

Mini Review Article | DOI: https://doi.org/10.31579/2835-8325/051
Ileocecal Tuberculosis Mimicking Malignant Tumors
1 The First College of Clinical Medical Science, China Three Gorges University, Yichang, China
2 Institute of Digestive Disease, China Three Gorges University, Yichang, China.
3 Department of Gastroenterology, Yichang Central People’s Hospital, Yichang, China.
*Corresponding Author: Wei Liu, Institute of Digestive Disease, China Three Gorges University, 8 Daxue Road, Yichang 443000.
Citation: Qian Hu, Wei Liu, Shi-Hua Zheng, (2024), Ileocecal tuberculosis mimicking malignant tumors”, Clinical research and Clinical reports 6(2): DOI: 10.31579/2835-8325/051
Copyright: © 2024, Wei Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 November 2024 | Accepted: 11 December 2024 | Published: 23 December 2024
Keywords: tomography; lymphocytic; abdominal pain
Abstract
A 77-year-old man with no significant past medical history presented with right lower abdominal pain. He complained weight loss of 5 kg in 3 months. The patient denied fever, vomiting, diarrhea, and change of stool color.
Introduction
A 77-year-old man with no significant past medical history presented with right lower abdominal pain. He complained weight loss of 5 kg in 3 months. The patient denied fever, vomiting, diarrhea, and change of stool color. Physical examination revealed a distended abdomen with tenderness at palpation within the right lower quadrant. The initial blood count showed mild anemia (hemoglobin 10.6 g/dL) and hypoproteinemia (29 g/L). Normal lungs were shown by computed tomography (CT) of the chest. Abdominal CT showed bowel wall thickening in the caecum and ascending colon (Figure 1A, B).
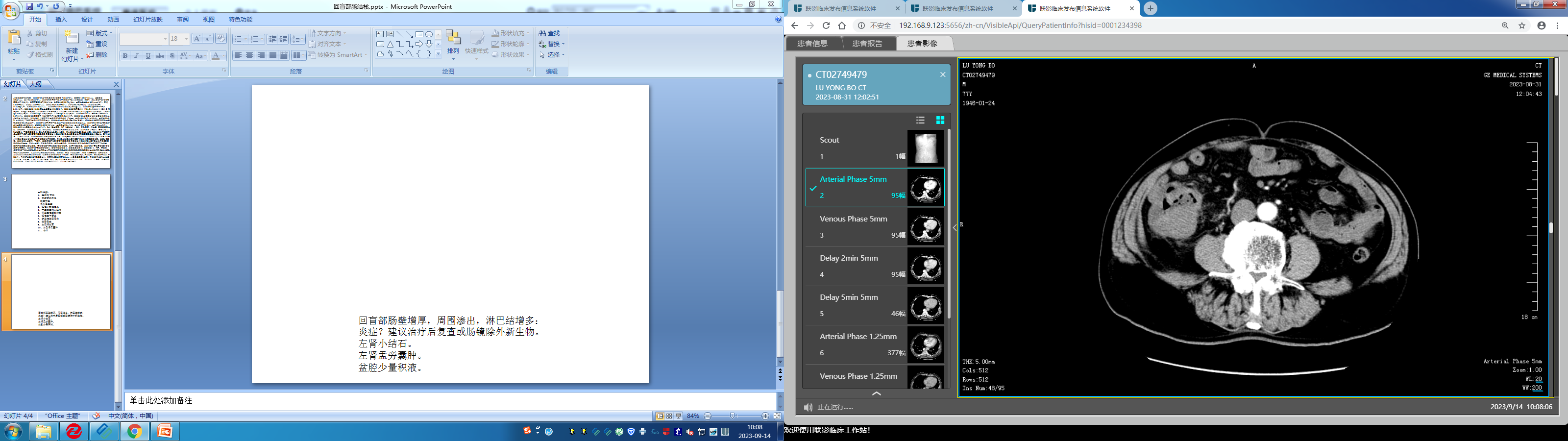
Figure 1: A, B. Abdominal CT showed bowel wall thickening in the caecum and ascending colon.
Retrograde ileocolonoscopy was performed. A 5-cm semicircular, exophytic neoplasm with an ulcerating surface occupying the ileocecal region was discovered (Figure 2A, B, C).
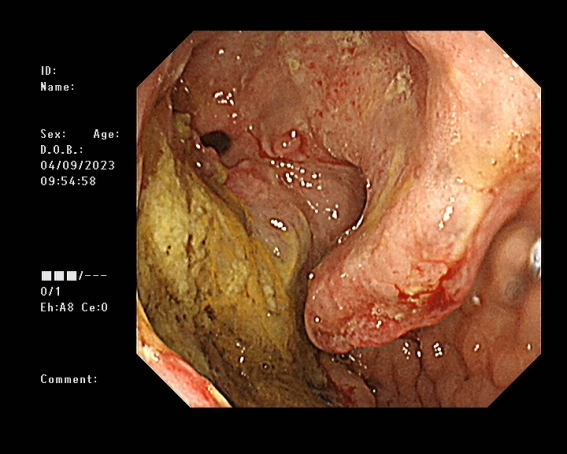
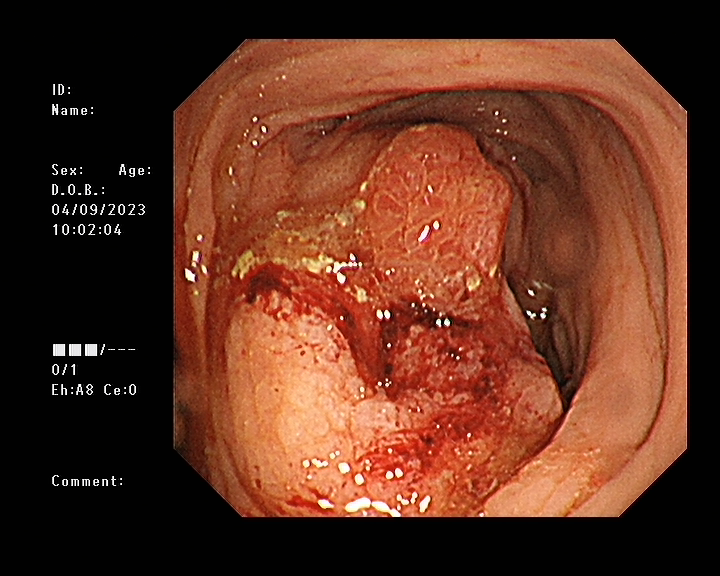
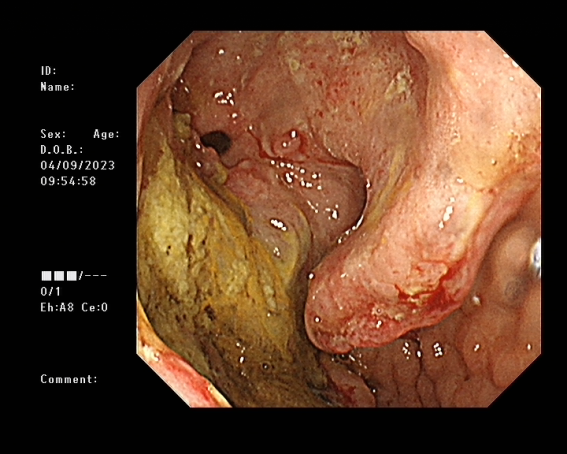
Figure 2: A, B, C. Retrograde ileocolonoscopy showed a 5-cm semicircular, exophytic neoplasm with an ulcerating surface occupying the ileocecal region.
Upper gastrointestinal endoscopy did not reveal any irregularities. Histologic examination of samples extracted from the tumor by means of hematoxylin and eosin staining showed a lymphocytic infiltrate of the colonic mucosa and granulomatous inflammation (Figure 2D).
Figure 2: D. Hematoxylin and eosin staining revealed a lymphocytic infiltrate of the colonic mucosa and granulomatous inflammation. No malignant cell was found. The T-SPOT.TB test was positive. Diagnosis of Ileocecal tuberculosis was confirmed by the detection of DNA of Mycobacterium tuberculosis though polymerase chain reaction. The lesion was isolated and localized to the ileocecal region considering normal chest CT and upper gastrointestinal endoscopy. The patient responded well to conventional antituberculous drugs. In conclusion, Ileocecal tuberculosis may mimic malignant tumors in endoscopic and radiographic findings, which is a rare cause of abdominal pain [1-3]. Endoscopic and molecular techniques may contribute to make a correct diagnosis and avoid risky surgical interventions.
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Written informed consent was obtained from the patient for publication of this “GI Image”. Board institutional approval was not required.
Author’s contributions
Collection of data and writing: Qian Hu.
Manuscript preparation: Shi-Hua Zheng.
Final approval of the manuscript: Wei Liu.
Introduction
A 77-year-old man with no significant past medical history presented with right lower abdominal pain. He complained weight loss of 5 kg in 3 months. The patient denied fever, vomiting, diarrhea, and change of stool color. Physical examination revealed a distended abdomen with tenderness at palpation within the right lower quadrant. The initial blood count showed mild anemia (hemoglobin 10.6 g/dL) and hypoproteinemia (29 g/L). Normal lungs were shown by computed tomography (CT) of the chest. Abdominal CT showed bowel wall thickening in the caecum and ascending colon (Figure 1A, B).
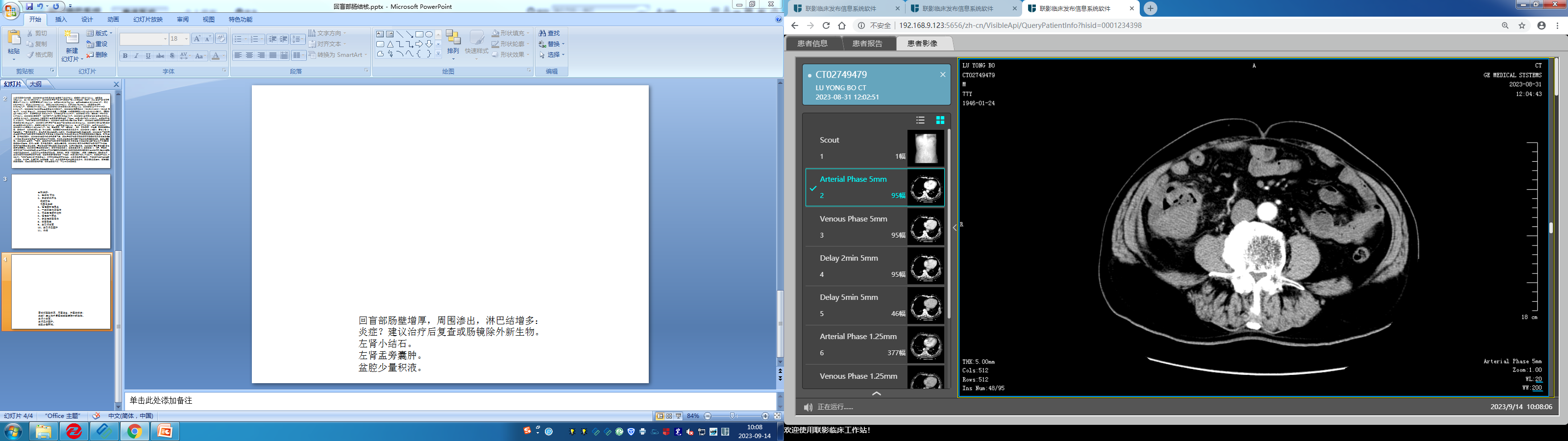
Figure 1: A, B. Abdominal CT showed bowel wall thickening in the caecum and ascending colon.
Retrograde ileocolonoscopy was performed. A 5-cm semicircular, exophytic neoplasm with an ulcerating surface occupying the ileocecal region was discovered (Figure 2A, B, C).

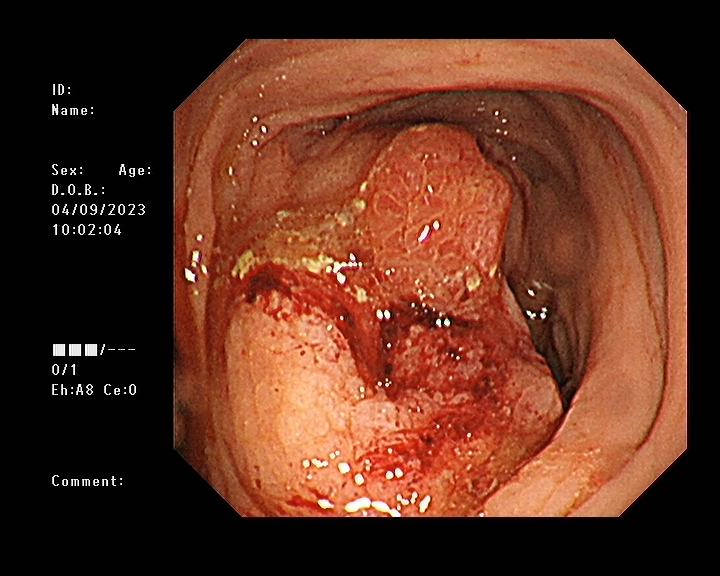
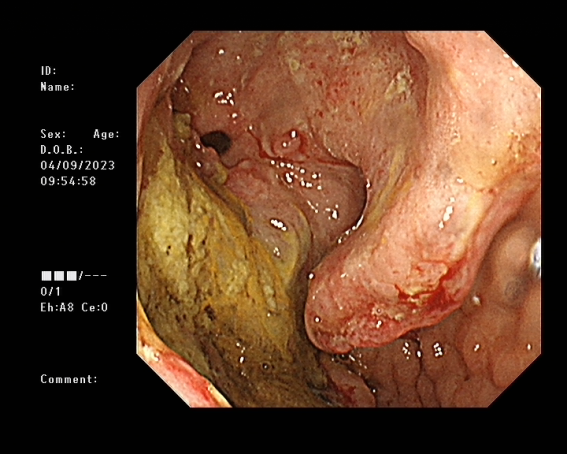
Figure 2: A, B, C. Retrograde ileocolonoscopy showed a 5-cm semicircular, exophytic neoplasm with an ulcerating surface occupying the ileocecal region.
Upper gastrointestinal endoscopy did not reveal any irregularities. Histologic examination of samples extracted from the tumor by means of hematoxylin and eosin staining showed a lymphocytic infiltrate of the colonic mucosa and granulomatous inflammation (Figure 2D).
Figure 2: D. Hematoxylin and eosin staining revealed a lymphocytic infiltrate of the colonic mucosa and granulomatous inflammation. No malignant cell was found. The T-SPOT.TB test was positive. Diagnosis of Ileocecal tuberculosis was confirmed by the detection of DNA of Mycobacterium tuberculosis though polymerase chain reaction. The lesion was isolated and localized to the ileocecal region considering normal chest CT and upper gastrointestinal endoscopy. The patient responded well to conventional antituberculous drugs. In conclusion, Ileocecal tuberculosis may mimic malignant tumors in endoscopic and radiographic findings, which is a rare cause of abdominal pain [1-3]. Endoscopic and molecular techniques may contribute to make a correct diagnosis and avoid risky surgical interventions.
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Written informed consent was obtained from the patient for publication of this “GI Image”. Board institutional approval was not required.
Author’s contributions
Collection of data and writing: Qian Hu.
Manuscript preparation: Shi-Hua Zheng.
Final approval of the manuscript: Wei Liu.
References
- Yu SM, Park JH, Kim MD. (2012). A case of sigmoid colon tuberculosis mimicking colon cancer. J Korean Soc Coloproctol 2012;28:275-277.
View at Publisher | View at Google Scholar - Mukhtar AU. (2000). Ileo-caecal tuberculosis mimicking colonic tumour--case report. Cent Afr J Med, 46:44-45.
View at Publisher | View at Google Scholar - King HC, Voss EC, Jr. (1980). Tuberculosis of the cecum simulating carcinoma. Dis Colon Rectum, 23:49-53.
View at Publisher | View at Google Scholar
