lesions (HR=7.5, p=0.020). This study showed that iNOS is expressed to a greater intensity in malignant breast lesions, compared to normal breast tissue and benign lesions. Its expression was also found to negatively affect survival of the patients.
Introduction
Nitric oxide (NO) is an intracellular second messenger that plays important roles in various regulatory mechanisms within biological systems such as signal transmission in neurons, vasodilatation, relaxation of smooth muscles, and cytotoxic effects of neutrophils and macrophages (1). This free radical gas is generated during conversion of L-arginine to L-citrulline by nitric oxide synthase (NOS). This enzyme is present in three isoforms that are classified into two groups of calcium dependent constitutive (cNOS) and calcium independent inducible (iNOS or NOS2). The former group includes the two endothelial (eNOS) and neuronal (nNOS) isoforms that mediate vasodilatation and neurotransmission, respectively. Whereas, iNOS is mainly involved in macrophage-induced cytotoxicity and tumor-related immunosuppression, and upon stimulation by proinflammatory cytokines, generates a much greater amount of NO compared to the other two isoforms(2). Studies have suggested a dose dependent biphasic role for NO in tumorigenesis, inhibiting tumor growth at high levels while promoting angiogenesis at low concentrations (3). The dual roles of this diatomic molecule have been reported to affect cell proliferation and migration, apoptosis, DNA damage and protection against cytotoxicity (4-7). The variations in the effects of NO could also be attributed to the micro environmental factors including the local concentration of superoxide and oxygen tension in the target tissue. In this regard, multiple studies focused on NOS expression and reported aberrant expression of the two eNOS and iNOS isoforms of this enzyme in tissues obtained from different malignant human cancers including head and neck (8), colon, Breast, prostate, Bladder, Skin, Esophagus (9), Endometrial, Cervical, lung, Gastric and brain cancers (10) and etc. The role of NOS in human breast cancer was first evaluated by Thomsen et al. in 1995 (11). Their study paved the way for further investigations about this correlation on various benign and malignant breast lesions, but these studies have yielded conflicting results and no consensus has been reached yet (12-20). Considering the disagreements between studies on the role of iNOS in breast carcinomas, and the lack of sufficient information on the correlation between iNOS expression and prognostic factors such as lymph node involvement, positivity of hormone receptors and grade of the tumor along with survival of the patients, the present study aimed to provide further evidence on this subject by comparing iNOS expression between specimens obtained from normal breast tissues, benign lesions and malignant tumors.
Materials and Methods:
Materials and Methods:
Study design and sample population:
The target population in this cross-sectional study included patients who had undergone resection of specimens from their breast tissues for various reasons in Shohadaye Tajrish hospital during 2019. Using convenience sampling method, a total of 110 subjects were recruited for the study, of which 12 were included as the control group with their specimens resected during breast reduction mammoplasty, 14 subjects had ductal hyperplasia, 21 had ductal carcinoma in situ (DCIS) and 63 patients were diagnosed with invasive breast cancer. Immunohistochemical evaluations were performed on the resected specimens obtained from the participants to evaluate the positivity of ER, PR, HER2 and iNOS in epithelial component of their breast tissues. If not available in their medical records, information about the final outcome of patients with invasive breast cancer was acquired by contacting them or their families, and if expired, the time of their death was recorded to be used in survival analysis.
Immunohistochemistry:
Representative paraffin-embedded tissue blocks were sectioned at 3 µm thickness, transferred onto polylysine-coated microslides and deparaffinized. A pressure cooker was used to boil the slides for 5 min at a pressure of 103 kPa after immersion in Reveal Emulgator (Biocarta, Hamburg, Germany) for antigen retrieval. The sections were washed in distilled water and phosphate buffered saline and then exposed to Aurion-BSA-c10% (Aurion, Wageningen, Netherlands) to block binding of unspecific agents. The slides were then subjected to the rabbit-derived primary monoclonal anti-iNOS antibody (Biosciences Pharmingen, Heidelberg, Germany) for at least 3 hours at room temperature. Subsequently, they were washed with PBS before and after undergoing 15 min of incubation with biotinylated secondary antibody. The sections were then incubated with Streptavidin-horseradish peroxidase (HRP) conjugate for 15 min. After being washed again with PBS, amino-ethyl carbazole (Vector Laboratories, Burlingame, CA, USA) was used as chromogen and haematoxylin was used for nuclear counterstaining. Slides prepared from iNOS positive colon carcinoma specimens were considered as positive controls, while section with no exposure to the primary antibody were considered as negative controls. Mouse-derived anti-estrogen receptor (ER) and anti-progesterone receptor (PR) monoclonal antibodies (DAKO, Carpinteria, CA, USA) were used for evaluating the expression of these two hormone receptors. The immunostaining process for these markers was similar to that of iNOS, except for an incubation period of 25 min. A steamer was used before treatment for antigen retrieval during HER2 immunohistochemistry assessment. Incubation of sections with diluted (1:4000) polyclonal anti-c-erb-B2 antibody (DAKO, oncoprotein) was done for 25 min, followed by detection using LSAB-kit.
Microscopic assessments:
Staining of sections for iNOS was evaluated according to the scoring system proposed by Soini et al. (21). In this system, cytoplasmic staining of the cells determined iNOS positivity which was assessed in two concepts of quantity and intensity. Quantity of staining was scored on a scale of 0-4 based on the proportion of the stained cells within the field, with 0 as no staining, 1 as less than 25%, 2 as 25-50%, 3 as 50-75% and 4 as greater than 75% staining. Intensity of staining was determined according to the visually estimated staining reaction, on a scale of 0-4 with 0 as no staining and 4 as a very strong reaction. Eventually, the total staining score was calculated for each section by adding the two quantity and intensity scores and was classified as three groups of no staining (total score=0), weak staining (total score=1-4) and strong staining (total score=5-8) (Figure 1).
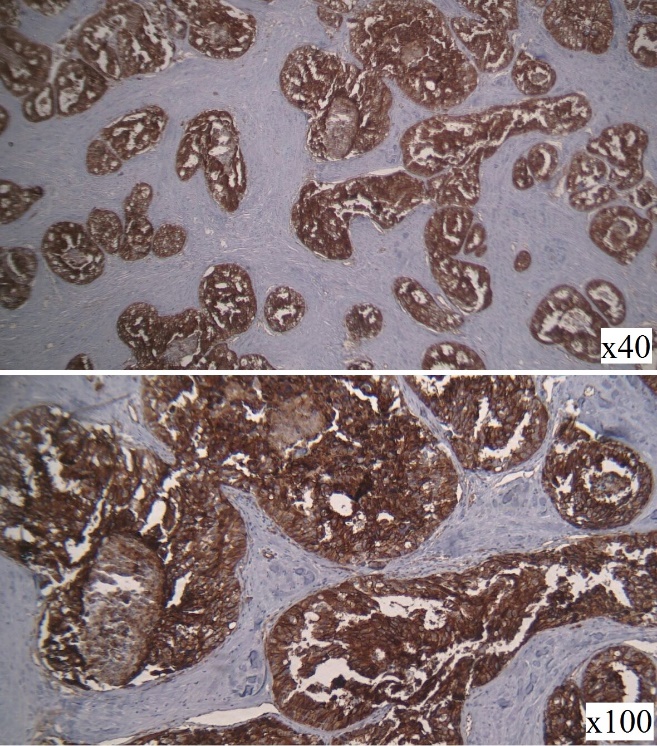
Figure 1: iNOS expression in epithelial component of invasive breast cancer tissue.
Staining for ER and PR were also evaluated and scored based on the Quick Score method (22). Similarly, in this scoring system the total score was calculated by adding the two staining intensity (1: weak, 2: moderate, 3: strong) and quantity (1: less than 25%, 2: 25 to 50%, 3: 50 to 75%, 4: greater than 75%) scores with the final classification of negative (total score=0-3) and positive (total score=4-7). HER2 expression was also scored semi-quantitatively on a scale of 0-3 as suggested by Wulfing et al. (23), 0 as membrane staining in ˂10% of tumor cells, 1+ as faint partial membrane staining in ˃10% of tumor cells, 2+ as weak to moderate membrane staining in ˃10% of tumor cells (borderline) and 3+ as strong staining of the entire membrane ˃10% of tumor cells. Sections scored as 0, 1+ (negative) and 2+ (equivocal) were considered as HER2-negative and 3+ was considered as HER2-positive.
Statistical analysis:
SPSS software for windows version 22.0 (IBM corp., Armonk, NY, USA) was used for data analysis (24). Considering the qualitative nature of all included variables in the study, descriptive findings were presented as frequency and percentage. Chi-squared test and Fisher’s Exact test were used to evaluate the correlations between these factors, as needed. Survival analysis in patients with invasive breast cancer was also performed using Kaplan-Meier method and the effects of included variables in the study on the survival of patients were assessed using the Peto’s Log-Rank test in univariate analyses. Factors with no linear correlation between each other that were found to yield a p value less than 0.1 in the univariate analysis were identified to be included in our multivariate Cox Regression model to determine the independent effects of these factors on survival of subjects. The results of these analyses were presented and Hazard Ratios (HR) and 95% Confidence Intervals (95%CI). Statistical significance was considered as a p value of less than 0.05 in all analyses.
Results:
Descriptive statistics:
As mentioned, a total of 110 participants were recruited in this survey, including 63 (57.3%) patients with invasive breast cancer, 21 (19.1%) with DCIS, 14 (12.7%) with ductal hyperplasia and 12 (10.9%) normal subjects. The descriptive statistics of the sample population are presented in Table 1.
Variables | Count | Percent | Variables | Count | Percent |
Group (n=110) | ER (n=39) | ||||
Normal | 12 | 10.9% | Negative | 17 | 43.6% |
Ductal Hyperplasia | 14 | 12.7% | Positive | 22 | 56.4% |
DCIS | 21 | 19.1% | PR (n=39) | ||
Invasive | 63 | 57.3% | Negative | 18 | 46.2% |
iNOS [removed]n=110) | Positive | 21 | 53.8% | ||
Negative | 82 | 74.5% | HER2 Score (n=40) | ||
Positive | 28 | 25.5% | 0-1+ (Negative) | 22 | 55.0% |
Weak | 17 | 15.5% | 2+ (Borderline) | 5 | 12.5% |
Strong | 11 | 10.0% | 3+ (Positive) | 13 | 32.5% |
Grade (n=48) | HER2 (n=40) | ||||
1 | 7 | 14.6% | Negative | 27 | 67.5% |
2 | 17 | 35.4% | Positive | 13 | 32.5% |
3 | 24 | 50.0% | Triple negative (n=39) | ||
Lymph node (n=55) | No | 31 | 79.5% | ||
Negative | 10 | 18.2% | Yes | 8 | 20.5% |
Positive | 45 | 81.8% |
|
|
|
Table 1: Descriptive statistics of evaluated variables
According to immunohistochemistry analyses, iNOS was expressed in 28 subjects (25.5%) with weak staining reported in 17 (15.5%) and strong staining observed in 11 (10.0%) participants. Grade of the tumor was recorded in 48 subjects out of the 63 patients with invasive breast cancer, among which 7 patients (6.4%) were reported to have grade 1 cancer, 17 (15.5%) had grade 2 and 24 (50.0%) had grade 3 breast carcinomas. Forty-five patients out of the 55 with recorded lymph node status (81.8%) were also found to have lymph node involvement. Considering the hormone receptors, 22/39 patients (56.4%) were ER-positive and 21/39 (53.8%) were PR-positive. HER2 expression was reported to be 0-1+ or negative in 22/40 (55.0%), 2+ or borderline in 5/40 (12.5%) and 3+ or positive in 13/40 (32.5%) patients. Accordingly, 8/39 (20.5%) patients were found to be triple negative. Patients diagnosed with invasive breast cancer were followed for an average of 25.4±12.7 months (ranging from 10 to 42 months), during which 15 (23.8%) were found to have expired. The overall survival for these patients was calculated to be 36.1 months (95%CI: 33.4-38.7).
Analytical statistics:
As presented in Table 2, iNOS expression was found to have a negative significant correlation with ER (p=0.008) and PR (p=0.016) positivity, while it showed a positive correlation with HER2 [removed]p=0.007). As for staining, a significantly greater proportion of patients diagnosed with invasive breast carcinoma were found to present with strong iNOS staining compared to the other 4 groups of subjects included (p=0.034). Lymph node involvement also showed a significant association with strong staining of the sections (p=0.023).
Variables | iNOS expression | P value | Staining | P value | ||
Negative (n=82) | Positive (n=18) | Weak (n=17) | Strong (n=11) | |||
Group | ||||||
Normal | 8 (66.7%) | 4 (33.3%) | 0.256 | 4 (100.0%) | 0 (0.0%) | 0.034 |
Ductal Hyperplasia | 9 (64.3%) | 5 (35.7%) |
| 5 (100.0%) | 0 (0.0%) |
|
DCIS | 19 (90.5%) | 2 (9.5%) |
| 1 (50.0%) | 1 (50.0%) |
|
Invasive | 46 (73.0%) | 17 (27.0%) |
| 7 (41.2%) | 10 (58.8%) |
|
Grade | ||||||
1 | 7 (100.0%) | 0 (0.0%) | 0.154 | 0 (0.0%) | 0 (0.0%) | 0.833 |
2 | 11 (64.7%) | 6 (35.3%) |
| 3 (50.0%) | 3 (50.0%) |
|
3 | 15 (62.5%) | 9 (37.5%) |
| 4 (44.4%) | 5 (55.6%) |
|
Lymph node | ||||||
Negative | 7 (70.0%) | 3 (30.0%) | 0.945 | 3 (100.0%) | 0 (0.0%) | 0.023 |
Positive | 31 (68.9%) | 14 (31.1%) |
| 4 (28.6%) | 10 (71.4%) |
|
ER | ||||||
Negative | 8 (47.1%) | 9 (52.9%) | 0.008 | 2 (22.2%) | 7 (77.8%) | 0.157 |
Positive | 19 (86.4%) | 3 (13.6%) |
| 2 (66.7%) | 1 (33.3%) |
|
PR | ||||||
Negative | 9 (50.0%) | 9 (50.0%) | 0.016 | 2 (22.2%) | 7 (77.8%) | 0.157 |
Positive | 18 (85.7%) | 3 (14.3%) |
| 2 (66.7%) | 1 (33.3%) |
|
HER2 Score | ||||||
0-1+ (Negative) | 17 (77.3%) | 5 (22.7%) | 0.015 | 3 (60.0%) | 2 (40.0%) | 0.071 |
2+ (Borderline) | 5 (100.0%) | 0 (0.0%) |
| 0 (0.0%) | 0 (0.0%) |
|
3+ (Positive) | 5 (38.5%) | 8 (61.5%) |
| 1 (12.5%) | 7 (87.5%) |
|
HER2 | ||||||
Negative | 22 (81.5%) | 5 (18.5%) | 0.007 | 3 (60.0%) | 2 (40.0%) | 0.071 |
Positive | 5 (38.5%) | 8 (61.5%) |
| 1 (12.5%) | 7 (87.5%) |
|
Triple negative | ||||||
No | 23 (74.2%) | 8 (25.8%) | 0.186 | 2 (25.0%) | 6 (75.5%) | 0.386 |
Yes | 4 (50.0%) | 4 (50.0%) |
| 2 (50.0%) | 2 (50.0%) |
|
Table 2: Correlation between iNOS expression and staining with evaluated variables in the study
Table 3 presents the results of univariate and multivariate analyses on the survival of patients with invasive breast carcinomas. According to the findings of univariate analyses, a negative ER (HR=17.7, p<0 HR=16.0, HR=4.0, p=0.011).> Count Events (%) Overall survival Mean (95% CI) Univariate analysis Multivariate analysis HR (95% CI) P value HR (95% CI) P value Triple negative No 31 8 (25.8%) 37.8 (35.3-40.3) 26.1 (6.4-107.2) <0> 47.4 (3.9-580.5) 0.003 Yes 8 7 (87.5%) 17.0 (12.1-21.9) iNOS expression Negative 46 8 (17.4%) 37.8 (35.1-40.4) 2.4 (0.9-6.6) 0.093 7.9 (1.7-35.4) 0.007 Positive 17 7 (41.2%) 32.2 (26.4-37.9) Grade 1 7 1 (14.3%) 41.7 (41.1-42.2) 4.0 (1.4-11.5)a 0.011a 7.5 (1.4-41.7)a 0.020a 2 17 3 (17.6%) 39.6 (37.3-41.9) 3 24 9 (37.5%) 30.3 (25.7-34.9) ER Negative 17 12 (70.6%) 25.0 (20.0-29.9) 17.7 (3.8-82.7) <0> - - Positive 22 3 (13.6%) 40.2 (38.2-42.2) PR Negative 18 12 (66.7%) 25.7 (20.8-30.6) 16.0 (3.4-75.5) <0> - - Positive 21 3 (14.3%) 40.1 (38.1-42.2) Staining Weak 7 1 (14.3%) 37.6 (29.5-45.6) 4.1 (0.5-34.4) 0.192 - - Strong 10 6 (60.0%) 27.8 (22.1-33.6) Lymph node Negative 10 2 (20.0%) 40.6 (39.0-42.2) 1.8 (0.4-9.3) 0.448 - - Positive 45 13 (28.9%) 35.5 (32.4-38.6) HER2 Negative 27 10 (37.0%) 33.8 (29.4-38.2) 1.1 (0.4-3.5) 0.794 - - Positive 13 5 (38.5%) 33.7 (29.6-37.9) HER2 Score 0-1+ (Negative) 22 9 (40.9%) 32.7 (27.5-37.9) 1.0 (0.6-1.8) 0.965 - - 2+ (Borderline) 5 1 (20.0%) 38.0 3+ (Positive) 13 5 (38.5%) 33.7 (29.6-37.9) a Grade 3 lesions were compared to the other two groups combined
Table 3: The results of univariate and multivariate analyses evaluating the effects of included variables on survival of patients
Moreover, subjects with negative expression of ER, PR and HER2, known as having a triple negative lesion, were also found to have lower survivals compared to other patients with a positive result for at least one of these three markers (HR=26.1, p<0 p=0.093)>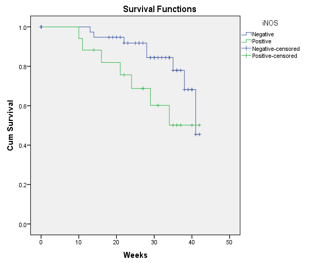
Figure 2: Overall survival of patients with invasive breast cancer according to their iNOS expression status
Among the variables with p values less than 0.1 in our univariate analyses, considering the linear correlation between expression of ER and PR and the lesion being triple negative, the latter was selected to be included in the multivariate analysis due to its higher HR. Other than that, grade of the tumor and iNOS expression were also included in our Cox regression model. According to the findings of this analysis, the lesion being triple negative had the worst effect on the survival of patients (HR=47.4, p=0.003), which was followed by iNOS [removed]HR=7.9, p=0.007) and grade 3 lesions (HR=7.5, p=0.020).
Discussion:
The present study used immunohistochemical methods to evaluate iNOS expression in a sample of Iranian patients diagnosed with ductal hyperplasia, DCIS and invasive breast cancer along with 12 normal subjects as the control group. The findings of this study showed that iNOS expression had a negative significant correlation with ER and PR positivity, and a positive correlation with HER2 expression. Strong iNOS staining was also found to be correlated with the diagnosis of invasive breast carcinoma and positive lymph node involvement. Survival analysis found the overall survival to be significantly lower in patients with negative ER, negative PR, grade 3 tumors and triple negative lesions. According to the findings of multivariate analysis, the lesion being triple negative had the worst effect on the survival of patients, which was followed by positive iNOS expression and grade 3 lesions. So this study showed that iNOS is expressed to a greater intensity in malignant breast lesions, compared to normal breast tissue and benign lesions. Its expression was also found to negatively affect survival of the patients. As mentioned, iNOS is one of the three isoenzymes than generate NO from L-arginine and this molecule is involved in various physiological functions. Although the exact role of NO in carcinogenesis and tumor growth has not been clearly identified yet, current literature suggests that based on its target organ, this radical gas exerts a dose-dependent biphasic effect on angiogenesis, apoptosis and adhesion of tumor cells (25-27). Of the three NOS enzymes, iNOS seems to have drawn the most attention due to its longer activity and the significantly higher concentrations of NO it can generate (28). Expression of this isoform has been reported in malignant lesions originated from multiple organs including liver, colon, pancreas, bladder, prostate, larynx, esophagus, lung and brain (9, 11, 21, 29). As for breast lesions, iNOS expression has been reported to be positive in 35 to 78 percent of patients with malignant breast cancers (13- 15, 18- 19, 30). In 1997, Dueñas-Gonzalez et al. evaluated a sample of 22 patients with primary breast tumors and found a strong correlation between iNOS expression and axillary lymph node metastasis. They also reported a significant correlation between expression of this enzyme with absence of nm23 protein which is believed exert anti-metastatic effects (13). Although in the present study, lymph node involvement was not associated with iNOS expression, but strong iNOS staining was found to be significantly correlated with lymph node metastasis. Two years later, Tschugguel et al. assessed iNOS expression in tissue samples obtained from 40 patients with grade 2 and 40 patients with grade 3 invasive ductal carcinomas, 50 patients with benign fibrocystic disease and 4 normal subjects after reduction mammoplasty. In contrast with our findings, these researchers reported a significantly higher proportion of cells to express iNOS in sections from benign lesions and grade 2 invasive ductal breast carcinomas compared to grade 3 tumors. They concluded that iNOS expression might play an inhibitory role in metastatic process in breast cancer (15). In the same year, Reveneau et al. evaluated iNOS expression in 8 benign lesions and 40 breast carcinomas. Their findings were also incongruent with ours as they reported a negative correlation between NOS activity and proliferation of tumor cells, an association between NOS activity and PR expression, and a significantly higher NOS activity in low grade tumors. In vitro assessments they conducted on MCF-7 breast cancer cells also confirmed their findings as cytokines induced iNOS expression and the resulting NO inhibited proliferation of these cells (14). In another study conducted in 2000, Vakkala et al. included 43 in situ and 68 invasive breast carcinomas. They reported significantly higher iNOS positivity in invasive carcinomas (58.8%) compared to in situ lesions (46.5%) and the percentage increased with increasing grade of the tumor. They also found increased vascularization and higher apoptotic indices in iNOS positive lesions (17). In agreement with their results, we also found strong staining to be more prevalent in higher grade lesions but the differences were insignificant. In their first study published in 2002, Loibl et al. performed immunohistochemical analysis on tissues obtained from 14 benign lesions, 9 in situ and 54 invasive breast carcinomas. They found iNOS positivity in 67% of in situ lesions and 61% of invasive breast cancers. Incompatible with our results, they reported a significant association between simultaneous iNOS and eNOS positivity and absence of lymph node involvement (18). In their next study published three years later in 2005, Loibl et al. included 161 primary breast cancer tissues and evaluated the correlation of their iNOS staining patterns with prognostic factors and patients’ survival. Based on their findings, iNOS positivity was significantly correlated with tumor size and decreasing differentiation of tumor cells. Survival analysis in these patients showed a remarkably worse overall survival in iNOS positive patients compared to iNOS negative subjects. However, in their multivariate analysis, iNOS expression was not identified as an independent prognostic factor for overall survival, whereas lymph node involvement and grading of the tumor were reported to be independently predictive of the survival (20). The findings of this survey was quite compatible with our results, but we found iNOS positivity to be correlated with ER, PR and HER2 expression, found no significant association between grading of the tumor and iNOS expression, and instead of lymph node metastasis, found triple negativity as the strongest prognostic factor for overall survival of patients. In another study published in 2005, Bulut et al. assessed iNOS expression in 100 invasive ductal carcinomas, 20 ductal hyperplasias, 20 fibroadenomas and 11 normal breast tissues. They reported iNOS immunoreactivity in 78% of malignant lesions and the intensity and quantity of iNOS staining was found to be significantly higher in these lesions compared to benign specimens. No significant correlation was observed between iNOS positivity and grading, lymph node involvement and ER expression. Disease free survival was evaluated in 50 subjects with negative lymph node involvement, in whom iNOS expression showed a negative correlation with survival (19). The findings of this study also had some discrepancies with our results, but the two surveys were in agreement considering the higher iNOS expression in malignant lesions and the overall negative association of this enzyme with worse outcome of the patients. Glynn et al. evaluated iNOS expression in 248 breast tumors and investigated its correlation with survival of patients in 2010. Their multivariate survival analysis found increased iNOS to predict inferior five-year and ten-year survivals in patients with ER negative lesions. Expression of iNOS was also associated with prognostic basal-like transcription pattern and other markers of poor prognosis including increased density of microvessels, frequency of p53 mutation and activated epidermal growth factor receptor. These researchers hypothesized that iNOS expression and the resulting increase in NO might lead to poor differentiation and aggressiveness of the tumor along with increased angiogenesis and inactivation of p53 gene (30). The findings of our survey were quite compatible with the results of this study; however, we found worse overall survivals in patients with positive iNOS expression, regardless of their ER status. Although the majority of these studies agree on the association between iNOS expression and negative prognostic factors in breast cancers such as grading of the tumor, lymph node involvement and hormonal receptor status, there are still considerable discrepancies between them that need to be addressed in future studies. Moreover, further investigations are required to determine the exact mechanism through which this enzyme affects breast cancer pathogenesis at different concentrations and to establish its role as a prognostic factor for patients’ survival and its possible application as a target for pharmaceutical treatments. One of the limitations of this study was the small sample population, which might have affected the results. Moreover, considering the methods of this study, there were considerable missing data in the patients’ medical records and survival analysis was performed on the basis of information acquired retrospectively through phone calls with the patients or their families, which subjects the results of this study to various biases. It is suggested that future studies on this topic include larger sample populations with a wider variety of breast lesions and follow patients prospectively to minimize the effects of recall bias in determining the role of iNOS expression as a prognostic factor. Considering the number of available literature on this subject, conducting a systematic review and meta-analysis might also be helpful. The findings of this study showed that iNOS expression had a negative significant correlation with ER and PR positivity, and a positive correlation with HER2 expression. Strong iNOS staining was also found to be correlated with the diagnosis of invasive breast carcinoma and positive lymph node involvement. Survival analysis found the overall survival to be significantly lower in patients with negative ER, negative PR, grade 3 tumors and triple negative lesions. According to the results of multivariate analysis, the lesion being triple negative had the worst effect on the survival of patients, which was followed by positive iNOS expression and grade 3 lesions.
Conflict of interest:
The authors have no conflicts of interest to declare.
Financial Support
The author received financial support from “Iran National Science Foundation Science, Deputy President” [Number: 92013932].
Acknowledgments:
The authors would like to express their gratitude to the medical personnel at Shohadaye Tajrish Hospital in Tehran and to all the patients who participated in this study.
References
- Bian K, Murad F. (2014) What is next in nitric oxide research? From cardiovascular system to cancer biology. Nitric Oxide. 43: 3-7.
View at Publisher | View at Google Scholar - Mattila JT, Thomas AC. (2014) Nitric oxide synthase: non-canonical expression patterns. Frontiers in immunology. 9(5);478.
View at Publisher | View at Google Scholar - Chinje EC, Stratford IJ . (1997) Role of nitric oxide in growth of solid tumours: a balancing act. Essays in biochemistry. 32: 61-72.
View at Publisher | View at Google Scholar - Wink DA, Cook JA, Pacelli R, Liebmann J, Krishna MC, (1995) Nitric oxide (NO) protects against cellular damage by reactive oxygen species. Toxicol Lett. 82-83:221-226.
View at Publisher | View at Google Scholar - Ambs S, Hussain S, Harris C. (1997) Interactive effects of nitric oxide and the p53 tumor suppressor gene in carcinogenesis and tumor progression. The FASEB Journal. 11:443-448.
View at Publisher | View at Google Scholar - Kim PK, Zamora R, Petrosko P, Billiar TR.(2001) The regulatory role of nitric oxide in apoptosis. International immunopharmacology.;1:1421-1441.
View at Publisher | View at Google Scholar - Pervin S, Singh R, Hernandez E, Wu G, Chaudhuri G. (2007) Nitric oxide in physiologic concentrations targets the translational machinery to increase the proliferation of human breast cancer cells: involvement of mammalian target of rapamycin/eIF4E pathway. Cancer Research. 67: 289-299.
View at Publisher | View at Google Scholar - Solomon I, Voiculescu VM, Caruntu C, Lupu M, Popa A, et al (2018).Neuroendocrine Factors and Head and Neck Squamous Cell Carcinoma: An Affair to Remember. Dis Markers.: 9787831.
View at Publisher | View at Google Scholar - James A. Crowell, Vernon E. Steele, Caroline C. Sigman and Judith R. Fay. Is Inducible Nitric Oxide Synthase a Target for Chemoprevention? Molecular Cancer Therapeutics. 2003; 2, 815– 823.
View at Publisher | View at Google Scholar - Vahora H, Ali Khan M, Alalami U, and Hussain A. (2007) The Potential Role of Nitric Oxide in Halting Cancer Progression Through Chemoprevention. Journal of Cancer Prevention 21:1-12.
View at Publisher | View at Google Scholar - LL, Miles DW, Happerfield L, Bobrow LG, Knowles RG (1995) Nitric oxide synthase activity in human breast cancer. British journal of cancer. 72(1): 41-44.
View at Publisher | View at Google Scholar - Korde Choudhari S., Chaudhary M., Bagde, S. Gadbail AR & Joshi V. (2013) Nitric oxide and cancer: a review. World J Surg Onc, 11: 118 .
View at Publisher | View at Google Scholar - Dueñas-Gonzalez A, Isales CM, del Mar Abad-Hernandez M, Gonzalez-Sarmiento R, Sangueza O, (1997) Expression of inducible nitric oxide synthase in breast cancer correlates with metastatic disease. Modern pathology: an official journal of the United States and Canadian Academy of Pathology, Inc. 10: 645-649.
View at Publisher | View at Google Scholar - Reveneau S, Arnould L, Jolimoy G, Hilpert S, Lejeune P, et al. (1999) Nitric oxide synthase in human breast cancer is associated with tumor grade, proliferation rate, and expression of progesterone receptors. Laboratory investigation; a journal of technical methods and pathology. 79: 1215-1225.
View at Publisher | View at Google Scholar - Tschugguel W, Schneeberger C, Unfried G, Czerwenka K, Weninger W, et al. (1999) Expression of inducible nitric oxide synthase in human breast cancer depends on tumor grade. Breast cancer research and treatment. ;56: 143-149.
View at Publisher | View at Google Scholar - Jadeski LC, Hum KO, Chakraborty C, Lala PK. (2000) Nitric oxide promotes murine mammary tumour growth and metastasis by stimulating tumour cell migration, invasiveness and angiogenesis. International journal of cancer. 86: 30-39.
View at Publisher | View at Google Scholar - Vakkala M, Kahlos K, Lakari E, Paakko P, Kinnula V, et. al, (2000) Inducible nitric oxide synthase expression, apoptosis, and angiogenesis in in situ and invasive breast carcinomas. Clinical Cancer Research. 6: 2408-2416.
View at Publisher | View at Google Scholar - Loibl S, von Minckwitz G, Weber S, Sinn HP, Schini-Kerth VB, et al. (2002) Expression of endothelial and inducible nitric oxide synthase in benign and malignant lesions of the breast and measurement of nitric oxide using electron paramagnetic resonance spectroscopy. Cancer. 95:1191-1198.
View at Publisher | View at Google Scholar - Bulut AS, Erden E, Sak SD, Doruk H, Kursun N, et. al, (2005) Significance of inducible nitric oxide synthase expression in benign and malignant breast epithelium: an immunohistochemical study of 151 cases. Virchows Archiv. 447:24-30.
View at Publisher | View at Google Scholar - Loibl S, Buck A, Strank C, von Minckwitz G, Roller M, et al. (2005) The role of early expression of inducible nitric oxide synthase in human breast cancer. European journal of cancer. 41:265-271.
View at Publisher | View at Google Scholar - Soini Y, Kahlos K, Puhakka A, Lakari E, Säily M, Paakko P et al. (2005) Expression of inducible nitric oxide synthase in healthy pleura and in malignant mesothelioma. British journal of cancer. 83:880-886.
View at Publisher | View at Google Scholar - Reiner A, Neumeister B, Spona J, Reiner G, Schemper M, et. al, (1990) Immunocytochemical localization of estrogen and progesterone receptor and prognosis in human primary breast cancer. Cancer research, 50:7057-7061.
View at Publisher | View at Google Scholar - Wulfing P, Diallo R, Muller C, Wulfing C, Poremba C, Heinecke A, et al. (2003) Analysis of cyclooxygenase-2 expression in human breast cancer: high throughput tissue microarray analysis. Journal of cancer research and clinical oncology. 129:375-382.
View at Publisher | View at Google Scholar - Corp I. IBM SPSS (2013) statistics for windows, version 22.0. Armonk, NY: IBM Corp.
View at Publisher | View at Google Scholar - Chinje EC, Stratford IJ. (1997) Role of nitric oxide in growth of solid tumours: a balancing act. Essays in biochemistry. 32:61-72.
View at Publisher | View at Google Scholar - Ziche M, Morbidelli L, Choudhuri R, Zhang HT, Donnini S, Granger HJ, et al. (1997) Nitric oxide synthase lies downstream from vascular endothelial growth factor-induced but not basic fibroblast growth factor-induced angiogenesis. Journal of Clinical Investigation. 99(11):2625-2634.
View at Publisher | View at Google Scholar - Lala PK, Chakraborty C. (2001) Role of nitric oxide in carcinogenesis and tumour progression. The lancet oncology. 2:149-56.
View at Publisher | View at Google Scholar - Forstermann U, Closs EI, Pollock JS, Nakane M, Schwarz P, et. al, (1994) Nitric oxide synthase isozymes. Characterization, purification, molecular cloning, and functions. Hypertension. 23: 1121-1131.
View at Publisher | View at Google Scholar - Oka K, Suzuki Y, Iida H, Nakano T. Pd-ECGF (2003) positivity correlates with better survival, while iNOS has no predictive value for cervical carcinomas treated with radiotherapy. International Journal of Radiation Oncology Biology Physics. 57:217-221
View at Publisher | View at Google Scholar - Glynn SA, Boersma BJ, Dorsey TH, Yi M, Yfantis HG, ,et al. (2010) Increased NOS2 predicts poor survival in estrogen receptor–negative breast cancer patients. The Journal of clinical investigation.120
View at Publisher | View at Google Scholar
